
Abstract
The current study examines the risk perceptions of HIV-negative men who have sex with men (MSM) who use the Internet to seek unprotected sex. The research questions include the following: How great do these men perceive their HIV risk to be? Are their perceptions based on HIV knowledge or related to their risk behaviors? What factors are associated with greater/lesser perceived risk? Results revealed that more than half of the men believed that they had no or only a slight chance of contracting HIV. Risk perceptions were not related to HIV knowledge or to involvement in HIV risk practices. Four factors were identified as being associated with greater perception of HIV risk: self-identity as a sexual “bottom,” having sex while high, greater use of bareback-focused websites, and younger age. Internet-using HIV-negative men who have sex with men tend to underestimate their risk for acquiring HIV, and interventions need to help them accurately assess their risk.
Introduction
Considerable research has been conducted to establish the relationship between beliefs and attitudes and relevant behaviors. Not surprisingly, what people think and how they feel about particular topics have direct relevance to the behaviors in which they engage. The linkage between beliefs and attitudes and behaviors has been well documented and appears to be fairly strong, with the former predicting the latter quite well for diverse health-related phenomena such as alcohol use (Ham, 2009; Hasking, Lyvers, & Carlopio, 2011); eating disorders such as anorexia and bulimia (Hill & Touyz, 2007; Siconolfi, Halkitis, Allomong, & Burton, 2009); physical exercise (Mahalik & Burns, 2011; O’Connor, Rousseau, & Maki, 2004); using condoms to prevent pregnancy, sexually transmitted diseases, and/or HIV (Boone & Lefkowitz, 2004; Williams & Sallar, 2010); and smoking cessation (Chassin, Presson, Sherman, Seo, & Macy, 2010; Weinberger, McKee, & George, 2010).
Indeed, the fact that so many studies have been able to replicate a relationship between beliefs and attitudes and behaviors has led to the development of the health belief model (Ajzen & Fishbein, 1980; Rosenstock, Strecher, & Becker, 1994) and the theory of planned behavior (Ajzen, 1985, 1991). Both these theoretical paradigms have been used to construct a variety of health promotion campaigns, including many targeting HIV-related risk behaviors (the subject of the present research). Among their basic assumptions is the notion that people’s perceptions (which are a hybrid of their beliefs and attitudes) predict their behaviors. Their perceptions, in turn, are influenced by factors such as the importance that the people place on the behavior in question, their perceived susceptibility to experiencing benefits or suffering consequences as a result of engaging in a particular behavior, and their estimation of the magnitude of the benefits or consequences resulting from engaging in the behavior. Both the health belief model and the theory of planned behavior posit that people are more likely to engage in behaviors that they consider important to them, that they perceive might lead them to experience benefits (or, alternatively, that they think cannot cause them harm), and that they think have a reasonable likelihood of yielding positive benefits to them (or, alternatively, that they consider to have only remote possibilities of causing them to incur problems).
Consistent with these postulates, many HIV intervention projects and research studies have examined people’s perceptions about HIV, HIV risk behaviors, HIV risk reduction strategies, and personal assessments of their levels of HIV risk (Chesney et al., 2003; Dilley et al., 2002; Wilton et al., 2009). The idea underlying these endeavors is that people who think that their behaviors are not very risky, those who are uncomfortable with available techniques that can be used to reduce their HIV risk, and those who believe that they cannot get HIV will be more likely to engage in risky behaviors than those who adhere to other perceptions. On that basis, many of these projects have tried to educate people about various aspects of HIV and AIDS while simultaneously trying to increase their sense of vulnerability to HIV. The hope is that not only would people learn about risky behaviors and strategies that can be used to reduce such risks but also that the heightened sense of HIV-related vulnerability would lead them to decrease their involvement in behaviors that could lead them to become infected with HIV.
Largely overlooked in this body of research are studies focusing on people who think that they have no risk or very minimal risk of contracting HIV. This oversight is intriguing, especially in light of previous research findings showing that sizable proportions of study participants perceive themselves as not being vulnerable to contracting HIV despite their involvement in a variety of drug- and sex-related risky practices (Klein, Elifson, & Sterk, 2003; O’Sullivan, Udell, & Patel, 2006). In Klein et al.’s (2003) research on “at risk” women, for example, 38% of the women considered themselves to have zero risk for acquiring HIV. Nearly half (44%) of these zero-perceived-risk women reported having engaged in unprotected sex during the previous year, and more than half of the zero-perceived-risk women (54%) had engaged in at least one behavior during the year prior to interview that placed them at risk for acquiring HIV. In their work with young adult heterosexuals, O’Sullivan et al. (2006) found that people in their study did not perceive themselves to be at risk for HIV even when they engaged in unprotected vaginal intercourse.
The present study examines HIV risk perceptions among a sample of HIV-negative men who actively seek partners for unprotected sex online. The study addresses the following research questions:
Research Question 1: To what extent do these men perceive themselves to be at risk for contracting HIV?
Research Question 2: What is the relationship between level of knowledge about HIV/AIDS and personal perceptions of vulnerability to HIV?
Research Question 3: What is the relationship between involvement in risky behaviors and perceptions of personal risk for contracting HIV?
