
Abstract
The purpose of this study was to identify and describe the process of HIV disclosure for rural African American men—a population disproportionately affected by HIV/AIDS. Forty men were interviewed about their experience of making an HIV disclosure. Grounded theory methodology guided data collection and analysis. The core category or variable that emerged from the data was a process—Making Decisions: The Process of HIV Disclosure. Five categories accounted for variations in disclosures: (a) beliefs and knowledge about HIV/AIDS, (b) influencing factors, (c) disclosure decisions, (d) disclosure efficacy, and (e) outcomes of disclosure. Most of the men had disclosed to others; however, the disclosures were selective, and the decisions were iterative. The majority of the men did not disclose their diagnosis for several months to several years. The findings provide a framework of the many factors related to HIV disclosure that can guide health care providers in counseling persons living with HIV/AIDS in making disclosure decisions.
People who receive a negative health diagnosis face a number of challenges and decisions about the information and how to manage changes in their lives. One decision that people make is about sharing the diagnosis with others or disclosure (Greene, 2009). Information about one’s health is considered to be private and should only be shared by the affected person. When there are no observable signs of an illness or disease, such as in HIV/AIDS, disclosure decisions are driven by personal attitudes, beliefs, knowledge, and comfort. Disclosure of being diagnosed with HIV presents unique and complex issues for persons living with HIV and AIDS (PLWHA) to consider. The benefits of disclosure include emotional support and decreased stress (Kalichman, Dimarco, Austin, Luke, & Difonzo, 2003), whereas risks of disclosure include rejection, discrimination, and associated stigma (Levy et al., 1999; Sowell, Seals, Phillips, & Julious, 2003). Two changes in the epidemic over the past 30 years have also influenced disclosure decisions and recommendations. Improved treatment has resulted in longer, healthier lives for PLWHA as HIV infection has become a chronic disease (Vetter & Donnelly, 2006). Also, the epidemiological profile of PLWHA has changed (Center for Disease Control and Prevention, 2011). Early in the epidemic, AIDS was perceived to mainly affect gay White men in urban areas. Currently, HIV infection is increasing fastest in the Deep South (Pence et al., 2007), where the epidemic has shifted to racial and ethnic minorities, the poor, and people living in rural areas. African American (AA) men are disproportionately affected by HIV/AIDS and have the highest rate of new cases of HIV infection in the United States. This population faces unique challenges in dealing with their diagnosis, and disclosure to others is a paramount issue for them.
A number of influential studies have been conducted on HIV disclosure, many conducted in urban areas and on women or gay men (Obermeyer, Baijai, & Pegurri, 2010). There is not one set of factors that influence or determine how HIV disclosure decisions are made and enacted. Nor is there one model that clearly captures the process of HIV disclosure and presents the sequence of decision making. None of the models have been developed with a focus on AA men in the South to address their unique issues with HIV disclosure. There is a critical need to focus research on this underserved group because of the growing epidemic in AA men. The purpose of this study was to identify and describe the process of HIV disclosure for rural Southern AA men.
Background
HIV disclosure is an ongoing social and psychological process of communication about private health information. There have been a number of studies on disclosure in the United States and other countries. Obermeyer et al. (2011) conducted a review of the literature on HIV disclosure in adults. The reviewed studies indicate that the majority of PLWHA eventually disclose their HIV status to someone. Women appear to be more likely to disclose than men. Women and relatives are more likely to be disclosure recipients than men and friends. Some studies suggest that racial and ethnic minorities have the most concern about being stigmatized if they disclose. This fear of stigma and discrimination decreases the likelihood of disclosure. A critical factor in disclosure decisions is the expectation of support from others. The information disclosed varies depending on the targeted recipient.
A wide variation in the time from diagnosis of HIV infection to disclosure to others has been reported in the literature (Serovich, 2001). Early in the epidemic, a disease progression theory predicted that PLWHA would be more likely to disclose their diagnosis as their disease progressed and they became ill (Babcock, 1998; Kalichman, 1995). Typically, there were observable signs or symptoms of the disease progression such as weight loss or swollen lymph nodes. Rates of disclosure to family and friends have been reported to be higher in PLWHA with symptomatic disease than those who are asymptomatic. Today, with better treatment for HIV infection, individuals do not exhibit a standard of declining health and are living longer, often asymptomatic lives. The consequences theory of HIV disclosure suggests that the costs and benefits of disclosure are assessed prior to disclosure to family and friends (Derlega, Lovejoy, & Winstead, 1998; Serovich & Mosack, 2003). There are possible negative physical, emotional, and social consequences of an HIV disclosure. Additionally, an HIV disclosure may lead to private information about sexual and drug-using behaviors being shared. Disclosure also has positive consequences, including acquisition of resources, emotional support, and decreasing stress. PLWHA must believe or perceive that the benefits or positive consequences of a disclosure outweigh the costs or negative ones. In a study comparing these two theories with 138 HIV-positive gay men, structural equation modeling was used to analyze each model (Serovich, 2001). The disease progression model was not supported, whereas the consequences theory was well supported.
