
Abstract
Anxieties regarding cancer and screening have been consistently linked in prostate screening behavior with cancer-related anxieties generally thought to be higher among minority men. To date, however, the literature linking cancer anxieties to screening among diverse men remains predicated on self-reported anxiety. Research has yet to consider how “accurate” the reporting of anxiety may be among distinct groups of men or the possibility that anxiety may influence prostate cancer (PC) screening behavior through conscious and nonconscious channels; the current study tested for discrepancies between self-report and Stroop-ascertained general- and prostate-specific anxiety and their links to screening among 180 U.S.-born African American, U.S.-born European American, and immigrant Jamaican men. Men provided self-report information regarding trait and prostate-related anxiety and completed an emotional Stroop task. Mixed model ANOVAs showed that while U.S.-born African Americans had few discrepancies between self-report and Stroop-ascertained anxiety, Jamaicans reported greater PC anxiety than indicated by Stroop performance, while the opposite was true among U.S.-born Europeans. As expected, self-reported (but not Stroop-ascertained) PC anxiety predicted screening in multivariate analysis. Although men from different age and ethnic groups varied in the discrepancy between self-reported and Stroop-ascertained PC anxiety, the influence of avoidance-producing emotions appears to operate predominantly through conscious channels.
The threat of prostate cancer (PC) and the associated screening and treatment provoke considerable anxiety. Men with lower urinary tract symptoms report prostate fear (Brown et al., 2003), uncertainty and well-being impairments follow screening (Torta & Munari, 2009) even after a favorable result (MacEfield et al., 2010), and anxiety is a major issue among PC patients (Roth et al., 2006). Although the literature remains small, anxieties regarding PC and PC screening are emerging as potentially among the most intervention accessible variables linked to prostate screening (Consedine, Adjei, Ramirez, & McKiernan, 2008). Ongoing debates regarding the recommended age of screening, the prostate specific antigen (PSA) levels requiring biopsy, the age to stop screening (Catalona, Loeb, & Han, 2006), and the possibility of overtreatment likely increase anxiety surrounding both PC and the question of whether to screen or not. Some work implies advantages to screening (Weinmann et al., 2005), although case–control (Concato et al., 2006) and meta-analytic work is inconclusive (Ilic, O’Connor, Green, & Wilt, 2007). At the time of data collection, American Cancer Society guidelines suggested that men older than 50 years be offered annual digital rectal examination and PSA screening (45 years where men have a family history or are African American) as long as men are informed of screening’s benefits and limitations (Smith, Cokkinides, & Eyre, 2004). Following a recent review, guidelines were altered in 2009 such that they no longer applied to men with a life expectancy of less than 10 years (Wolf et al., 2010).
Although they offer a useful avenue for interventions, anxieties regarding PC and PC screening are complex, poorly understood phenomena and numerous terminologies have been used. Prostate-related anxiety may be caused by screening itself (Roumier et al., 2004), men may avoid screening tests for fear of discovering PC (Cormier et al., 2002; Myers et al., 1996), and concerns regarding discomfort or embarrassment may also be important (Myers et al., 1996; Nijs, Essink-Bot, DeKoning, Kirkels, & Schroder, 2000). Men with greater state anxiety were more likely to drop out of a screening program (Roumier et al., 2004), and greater worry and concern about screening predicted self-care versus no care (Kunkel et al., 2004). Conversely, concern regarding PC has been associated with use of prostate-related complementary and alternative medicines (Beebe-Dimmer et al., 2004), and greater trait anxiety predicted more frequent screening in a diverse group of men (Consedine, Morgenstern, Kudadjie-Gyamfi, Magai, & Neugut, 2006).
It has been argued that one key function of anxiety is to motivate behaviors that ameliorate the felt experience of anxiety (Consedine, Magai, Krivoshekova, Ryzewicz, & Neugut, 2004) and/or anticipatorily prevent experiences of it. In this view, anxieties regarding PC predict screening because men anticipate feeling less anxious following screening (Dale, Bilir, Han, & Meltzer, 2005). Consistent with this expectation, anxiety is typically reduced after negative screenings (Taylor, Shelby, Kerner, Redd, & Lynch, 2002) or biopsies (Essink-Bot et al., 1998), with reductions being greater for younger men and African Americans (Taylor et al., 2002). Testament to the complexity of anxiety–screening links, however, other works considering anxieties regarding the screening procedures themselves have found that greater anxiety predicts less frequent screening (Consedine et al., 2008).