Research Question 4: What factors are associated with having a greater/lesser perception of risk for contracting HIV?
Method
Sampling and Recruitment
This article draws from data that were collected between January 2008 and May 2009 for The Bareback Project, a National Institute on Drug Abuse–funded study of men who use the Internet specifically to find other men with whom they can engage in unprotected sex. A total of 332 men were recruited from 16 different websites. Some of the sites catered exclusively to unprotected sex, and some of them did not but made it possible for site users to identify which persons were looking for unprotected sex. Barebacking-specific websites (e.g., Bareback.com, BarebackRT.com) contributed slightly more than one-half (50.6%) of the study participants to the final sample, and websites that were not exclusive to barebacking but that made it possible to identify which men were interested in barebacking contributed the other one-half (49.4%). A nationwide random sample of men was derived, with random selection being based on a combination of the first letter of the person’s online username, his race/ethnicity, and the day of recruitment. Recruitment efforts were undertaken 7 days a week, during all hours of the day and nighttime, variable from week to week to maximize the representativeness of the research sample.
Members of the research team who were involved with recruitment created profiles on the websites where recruitment of study participants was undertaken. These profiles provided minimal but accurate information about the research staff member and usually used the “free-form” field to indicate “I am here to learn more about barebacking and the men who are into this. I am 100% nonjudgmental and have a genuine interest in learning more.” Recruiters initially approached men privately via either instant message or e-mail (much more commonly via e-mail), using the randomization procedures described above. As part of the initial approach, a brief overview of the study was provided, and as part of the administration of the informed consent procedures, all men were given the opportunity to ask questions about the study before deciding whether or not to participate. A website link to the project’s online home page was also made available in order to provide men with additional information about the project.
Data Collection
Participation entailed the completion of a one-time, confidential telephone interview. Participants had the option of receiving their compensation through the online payment system PayPal via e-mail, which allowed for total anonymity, or if they preferred, they were allowed the option of receiving a check by mail, which required them to supply a name and mailing address for issuing the check. Telephone interviews were conducted instead of online surveys because the verbal communication between researcher and participant allowed for the establishment of greater trust and rapport with study participants, and it also gave participants the opportunity to ask any questions that they had regarding the purpose of the study, the nature of the questions, and so forth. Additionally, telephone interviews were chosen so as to facilitate the collection of data for the study’s qualitative research component. The qualitative data took the form of post-interview narrative summaries (what qualitative researchers often refer to as memos, or memoing; see Glaser, 1998, and Strauss & Corbin, 1998, for further information about this procedural approach), in which the interviewers recorded personal observations and thoughts, direct quotes from the participants themselves, and contextual information that the interviewers believed would help place the quantitative interview data into proper perspective. The idea underlying the memoing process was to capture information that otherwise would have been lost if the study had relied solely on the quantitative information contained in the survey instrument—information that, hopefully, could be used to illuminate and inform major study findings. Interviews were conducted during all hours of the day and nighttime, 7 days a week, based on interviewer availability and participants’ preferences. Interviews lasted an average of 69 minutes. Men who completed the interview were compensated $35 for their time. Efforts were undertaken to ensure that men did not participate more than once. The principal investigator kept a record of all e-mail addresses that were used to compensate men via PayPal and also maintained a confidential listing of the names of the men who opted to receive their compensation via mailed checks. Only one man participated twice in the study and only his first interview data were entered into the database. Prior to implementation in the field, the research protocol was approved by the institutional review boards at Morgan State University and George Mason University.
Measures Used
The questionnaire was developed specifically for use in The Bareback Project, with many parts of the interview derived from standardized scales previously used and validated by other researchers. Information about each man’s HIV serostatus was collected by self-reports. Men could self-identify as being HIV-negative, being HIV-positive, or as serostatus unknown, with the latter category being selected very rarely.
Perception of HIV risk was determined by one question, measured ordinally, asking HIV-negative men “How likely do you think you are to become HIV-positive? Would you say that you have: no chance at all, only a slight chance, some chance, about half a chance, a pretty good chance, or a very strong chance?” Additional clarification of these terms was provided by the interviewer, as needed (which occurred only on a few occasions throughout the entire study), quantifying “only a slight chance” as 1% to 20%, “some chance” as 21% to 40%, “about half a chance” as 41% to 60%, “a pretty good chance” as 61% to 80%, and “a very strong chance” as greater than 80%.
Knowledge about HIV/AIDS was ascertained via 15 questions inquiring about various ways that HIV could or could not be transmitted. For each item, respondents were asked to indicate whether they knew the statement was true, thought the statement was true, knew the statement was false, thought the statement was false, or simply did not know whether it was true or false. Responses were deemed correct only when people gave a response indicating that they knew the correct answer. Correct guesses were considered wrong answers because they indicated a lack of true knowledge on the part of the participant. Items for this quiz were adapted from the work of M. P. Carey, Morrison-Beedy, and Johnson (1997). Correct responses to items on this scale skewed slightly on the high side but generally had a fairly normal distribution (mean = 10.6 correct answers out of 15, SD = 3.3).