There is not one universal disclosure process that is shared by all PLWHA across all social contexts (Arnold, Rice, Flannery, & Rotheram-Borus, 2008; Black & Miles, 2002). However, decisions about when, to whom, and how to disclose are partial and gradually increase over time rather than being a onetime full disclosure to everyone (Obermeyer et al., 2011). Three disclosure pathways are possible: (a) disclosure to everyone, (b) disclosure to selected people, and (c) nondisclosure. Disclosure to everyone and total nondisclosure are the exceptions. Both pathways have a relatively simple coping style as the problem solving skills are consistent and not complicated. Disclosure to selected people has been reported to be the most common and the most complex disclosure pathway (Arnold et al., 2008; Black & Miles, 2002). The selective disclosure pathway requires that decisions be made about information to share every time a disclosure is made, and there are no simple answers that fit every recipient of a disclosure.
Models of HIV disclosure have been developed for different factors and aspects of the process. Arnold et al. (2008) described social identities and role relationships as being the main considerations in how PLWHA developed decision rules that inform and guide disclosure behaviors. Their model was developed from reviewing the literature on HIV disclosure in adults focusing on the context of their relationships.
In Black and Miles’s (2002) model of disclosure for AA women, selective disclosures were made by calculating the risks and benefits of telling specific people. Stigma was the major risk of disclosure, and receiving support was the major benefit of disclosing. Data from a qualitative study with 48 women informed the development of the model. Derlega, Winstead, Greene, Serovich, and Elwood (2004) developed a model of HIV disclosure decision making indicating that cultural attitudes and contextual factors influence PLWHA’ reasons for disclosure and nondisclosure. Male and female participants considered the benefits and costs to themselves and others in making disclosure decisions. In developing the model, two questionnaires were completed for disclosure to a friend, an intimate partner, and parents.
The model of HIV disclosure developed by Bairan et al. (2007) contends that social relationships (sexual or nonsexual) determine the likelihood of PLWHA disclosing to specific people. Disclosure was viewed as a continuum from nondisclosure to full disclosure to people in certain categories. Findings indicated that fear and stigma were also major factors that influenced disclosure decisions in all types of relationships.
In summary, disclosure of an HIV diagnosis is difficult and complex for all infected individuals. The process of disclosure varies across settings and populations and depends on evolving motivations and consequences of PLWHA. This study will explore the process and context of HIV disclosure to sexual partners and family members, specifically for rural AA men.
Method
Design
Grounded theory, a qualitative research method, guided the data collection and analysis in the study. Grounded theory is a method of inquiry used to study social psychological processes in order to understand people’s behavior (Munhall, 2001). The goal of grounded theory is to identify a framework or theory that is able to explain specific human behavior in context (Strauss, 1987). This framework or theory is developed through inductive analysis of the data. The study was approved by the institutional review board at the researchers’ academic institution and at the recruitment sites.
Sample and setting
Purposeful sampling was used in selecting 40 AA men living in rural Alabama (Polit & Beck, 2012). PLWHA were recruited who were likely to have made decisions about disclosing their HIV status to others. Inclusion criteria for participation were as follows: (a) a confirmed diagnosis of HIV, (b) ability to speak English, (c) residence in a rural area, and (d) being between 18 and 49 years of age.
Procedure
PLWHA who met the study criteria were recruited from AIDS service organizations (ASOs) and clinics serving rural populations by staff, peer mentors, and recruitment flyers. Interested potential participants contacted the researcher directly if they obtained the information or by a contact number from the flyers, the agency staff, or peer mentors. Alternatively, agency staff and peer mentors recruited potential participants and contacted the researcher to arrange an interview if inclusion criteria were met. Individual interviews were scheduled at a location, date, and time preferred by participants. The majority of the interviews were conducted in a private office at the collaborating ASO or a clinic. Interviews were conducted by a graduate research assistant (GRA) using a semistructured interview guide. Prior to the first interview, the GRA was trained by conducting a mock interview with a person who met the study inclusion criteria but who was not included in the actual study. The mock interview was conducted in a room with a one-way mirror and observed by the principal investigator (PI). The PI then reviewed the transcribed interview with the GRA and made suggestions for prompts, responses, and strategies to enhance participant’s answers to the interview questions. Informed consent was obtained prior to data collection, including permission to audiotape the interview.
