
Abstract
The purpose of this study was to determine if a particular set of health behaviors of health care providers and African American men (AAM) influence patient satisfaction from the AAM’s perspective. This descriptive, correlational study consisted of 505 AAM in North Carolina diagnosed with prostate cancer and enrolled in the North Carolina–Louisiana Prostate Cancer Project (PCaP). Analyses consisted of bivariate analyses and multiple regression. Patient-to-provider communication, interpersonal treatment, and provider-to-patient communication accounted for 45% (p ≤ .0001) of the variability in patient satisfaction. Interpersonal treatment (provider focusing on the patient) explained the greatest amount (F = 313.53, R2 = .39) of patient satisfaction. Since interpersonal treatment focuses on the patient and demonstrated to be the strongest predictor in patient satisfaction, it is noteworthy to consider the emphasis that should be placed on patient-centered care. In addition, knowing important variables positively affecting patient satisfaction provides useful information for developing appropriate interventions to improve AAM health care experiences.
Keywords
Introduction
Prostate cancer is the second leading cause of mortality in all men, and African American men (AAM) and Jamaican men of African descent have the highest prostate cancer incidence rates in the world (American Cancer Society, 2011). Over the past 25 years, the 5-year survival rate for prostate cancer has increased for both AAM and Caucasian men to nearly 100% when diagnosed and treated in the early stages (American Cancer Society, 2011). This improved survival rate has been attributed to early diagnosis and improved treatments; however, more AAM are diagnosed in late stages (metastatic disease) than Caucasian men where treatment options are less effective and outcomes are poorer, with only a 29% 5-year survival rate (American Cancer Society, 2011).
North Carolina Mortality Rates
While prostate cancer mortality rates for AAM in North Carolina have improved over the years (61.4 in 2004 to 53.4 in 2009), the prostate cancer burden and disparity gap for AAM compared with Caucasian men (23.6 in 2004 to 19.1 in 2009) in North Carolina has made very little progress in narrowing that gap (North Carolina State Center for Health Statistics, 2006, 2011). As evidenced by these prostate cancer mortality rates, the disparity death rate gap is similar to the national rate and continues to remain more than twice the rate for Caucasian men (American Cancer Society, 2011).
If early screening and treatment improves prostate cancer death rates, AAM are disadvantaged due to their underutilization of health care services; therefore, a more in-depth examination is needed to explore why more AAM do not use health care services. One needs to take caution in solely blaming AAM for avoiding or not using the health care system. How AAM view the health care system has historical underpinnings related to their treatment from general society as well as the health care system.
From a historical perspective, the United States has a long documented history of mistreating AAM. This mistreatment of AAM began with slavery, continued through legal segregation, and extended through more current times with discrimination and racism, which resulted in the likely foundations for mistrust or distrust. Even African American physicians, who provided care for AAM, were also mistreated by society and the American Medical Association (Aluko, 2008). These negative experiences from general society affected AAM’s health in many ways including when and how they interact with the health care system today (Washington, 2006). Lack of formal education affected literacy levels, type of jobs held, affordable health insurance, and access to care (Friedman, Corwin, Dominick, & Rose, 2009). AAM’s frame of reference for health was learned from their father and grandfathers (who rarely sought help from health professionals), who considered that men’s health was secondary to their primary social and family roles (Griffith et al., 2007). Some older African Americans viewed hospitals as a place where sick people go and die (Griffith et al., 2007).
Since the majority of health care professionals, who are Caucasian, lack understanding of this historical perspective for AAM, they tend to stigmatize AAM once they do seek health care (Dovidio et al., 2008). African Americans entering emergency departments for needed pain relief from sickle cell crisis are labeled drug seekers; others not taking medication as prescribed, regardless of ability to afford medications or understand how to take them, are labeled noncompliant; or some are labeled as noncaring for seeking care only after exhausting home remedies (Jenerette & Brewer, 2010; Martin et al., 2010). Regardless of educational level and adequate health insurance, AAM avoid the health care system, further worsening health conditions, as a result of mistrust, negative experiences, inferior care, and being stigmatized by health care providers and other health care workers (Byrne, 2008). One way to evaluate experiences of AAM with the health care system is to look at patient satisfaction.