Eight specific HIV risk behaviors were examined in conjunction with Research Question 3, and all but one (Item 5, below) were assessed via continuous measures. The first was the percentage of all sex acts involving the use of condoms. 1 This was derived from men’s responses to separate questions inquiring about their oral sex, anal sex, and vaginal sex practices (range = 0-100, mean = 12.1, SD = 23.0, median = 0). 2 Second, the percentage of all anal sex acts (insertive and receptive) involving the use of condoms was examined (range = 0-100, mean = 26.7, SD = 38.3, median = 0). The third measure was the percentage of all sex acts involving internal ejaculation (range = 0-100, mean = 34.2, SD = 28.4, median = 29.0), and the fourth was the percentage of all anal sex acts (insertive and receptive) involving internal ejaculation (range = 0-100, mean = 45.8, SD = 39.2, median = 44.2). All the preceding measures used a past-30-days time frame of reference. The fifth HIV risk item, a categorical measure, asked people about the desired HIV serostatus of prospective sex partners, allowing them to respond either that their sex partners must be HIV-negative, that they would prefer their sex partners to be HIV-negative, that they did not care whether their partners were HIV-negative or HIV-positive, that they preferred their sex partners to be HIV-positive, or that their partners must be HIV-positive. Sixth and seventh, men were asked the number of different people with whom they had sex of any kind during the preceding 30 days (range = 0-151, mean = 7.7, SD = 15.3, median = 3.0) and during their lifetimes (range = 0-10,000, mean = 453.3, SD = 1,145.1, median = 98). Finally, men were asked about the number of times during the previous month that they had engaged in sexual relations while under the influence of alcohol and/or other drugs (range = 1-150, mean = 7.8, SD = 20.9, median = 0). This measure was derived from separate questions inquiring about their recent use (number of days of use, number of times using on a “typical” day of use) of alcohol and nine different types of illegal drugs and then about substances that had been used and the number of times in which use had occurred “shortly before you had sex with someone or while you were having sex.”
Consistent with The Bareback Project’s theoretical underpinnings as a syndemics theory–based study (see Klein, 2011c, for additional details about this), for Research Question 4, items chosen for examination as possible predictors of HIV risk perception were divided into four categories: demographic measures, substance use/abuse variables, risk-related preferences, and psychological/psychosocial functioning.
Demographic measures examined in conjunction with Research Question 4 included age (continuous), educational attainment (continuous), race (categorical), sexual orientation (gay vs. other), relationship status (“involved” vs. “not involved” with a partner), and population density of the area of residence (continuous, as computed from the person’s zip code; U.S. Census Bureau, 2000). Additionally, the person’s role identity as a sexual “top,” “versatile top,” “versatile,” “versatile bottom,” and “bottom” was included here. Finally, the number of persons known to the person who had died from AIDS (continuous) was examined as a possible predictor of perceived HIV risk as well.
Three substance use/abuse variables were included in this part of the analysis. The first was a dichotomous measure indicating whether or not the person had used any illegal drugs during the 30 days prior to interview. The second assessed the number of drug problems the person had experienced during the preceding month. This was a scale measure (Cronbach’s α = .87) based on 14 possible drug abuse or drug dependency symptoms the person may have experienced. These drug abuse/dependency symptoms were derived from the criteria established in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; American Psychiatric Association, 1994) for diagnosing substance abuse and substance dependency, but the time-clustering criteria used for diagnostic purposes were not used in this study. These items, therefore, represent the extent to which substance use/abuse adversely affected the person’s life. Further information about this subject may be found in one of the recent articles published from The Bareback Project’s data (Klein, 2011b). The third measure indicated the number of times the person had engaged in sexual relations while under the influence of alcohol and/or other drugs during the month prior to interview (continuous). This measure was derived from separate questions inquiring about the quantity and frequency of recent use of alcohol and nine different types of illegal drugs and then about substances that had been used and the number of times in which use had occurred “shortly before you had sex with someone or while you were having sex.”
Several risk-related preferences items were examined as possible predictors of HIV risk perceptions as well. These included liking to have sex that was “wild” or “uninhibited” (continuous), physically rough (continuous), done in public places (continuous), or long-lasting (continuous). Additionally, men were asked separate questions about how much they were aroused by the sight, smell, taste, and feel of ejaculatory fluids (ordinal items that were subsequently combined into a continuous scale measure; Cronbach’s α = .84). Men’s use of the Internet on a typical day (number of minutes, continuous) and over the course of a typical month (continuous) to meet men for sex were included, as was another item asking men how often they used barebacking websites to find partners specifically for unprotected sex (ordinal).
Finally, several measures assessing various aspects of psychological and psychosocial functioning were examined via various continuous scales. These included attitudes toward condom use (derived from applicable items used in Brown, 1984; Cronbach’s α = .91), condom use self-efficacy (derived from Brafford & Beck, 1991; Cronbach’s α = .86), self-esteem (Rosenberg, 1965; Cronbach’s α = .89), current life satisfaction (derived from Diener, Emmons, Larsen, & Griffin, 1985; Cronbach’s α = .83), optimism about the future (Scheier & Carver, 1985; Cronbach’s α = .78), depression (Radloff, 1977; Cronbach’s α = .93), partner communication (derived from McCroskey, 1982; Cronbach’s α = .78), and childhood maltreatment experiences (Bernstein & Fink, 1998; Cronbach’s α = .94).