Data collection
A personal information form was used to collect sociodemographic data and a brief medical history. Sociodemographic variables, including age, education, living arrangement, and annual income, were measured to describe the sample. The medical history questions addressed length of time since diagnosis, medications, where care was received, and whether or not the participants were symptomatic. During an audiotaped interview, participants were asked questions about how they made decisions about disclosing their HIV status and why. Communication Privacy Management (CPM; Petronio, 2002) provided a framework for content areas in the interview guide. CPM is a practical theory that contextualizes how people make decisions to conceal or reveal private information to others or regulate their privacy. According to CPM, privacy rules are developed to protect private information depending on one’s culture, gender, motivations, context, and risk–benefit ratio. These sensitizing concepts provided tentative tools to begin studying the process that was defined in the data (Charmaz, 2006). Participants’ responses to all questions were open-ended and unrestricted. Each interview lasted approximately 1½ hours. Participants were compensated for their participation and travel expenses.
Data analysis
Descriptive statistics were used to describe the sample. Each interview was transcribed verbatim for analysis. Initially, line-by-line open coding was conducted to identify relevant concepts using the constant comparative method (Holton, 2007). Related codes were clustered to form categories. Axial coding then was used to determine the relationships of the categories. Theoretical coding was conducted to integrate the codes and determine a temporal ordering in the process of disclosure. Finally, the core category that captured all categories involved in the process was identified (Holton, 2007). A computer software program, NVivo, was used for data management and to assist with data analysis. Exemplary quotes were identified for each theme. The researchers and the graduate student met to discuss the identified codes and categories throughout the analysis process.
Results
Sample
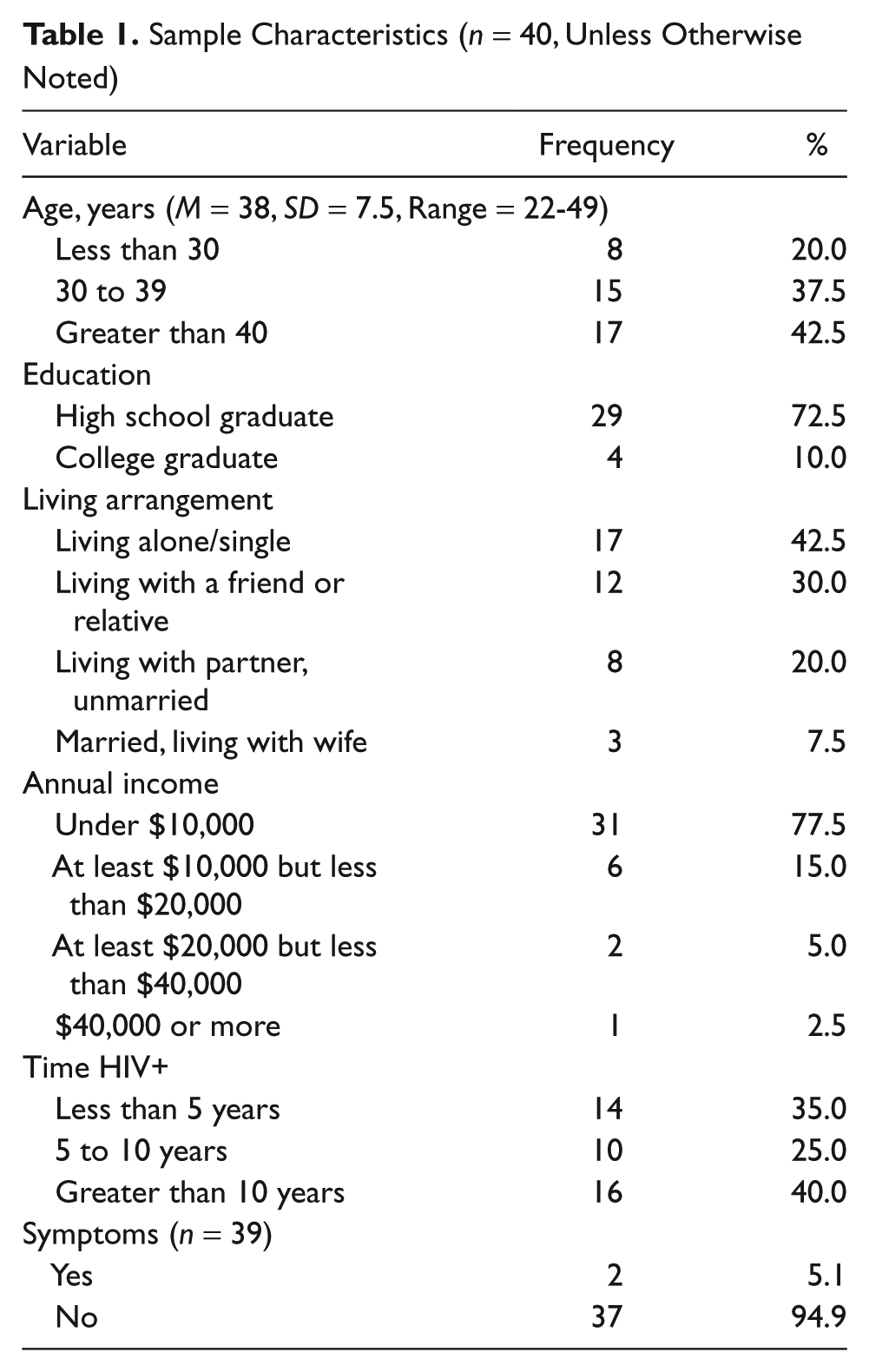
The participants in the study were between the ages of 22 to 49 years, with a mean age of 38 years (SD = 7.5 years). The majority of participants (29, 72.5%) were high school graduates and had an income of less than $10,000 annually (31, 77.5%). Also, the majority (30, 75%) of them were unemployed. The most frequent living arrangement was living alone (17, 42.5%), followed by living with a friend or relative (12, 30%) and living with a partner (8, 20%). Only three men in the study were married and living with their wife. The length of time participants had known that they were HIV positive was fairly evenly distributed with the greatest percentage in the greater than 10 years category (16, 40%), followed by the less than 5 years category (14, 35%). Only two participants were experiencing HIV-related symptoms (Table 1).