Patient satisfaction is an indicator for quality of medical care received (National Committee for Quality Assurance, 2010; The Joint Commission, 2010). Examining patient satisfaction is an approach for investigating factors influencing health care services utilization and quality of care (Andersen, 2008). Patient satisfaction is conceptualized as a patient’s personal perception and evaluation of care (Hekkert, Cihangir, Kleefstra, Berg, & Kool, 2009). Multiple factors affect patient satisfaction such as age, mistrust, racism, education, health literacy, religious participation, health insurance, and access to care (Moore et al., in press; Napoles, Gregorich, Santoyo-Olsson, O’Brien, & Stewart, 2009); however, health behaviors affecting patient satisfaction for AAM have been understudied. In this article, we address health behaviors of AAM and health care providers related to the process of receiving medical care and AAM’s personal use of health care services to help us better understand the association with patient satisfaction. The purpose of this study was to explore whether a particular combination of patient self-reported health behaviors influenced patient satisfaction with the health care system among a sample of AAM in North Carolina with prostate cancer.
Conceptual Framework
A modified form of Andersen’s Behavioral Model for Health Services Use was used to guide this study (Andersen, 2008). Although the original model has four broad domains—contextual characteristics, individual characteristics, health behaviors, and health outcomes—the conceptual model (see Figure 1) for this study used only two domains (health behaviors and health outcomes). The health behavior domain consists of two subdomains: (a) process of medical care and (b) use of personal health service. The outcome variable is patient satisfaction with the health care system. Study results from the individual characteristics domain including age, mistrust, racism, education, health literacy, religious participation, health insurance, and access to care have been reported elsewhere (Moore et al., in press).

Conceptual model
Process of Medical Care
The first subdomain for health behaviors is process of medical care. Process of medical care was defined as the behavior of providers as they interact with patients in the delivery of medical care (Andersen, 2008). The Institute of Medicine publicly reported that African Americans have been subjected to inferior medical care when compared with Caucasians (Institute of Medicine, 2002). For example, African Americans have received unequal treatment in cardiac care, kidney transplants, and timely cancer care (Brawley & Wallington, 2009; Institute of Medicine, 2002). Thus, communication and how the patient is treated during these patient encounters are important concepts in the process of receiving medical care. African American men, who are mistreated and not trusting of health care providers, find it difficult to communicate (Allen, Kennedy, Wilson-Glover, & Gilligan, 2007; Gordon, Street, Sharf, & Souchek, 2006), are less active participants during interactions (Gordon et al., 2006), and find it challenging to follow recommended treatments (Forrester-Anderson, 2005). Trust is generated and maintained through repeated interactions in a continuing relationship and is a central component of patient–provider communications (Cobie-Smith, Thomas, & St. George, 2002; Jones, Steeves, & Williams, 2009; McKinstry, Ashcroft, Car, Freeman, & Sheikh, 2006; Pearson & Raeke, 2000).
The ability of the health care provider to elicit and respond to patient concerns is consistently and strongly related to patient satisfaction (Napoles et al., 2009). Good communication skills are essential for the delivery of quality care. For example, patient-centered communication styles (informative, supportive, respectful, partnership-building, empathic, and positive affect) may elicit more active patient participation (asking more questions), more information (for the provider and patient), trust, shared decision making, stronger intentions to adhere to recommendations, compliance, patient satisfaction, and better health outcomes (Johnson, Roter, Powe, & Cooper, 2004; Royak-Schaler et al., 2008; R. L. Street, O’Malley, Cooper, & Haidet, 2008).
On the other hand, provider-centered communication styles may breed passiveness, less information sharing, more mistrust, noncompliance, avoidance, negative effects, and poorer patient satisfaction and health outcomes (Arora, 2003; Siminoff, Graham, & Gordon, 2006; Williems, Maesschalck, Deveugele, Derese, & Maeseneer, 2004). Communication is a dyadic relationship with one person’s behavior influencing the other person’s behavior, and so certain conditions must be met for prostate cancer detection and treatment to occur. When people depend on each other, interdependence is created (Lewis, DeVellis, & Sleath, 2002).
Health care providers have a greater responsibility than patients to communicate effectively, particularly for older AAM who tend to have lower levels of education and health literacy (Friedman et al., 2009). However, the communication between AAM and the health care system continues to be poor, with these exchanges leading to poor health-related outcomes (Gordon et al., 2006; Napoles et al., 2009; Plumb & Brawer, 2006). African American men have also reported that health care providers did not genuinely demonstrate concern for their health and welfare and were unwilling to provide the information necessary for informed decision making (McFall, Hamm, & Volk, 2006; Ross, Kohler, Grimley, Green, & Anderson-Lewis, 2007; Woods, Montgomery, Belliard, Ramirez-Johnson, & Wilson, 2004).
