
Abstract
The objective of this study was to determine femoral cartilage thickness (FCT) in patients with Klinefelter syndrome (KS), which is the most common sex chromosome disorder in men with varying degrees of androgen deficiency. This cross-sectional controlled study was conducted in a tertiary care center. Participants were 33 male patients (mean age = 36.2 years) with KS and 35 aged-matched healthy male controls (mean age = 32.9 years). Femoral condyle cartilage was measured by ultrasonography at three locations in each knee. Total testosterone, estradiol, sex hormone binding globulin, free androgen index, bioavailable testosterone, and albumin levels were measured. Femoral cartilage of patients at right and left knee lateral (3.03 and 2.99 mm), mid (3.81 and 3.74 mm), and medial (3.01 and 3.20 mm) were statistically thicker than in controls (right and left knee lateral 2.29 and 2.36 mm, mid 2.64 and 2.53 mm, medial 2.39 and 2.32 mm, respectively, p < .001). There was no significant correlation between FCT and sex hormones. In conclusion, patients with KS had thicker femoral cartilage. Relatively low testosterone levels in these patients and altered estrogen metabolism may hypothetically explain increased cartilage thickness in these patients.
Osteoarthritis (OA) is a major cause of disability and one of the most common disorders of the joints. OA is a disease of articular cartilage, however, changes in subchondral bone are also responsible (Creamer & Hochberg, 1997). When the disease severity increases, articular cartilage is lost and bony changes become apparent (Wluka, Wang, Davis, & Cicuttini, 2005). Heredity, obesity, trauma, and physical overload are risk factors for development of OA and the disease becomes more common with age, after 50, and women are more frequently affected than men, suggesting the potential role of differences in sex steroid levels or tissue response to these sex steroids (Bijlsma, Berenbaum, & Lafeber, 2011). Klinefelter’s syndrome (KS) is one of the most common forms of male hypogonadism and chromosome aneuploidy in humans characterized by small firm testes, gynecomastia, hypogonadism, and high follicle-stimulating hormone levels (Lanfranco, Kamischke, Zitzmann, & Nieschlag, 2004). Affected males carry one or more additional X chromosomes, and the karyotype 47XXY is most prevalent type. The changes of sex steroid levels in patients with KS offer an exceptional opportunity to investigate changes in articular cartilage in these patients. Ultrasonography is an inexpensive and widely available technique that can effectively and reliably measure the cartilage thickness (Filippucci et al., 2006). The aim of this cross-sectional case–control study was to investigate femoral cartilage thickness values in patients with KS and to compare with those of healthy men matched for age and body mass index (BMI).
Materials and Method
Patients
Thirty-three patients with nonmosaic KS were consequently recruited from the infertility outpatient clinic of the Department of Urology, Erciyes University. The patients who were older than 18 years and who were genetically proven to have KS were included in the study. Patients with following characteristics were excluded: people above 50 years of age and people who have a history of knee surgery, synovial fluid aspiration, intra-articular injection, or joint aspiration for any reason; and people who have an endocrine disease. Thirty-five-year men and BMI matched healthy men (1:1) who did not have infertility problems or rheumatic disorders were recruited from hospital visitors. For all patients karyotyping was performed. None of the patients or healthy controls had regular exercises. All the participants were informed of the study protocol, and written consents were obtained from all participants. The study was approved by the local ethical committee of Erciyes University, Faculty of Medicine.
Demographic and clinical features in all participants (including previous medical history, age, BMI) were recorded. Laboratory variables of patients including total testosterone, estradiol, sex hormone binding globulin, free androgen index, bioavailable testosterone, and albumin as well as follicle stimulating hormone and luteinizing hormone were recorded. Ultrasonography of the femoral condylar cartilage was performed.