Sample Characteristics (n = 40, Unless Otherwise Noted)
A Model of the Process of HIV Disclosure
Analysis of the data revealed five categories that accounted for variations in HIV disclosures for the men: (a) beliefs and knowledge about HIV, (b) influencing factors, (c) disclosure decisions, (d) disclosure efficacy, and (e) outcomes of disclosure. A core category or variable was identified—Making Decisions: The Process of HIV Disclosure—which integrated the categories and provided a temporal perspective of making disclosures (Strauss, 1987). See Figure 1. For most of the participants, there was a period after being diagnosed with HIV that they needed to figure out what a diagnosis of HIV infection meant and how it would change their lives. This was a time when prior beliefs and knowledge were considered and information was sought. Before making a disclosure, there were a number of decisions to be made about disclosing, and there were also factors that influenced how those decisions were made. The influencing factors included social, cultural, and environmental factors, as well as the anticipated response from recipients. Disclosure decisions were made for targeted potential recipients. These decisions provided a framework that guided future disclosure decisions. For most of the participants, disclosure was iterative and selective, so the initial decisions were not to disclose to everyone or no one. Before a disclosure was enacted, disclosure self-efficacy, or the belief that they could communicate the information to others, determined the likelihood of a disclosure. Once a disclosure was made, the outcomes or consequences influenced future disclosure decisions. Two participants described how they made disclosure decisions as follows:
It is a process. And that process is ongoing. It’s never a right time. It’s an individual in a relationship personal one-on-one thing. So, there’s a lot of components that goes on and into that but the main thing is, you want to hope that it’s the safe time, it’s comfortable and safe and it’s the environment and the cultural and the tone is the right. But you never know. So, I pick and choose. I don’t tell everybody because I don’t think that’s a wise decision for anyone unless you just, some kind of super star like Magic Johnson.

Making decisions: The process of HIV disclosure
Each identified category in the process of disclosure will be described followed by an exemplary quote from the category.