The quality of the patient–provider interaction is one of the most important factors in determining patient satisfaction (Gordon et al., 2006; Jackson, 2005; Saha, Arbelaez, & Cooper, 2003;R. L. Street et al., 2008). The highest levels of patient satisfaction are reported when health care providers focus on the patient; spend time actively and patiently listening to questions, worries, or concerns; and project a genuine friendly, warm, caring, and respectful attitude (Napoles et al., 2009; Royak-Schaler et al., 2008; Saha et al., 2003). However, historically, AAM have had little interaction with health care providers and the health care system; therefore, cultural differences may lead to dissimilar expectations regarding patient and provider roles (Allen et al., 2007).
Use of Personal Services
The second subdomain for health behaviors is use of personal services. Use of personal health services was defined as the type, site, purpose, and coordination of health services received in an illness episode (Andersen, 1995). Habits of health care utilization and usual site of care were variables used to measure the use of personal health services. Through AAM’s upbringing and life experiences, some older men have a different value system that affects their intent to actually seek health care services and perception or evaluation of care received (Byrne, 2008).
African American men’s definition of health or what they believe is health may be different from the way Caucasian men define health. For example, some older AAM define healthy as physical well-being with the absence of physical ailment, mental and emotional well-being, economic stability, a sense of spirituality, and being able to take care of one’s own needs without assistance and physical dependence (Ravenell & Whitaker, 2006). This view of health is quite different from participating in health promotion and prevention activities or visiting a health care provider regularly (Ross et al., 2007). Where AAM receive care is important. Because of the lack of affordable health insurance and limited access, AAM often visited emergency department or public health centers, which are known to be associated with lower levels of trust and patient satisfaction (Fowler-Brown, Ashkin, Corbie-Smith, Thaker, & Pathman, 2006).
Having a consistent health care provider and participating in routine health checks have been associated with better communications and relationships with health care providers, continuity of care, reduced emergency department visits, and higher levels of patient satisfaction (Gerend & Pai, 2008; Napoles et al., 2009; Paez, Allen, Beach, Carson, & Cooper, 2009). Even though some AAM may have adequate health insurance, some frequently use emergency departments (Bade, Evertsen, Smiley, & Banerjee, 2008; Byrne, 2008). Although emergency departments focus on acute care, public health departments concentrate on preventive care; however, most public health clinics have programs that focus on women and children (Ross et al., 2007).
African American men are less trusting when they fail to receive adequate information and clear explanations and instructions during patient–provider interactions (Griffith et al., 2007; Song, Hamilton, & Moore, in press). Lack of information interferes with AAM’s ability to make informed decisions (McFall et al., 2006) and satisfaction with care (LaVeist, Nickerson, & Bowie, 2000). With the continuous controversy of prostate cancer screening and treatment, it becomes difficult for AAM to make informed screening and treatment decisions.
Patient satisfaction can be linked to efforts put forth by health care providers that allow patients to feel comfortable, respected, and meaningful (Song et al., in press). Verbal and nonverbal (e.g., body language, posture, and facial expressions) methods of communication are important in patient–provider interactions. Health care provider’s conscious and/or unconscious beliefs or stereotypes about AAM such as assuming they are not educated, poor communicators, and avoid the health care system without good justification can influence their interpretation of problems or symptoms (Plumb & Brawer, 2006; R. L. J. Street, Gordon, & Haidet, 2007). Such beliefs and stereotypes subsequently affect the patient’s attitudes, self-efficacy, trust, and behavioral intentions that influence health decisions, health behaviors, and patient satisfaction (Plumb & Brawer, 2006). Negative perceptions by health care providers can translate into lower levels of patient satisfaction (Freeman & Chu, 2005).
The purpose of this study was to explore whether a particular combination of health behaviors from the patient’s perspective influence patient satisfaction with the health care system among a sample of AAM in North Carolina with prostate cancer. The research question to be answered is as follows: Is patient satisfaction explained by health behaviors (patient–provider communications, communications, interpersonal treatment, habits of health care utilization, and usual site of care)? Results will expand current knowledge to better understand some of the complexities of factors associated with patient satisfaction particularly in AAM.
Materials and Method
A descriptive, correlation design was used to conduct a secondary data analysis of cross-sectional data consisting of a subset of 505 AAM in North Carolina newly diagnosed with prostate cancer. The data in this study were obtained from the North Carolina–Louisiana Prostate Cancer Project (PCaP), which is a multidisciplinary population-based case-only study designed to address racial differences in prostate cancer aggressiveness through a comprehensive evaluation of social-, individual-, and tumor-level characteristics (Schroeder et al., 2006). The overall goal of the PCaP study was to determine the most effective focus of public health efforts to reduce racial disparities and improve prostate cancer survival (Schroeder et al., 2006). These data were collected from September 2004 to November 2007.