Ultrasonographic Measurements of the Femoral Cartilage Thickness
Ultrasonography of the knee is particularly useful in assessing articular cartilage of the femoral condyles and also gives important anatomical information about structural integrity of the supporting tissues around the knee (Meenagh et al., 2006). Ultrasonography was performed by an experienced rheumatologist using a commercially available ultrasonography scanner with a linear probe (7-12 MHz, Logic P5: GE Medical Systems, Buckinghamshire, UK). Femoral cartilage was examined with patients in supine position and both knees were at maximum flexion. The probe was placed in axial plane on the suprapatellar area and the cartilage was visualized. Three midpoint measurements of the cartilage thickness were taken in both knees: at the lateral femoral condyles, intercondylar areas, and medial condyles (Figure 1). To reduce bias, the sonographer was blinded to participants’ identity and diagnosis.
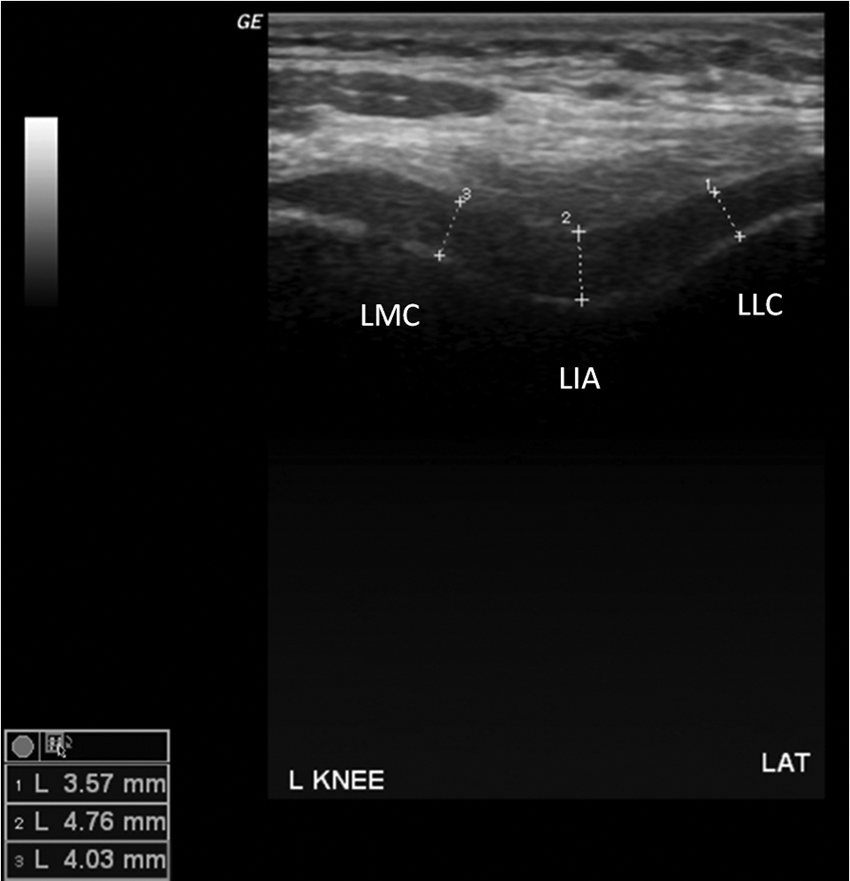
Ultrasonographic images (suprapatellar axial view) showing left femoral cartilage measurements in a patient with Klinefelter’s syndrome
Statistical Analysis
Statistical analysis was performed using Statistical Package for Social Sciences (SPSS 15.0, SPSS Inc.) software. Data were expressed as the mean value ± standard deviation. The normality of distribution was analyzed by Kolmogorov–Smirnov test, and categorical variables were analyzed by chi-square test and correlations by using Pearson correlation coefficients. The statistical significance of the mean difference was examined using the Student’s t test for independent samples. The subgroups were also analyzed using independent samples t test. A p value .05 was considered statistically significant.
