
Abstract
The majority of men’s sports need high levels of strength and power. The effects of any given type of performance-enhancing substance are mostly directly related to its ergogenic effects (enhanced strength, higher energy production, and better recovery), anabolic potential (increased protein synthesis, especially in muscles), and/or stimulating properties (increased attention and loss of fear), which give a competitive advantage to athletes. A descriptive correlational study was conducted to identify bodybuilders’ and athletes’ perception toward substance use and to identify the relationship between substance use and those athletes’ sociodemographic characteristics of age, level of education, social status, and monthly income. A purposive “nonprobability” sample of 172 bodybuilding athletes were recruited from gym users of Baghdad city. The study found that two fifths of those who used anabolic-androgenic steroids (AAS) were 19 years old or younger, less than one half were overweight (body mass index = 25-29.9), two fifths of participants enjoyed exercise/training to an extreme level, two fifths of study participants highly perceived the improvement of athletic performance, two fifths of the study participants highly perceived the importance of improving athletic performance, less than half of the study participants used AAS, one quarter of the study participants who used AAS had been influenced by their coaches to use such substances, and more than one third of the study participants who used AAS were using such substances in the form of oral tablets and intramuscular injection together.
Keywords
Background
The majority of men’s sports need high levels of strength and power. The highest level of competition technique is a strong measure of success that athletes must bring under control to exploit athletic performance (Rogol, 2010).
Two types of substances used in sports have been recognized by contemporary sport legislation: (a) noncontrolled substances, such as the majority of nutritional supplements and (b) products that contain prohibited substances, the use of which is often referred to as “doping” (Ayotte et al., 2001).
The terms anabolic steroids, anabolic-androgenic steroids (AAS), performance-enhancing supplements, or performance-enhancing substances (PES) could be used interchangeably. Athletes, from professional athletes to junior high school students, use PESs. AAS have serious adverse effects, such as reduced fertility and gynecomastia in males, masculinization in women, cardiovascular complications, cancer, liver toxicity, behavioral disorders, and, after prolonged high-dose usage, irreversible organ damage (Sánchez-Osorio, Duarte-Rojo, Martínez-Benítez, Torre, & Uribe, 2008). Other known side effects include atherosclerosis, hypertension, dilated cardiomyopathy, and sudden death. Psychiatric side effects involve irritability, aggressiveness, mood swings, decreased impulse control, and suicidal or homicidal behavior (Casavant, Blake, Griffith, Yates, & Copley, 2007).
The effects of any given type of PES are mostly directly related to its ergogenic effects (enhanced strength, higher energy production, and better recovery), anabolic potential (increased protein synthesis, especially in muscles), and/or stimulating properties (increased attention and loss of fear), which give a competitive advantage to athletes. There are two different origins of the prohibited substances: exogenous, that is, cannot be produced by the body naturally, and endogenous, that is, substances naturally produced by the body. Synthetic AAS, such as methyltestosterone and nandrolone, are examples belonging to the former category. Endogenous hormones, such as human growth hormone, erythropoietin, testosterone, dehydroepiandrosterone, and insulin, are forms of the latter group. There is a belief among some athletes, especially bodybuilders, that anabolic steroids will allow them to increase the periods of intensive training in order to enhance muscle strength (Bergman & Leach, 1985). Taking ergogenic “effectors,” such as recombinant human insulin-like growth factor-I, anabolic steroids, or erythropoietin, could enhance the size and strength of the athletes, which makes them perform better. Anabolic steroids may also be used by some boys who are not athletes, as they believe that they, and perhaps other ergogenic effectors, help them “look better” (Rogol, 2010).