Recruitment data, sample criteria, and data collection methods have been documented elsewhere (Schroeder et al., 2006); therefore, only a brief explanation will be provided. Participants in this study are 505 AAM age 40 to 79 years old living within 41 counties in North Carolina who have been diagnosed with localized and advanced prostate cancer after July 1, 2004, and ending in November 2007. Eligible participants in this study were able to complete the study interview in English, did not live in an institution, had no apparent cognitive impairment or psychosis, and were not under the influence of alcohol or severely medicated.
An introductory letter and brochure describing PCaP were sent to potential participants. A week later, an enrollment specialist called to confirm eligibility, explained the study, answered questions, solicited participation, and scheduled a home visit. The average time from diagnosis to study visit was 169.5 days with the median time of 138 days and ranged from 48 to 831 days (PCaP, 2009). The participation rate for eligible cases was 62%, defined as the number of enrolled plus the number that refused participation (505/505 + 310).
Registered nurses visited the homes of participants, explained the study, obtained Health Insurance Portability and Accountability Act authorization and written consent to conduct the questionnaire, collected anthropometric measurements, and collected samples needed for the other PCaP Consortium projects. Study visits took approximately 4 hours to complete, and participants received up to $75 for completing the study (Schroeder et al., 2006). This study was reviewed and approved by the institutional review board at the University of North Carolina at Chapel Hill.
Measures
Education and health literacy data will be used for descriptive purposes only. Education represents the highest grade or year of schooling completed. Health literacy was measured using the short form of the Rapid Estimate of Adult Literacy in Medicine, which consisted of 66 common medical terms (Davis et al., 1993). Participates with raw scores 0 to 18 read at 3rd grade level or below, 19 to 44 read between the 4th and 6th grade levels, 45 to 60 read between the 7th and 8th grade levels, and 61 to 66 read at the 9th grade level or above.
Patient–provider communication
This measure was defined as the degree to which the patient communicated to the health care provider from the patient’s perspective (Mishel et al., 2002). Patient-to-provider communication was measured with a 5-item scale that assessed the degree to which the patient communicated with his health care provider (Mishel et al., 2002; Mishel et al., 2003). Items for the scale had 5 responses in a Likert-type format ranging from 1 (a great deal) to 5 (nothing at all). All responses were reverse scored, with higher scores indicating greater degree of communication from the patient to the health care provider. Sample items include the following: How much did you tell your health care provider about your concerns? How much did you help with the planning of your treatment? This scale has been previously validated on AAM (Mishel et al., 2002), and Cronbach’s α for the current study was .75.
Communications
Communications, although similar to patient–provider communication, focuses on the health care provider’s behavior in communicating with the patient. The different direction in communication illustrates the interdependence relationship as to how one individual’s actions can influence another’s actions. Communication was measured with a 5-item scale that is a subscale from the Primary Care Assessment Survey that assessed health care provider-to-patient communication with reference to explanation of health problems and treatments, instructions about symptoms, answering of patient’s questions, and advice and assistance in making decisions about care (Safran et al., 1998). Items for the scale had 5 responses in a Likert-type format ranging from 1 (very poor) to 5 (very good), with higher scores indicating greater degree of health care provider to patient. Sample items include the following: Thoroughness of your health care provider’s questions about your symptoms and how you are feeling? Attention your health care provider give to what you have to say? This scale has been validated with AAM (Safran et al., 1998), and Cronbach’s α for the current study was .92.
Interpersonal treatment
Interpersonal treatment is related to the patient’s perception of the health care provider’s patience, friendliness, caring, respect, and time spent with the patient during interactions (Safran et al., 1998). Interpersonal treatment was measured with a 5-item scale that is a subscale from the Primary Care Assessment Survey that assessed how the patient perceived the provider focused on them. Items for the scale had 5 responses in a Likert-type format ranging from 1 (very poor) to 5 (very good), with higher scores indicating a greater degree of interpersonal treatment from the health care provider. Sample items include the following: Amount of time your health care provider spends with you? Health care provider’s respect for you? This scale has been validated with AAM (Safran et al., 1998), and Cronbach’s α for the current study was .93.
Habits of health care utilization
This measure was defined as the general likelihood of using health care services and measured with a 9-item scale (Facione, 1999). Items for the scale had 5 responses in a Likert-type format ranging from 1 (strongly disagree) to 5 (strongly agree). Items 2, 4, 5, and 6 were reverse scored, with higher scores indicating a greater degree of health promotion, early detection, and use when self-discovered symptoms are attributed to serious illness. Sample items include the following: I really have to be hurting before I go to the doctor. Going to the doctor regularly is a normal part of how I take care of myself. Cronbach’s α for the current study was .85.