Readers who are interested in additional information (e.g., distribution of the variables, means, standard deviations, etc.) about any of the specific measures used in this study are encouraged to contact the lead author for further details.
Analysis
Research Question 1, which pertains to men’s self-assessments of their chances of acquiring HIV, is examined via descriptive statistics. Analyses of risk perception based on HIV knowledge (Research Question 2) were assessed via chi-square tests and Student’s t tests. For the individual knowledge items, responses were divided into “correct” and “incorrect” answers, and then chi-square tests were used to compare men who estimated their chances of contracting HIV to be zero or near zero (i.e., “only a slight chance of contracting HIV”) with men who estimated their chances to be greater than that. For the overall level of HIV/AIDS knowledge analytical comparison, the outcome measure was continuous, thereby warranting the use of the t test to compare men based on their estimated level of HIV infection risk.
Most of the analyses examining the relationship between level of perceived HIV risk and involvement in specific risk practices (Research Question 3) used simple regression. For all but one of these analyses, the dependent variable was a continuous measure, and the risk perception measure was a six-level ordinal measure. The other analysis performed to address Research Question 3—namely, between HIV risk perception and not caring about a potential sex partner’s HIV serostatus—was undertaken via logistic regression because the dependent variable was dichotomous (men who reported no preference for their potential sex partner’s HIV serostatus vs. those who had a preference for either HIV-negative or HIV-positive partners).
For Research Question 4, which focused on the factors associated with greater/lesser HIV risk perception, the analysis was done in two parts. First, bivariate relationships were assessed for each of the independent variables outlined above and risk perception level, using the latter as the dependent variable. Whenever the independent measure was dichotomous (e.g., sexual orientation, relationship status), Student’s t tests were used. Whenever the independent variable was continuous (e.g., educational attainment, self-esteem level), simple regression was used. Then, all items found to be related either significantly (p < .05) or marginally (.10 > p > .05) to risk perceptions were entered into a multivariate equation and then removed in stepwise fashion until a best fit model containing only statistically significant measures remained.
Results
Sample Characteristics
In total, 332 men participated in the study. The present research is based on 137 of those men who self-reported as being HIV-negative at the time of interview. These men ranged in age from 18 to 72 years (mean = 41.2 years). Racially, 102 of the men in this subsample (74.4%) were Caucasian, 13 men (9.5%) were African American, 9 men (6.6%) self-identified as Latino, 9 men (6.6%) self-identified as biracial or multiracial, 3 men (2.2%) were Asian, and 1 man (0.7%) self-identified as Native American. One-hundred-fourteen men (83.2%) considered themselves to be gay, 22 men (16.1%) said they were bisexual, and 1 man (0.7%) considered himself to be curious. On balance, HIV-negative men participating in The Bareback Project were fairly well educated: 19 men (13.9%) had completed no more than high school, 54 men (39.4%) had some college experience without earning a college degree, 39 men (28.5%) had a bachelor’s degree, and 25 men (18.2%) were educated beyond the bachelor’s level.
Assessment of Risk
One HIV-negative man in 12 (8.1%) said that he had zero chance of becoming HIV-infected. An additional 60 men (43.4%) said that they had “only a slight chance” of contracting HIV. Slightly more than one-third of the HIV-negative men studied estimated their risk of becoming HIV-positive to be “some chance” (34 men; 25.0%]) or “half a chance” (15 men; 11.0%). Relatively few of the men thought that they had “a pretty good chance” (12 men; 8.8%) or “a very strong chance” of contracting HIV (5 men; 3.7%).
Personal Risk Estimation and HIV Knowledge
Overall, men perceiving themselves to have zero risk or only a slight risk of contracting HIV did not differ from men perceiving themselves to be at greater risk for HIV in terms of their levels of knowledge about HIV and its transmission (t = 1.12, p = .266). For 14 of the 15 HIV knowledge questions, these individuals were just as likely as their counterparts who perceived themselves to have a greater risk for acquiring HIV to answer correctly. The only exception was in response to the item “Using Vaseline or baby oil with condoms lowers the chance of getting HIV,” for which the men who perceived themselves to have no chance or only a slight chance of becoming HIV-infected were more likely to give a correct answer than their peers who perceived themselves to be at greater risk (83.8% vs. 62.5%; χ2 1df 7.69, p = .006).
Personal Risk Estimation and Involvement in Risky Practices
On most measures of sexual risk, men’s assessments of their level of HIV risk did not correspond to their involvement in risky practices (Table 1). For example, no association was found between the likelihood that men thought they had of contracting HIV and the overall proportion of the time that they practiced protected sex (p = .171). As another example, no relationship was found between how likely men thought they were to become HIV-positive and the proportion of their sex acts that involved internal ejaculation (p = .772). The same basic finding was obtained when the dependent measure was the proportion of anal sex acts involving internal ejaculation (p = .408). Furthermore, no relationship was found between the desired HIV serostatus of potential sex partners and men’s estimates of their chances of becoming HIV-infected (p = .153). As yet another example, the number of sex partners that men reported having during the month prior to interview was not related to their estimations of their chances of becoming HIV-infected (p = .521). The same was true with regard to the number of sex partners that the men reported having had during their lifetimes (p = .608).