Men who are concerned about their body image may be motivated to use AAS at first, and then illogically, their concern may extend to involve muscularity even as they are growing bigger on AAS. Muscularity can be considered as key factor framing self-concept for some men, with a loss of muscularity triggering anxiety. Anxiety over loss of musculature contributes to AAS dependence (Brower, 2002, Brower, Eliopulos, Blow, Catlin, & Beresford, 1990). Pope, Phillips, and Olivardia (2000) have described bodybuilders as having an altered perception of body image, leading to psychopathology.
Athletes who practice recreational sports may abuse these drugs to enhance their physical appearance and may base such practices on teammate recommendations or underground literature (Urhausen, Albers, & Kindermann, 2004).
The use of these PESs among professional athletes persists, even in the face of increasing public scrutiny and severe consequences (Rogol, 2010). Many studies have examined the prevalence of gym users’ use of performance-enhancing drugs such as anabolic steroids, clenbuterol, and growth hormones and indicate that performance-enhancing drugs are used widely, ranging from 1% to 12% among adolescents in an open population, from 3% to 31% among gym users, and from 16% to 50% among bodybuilders (Conway & Morgan, 2002; Irving, Wall, Neumark-Sztainer, & Story, 2002; Kindlundh, Isacson, Berglund, & Nyberg, 1999; Lindstrom, Nilsson, Katzman, Janzon, & Dymling, 1990; Maharaj et al., 2000; Vogels et al., 1996; Yesalis & Bahrke, 2000).
Method
Instrument Description
The study instrument was developed by the researchers through extensive reviewing of the relevant literature. It encompasses seven domains: demographic and personal characteristics (age, level of education, body mass index (BMI), social status, and monthly income), users’ perception, Motives for Physical Activities Measure–Revised, hormones use, fat burners and endurance boosters, illicit fat burners and endurance boosters, and athlete’s future.
Instrument Validity
The study instrument was translated into Arabic and then validated through presenting it to 10 faculty members for modifications. Back-translation (decentered translation, which involves the possibility of modifications to items of the original scale), which reflects the goal of replacing culturally exclusive language with more universally understood language, was carried out by two faculty members at the College of Nursing at the University of Baghdad who were unfamiliar or “blinded” to the original wording. The back-translation correlated to the original text (English) language to a great degree (α = .90).
Study Sample
A purposive “nonprobability” sample of 172 bodybuilding athletes were recruited from gym users to participate in the current study. These gyms do not belong to the Iraqi Bodybuilding Federation and are not licensed. These gyms lie on either side (Al-karch and Al-russafa) of Baghdad city; registered clubs were not included. Selected gyms were distributed across different neighborhoods. Self-reported questionnaires were distributed to those athletes; 200 questionnaires were distributed, of which 172 were returned. Data were analyzed by using SPSS 16 through the application of descriptive statistical measures of frequency, percentage, and mean of scores and the inferential statistical measure of linear regression. Written consent was obtained from participants, who were assured that their answers would be kept confidential by the researchers for the purpose of research.
Results
Table 1 reports that two fifths of the study participants are 20 to 24 years old (n = 72; 41.9%), about one quarter of them are intermediate school graduates (n = 44; 25.6%), about less than the half are overweight (BMI = 25-29.9; n = 82; 47.7%), the majority of them are unmarried (n = 138; 80.2%), and less than the half of participants have sufficient monthly income (n = 74; 43%).
Participants’ Demographic and Personal Characteristics (N = 172)