Usual site of care
Usual site of care is a place where the individual usually goes when there is a medical problem. This was a categorical variable indicating doctor’s office/group practice, public health or community health clinic, hospital-based clinic, Veteran’s Administration, emergency department, urgent care, some other place, or no usual place. Knowing when and how a person chooses to seek heath care provides pertinent information about the value placed on health.
Patient satisfaction with the health care system
This measure was the outcome variable used to measure patient satisfaction. Patient satisfaction with health care system was measured with a 15-item scale that assessed satisfaction with wait time, time spent with physician, information received, and quality of care (Mishel et al., 2003). Items for the scale had 5 responses in a Likert-type format ranging from 1 (very dissatisfied) to 5 (very satisfied), with higher scores indicating greater degree of patient satisfaction. Sample items include the following: Satisfied with time waiting at the clinic or office to see the health care provider? Satisfied with quality of care received? Cronbach’s α for the current study was .90.
Statistical Analysis
Statistical software SAS 9.2 (SAS Institute, Cary, NC) was used to analyze the data for this study. Initially, the data file was screened for accuracy and missing data, and all negative item responses were reverse coded prior to computing scales. Bivariate regression models were computed for patient satisfaction in terms of each of the five independent health behavior variables. All models were assessed and interpreted for null hypothesis significance tests (p < .05) and variation (r2) in patient satisfaction represented by the β coefficient, parameter estimates, and confidence limits.
After analysis of the bivariate regression models, all independent variables were placed in a multiple regression equation to predict patient satisfaction. Assessment and interpretation of multiple R2, hypothesis tests, slopes, parameter estimates, and squared partial (pr2) correlation coefficients were conducted (Allison, 1999; Tabachnick & Fidell, 2001). Variance inflation factor (VIF) >10 was used as the criteria for assessing multicollinearity in this study (Cohen, Cohen, West, & Aiken, 2003; Katz, 1999).
Forward selection, backward elimination, and stepwise procedures were used to generate reduced multiple regression models in terms of health behaviors. The significance limit was set at p ≤ .05 as the criteria for a predictor to be considered for entry into the model using forward selection. For backward elimination, the significance limit was also set at p ≤ .05 as the criteria for predictors not to be removed from the model. So all predictors with a p > .05 were removed from the model. For stepwise regression, the significance limit was set at p ≤ .05 as the criteria for a predictor to be considered for entry into the model, and the significance limit was set at p > .05 for the criteria for predictors to be removed from the model. So all predictors with a p > .05 were removed from the model. The full model and the reduced models were compared using predicted sums of squares (PRESS). Assumptions were assessed for all regression models using residual analyses.
Results
The total sample in this study consisted of 505 AAM in North Carolina newly diagnosed with prostate cancer. Tumor aggressiveness was categorized into low, intermediate, or high (see Table 1). Of the participants in this study, 80% (n = 401) had low or intermediate tumor aggressiveness, whereas only 20% (n = 103) had high tumor aggressiveness. The participants in this study had a mean age of 61.1 years (8.1). Seventy-three percent (n = 368) of them had at least a high school education, and 60% had at least a 7th grade or higher health literacy level (see Table 2).