In any case, the current literature is limited in several important ways. First, most work examining anxiety–screening links is based on the assumption that men from different age and ethnic groups are equally willing or able to report on experiences of PC-related anxieties. This assumption remains despite documented ethnic and age differences in patterns of emotion regulation (Consedine, Magai, Horton, & Brown, 2011; Gross & John, 2003), coping (Brantley, O’Hea, Jones, & Mehan, 2002), and repression (Steele, Elliot, & Phipps, 2003) that have been linked to the underreporting of anxiety. It has been argued that the early experiences of both U.S.-born African American (Pinderhughes, Dodge, Bates, Pettit, & Zelli, 2000) and English-Caribbean men (Gopaul-McNicol, 1999) have made them emotionally stoic and tend to reduce the extent to which experiences of anxiety are reported by these groups of men (Magai, Consedine, Gillespie, O’Neal, & Vilker, 2004).
Second, most work seeking to illuminate the link between anxiety and health behavior is based in the notion that it is the consciously experienced aspect of anxiety that affects screening behavior (Consedine, Magai, Krivoshekova, et al., 2004). In this view, cancer-related anxieties are linked to screening behavior predominantly through the motivational functions of emotions—persons behave in ways that deliberately or involuntarily reduce felt anxiety, screening when they are cancer worried, and/or avoiding screening contexts when they are afraid of screening (Consedine et al., 2008). This experiential–motivational view might imply that when contrasting the utility of conscious and unconscious PC and PC screening anxiety metrics, only conscious anxiety or worry should predict screening outcomes.
Basic research, however, implies a key role for unconscious emotional vigilance or threat sensitivity (Etkin, et al., 2004) in behavior; the motivational impetus associated with experience is only one function and most emotions have multiple functions and pathways by which they may affect health-relevant behavior (Consedine & Moskowitz, 2007). In emotions theory, the question of whether an emotion must be consciously experienced to manifest function (or impact behavior) is typically left as an “open” dimension of the emotion, meaning most writers are agnostic about whether consciously experienced emotions are always needed to manifest a behavioral impact. Anxiety may influence behavior nonconsciously by affecting ability or motivation regarding the anticipation of possible future dangers (Etkin et al., 2004) or through rehearsal and preparatory coping (Matthews, 1990). For example, it may be that unconscious anxiety increases attention to, or absorption of, health-relevant information and that behavior is thus influenced through processes other than motivational channels alone.
Methodologically, the presence of unconscious emotional processing is typically inferred through an examination of the impact the unconscious emotional process may have on the cognitive process. Consistent with this approach, the current study used a variation on the emotional Stroop test (McKenna & Sharma, 1995) to assess conscious and nonconscious PC specific and general (trait) anxiety among samples of U.S.-born African American, U.S.-born European American, and Jamaican men. The Stroop approach is based on the assumption that where word meaning is relevant to underlying anxieties and concerns, attentional bias interferes with the processing of word color, increasing reaction times (Phaf & Kan, 2007). In this approach, the precise meaning that participants assign to the words is perhaps less relevant than the level of implicit threat the words contain.
Despite debate (Algom, Chajut, & Lev, 2004), there is increasing evidence that Stroop effects may be domain specific, with greater interference in trait-related but not unrelated areas (Edelstein & Gillath, 2008) and in domains of ideographic importance (Wingenfeld et al., 2006). Reaction times consistent with specificity occurs among smokers (Drobes, Elibero, & Evans, 2006), drinkers (Carrigan, Drobes, & Randall, 2004), persons worried about health (Matthews & MacLeod, 1986), and asthmatics (Jessop, Rutter, Sharma, & Albery, 2004). In addition to suggesting that Stroop methods have the potential to validly assess anxieties regarding PC and screening that are not being experienced by men, there is some evidence suggesting a relation between such anxiety and screening outcomes should be found (Jessop et al., 2004; Waters et al., 2003).