Table 2 reports that less than the half of the study participants had four training sessions weekly (n = 79; 45.9%), with the vast majority having one training session daily (n = 159; 92.4%). Most participants trained for 1 to 2 hours daily (n = 113; 65.7%).
Participants’ Training History (N = 172)

Table 3 identifies that about two fifths of participants enjoy exercise/training to an extreme level (10 on a 10-point visual analogue scale; n = 64; 37.2%), about two fifths of study participants highly perceive the importance of improvement of athletic performance (e.g., increased explosive strength, sprint speed, endurance; n = 68; 39.5%), about two fifths of the study participants highly perceive the importance of improving the body composition (e.g., increase muscularity, vascularity, muscle hardness, reduce body fat, etc.; n = 105; 61.0%), about two fifths of the study participants perceive that physical exercise and “bodybuilding” can represent their identity and goals by improving their athletic performance and body composition (n = 67; 39.0%), and most of the study participants perceive that increase in hardness, leanness, and vascularity is more important for improving their body composition than increase in their size/weight (n = 112; 65.1%).
Participants’ Perceptions Toward Training

Table 4 reveals that less than the half of the study participants use AAS (n = 77; 44.8%).
Use of Anabolic-Androgenic Steroids

Table 5 describes that most of the study participants who use AAS have used such hormones in the early years of their lives (n = 30; 38.96%; for those 19 years old or younger and the same for the 20- to 24-year age-group).
Participants’ Ages on Using Anabolic-Androgenic Steroids for the First Time

Table 6 reports that about one quarter of the study participants who use AAS have used such hormones for the last time from 1 week earlier (n = 20; 25.97%).
The Last Time of Using Anabolic-Androgenic Steroids

Table 7 reports that one quarter of the study participants who used AAS have been influenced by their coaches to use such substances (n = 20; 25.97%).
Source of Influencing to Use Anabolic-Androgenic Steroids

Table 8 reports that more than one third of the study participants who use AAS are using such substances in the form of oral tablets and intramuscular injection together (n = 28; 36.36%).
Route of Administering Anabolic-Androgenic Steroids

Table 9 reports that more than one third of the study participants who use AAS in the form of injection were receiving injection from a nurse (n = 22; 36.6%), followed by a coach (n = 9; 15%).
The Person Who Gives Injection of Anabolic-Androgenic Steroids (n = 60)