Beliefs and Knowledge About HIV/AIDS
Many of the men talked about their lack of understanding of HIV disease when diagnosed. Initially, many of them thought that they would die soon. They talked about other reactions, including fear of how their lives would change, being embarrassed, depressed, devastated, and concerned about how others would react to them. Most of the participants did not personally know a PLWHA when diagnosed. This was a time when their prior beliefs and knowledge about HIV/AIDS were considered, plus additional knowledge was sought. For most of the men, prior knowledge was about HIV/AIDS being a fatal disease that usually affected homosexuals. Some spoke about going numb, being in shock or denial initially. Information was obtained from health care providers (HCPs), ASO staff, and other PLWHA. Participants talked about reading pamphlets and fact sheets from the health department, clinics, and ASOs to learn more about HIV/AIDS.
I just thought it was death sentence. I was just wondering how long do I have to live.
Disclosure Decisions
There were five decisions that participants considered for each disclosure: (a) who, (b) why, (c) when, (d) where, and (e) the disclosure message.
Who
As the participants considered sharing their HIV status, most of them identified recipients who they wanted to tell about their diagnosis as well as recipients who needed to be told. Both of these recipient targets were based on prior relationships or the role of the recipient in the men’s lives. Family members were the most likely recipients whom the participants wanted to tell. Mothers were the most likely to be told and the most likely to be the first recipient. Siblings were the second most frequent recipients of a disclosure, and sisters were more likely to be told than brothers. Friends were not likely recipients to be chosen unless they were very close to the participant or were a PLWHA. Sexual partners were identified as recipients who needed to be told by all the participants. However, the participants did not always disclose to sexual partners, especially casual ones. The men did say that they used protection (condoms) if they did not disclose. All the participants who were married or in committed relationships had disclosed to their partners immediately. Most of the participants with children had not told their partners, although they talked about wanting to tell them in the future. Two participants talked about telling their families as follows:
My family, because it’s someone you trust who won’t tell everybody, so I told my mom and my brother and my aunt because she had to take me back and forth to the doctor. But at the same time, some of your family members, you can’t tell them either. It took me a while to decide because I didn’t know how they would react to it and I know I, I decided right away to tell my mom . . . because, you know, she’s my mom and I love her, my mother and my father, those are the main people I depend on so I knew I had to tell them.
The men not only considered their relationships with targeted recipients of a disclosure but also with the recipient’s personal characteristics. The most important characteristic of a recipient was that they needed to be trustworthy. Trustworthy in the sense that they would not share the information with others and that they would not reject the men. Also, the men talked about feeling comfortable with the recipient. Therefore, it was the quality of their prior relationships with people that guided them in choosing recipients of an HIV disclosure.
They are more trustworthy. I felt like I could talk and it wasn’t going to go anywhere.
Why
For some of the participants there was a catalyst or event that precipitated a disclosure. The most likely catalyst was a health problem, either they were hospitalized or became symptomatic. Two of the participants had been told that they only had a few months to live. The subcategories of reasons why participants disclosed were (a) to relieve stress, (b) the need to tell specific people, (c) to help others, and (d) to receive support. The need to relieve stress was related to keeping their diagnosis a secret and feeling the need for a confidant. Besides sexual partners, the men thought that family members with whom they lived or were in a close relationship needed to know. The men wanted certain family members to be forewarned about their diagnosis so that they would understand the importance of their health care and potential problems. Making a disclosure to help others was most often to educate others at risk of infection to practice prevention. The men talked about needing support to deal with having HIV/AIDS.
The participants talked about reasons for not disclosing. Five subcategories for not disclosing were the following: (a) fear of negative reactions or stigma, (b) fear of recipients telling others, (c) recipients not needing to know, (d) not being ready, and (e) to prevent burdening others. The men’s biggest fear was of being rejected by others if they knew about their disease. Participants were aware of the stigma associated with HIV/AIDS, and many thought it was worse in rural areas because people were less educated about the disease. The fear of recipients telling others was also related to living in a rural area where many people know each other. The men had strong beliefs about others not needing to know their diagnosis unless they were at risk of infection or involved in their lives. Participants talked about the importance of being comfortable with their disease and the intended recipient before a disclosure was made. Finally, they worried about the knowledge of their infection being a worry or burden for the recipients, especially parents.
I keep my status confidential, not because I’m embarrassed. Not because I’m ashamed. I keep it that way because people can destroy you, you know. Cause some people are still ignorant to this. . . . I mean real ignorant. So, I mean the real reason, rejection is the biggest thing.
When
The participants reported a wide range of time from the time of diagnosis of HIV infection to the first disclosure. The participants spoke candidly about their reasons for not disclosing early after diagnosis, including being in denial, fear of stigma or negative reactions, and needing to accept the diagnosis themselves. Many could not identify a specific time period but said that it took several years. A few disclosed within the first week, but the majority said that the time frame was from months to many years. The men talked about the importance of getting comfortable with their diagnosis prior to telling other people. One participant said that he had disclosed to his family after a year or two but had waited 3 years to tell any friends. When asked why he waited, he commented,
Because I was still trying to get over the shock, that is why. I was trying to understand what was going on with me first.