Finally, there remains an ongoing need to examine PC-related anxiety among specific ethnic subpopulations. Most studies group minority persons within general racial rubrics such as “White,” “Black,” and “Hispanic” (O’Malley, Kerner, Johnson, & Mandelblatt, 1999) and assumes little within-group variation. However, ethnic categories such as “African American” are arbitrary, often encompassing U.S.-born African Americans as well as individuals of African descent from the West Indies (Consedine, Magai, & Conway, 2004). Blacks from the Caribbean constitute the largest subgroup of Black immigrants in the United States (Williams, Lavizzo-Mourey, & Warren, 1994), with 1990 estimates suggesting that nearly 1 million persons were of English-speaking West Indian ancestry and 300,000 of Haitian ancestry (Schmidley & Gordon, 1999). To understand disparities and their origins, researchers must first examine samples that access diversity and employ greater specificity in sample definition.
Perhaps because PC incidence and mortality rates are elevated among African Americans and men from the Caribbean (Phillips et al., 2007), anxiety regarding PC and screening are common themes in these men. African Americans report greater anxiety regarding both PC and screening, particularly digital rectal examinations (Consedine et al., 2008; Gelfand, Parzuchowski, Cort, & Powell, 1995), and anxiety is an important barrier to cancer screening in the Caribbean (Consedine, Adjei et al., 2009). Some prior work including samples of Black men of Caribbean descent has reported ethnic differences in felt anxiety (Consedine et al., 2006) although other studies have not (Consedine et al., 2007).
Intriguingly, however, studies of general negative affect show a different pattern with frequently lower self-report among minorities (Consedine, Magai, et al., 2011). Rates of affective disorders are generally lower among Black Americans and Caribbean-born groups (Williams et al., 2007), as are reports of most negative emotions (Consedine & Magai, 2002). Indicative of the need for measurement models that bypass biases or limitations in self-report are data suggesting that African Americans have more “defended” regulatory styles (Magai et al., 2001), are more distancing and avoidant (Brantley et al., 2002), and are more repressive (Consedine, Magai, et al., 2011; Steele et al., 2003). African American (Pinderhughes et al., 2000) and Caribbean groups (Gopaul-McNicol, 1999) are socialized in ways that produce dissociation from the conscious experience of negative emotions (Consedine, Magai, et al., 2011). Such tendencies may be exaggerated in older samples who differentially dis-attend to negative stimuli (Isaacowitz, Wadlinger, Goren, & Wilson, 2006).
The Current Study
Given the near-exclusive reliance on self-report when assessing PC-related anxieties in prior work, the current report was designed to extend current understanding by assessing both conscious and nonconscious PC-related anxieties in a diverse group of men. In addition to documenting possible discrepancies between conscious and unconscious anxiety metrics, the study was intended to examine the possibility that either/both metrics may predict screening behavior. Based on prior findings regarding (a) prior data regarding PC-related anxiety in diverse samples of older men and (b) theoretical explanations for lower negative emotion reporting among Black minority groups, the following predictions were made:
African American and Jamaican men would report greater PC anxiety than indicated by their Stroop scores but underreport general anxiety.
Concurrently, older men were expected to show a broad pattern in which consciously reported PC and general anxiety were lower than that indicated by Stoop scores.
Finally, it was expected that consciously reported anxiety (but not Stroop ascertained anxiety) would predict PC screening classification.
Method
Participants
One hundred and eighty community-dwelling men (60 men who self-identified as belonging to each of three ethnic groups—U.S.-born European American, U.S.-born African American, and Jamaican immigrants) were recruited to a study of “emotion and men’s health.” Because PC risk is greater at younger ages among minority men (American Cancer Society, 2003), the study recruited U.S.-born African American and immigrant Jamaican participants in the 40 to 70 years age bracket and U.S.-born European American participants in the 50 to 70 years age bracket. Three men (one U.S.-born African American, two immigrant Jamaicans) were excluded from the analysis because of a prior PC diagnosis.
Procedure
Permission to conduct the study was obtained from the Long Island University Institutional Review Board; data were collected for 14 months during 2004 to 2005. Men were recruited through newspapers, community postings and contacts, and at health fairs and senior centers. Interviews were conducted by trained staff in laboratory sessions lasting approximately 60 to 90 minutes, with a small proportion of men tested on equivalent laptop computers in community settings (typically a home environment). Participants completed a background questionnaire that included questions about their ethnicity, income, education, and health history; measures of dispositional emotion; and a PC attitudes as well as a computer-administered emotional Stroop task. To avoid priming of the less common PC-related words, questionnaires were sequenced such that the Stroop task was performed prior to measures that directly related to PC. On completion, men were given $30 in reimbursement for their participation.