Table 10 describes that about two fifths of the study participants who use AAS report no difference in using such substances between competitive season and off-season (n = 31; 40.8%).
Time of using Anabolic-Androgenic Steroids
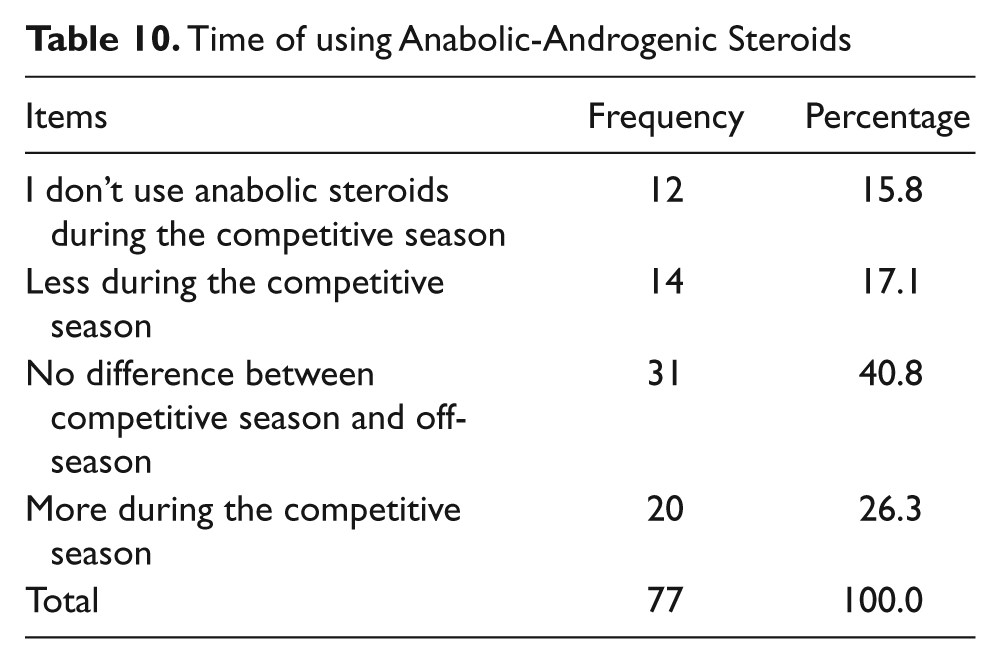
Table 11 describes that most of the study participants who use AAS have reported that their coaching staff know of their using such substances (n = 49; 63.6%).
Coaching Staff’s Knowledge of Anabolic-Androgenic Steroids Use
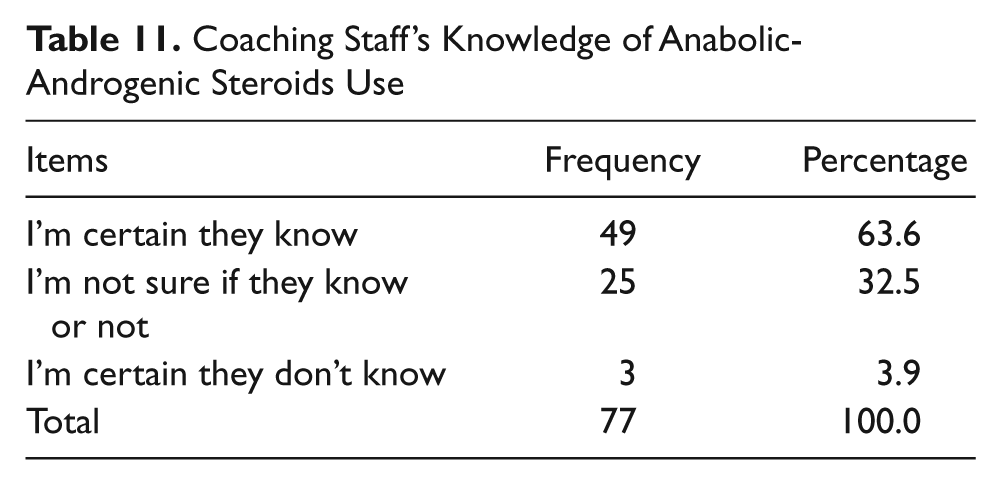