Where
Disclosures were made in private locations. The most likely place for disclosing was in a home. Typically, the disclosure was to only one person at a time, but several participants had called their immediate family together and told them as a group. Two participants had not lived close to family members and had told them on the telephone. The men talked about the importance of the environment being private and safe. Several participants had been diagnosed in a hospital and were very ill, so they told their families there. These disclosures were not planned but necessitated by the situation. Also, several participants had been in prison and told visitors when they came. Alabama segregates all PLWHA at one location, Limestone, so it is known that prisoners there have HIV/AIDS. Again, these disclosures were necessitated by the situation.
It has always been in a personal environment. It has to be a safe environment that is comfortable.
Message
When the participants disclosed to others, they frequently tried to educate recipients about the disease, especially transmission and prevention. If the recipient was at risk of infection because of high-risk behaviors, the participants encouraged them to get tested. Most of them stated that educating others was an essential part of a disclosure. Therefore, the men talked about giving others educational reading materials such as booklets or pamphlets. Some participants told recipients how long they had been infected and how they were infected, but many did not. A number of participants talked about not being sure how long they had been infected. They tried to reassure the recipients that they were doing well and would continue to be well as long as they took their medications. Although most of the participants told the recipients not to tell anyone, the ones who did not felt that the recipients could be trusted not to share the information. One participant described his message about asking recipients not to share the information with others as follows:
I just tell them to keep my secret, our secret right with us. I don’t want anyone else to know. So far it’s been pretty good.
Factors Influencing Disclosure Decisions
There were four factors that influenced the way in which the men made disclosure decisions: (a) anticipated response, (b) personal characteristics, (c) the environment, and (d) barriers and facilitators. The men weighed the benefits and risks of disclosure for themselves as well as the recipients. The men also talked about the responses that they anticipated receiving from recipients. Personal characteristics or sociodemographics refer to how the men identified themselves. The environment or context of where participants lived also influenced their disclosure decisions. There were factors that made it easier or that presented barriers to them disclosing.
Anticipated response—Risk versus benefit
The men expressed uncertainty about how the recipients would respond, even people to whom they were close. The benefits and risks of disclosure are related to why the decision was made to disclose or to not disclose to targeted recipients. These factors were considered together to determine which was greater. For example, participants told others to relieve their stress and to receive support, which are benefits and led to disclosure. The fears of stigma and negative reactions, concern about others telling the information, and burdening others were risks and led to nondisclosure. Therefore, the men made disclosure decisions to specific recipients based on a case-by-case assessment of whether the benefits or risks were higher. A strategy to help some of the men anticipate a recipient’s response to a disclosure was to listen to conversations about other PLWHA. Some even would probe for information on how potential recipients viewed PLWHA or their knowledge and beliefs about HIV/AIDS. Exemplary statements include the following:
What makes it hard is, is not knowing how they might respond. Just projecting how, I think in my mind how they might respond to me. And, the fear of being rejected, would probably prevent me from doing it. You need to just tell the ones you know would support you. Don’t tell the ones who are going to bring drama or distress to you. I listen real closely to the people that I hang around and I deal with, their conversations speak for themselves, that’s how you have to pick and choose who you tell; because you can’t just come out and tell everyone about your HIV.
Sociodemographics
Participants talked about what it meant to be an AA man and have HIV/AIDS. Some of the men did not think that being AA and having HIV/AIDS resulted in differences in how people viewed or treated them. However, many of the gay men feared being stigmatized for being infected with HIV. They referred to people thinking that they were “junkies” or on the down-low.
You know, in the Black community, being gay is taboo . . . you (already) shunned and ostracized. It’s hard being an African American man anyway, and then being an African American gay man, and then being African American gay man who’s HIV positive. It is hard.
Environment/context
The men were asked if living in a rural area or a small town had influenced their disclosure decisions. Most of them stated that they had chosen not to disclose being a PLWHA because most people know each other in a small town. They also thought that there was more stigma associated with HIV/AIDS because people were not as educated about the disease. All the men had access to health care and were pleased with the care and the providers.
I would not want nobody to know here because once it gets out, it is all over town. Down here everybody is uneducated about HIV and AIDS, so they’ll treat you different.