Results
Sixty-six knees in 33 patients with KS and 70 knees in 35 healthy controls were examined. Demographic characteristics of patients and controls are summarized in Table 1. There was no statistically significant difference in age and BMI between patients and controls; the mean ages were 36.24 ± 5.51 and 32.86 ± 5.55 and BMI were 25.49 ± 4.46 and 24.83 ± 3.33 for KS patients and healthy controls, respectively (p > .05). Twenty (60.6%) of the patients and 20 (57.1%) of the controls were nonsmokers, which was not statistically significant (p > .05). None of the patients or controls had regular exercise habits and were all sedentarily living men defined as those expending less than 10% of their daily energy in the performance of moderate- and high-intensity activities (such as walking, climbing stairs, gardening, etc.). This was decided by taking a survey of all patients; we questioned the frequency, duration, and intensity of the daily living activities and the answers were noted. Mean values of sex hormones in patients were as follows: follicle stimulating hormone 34.4 ± 12.2 IU/mL, luteinizing hormone 22.4 ± 10.3 IU/mL, total testosterone 219.1 ± 114.2 ng/dL, estradiol 33.4 ± 15.8 pg/mL, sex hormone binding globulin 45.7 ± 29.5.1 nmol/L, albumin 4.5 ± 0.3 g/dL, free androgen index 22.9 ± 21.2, and bioavailable testosterone 92.1 ± 64.1 ng/dL.
Demographics and femoral Cartilage Thickness in Patients with Klinefelter Syndrome (KS) and Controls (Mean± Standard Deviation)
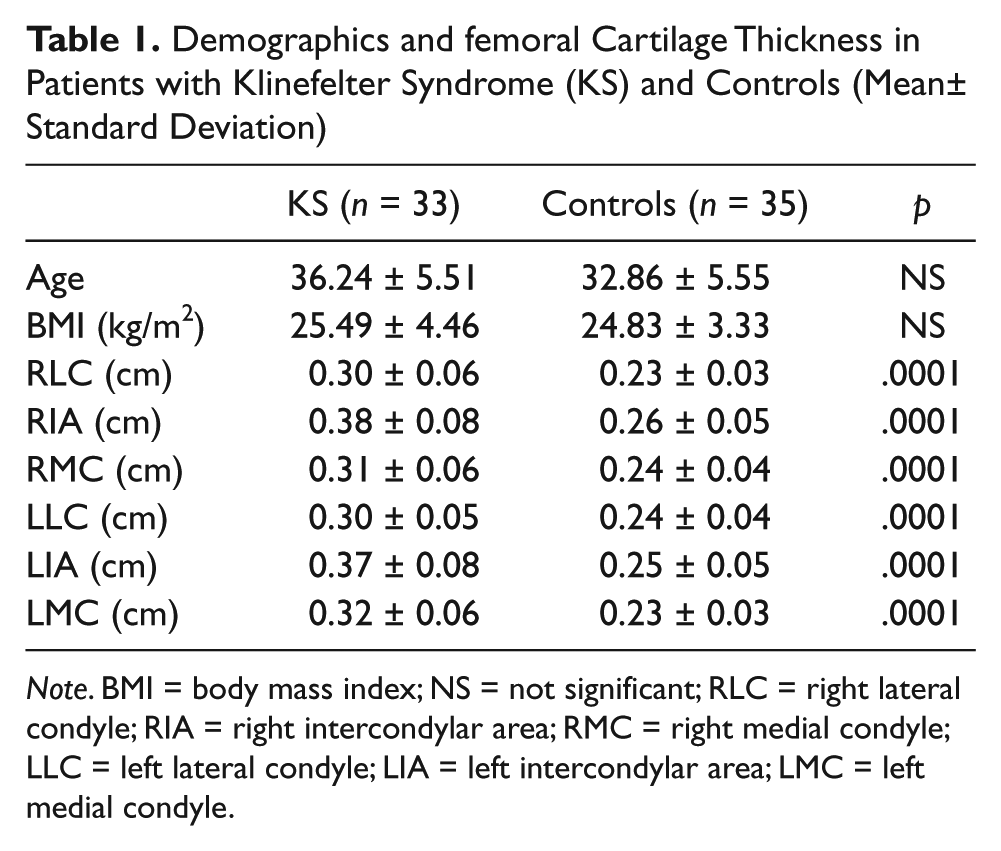
Note. BMI = body mass index; NS = not significant; RLC = right lateral condyle; RIA = right intercondylar area; RMC = right medial condyle; LLC = left lateral condyle; LIA = left intercondylar area; LMC = left medial condyle.