Table 12 reveals that most of the study participants who never used or have stopped using anabolic hormones have attributed this to their concern about what it might do to their health (n = 39; 41.1%).
Causes of Not Using or of Stopping Anabolic Hormones
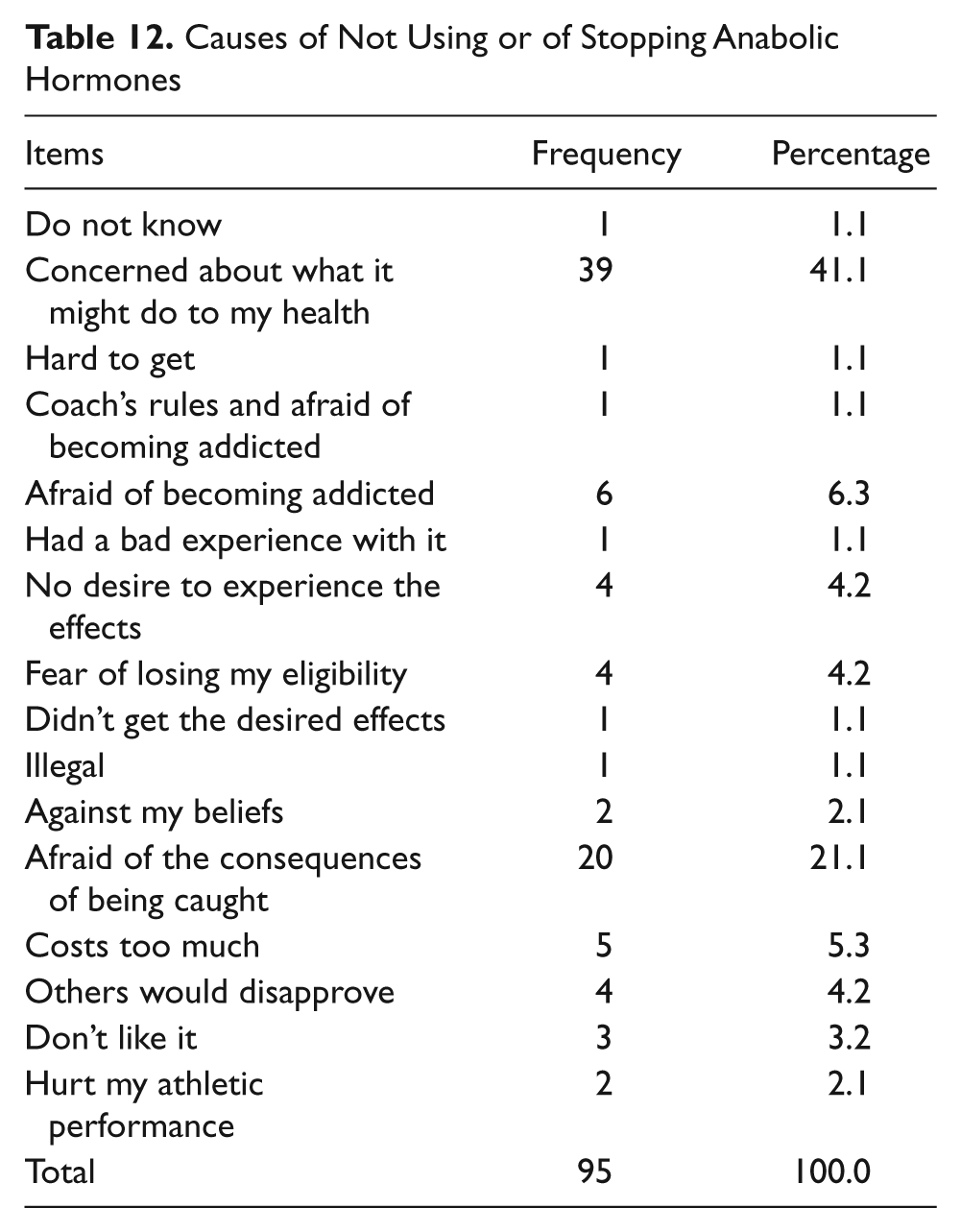
Table 13 reports that the vast majority of study participants do not use over-the-counter fat burners or endurance boosters such as Stacker 2 or Xenadrine (n = 156; 90.7%).
Using of the Over-the-Counter Fat Burners or Endurance Boosters