Cancer Aggressiveness
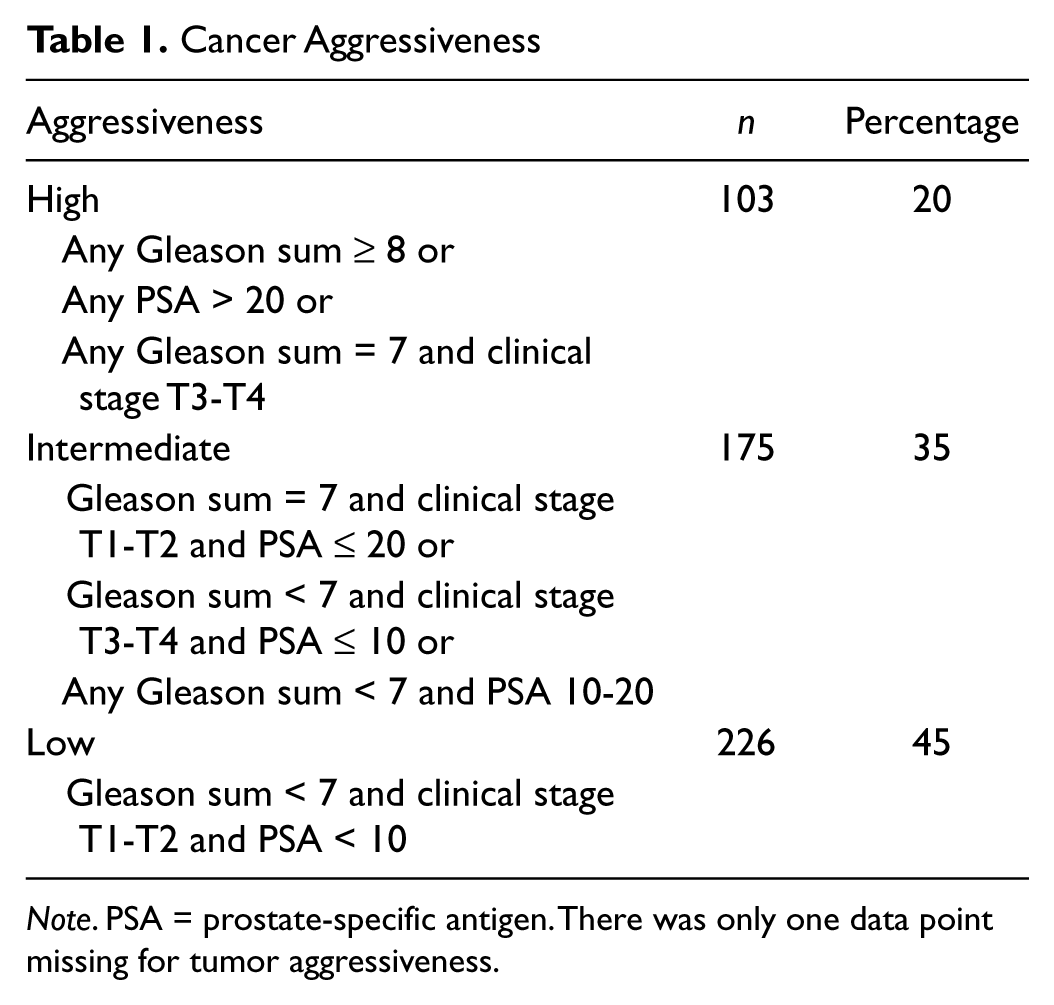
Note. PSA = prostate-specific antigen. There was only one data point missing for tumor aggressiveness.
Demographics

Table 3 describes the means, standard deviation, and p values associated with bivariate analyses conducted for continuous health behavior variables. Patient satisfaction depended significantly on each of the four continuous health behavior variables independently.
Health Behavior (Continuous) Variables

Note. P values are from bivariate analyses regressing patient satisfaction on each variable independently involving smaller samples due to missing data.
Table 4 contains results for the one categorical health behavior variable: usual site of care or where the AAM usually went when there was a medical problem. The majority (69%, n = 350) of the men received care at a doctor’s office or group practice, followed by the Veteran’s Administration (13%, n = 65). Usual site of care was not found to be significant in predicting patient satisfaction in this one-way ANOVA.
Usual Site of Care

Usual Site of Care global p value = .785 (from bivariate analysis using one-way ANOVA).
Patient satisfaction was regressed on all health behavior variables. Model 1 (n = 491) was significant (p ≤ .0001) with an R2 of .45, F value of 79.76, and a PRESS score of 12318; however, only patient-to-provider communication (p ≤ .0001), provider-to-patient communications (p = .002), and interpersonal treatment (p ≤ .0001) were associated with patient satisfaction. Habits of health care utilization (p = .10) and usual site of care were not significant. All health behavior variables had VIF values <3, so multicollinearity was not an issue.