The results of FCT are shown in the Table 1. The patients with KS had thicker femoral cartilage than the healthy controls at all measurement sites. There was no significant correlation between FCT and sex hormone levels (r values ranges −0.33 to 0.22 and p > .05 for all). Patients with history of testosterone treatment (n = 16, right and left knee lateral 0.31 and 0.29 cm, mid 0.38 and 0.37 cm, medial 0.30 and 0.30 cm, respectively) had similar FCT (p > .05) compared with the patients who never used testosterone treatment (n = 17, right and left knee lateral 0.29 and 0.30 cm, mid 0.38 and 0.38 cm, medial 0.31 and 0.33 cm, respectively).
Comments
This is the first study documenting FCT and assessing the relationship between sex hormones and cartilage thickness in patients with KS. Our results show that patients with KS had thicker femoral cartilage than the healthy matched controls; femoral cartilage of patients at right and left knee lateral (0.30 and 0.30 cm), mid (0.38 and 0.37 cm), and medial (0.31 and 0.32 cm) were statistically thicker than those in controls (right and left knee lateral 0.23 and 0.24 cm, mid 0.26 and 0.25 cm, medial 0.24 and 0.23 cm, respectively, p < .001). However, there was no relationship between sex hormone levels and cartilage thickness (r values were not statistically significant).
The role of androgens and preandrogens on the cartilage structure may be very complex. In previous studies, it was suggested that in healthy men higher serum testosterone levels are associated with greater cartilage in the tibiofemoral compartment; however, serum testosterone levels have no association with cartilage volume or bone structures in women (Cicuttini et al., 2003; F. S. Hanna et al., 2007). Steroid hormones have been found to counterbalance catabolic chondrocyte metabolism and counteract proinflammatory effects of catabolic cytokines such as interleukin-1β, interleukin-6, and tumor necrosis factor (Englert et al., 2006). In male rabbits, castration results in an increase in apoptosis and a decrease in the proliferation of the chondrocytes in the growth plate (Irie, Aizawa, & Kokubun, 2005). However, little data are available about the effect of testosterone on joints. In a previous cross-sectional study, the association between serum-free testosterone levels and tibial cartilage volume has been documented; however, these patients were followed for a while and it was seen that serum-free testosterone was associated with increased cartilage loss (F. Hanna et al., 2005). There is still no robust evidence for a connection between serum sex hormone levels and OA (Koelling & Miosge, 2010). In a previous study, patients with polycystic ovary syndrome (PCOS) were assessed for FCT using same method as ours (Eryilmaz et al., 2012). Patients with PCOS were shown to have thicker femoral cartilage compared with the matched controls (Eryilmaz et al., 2012).
Our results suggest that patients with KS had thicker cartilage than healthy controls. It seems that this matter may be multifactorial and there may be many influencing factors other than low testosterone levels effecting cartilage metabolism in patients with KS. The complex biology of cartilage metabolism as well as complex nature of KS poses some difficulty to make clear-cut conclusions.
A limitation of this study may be the lack of cartilage marker results. Biomarker development for OA diagnosis is important for research in OA. Combinations of cartilage-derived and bone-derived biomarkers have been used to subgroup OA patients that could influence treatment and address the importance of bone turnover in cartilage integrity (Patra & Sandell, 2011). In patients with KS, cartilage markers may serve to better understand the causal relationship between sex steroids and cartilage thickness.
Conclusions
In patients with KS, FCT is higher than in healthy controls and there is no apparent association with sex steroid levels, at least in this cross-sectional design. Further studies are needed that explore the factors influencing the cartilage metabolism in patients with KS.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.