Table 14 elucidates that the vast majority of study participants do not use fat-burners or endurance boosters that they could not buy over the counter, such as clenbuterol, T3, dinitrophenol, or levoxyl (n = 154; 89.5%).
Using of Fat Burners or Endurance Boosters That You Could Not Buy Over-the-Counter

Table 15 describes that the vast majority of the study participants would not like to continue to use drugs or supplements if they were to discover absolute proof that the use of such substances, though they improve outward appearance, is likely to cause severe health problems (n = 154; 89.5%).
The Intent to Continue Using Drugs or Supplements

Table 16 describes that about one third of the study participants do not know the number of years they will be willing to sacrifice to meet all of their physical training goals through the use of drugs or supplements but know that using these drugs would shorten their life.
Number of Years That Participants Intent to Sacrifice to Meet Physical Training Goals

Table 17 describes that most of study participants choose highest IQ and the worst physique rather than having the best physique in the room but the lowest IQ (n = 110; 64.0%).
Participants’ Preference Between Physique and IQ

Table 18 reports that most of study participants choose best physique and least financial success rather than most financial success and worst physique (n = 112; 65.1%).
Participants’ Preference Between Best Physique and Least Financial Success and Most Financial Success but Worst Physique

Table 19 reports that most of the study participants do not know how long will they use anabolic or ergogenic drugs (n = 100; 58.1%).
Duration of Participants’ Anticipation of Anabolic-Androgenic Steroids Use
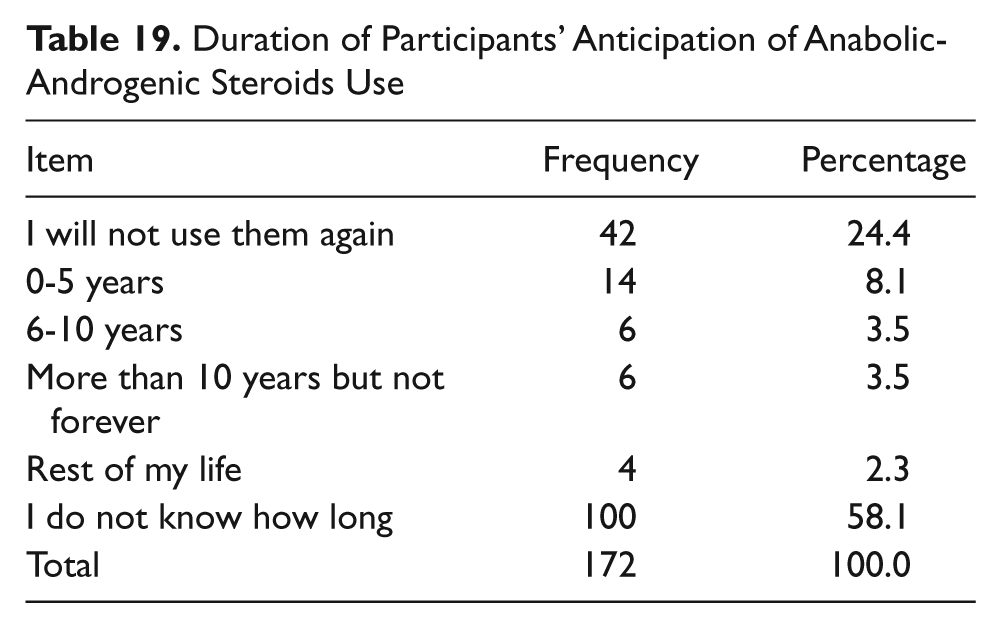
Table 20 describes that the 20- to 24-year-old age-group finds their highest identity and goals through physical exercise (10 out of 10 [n = 24 out of 71]; 9 out of 10 [n = 16 out of 71]; 8 out of 10 [n = 16 out of 71]).
Association Between Age and Identity and Goals

Table 21 reports that the 20- to 24-year-old age-group has used anabolic hormones more than other age-groups (n = 32), followed by the 25- to 29-year-old age-group (n = 24).
Association Between Age Group and Anabolic-Androgenic Steroids Use

Table 22 reports that there are significant associations of BMI, level of education, marital status, and age with identity and goals: p = .002, p = .003, p = .034, and p =.044, respectively.
Association Between Sociodemographic Variables and Identity and Goals