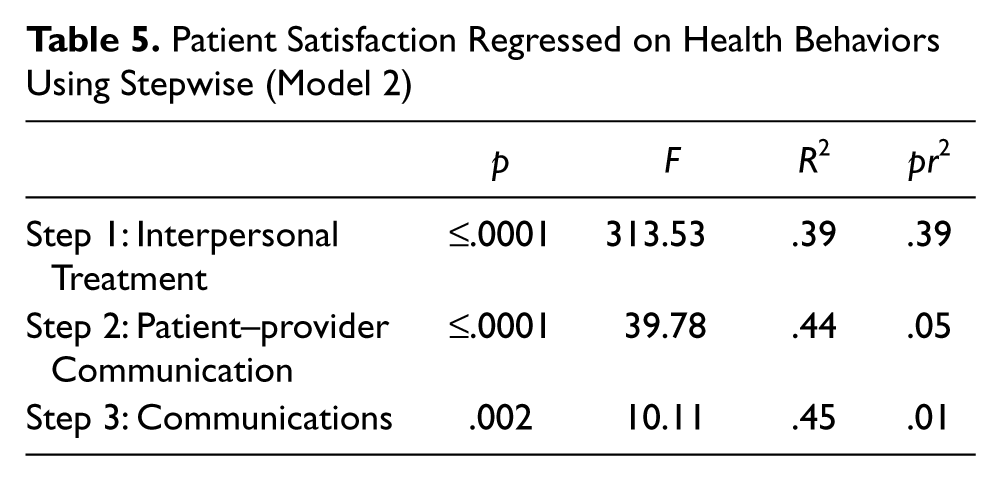
Forward selection, backward elimination, and stepwise procedures generated the same model; therefore, Model 2 is represented by stepwise procedure. Model 2 (n = 491) of Table 5 was significant (p ≤.0001) with an R2 of .45, F value of 131.78, and a PRESS score of 12298. First, interpersonal treatment (p ≤.0001) was entered into the model, followed by patient-to-provider communication (p ≤.0001), and finally provider-to-patient communications (p = .002). All three variables were positively associated with patient satisfaction. Habits of health care utilization (p = .10) and usual site of care were not significant and did not enter into the model. All health behavior variables had VIF values <3, so multicollinearity was not an issue. Outliers were identified in residual analyses, but conclusions were unchanged when these outliers were removed indicating those conclusions are not sensitive to the presence of outliers.
Patient Satisfaction Regressed on Health Behaviors Using Stepwise (Model 2)
Discussion
Individually, four (patient-to-provider communication, interpersonal treatment, provider-to-patient communications, and habits of health care utilization) out of the five health behavior variables significantly explained variability in patient satisfaction; however, habits of health care utilization became nonsignificant when entered into multiple regression models. Usual site of care did not reach significance.
Interpersonal treatment of AAM accounted for the majority (39% of the 45%) of the variability in patient satisfaction. The interpersonal treatment scale contained questions referring to the amount of time the health care provider spent with the patient and the health care provider’s patience with questions or worries, friendliness, warmth, caring, concern, and respect shown toward the patient. According to the AAM in this study, the more health care providers displayed or demonstrated these qualities during interactions the higher the level of patient satisfaction. Consistent with previous results, our study showed the interaction between the health care provider and patient is one of the most important factors in determining patient satisfaction (Gordon et al., 2006; Napoles et al., 2009; R. L. Street et al., 2008). Caring for and focusing on patient needs and concerns in a truly genuine manner is a necessary component for the delivery of culturally competent care by health care providers (Saha, Beach, & Cooper, 2008). In addition, adequate communication from health care providers must coincide with good interpersonal treatment.
Second, increases in communication scores (provider-to-patient and patient-to-provider communication) was associated with increases in patient satisfaction. Although both communication variables were positively associated with patient satisfaction, the degree to which the patient communicated with the health care provider accounted for more of the variability in patient satisfaction than the degree to which the health care provider communicated with the patient. These results were consistent with another study of multiethnic health care providers (41% Asian, 28% African American, and 31% Caucasian) and multiethnic patients (39% African American, 11% Hispanic, and 50% Caucasian) that reported greater satisfaction occurred when providers perceived patients to be better communicators (R. L. J. Street et al., 2007).
Interestingly, even though the percentage of variability of patient satisfaction for provider-to-patient communication was small, this association was still significant. This was consistent with other studies that have shown that health care providers that communicate effectively with patients tend to foster more active patient participation, better exchanges of information, more engagement in shared decision making, better satisfaction, and improved adherence to treatments regimens (Song et al., 2011; R. L. Street et al., 2008).
Communicating is an interdependent process, because one person’s communication style affects the other person’s communication style (Lewis et al., 2002). Communication does not take place in a vacuum, and in health care, the patient and health care provider must exchange words, gestures, or expressions. The patient communicates to the health care provider, and the health care provider communicates with patient representing a reciprocal relationship. Nevertheless, the onus is on health care providers and workers within the health care system to demonstrate health behaviors that apply culturally competent principles to improve patient health care experiences. Knowing important variables that are predictors of patient satisfaction provides useful information for developing interventions that positively affect patient satisfaction.