Involvement in Risky Practices and HIV-Negative Men’s Estimation of Acquiring HIV

Inverse association.
Direct association.
The only main sexual risk measures for which statistically significant findings were obtained were practicing protected anal sex and having sex while under the influence of an illegal drug (Table 1). The more that men practiced protected anal sex, the less likely they considered their chances to contract HIV to be (p = .045). Protected anal sex was reported 33.8% of the time among men estimating their chances of becoming HIV-infected to be zero or only slight (n = 54), 20.4% of the time among men estimating their chances of becoming HIV-infected to be “some” or “about half”’ (n = 41), and 18.9% of the time among men who thought that they had a “pretty good” or a “very strong” chance of becoming HIV-infected (n = 17). Men who reported having had any sexual relations while under the influence of an illegal drug during the month prior to interview estimated their chances of contracting HIV to be greater than did their HIV-negative peers who did not have sex while high during that time period (p = .001).
Factors Associated With Estimations of HIV Risk
Several demographic and background variables were related (although not very strongly, for the most part) to HIV-negative men’s perceptions of their chances of becoming HIV-positive (Table 2). Men who had completed no more than a high school education perceived themselves to have a slightly greater HIV infection risk than their more well-educated counterparts did (p = .079). Men who self-identified as sexual “tops” thought that their chances of becoming HIV-positive were lower than their sexually versatile and “bottom” counterparts did (p = .050). The older a man was, the lower he tended to perceive his chance of becoming HIV-positive to be (p = .070). Knowing at least one person who had died from AIDS was associated with a somewhat lower perception of risk compared with not knowing such a person (p = .063).
Bivariate Factors Associated With HIV-Negative Men’s Estimations of Their HIV Risk

Inverse association.
Direct association.
Several of the drug-related behavioral risk and sexual risk-related preferences measures were found to differentiate men on the basis of their perceived risk of becoming HIV-positive (Table 2). For example, the greater the number of times men reported recently having had sex while under the influence of an illegal drug, the greater they perceived their risk for becoming HIV-positive to be (p = .001). The more substance abuse problems that men reported experiencing during the previous 30 days, the greater they tended to estimate their chances of becoming HIV-positive to be (p = .007). Recent users of illegal drugs were more likely to think that they could become HIV-infected than nonusers did (p = .028). There was a tendency for men who liked their sexual encounters to be “wild” or “uninhibited” to estimate their chances of acquiring HIV to be greater than did their peers who did not like this type of sex as much (p = .092). The more time men spent online in search of sex partners on a typical day (p = .021) or during the previous month in the aggregate (p = .053), the more likely they were to think that they might become HIV-positive. Moreover, the more often men said that they used bareback-focused websites to try to identify sex partners, the greater they perceived their overall risk for acquiring HIV to be (p = .003).
Many, but not all, of the psychological/psychosocial functioning items differentiated men’s perceptions of their risk for acquiring HIV (Table 2). A greater perceived risk was reported by men who were: more opposed to using condoms (p = .034), less confident in their ability to use condoms correctly or to negotiate for their use effectively (p = .021), slightly lower in self-esteem (p = .094), somewhat less satisfied with their current lives (p = .076), or slightly less knowledgeable about HIV/AIDS transmission (p = .086).
When the statistically significant and marginally significant items reported above were entered into a multivariate equation, four were identified to contribute uniquely and significantly to the determination of the extent to which men perceived themselves likely to acquire HIV (Table 3). These were sexual role identity as a “top” versus as a “bottom” or “versatile” (p=.017), whether or not the person recently had sex while under the influence of illegal drugs (p = .003), how often the man used bareback-focused websites to identify potential sex partners (p = .013), and the man’s age (p = .019). Together, these four items explained 18.7% of the total variance.
Multivariate Model of HIV-Negative Men’s Perception of Acquiring HIV
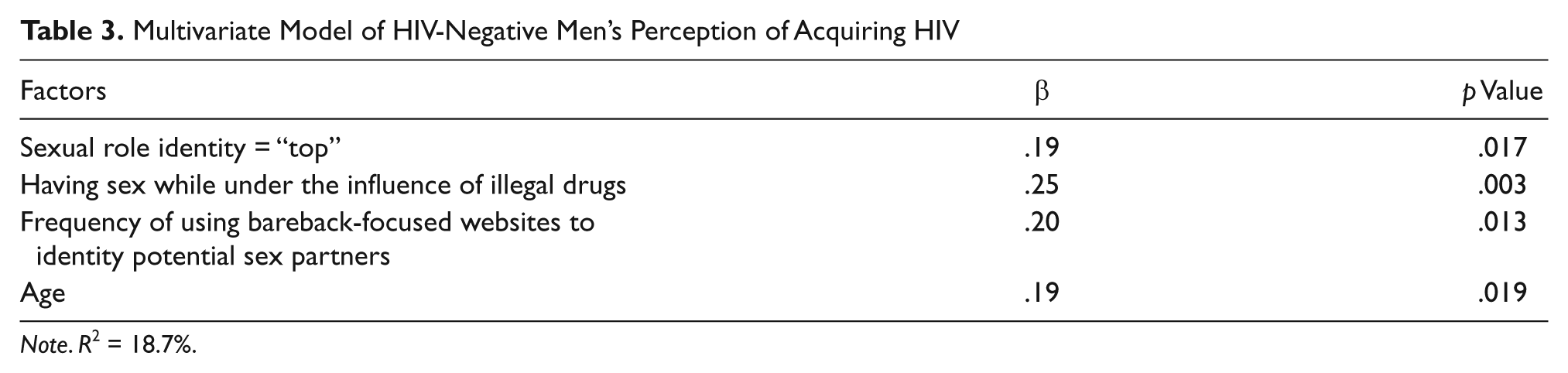
Note. R2 = 18.7%.