Note. df = degrees of freedom. Significant level of probability at p ≤ .05. Dependent variable: Identity and goals.
Discussion
Age and Marital Status
The study findings identify that about two fifths of study participants were 20 to 24 years old, which could be attributed to a perceived need to manifest musculature. This is consistent with Parkinson and Evans (2006), who found that most of the users begin using AAS in their teens or early twenties. Mean age was lower than that of Tahtamouni et al. (2008), who found the age of collegiate student enhancement to be 18 to 29 years and the age of athlete users to be 18 to 45 years. The majority (62.5%) were in the 18 to 29 years group, with a lower average age than that found by Cohen, Collins, Darkes, and Gwartney (2007), who revealed that the average AAS user was 31.1 years of age (SD = 9.16; age range = 18-76 years) and the median age was 29 years.
The study findings showed that the majority of study participants were unmarried (Cohen et al., 2007). This could be a social issue, as most youth cannot marry young because they are unable to afford the cost of marriage. This was consistent with that of Cohen et al. (2007), who revealed that about half had never been married, although many were currently married and some were divorced.
Education and Income
The findings identified that in about one quarter of study participants the highest educational level achieved was intermediate school, which can be attributed to lack of legislation for mandatory education in Iraq. This was inconsistent with that of Cohen et al. (2007), who revealed that the group was well educated; most held postsecondary degrees.
The study findings showed that less than the half of study participants reported sufficient monthly income, reflecting the economic recovery that Iraq has witnessed after the 2003 war, reflected in the living conditions of the population.
Personal Data
The study findings described that less than the half of study participants were overweight, which could be attributed to the fact that body weights of participants were not monitored either by the athletes themselves or by their coaches and to lack of knowledge of BMI calculation.
Users’ Perceptions
The study findings revealed that less than the half of study participants were using AAS, and less than the half of them had four training session per week. The vast majority of athletes had one training session per day, and most of them trained for 1 to 2 hours per day.
The study findings demonstrated that about two fifths of study participants have an extreme degree of enjoying exercise/training (10 on a 10-point visual analogue scale), followed by about one fifth who has less degree of enjoying exercise/training (9 on a 10-point visual analogue scale) and about one fifth who had a lesser degree of enjoying exercise/training (8 on a 10-point visual analogue scale). Furthermore, the study findings revealed that about one quarter of the study participants who used AAS were influenced by their coaches to use hormones. This was consistent with the study conducted by Schwenk and Costley (2002), who found that the athletes’ most common sources of dietary and supplement information was (in rank order) their trainer or coach, a family member or friend, magazines and books, a physician, and a nutritionist.
Tahtamouni et al. (2008) found that study participants had the greatest degree of interest/enjoyment when all the items that measure it were highly significant. In comparison with others, respondents considered their drive and motivation in the “average/above average to above average” range. Most responded as setting “average/high to high” goals and a majority self-identified as “perfectionists.” They tended to view “some to some/all” of life as a competition and felt that “half to most” of daily activities focused on goal achievement, and users self-identified as being driven and motivated, viewed life competitively, and focused on goal achievement.
Methods of Obtaining AAS
The study findings identify that retail stores were the most available source through which participants could obtain AAS. This could reflect that there was no monitoring from the health authorities in Iraq for importing and releasing such hormones. This was inconsistent with Tahtamouni et al. (2008), who reported that a friend (most probably a user) was the major source for AAS, whereas for athletes the sources were mainly a friend, and inconsistent with Cohen et al. (2007), who revealed that the Internet having become a major source for obtaining AAS, smaller percentages obtained AAS via local sources, friends or training partners, or physician’s prescription or by transporting them from foreign countries (Tahtamouni et al. 2008).
How Are AAS Being Used? Training Experience and Practices
The study findings demonstrate that less than the half of study participants had 4 days per week of training. This is consistent with Cohen et al. (2007), who revealed that the majority averaged four to five workout days per week. Most maintained a fairly standard training regimen and few trained 7 days per week, a level at which some concern might be noted.
The study findings demonstrated that one third of the study participants who use ASS were using such substances in the form of oral tablets and intramuscular injection together, whereas Cohen et al. (2007) and another studies (Evans, 1997; Parkinson & Evans, 2006) reported that injection has been noted as the most common method of self-administration of NMAAS.
The study findings revealed that about two fifths of study participants perceive to a maximum degree (10 points) that their identity and goals can be represented through physical exercise, followed by about one quarter (9 points), and about one fifth (8 points), respectively, on a 10-point visual analogue scale.
The study findings elucidated that most of the study participants prefer to improve their body composition through an increase in hardness, leanness, and vascularity rather than an increase in size/weight.