We expected to find that patterns of health care utilization and usual site for receiving health care would be predictors of patient satisfaction for these men would be similar to that reported previously; however, this was not the case (Allen et al., 2007; Griffith et al., 2007). One plausible explanation could be that the majority of AAM in this study primarily received their care in physician offices and not in emergency departments or public health clinics where low patient satisfaction has been consistently reported (Fowler-Brown et al., 2006). In addition, the majority of these men also had fairly higher (7th grade or higher) levels of health literacy.
Although patient satisfaction has received an increased amount of attention recently, this study examined an understudied area of AAM’s perception of patient satisfaction with the health care system when treated for prostate cancer (Jayadevappa, Chhatre, Wein, & Malkowicz, 2009). This study also extended what was known of patient satisfaction as a predictor variable associated with treatment, decision making, quality of life, or survivorship outcomes to include patient satisfaction as the outcome from experiences with health care services use.
Implications for Clinical Practice
With the persistent controversy surrounding prostate cancer screening and treatment, it is paramount that health care providers provide a clinical environment where AAM feel comfortable, safe, and respected to allow positive interpersonal treatment and patient-centered communications in order to assist AAM in making informed decisions as recommended by the American Cancer Society (Brooks, Wolf, Smith, Dash, & Guessous, 2010). African American men need to have all the necessary information needed to make an informed decision, and the information about screening, treatment, and survivorship care should be clear and culturally relevant. Cultural competency training should be mandatory for health care providers, implemented early in their medical education, and continually assessed for compliance. In addition, health care providers should receive education and training needed to demonstrate good communication and bedside mannerism when interacting with all patients.
Limitations
This study was limited by cross-sectional data and therefore causality cannot be assumed. Furthermore, the findings may not be generalized beyond the values and patient characteristics in this data set (Shadish, Cook, & Campbell, 2002). In particular, the majority of the AAM in this study were fairly educated, had higher levels of health literacy, and used physician office for health care, which does not represent the majority of older AAM. Another limitation was that patterns of communication were limited to self-report and likely affected by memory and recall. Nevertheless, the patient is the best source for evaluating health care services, because they are on the receiving end of the care delivered. Finally, this study did not consider interactions between the predicted variables during the analyses; however, multicollinearity was not an issue with all variance inflation factors (VIF) ≤ 3.
Future Research
Research should compare the results of this study with other AAM in northern parts of United States to determine if similar variables are significant in accounting for patient satisfaction. Comparing AAM in northern geographic areas has the potential to provide insight and additional information about differences or similarities within multiple health care systems. In addition, future studies should also consider possible interactions between variables. Components of patient-centered care should be further studied to assess the relationship with patient satisfaction, health care utilization, psychosocial factors, and other health outcomes.
Future studies should also conduct prospective studies to directly measure communication and interactions in addition to measuring patient’s perspectives. Intervention studies, focused on enhancing patient–provider communication (Mishel et al., 2002), should consider the ways in which health care providers interact and communicate with patients and how patients communicate with health care providers (Campbell et al., 2007; Hamilton, Agarwal, Song, Moore, & Best, 2011). Health care providers need to be educated and taught how to communicate and interact with patients and their family members in a way that engenders cultural competent care. The synergy of good interpersonal treatment and communication from health care providers produce positive patient experiences or patient satisfaction. If consistent, health care environments can move toward reversing mistrust and overcoming known barriers for AAM in seeking health care services. Ultimately, the goals are to increase regular care, early detection and treatment for prostate cancer, survivorship, and subsequently reduce the racial disparity in prostate cancer outcomes for AAM.
Conclusion
Since interpersonal treatment focuses on the patient and was demonstrated to be the strongest health behavior predicting patient satisfaction, it is noteworthy to consider the emphasis that should be placed on how health care providers treat AAM during their interactions with them. Adequate communications between the health care provider and the patient is needed to address relevant patient needs and concerns during all medical encounters to improve patient satisfaction. Moreover, embracing patient-centered care also may produce the capacity to cultivate more trusting relationships. When health care providers direct their attention to patients and their concerns in a respectful manner, the potential exists to create a comfortable atmosphere for AAM that may promote communication and patient satisfaction.
Footnotes
Acknowledgements
The North Carolina- Louisiana Prostate Cancer Project (PCaP) is carried out as a collaborative study supported by the Department of Defense contract DAMD 17-03-2-0052. The authors thank the staff, advisory committees, and research subjects participating in the PCaP study for their important contributions. This study was reviewed and approved by the Institutional Review Board at the University of North Carolina at Chapel Hill, Study#: 10-0133.
Author’s Note
Disclaimer: “The views expressed in this manuscript are those of the authors and do not reflect the official policy or position of the Department of the Army, Department of Defense, or the U.S. Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.