Discussion
Potential Limitations
As with any research study, the present study has a few potential limitations. First, the response/participation rate was low (~10%), which could raise concern of selection bias and, therefore, the representativeness of the sample. Although it is difficult to be certain that the men who participated represent the men who did not, there is compelling evidence to suggest that differences between the two groups are minimal. Before The Bareback Project was started, the principal investigator conducted a large-scale content analysis with a random national sample of one of the main websites used by men to meet other men seeking unprotected sex partners (for additional information, see Klein 2009a, 2009b, 2008). The demographic composition of that sample and the one obtained in The Bareback Project closely match one another in terms of age representation, racial group composition, sexual orientation, and rural/suburban/urban location of residence. The two samples also resemble one another closely in terms of the types of sexual practices that men sought. The similarity of the two samples suggests that men who chose to participate in the present study represent those who did not, in terms of identifiable characteristics that are likely to be the best indicators of selection bias. Despite these similarities, the participation rate remains on the low side and thus represents a potential limitation for generalizability.
Second, as with most research data on sexual behaviors, the data in this study are based on uncorroborated self-reports. Therefore, it is unknown whether participants underreported or overreported their involvement in risky behaviors. The study’s reliance on self-reported data is acceptable, however, as other authors of previous studies conducted with similar populations have reported good levels of data quality (e.g., reliability and validity) in their research (Schrimshaw, Rosario, Meyer-Bahlburg, & Scharf-Matiick, 2006). This is particularly relevant for self-reported measures that involve relatively small occurrences (e.g., number of times having a particular kind of sex during the previous 30 days), which characterize the substantial majority of the data collected in this study (Bogart et al., 2007). Other researchers have also commented favorably on the reliability and/or the validity of self-reported information in their studies regarding topics such as condom use (Morisky, Ang, & Sneed, 2002) and substance use/abuse (Anglin, Hser, & Chou, 1993; Jackson, Covell, Frisman, & Essock, 2004; Yacoubian & Wish, 2006).
A third potential limitation is the possibility of recall bias. For most of the measures used, respondents were asked about their beliefs, attitudes, and behaviors during the past 30 days. This time frame was chosen specifically (a) to incorporate a large enough time frame in order to facilitate meaningful variability from person to person and (b) to minimize recall bias. Although the authors cannot determine the exact extent to which recall bias affected the data, other researchers who have used similar measures have reported that recall bias is sufficiently minimal that its impact on study findings is likely to be negligible (Kauth, St. Lawrence, & Kelly, 1991). This seems to be especially true when the recall period is small (Fenton, Johnson, McManus, & Erens, 2001; Weir, Roddy, Zekeng, & Ryan, 1999), as was the case for most of the main measures used in the present study.
Fourth, as discussed in our “Measures Used” subsection, men’s perception of HIV risk was determined by one question, measured ordinally, asking HIV-negative men: “How likely do you think you are to become HIV-positive? Would you say that you have: no chance at all, only a slight chance, some chance, about half a chance, a pretty good chance, or a very strong chance?” Additional clarification of these terms was provided by the interviewer, as needed, quantifying “only a slight chance” as 1% to 20%, “some chance” as 21% to 40%, “about half a chance” as 41% to 60%, “a pretty good chance” as 61% to 80%, and “a very strong chance” as greater than 80%. Some researchers may disagree with our operational definition of a slight chance being between 1% and 20%. However, the overwhelming majority of men who were asked this question did not ask for clarification of the distinction between “a slight chance” or “some chance” (or any of the other response categories). They simply interpreted the ordinal response options on their own as they did, without problems, with other ordinal measures used in the study. Therefore, we do not believe that this potential limitation has any consequential bearing on the findings reported in this article.
Interpretation of Findings
Despite these limitations, a number of interesting findings were revealed by this research. First, despite their involvement in risky sex, most of the HIV-negative men in this study did not think that their chances of contracting HIV were very strong. More than half believed that they had no chance whatsoever or at most a slight chance of becoming HIV-infected, and more than three-quarters said that they had a less than fifty-fifty chance of contracting HIV. These estimates are unrealistically low, particularly when one considers that all of the men participating in The Bareback Project were searching online for sex partners with whom they could engage in unprotected sex. Additionally, sexual protection rates were extremely low, with protected sex accounting for fewer than one in six sex acts among HIV-negative men who perceived themselves to have no chance or only a slight chance of contracting HIV.