Barriers/facilitators
When the men talked about recipients, several mentioned people that they had not told but hoped to tell in the future. The major barrier to intended disclosures was distance from the recipient. Several men identified people to whom they wanted to disclose, but the people lived in other states or cities, and they preferred to tell recipients face to face. Similarly, proximity to a recipient made it easier and more convenient to disclose. Most of the men had a number of family members living nearby and that facilitated sharing the information among them as they were the primary support system. Other facilitators for some of the men were support groups or PLWHA from the ASOs, who could share experiences and provide guidance. HCPs and staff from the ASOs also encouraged some of the men to disclose, especially to their families.
I told all my family that were in the area, except the sister who was out of town.
Disclosure Efficacy
After HIV disclosure decisions are made, PLWHA must perceive that they are able to enact the disclosure or communicate the information to recipients (Bandura, 1997). Several participants talked about wanting to make disclosures that had not been made. These men talked about disclosing in the future or when they were ready, which indicated that they did not possess disclosure efficacy.
I’ll talk to them about it one day. Right now, I’m just not ready to tell a lot of people. It’s like death. You are never ready for it.
Outcomes
Participants described how recipients reacted to the disclosure initially as well as how they responded over time. These responses influenced future disclosure decisions. The men were very concerned about the initial reaction and talked about worrying about how people would react and possibly reject them. Many of the recipients had not anticipated the disclosure and were shocked, sad, and even “hurt.” Most of the family members immediately offered support. Reactions from sexual partners varied and included fear of being infected and trying to determine their risk. Some of the sexual partners ended the relationship, especially if it was not a long-term one.
Over time, most of the family members, especially parents and siblings, were supportive. Family recipients often reminded participants to take their medications, called or visited them, and provided emotional support. Nonsupportive responses were most likely exhibited by cousins, aunts, and uncles. These behaviors included treating the participants differently when they visited and telling others about their infection. Some friends also had told others and no longer socialized with the participants.
I thought they (my family) was going to be more supportive, but they wasn’t.
It’s the reception that I get afterward, you know, because there’s always this fear of rejection, but then once you tell, a lot of people are so supportive until, you know, you go, “Wow. That wasn’t as bad as I thought it was gonna be.” So, it makes it easier to do the next time.
Discussion
Our results extend findings reported from other research and models on HIV disclosure by integrating them into a global process of decision making. The model explicates the myriad considerations involved in making HIV disclosures in rural AA men. There are clearly many dimensions and meanings of disclosure. Similar to other disclosure studies, the majority of the men had disclosed their HIV status to someone (Obermeyer et al., 2011). Before a disclosure was made, most of them took time to learn about HIV/AIDS and make decisions about disclosing to targeted recipients. Consistent with other studies, family members were the most likely recipients of disclosure. Also consistent with other studies, mothers were not only the most likely recipient of a disclosure but also most likely to be the first recipient (Greene & Faulkner, 2002; Serovich, Esbenson, & Mason, 2005; Stemple, Mouton, Bachetti, & Moss, 1995). These patterns of disclosure emphasize the important role of family for AAs in the South. The men viewed family members as people who needed to know their diagnosis so that they would understand how their lives had changed or would change in the future as their disease progressed. Family members also were the most likely source of support for the men. The most trusted recipients of a disclosure were family members, and the information was guarded by the family. Many of the men talked about strong family support as being the strength for AAs. This finding is inconsistent with research that reported that gay men do not consider their biological family as a primary source of support and are more likely to make an HIV disclosure to friends and partners (Bor, Plessis, & Russell, 2004).
As reported in other studies (Bairan et al., 2007; Kalichman & Nachimson, 1999; Parsons et al., 2005), the participants reported inconsistent disclosure to sexual partners, which is a concern because of the implications for transmission of HIV. In view of these findings, it is critical that PLWHA be educated on the importance of safer sexual practices to prevent transmission as well as adherence to medications to maintain a low viral load, which decreases the likelihood of transmission (Bartlett, Gallant, & Pham, 2009).
The delay in HIV disclosure is a concern for HCPs as the time after diagnosis is recognized as a high-stress time. This is a time when emotional support is needed to deal with the news of having a chronic disease that will require treatment and monitoring throughout one’s life. Rather than seeking support, most of the men feared the consequences of disclosure after their diagnosis. The delay in disclosure of months to years after diagnosis is longer than has been reported by other researchers (Serovich et al., 2005). HCPs must be vigilant about outreach and follow-up with newly diagnosed individuals, especially rural AA men, to ensure that they engage in HIV care and services, such as counseling.