The study findings revealed that less than the half of study participants use AAS during physical exercise. They use such substances to enhance their athletic performance and increase their body size/weight. In this regard, a couple of studies indicate that the athletes’ decision to use AAS is triggered by a number of beliefs and values, some of them related to gaining muscular strength and improving performance and others involving expectations about friends’ use of these drugs (Carfi et al., 2005; Kindlundh et al., 1999). It has also been indicated that the use of these drugs is related to self-esteem, academic performance, use of other drugs, knowledge of other people who have used them, dissatisfaction with one’s own appearance, and frequency of gym visits (Carfi et al., 2005; Kindlundh et al., 1999; Vogels et al., 1996).
Two fifths of study participants who use AAS are 19 years old or younger and two fifths are 20 to 24 years old. This could be because the majority of participants within these two age-groups are probably not aware whether the behavior (using AAS) was healthy or not.
One third of study participants who use AAS were using such hormones in the form of oral tablets and intramuscular injection together. This could be attributed to the fact that athletes are not aware of the side effects of such hormones.
One third of study participants who use AAS in the form of injection were receiving injection administered by the nurse, followed by a smaller percentage who were administered injection by their coaches.
One tenth of study participants who use AAS were getting substances from retail stores. This could reflect the lack of monitoring of importing and releasing such substances by the ministry of health and the concerned athletic authorities.
In two fifths of study participants who use AAS, there is no difference in usage between the competitive season and the off-season. Most of participants who use AAS have reported that they are certain that their coaching staff know they use such substances. This could reflect that neither coaching staff nor concerned athletic authorities monitor AAS use or antidoping laws.
Most of the participants who never used or have stopped using anabolic hormones did so because of their concern about what it might do to their health. This could reflect that AAS users do not have enough knowledge about the actions and side effects of such hormones.
The vast majority of participants do not use over-the-counter fat-burners or endurance boosters. This could be because both athletes and their coaches do not have knowledge about the actions and side effects of such substances.
The vast majority of participants have no intention of continuing to use anabolic hormones or supplements if they discover absolute proof that the use of such substances, though they improve outward appearance, are likely to cause severe health problems. This could be attributed to the fact that they have concerns related to their harmful effects on health. This is inconsistent with the study of Wiefferink, Detmar, Coumans, Vogels, and Paulussen (2008), who found that most of the respondents who had used AAS intended to use them again in the future.
Most of the study participants prefer to have highest IQ and worst physique. Most of participants prefer to have best physique and least financial success. This could reflect their desire for a body image that could bring them others’ attention.
Higher degrees of motivation were recorded for 20- to 24-year-olds. Individuals in this age stage have the highest level of potential energy, and physical exercise is the best way to invest such energy.
The greatest feelings of identity and goals were recorded for the 20- to 24-year-old age-group. Individuals in this age stage are seeking others’ interest, especially that of the opposite sex, and physical exercise can figure in their identity and goals, which can be realized through having an outstanding physique. Ultimately, the scope of AAS use in Baghdad city, as seen by the researchers, could be close to that existing in other Iraqi cities.
Conclusion
In this study, we have identified that the participants started their gym training with the addition of dietary supplements and were later advised to add AAS and other hormones to improve their athletic performance. A common reason for taking AAS is that it seems to increase their body size and muscle strength. Some participants used AAS more in the on-season period because they wished to compete in bodybuilding and believed that AAS use was key for winning in competitions.
The information from this study may be valuable for officials. It is important that there be policies for monitoring the use and release of AAS that can assist in designing programs for the prevention of AAS abuse.
Bodybuilding athletes perceive that physical exercise, “bodybuilding,” can represent their identity and goals, which result from improving their athletic performance and improving their body composition. Most of the study participants perceive that increased hardness, leanness, and vascularity are more important in improving their body composition than increased size/weight. Most of the study participants who used AAS have used such substances in the early stages of their lives. One quarter of the study participants who used AAS had been influenced by their coaches to use such substances. More than one third of the study participants who used AAS were using such substances in the form of oral tablets and intramuscular injection together. More than one third of the study participants who used AAS in the form of injection were receiving the injection from a nurse, followed participants who received the injection from a coach. In two fifths of the study participants who used AAS, was no difference in using such substances between competitive season and off-season. Most the study participants who used AAS have reported that their coaching staff knew of their substance use. And ultimately, most the study participants who never used or have stopped using anabolic hormones have done so because of their concern about what it might do to their health.
Study Limitations
The results of this study must be analyzed with regard to its limitations. The study sample did not involve broader regions in Baghdad Governorate nor is it representative of all gym users in Baghdad Governorate.
Future Practice and Research
The findings of the present study have implications for clinical work and prevention efforts. Health professionals, in collaboration with Ministry of Youth and the Iraqi Olympic Committee, must conduct further studies that aim at determining health-related consequences for AAS users.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.