Gaps in HIV-related knowledge may account for some, but by no means all, of the underestimation of personal risk exhibited by this study’s HIV-negative men: More than a quarter of the men perceiving themselves to have zero or only slight risk for contracting HIV believed that withdrawing a penis prior to internal ejaculation will keep a man safe from HIV. Nearly one-half of the men thought that performing oral sex cannot lead to the transmission of HIV (see Klein, 2011a, 2011c, for additional details about this). More than a quarter of the men perceiving themselves to have no risk or only slight risk of becoming HIV-infected believed that, at the present time, there is a vaccine that can prevent adults from becoming HIV-infected. On average, zero-/low-risk perception men answered nearly 11 of the 15 HIV knowledge questions correctly, indicating a moderate level of understanding of the facts surrounding HIV and HIV transmission. If barebacking men do not understand all the facts regarding HIV transmission and sexual protection, they cannot be expected to develop accurate assessments of their personal level of risk for acquiring HIV.
But lack of knowledge about HIV transmission alone does not account for men’s estimations of their level of risk for acquiring HIV. Undoubtedly, denial of risk plays a key role here, as does health-related optimism. Some researchers have shown that men engaging in HIV-related risk behaviors have optimistic outlooks about their health and health practices, thereby minimizing their perceptions of harm (Hart, James, Hagan, & Boucher, 2010; Peterson & Bakeman, 2006). The present study’s findings are consistent with the notion of health optimism discussed in those reports.
The present study’s data suggest that HIV interventionists working with high-risk MSM (men who have sex with men) populations need to assess their target population’s perceptions of their personal risk for becoming HIV-infected. Whenever they encounter persons whose perceptions of risk are unrealistically low, given their particular risk behavior profiles, the interventionists should educate these men as to their actual levels of risk and the specific steps that they can take to reduce their HIV risk. Previous studies have shown that greater perceived vulnerability to HIV is associated with lesser involvement in risk taking (Brooks, Lee, Stover, & Barkley, 2011; Jemmott, Jemmott, Hutchinson, Cederbaum, & O’Leary, 2008). Therefore, intervention programs that can heighten MSM’s concerns about their chances of acquiring HIV to a level that is commensurate with their actual risk behaviors may yield successful outcomes in terms of helping men reduce their involvement in HIV risk practices. It is exactly this “it can happen to you” type of message that has been shown to be most likely to bring about risk behavior reductions in at-risk populations (Cohen & Bruce, 1997; Jemmott et al., 2008).
Another interesting finding obtained in this study was that, by and large, men’s perception of risk was not related to their actual involvement in risky practices. It had nothing to do with the amount of sex they had involving internal ejaculation; it was not related overall to rates of (un)protected sex; it was not based on the number of sex partners the men had had, recently or over the course of their lifetimes; and it was not associated with insisting (or failing to insist) that one’s sex partners be HIV-negative. Overall, HIV-negative men’s risk perceptions were attributable to factors other than the actual levels of risk inherent in their particular sexual practices.
One exception to this was their involvement in having sex while high on illegal drugs, which was linked to a greater perception of risk of becoming HIV-positive. This is a founded, realistic fear, and numerous studies have shown that having sex while high is a risk factor for HIV (J. W. Carey et al., 2009; Semple, Strathdee, Zians, & Patterson, 2009). Intervention efforts need to find ways to reduce men’s practice of having sex while high. One good way to do this would be to encourage men who need substance abuse treatment to get such help. This recommendation is particularly salient in light of the fact that a sizable proportion of the HIV-negative men who took part in this study (41.2%) reported at least some sex while “under the influence” during the month prior to interview. Moreover, more than one-quarter of this study’s HIV-negative men (26.5%) could be classified as substance abusers based on the diagnostic criteria listed in the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (see, Klein, 2011b, for more information about this). Completing drug treatment has been shown to be effective at helping reduce HIV risk practices in a variety of population groups (Booth et al., 2011; Metzger, Woody, & O’Brien, 2010), including MSM (Jaffe, Shoptaw, Stein, Reback, & Rotheram-Fuller, 2007; Shoptaw et al., 2008).
It is noteworthy that, for many years now, the MSM community itself has been aware of the need to promote substance abuse awareness among gay and bisexual men. Indeed, numerous grassroots efforts such as Tweaker.org, LifeOrMeth.com, MyMethLife.org, DrawTheLine.org (all of which are online initiatives to combat the effects of methamphetamine in the gay community), the Stonewall Project (which targets MSM and substance abuse more generally via a website as well as various individual counseling and group counseling programs), and Recovering With Pride (a community-based substance abuse assessment and treatment program for MSM in the Chicago area) have been developed and implemented by members of the MSM community to try to educate gay and bisexual men about the risks associated with drug use/abuse and to provide resources that can help them overcome their substance abuse problems. Efforts such as these are to be applauded, and more work of this type at the grassroots level is needed.