The factors that influenced the men’s disclosure decisions support findings from other studies (Derlega et al., 2004; Gaskins et al., 2011; Herek, 1999). Participants were well aware of the potential substantial consequences of negative or positive responses from others and tried to determine how the recipients would react or respond to a disclosure. The fear of stigma has been identified as a risk that PLWHA are concerned about when they disclose as it negatively affects their quality of life and mental health (Herek, 1999; Sengupta, Banks, Jonas, Miles, & Smith, 2010). For most of the men, their concerns about being stigmatized were from perceived stigma or observed societal stigma, rather than enacted stigma that they had experienced, as has been reported in other studies (Foster & Gaskins, 2009). Stigma was recognized early in the HIV/AIDS epidemic, and it is recognized as a barrier to prevention and treatment efforts, as well as disclosure to others (Herek, 1999; Holloway, Seaton, & Crowley, 2004). Stigma is a powerful force in society, and it is important that HCPs recognize the potential dire effects it can have on PLWHA, their families, and sexual partners. The men talked about the multiple layers of stigma associated with being an AA, gay man with HIV/AIDS. Even if the men were not gay, they feared that others would think that they were, or would think that they used intravenous drugs, because of the history of people who have been infected with HIV. HIV-related stigma is particularly pronounced in rural areas in the Deep South (Pence et al., 2007). The men’s concerns about being stigmatized in the AA community (because they were gay and had HIV infection) made nondisclosure of their HIV infection a rational decision in many cases.
Selective disclosures were made by the men that would likely increase the benefits and decrease the risks. The men were pleased with their lives and quality of care in a rural environment. However, the environment inhibited HIV disclosures for most of the men. Considering that the majority of men had been diagnosed for more than 5 years, their disclosure recipients were limited, and participants did not plan to increase disclosures. Konkle-Parker, Amico, and Henderson (2011) reported that PLWHA in the South have concerns about their privacy, and some seek health care in other areas because of this concern. Although most of the men received their health care in their hometowns, some did travel to other locations where they were not known. The majority of the men worried about their privacy, and some were concerned about visiting the collaborating ASOs. In response to this concern, ASOs did not have any signage that identified them as HIV/AIDS agencies. One of the ASOs had a red ribbon by the door that clients had requested be removed. Another ASO only had the street number on the building.
It is important that PLWHA possess the skills and efficacy to make planned disclosures. Nondisclosure has been reported to be associated with lower self-efficacy for disclosing, especially to sexual partners (Kalichman & Nachimson, 1999). It was a factor inhibiting disclosure for the participants. HCPs can provide counseling to PLWHA, as well as refer them to skill-building support services, to assist in making and enacting disclosure decisions. However, it is critical that HCPs consider the myriad factors and decisions involved for different populations.
Once a disclosure was made, the outcomes or consequences influenced future disclosure decisions. Positive outcomes encouraged the men to consider disclosing to others, whereas negative outcomes resulted in disclosure regret and a reluctance to disclose to others. Careful planning and decision making increased the likelihood of positive responses and increased disclosures.
A limitation of the study is that the time from diagnosis until entering treatment was not addressed in the interview. It is not clear if the delay in disclosure is associated with the delay in seeking care. Other researchers have reported that PLWHA in the Deep South delay entry into care and fail to attend their first care visit (Konkle-Parker et al., 2011; Mugavero et al., 2006). This is a critical time to begin treatment and decrease the likelihood of mortality and poor treatment responses (Lanoy et al., 2006). Research is clearly needed on this time period in this high-risk population.
Conclusion
This model of HIV disclosure is grounded in data from a population in the United States that bears a disproportionate burden of HIV/AIDS: rural AA men. The process gives HCP insight into how and why PLWHA make disclosure decisions. It is critical that HCPs understand the potential negative reactions to an HIV disclosure that PLWHA fear as well as the potential benefits. The model provides a framework for planning cultural interventions that will assist rural AA men in making disclosure decisions that will lead to support, care, and positive reactions rather than betrayal, discrimination, and negative consequences. Because the decisions in the process of disclosure are selective and iterative, interventions to support disclosure need to be ongoing and be aware of evolving or changing motivations and consequences (Obermeyer et al., 2011). Also, the model can guide future research on disclosure and needs to be studied with other populations, especially those that are underserved and stigmatized.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This research was supported by grants from the National Institute of Nursing Research (Award # 1R03NR010996-01A1).