The present research identified a number of factors that were associated with men’s risk perceptions. These merit further discussion, because they have important implications for prevention and intervention. First, this study found that the more “bottom” oriented a man was sexually, the greater his perception of risk tended to be. Again, this is a founded, realistic basis for concern because sexual “bottoms” are, indeed, more at risk for acquiring HIV than “top” men are by virtue of their practices of receptive sex and semen acceptance during sex. HIV interventions, therefore, especially need to address the sexual health needs of men who prefer engaging in receptive sex and to work with these men to develop strategies that can reduce their risk for HIV. Easily overlooked by this finding, however, is that men who self-identify as sexual “tops” also may underestimate their chances of becoming HIV-infected. For example, nearly two-thirds of the HIV-negative “tops” estimated their chances of becoming HIV-infected to be zero or only slight. This was true despite the fact that these men reported an overall condom use rate of 8.9%, a condom use rate of only 18.3% during anal sex, and an internal ejaculation rate of 48.4% during anal sex. Clearly, these men are not at zero or slight risk of contracting HIV. Like their “bottom”-oriented counterparts, they comprise a group in need of targeted intervention messages. Research has shown that self-identification as “tops” and “bottoms” is a meaningful distinction among MSM (Carballo-Diéguez et al., 2004; Moskowitz, Rieger, & Roloff, 2008) and indicates that targeted intervention efforts aimed at these groups might be effective if implemented properly.
Additionally, greater use of bareback-oriented websites to identify potential sex partners was linked with a greater perception of risk of acquiring HIV. Once again, this concern is founded and realistic in light of recently published reports documenting the propensity for men who use the Internet to locate sex partners to seek high-risk sex via this venue (Berg, 2008; Grov et al., 2007). Many men who actively use the Internet to find sex partners do not ask potential partners about their HIV serostatus, about the recency of their HIV testing, about whether they will consider using condoms, or about whether they are under the influence of alcohol and/or other drugs when they show up for their agreed-on sex sessions (Carballo-Diéguez, Miner, Dolezal, Rosser, & Jacoby, 2006; Davis, Hart, Bolding, Sherr, & Elford, 2006). Other men make the effort to broach these subjects but take new partners (who are ostensibly strangers to them, if they are hooking up for sex after finding one another online and having a brief chat or e-mail exchange with them there) at their word regarding matters of HIV serostatus, recency of testing, and so forth. For example, 40.0% of the HIV-negative men who took part in The Bareback Project said that they were “fairly confident” or “very confident” in the accuracy of the information provided to them by Internet-met sex partners when they inquired about their HIV serostatus. Although it is good that these men are asking partners about their HIV serostatus, it is unwise for them to take strangers at face value with regard to important health matters such as HIV serostatus. This is especially true when decisions about whether or not to use condoms are, subsequently, based on the information supplied to them by these men during those discussions.
Last, older men, particularly those older than 50, were less likely to perceive themselves as being at risk of acquiring HIV when compared with their younger counterparts. Analysis of their actual risk practices showed that older and younger men are nearly identical in terms of their risk behavior profiles (Klein, 2012); so this is an unrealistic assessment of lower risk for HIV on their part. Recent trends in the national HIV data have shown slow but steady increases in the proportion of all new HIV diagnoses comprised by older adults (Centers for Disease Control and Prevention, 2007, 2011). Undoubtedly, one reason for this alarming trend is that older persons do not perceive themselves to be at risk for contracting HIV (Small, 2010; Ward, Disch, Levy, & Schensul, 2004). The main implication of this particular finding is clear and straightforward: Older men need targeted intervention, particularly education about HIV risk/transmission, so that they can come to assess their personal risk more accurately. Age-specific/age-appropriate interventions have been recommended by numerous scholars, and they have been shown to be effective at reducing HIV risk (Orel, Spence, & Steele, 2005; Salomon et al., 2009).
Conclusion
In summary, despite engaging in sexual practices that placed them at risk for acquiring HIV, most of the HIV-negative MSM in this study did not think they had a very strong chance of acquiring HIV. This misperception undoubtedly puts men in harm’s way as they actively seek partners for unprotected sex online. A lack of knowledge regarding HIV transmission behaviors may be responsible, in part, for unrealistically low risk perceptions among HIV-negative MSM; but this is not a convincing or comprehensive explanation for their perceptions of having zero or very low risk for contracting HIV. As a general rule, the extent to which men were involved in risky behaviors was not influential in their perceptions of their personal risk for contracting HIV (although having sex while high was found to be associated with risk perceptions). What was found to affect men’s risk perceptions, however, were their sexual role identity (particularly if they considered themselves to be sexual “bottoms”), the use of bareback-oriented websites to identify sex partners, and their age, as well as their involvement in having sex while under the influence of alcohol and/or other drugs. These factors must be taken into account by HIV prevention workers and interventionists if they wish to have a positive impact on HIV-negative men’s perceptions of their risk for acquiring HIV.
Footnotes
Acknowledgements
The authors acknowledge, with gratitude, the contributions made by Thomas P. Lambing to data collection and data entry/cleaning efforts.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This research was supported by the National Institute on Drug Abuse (5R24DA019805).