Experimental Task
Random number generation was used to randomize participants to one of six counterbalanced stimulus orders, a step that controls for potential habituation and attentional decline confounds (McKenna & Sharma, 1995). Participants were told that they were performing a computerized color perception task in which they would be presented with words in one of four colors (red, blue, green, or yellow). Instructions asked them to ignore the meaning of the word and use a response pad to identify the word’s color as quickly and accurately as possible.
All words were presented using SuperLab Pro Version 2.0 on one of three identical Dell Latitude D600 14-inch monitors (XGA resolution of 1,024 × 768 pixels) in capital letters using Courier New font at a font size of 55. Responses were made on an RB-620 response pad (Cedrus Corporation) using four keys that matched the colors of the words (red, blue, green, or yellow). Participants positioned the index and middle fingers of each hand on top of the keys; placement of key colors was counterbalanced, and participants were informed to disregard errors. The session began with a practice session using nonsensical letter strings (e.g., XXXXX, OOOOOO, SSSSS, ZZZZZZZZZ, and HHHHH). Participants completed 40 practice trials that were repeated if they felt they could not respond to the stimuli color without looking at their response pad. Following familiarization, a 60-second break was taken before the experimental session began.
The Stroop task involved presenting a single color word (red, blue, green, or yellow) at the center of a laptop computer monitor with a white background. Each word remained on the screen until a response was made by the participant. Following a response, each word was immediately replaced with the next stimulus. Each of the 10 neutral, general threat, and cancer threat words was presented in a randomized order within each word type group with the restriction that the same word color was not repeated consecutively. Three 40-word blocks were formed (in which each word was presented in each of the four colors) to complete the stimulus array and to produce a total of 120 responses; a 60-second rest period was given between each 40-word block. Once the three blocks had been completed, participants attempted to recall the 30 words before being provided with the lists and making ratings of their frequency, valence, and threat (McKenna & Sharma, 1995).
Materials
Three matched word lists (cancer-specific threat, general threat, and neutral) were created using cancer words (C) as a length and frequency reference point (Table 1). Since the cancer-specific words were not included in traditional counts of word frequency (Francis & Kucera, 1982), estimates of lexical incidence were computed using the AltaVista (Blair, Urland, & Ma, 2002) between December 1, 2003, and January 7, 2004. This technique permits frequency estimates for words and word classes that are not included in the classical listings (Buchanan, Tranel, & Adolphs, 2006). Matched “sets” of cancer, general threat, and neutral words were accepted where (a) length was the same and (b) the AltaVista-estimated frequency for each did not deviate more than 10% from the mean for the set. A post hoc comparison of the lists showed no differences in AltaVista estimated frequency, F(2, 27) = 0.001, p = .999.
Stroop Task Word Stimuli Listing Broken Down by Neutral, General Threat, or Cancer-Specific Threat Block

Measures
Background questionnaire
A questionnaire elicited information regarding self-reported ethnic group membership, age, household income, and education.
History and access variables
Men reported on whether they had health insurance (yes/no), a primary source of care or regular physician (yes/no), an annual exam (yes/no), as well as whether they had a personal or family history of PC and whether their physician had recommended screening. Men were asked three family history questions, regarding whether there had been prior family diagnoses in their father, grandfathers, uncles, and/or brothers; men reporting one or more relatives with a prior diagnosis were categorized as having a positive family history. Three items assessed levels of physician recommendation. Men were asked whether their physician had ever discussed their family history of PC, their risk, and/or recommended that they screen. Responses to these three items were summed to create an aggregate (α = .69), which, for predictive models, was dichotomized based on a median split as indexing lower and greater degrees of physician recommendation.
Prostate cancer knowledge
A PC knowledge questionnaire was developed based on prior work (Weinrich, Weinrich, Boyd, & Atkinson, 1998) and expanded in consultation with expert oncologists and urologists. This scale has subsequently been used in several published works among Caribbean groups (Consedine, Christie, & Neugut, 2009; Consedine et al., 2007; Gonzalez, Consedine, McKiernan, & Spencer, 2008; Lee, Consedine, & Spencer, 2011). The final scale contained 50 items that assessed knowledge in six domains of PC knowledge—anatomy, screening, risk, warning signs, treatment, and general. Covariance among the scores for the six knowledge subscales was high, and for the current report, items were aggregated to form a total knowledge score (Cronbach’s α = .68).
Prostate cancer fears
Anxieties regarding PC and the associated screening procedures were assessed with 11 items assessing cancer worry and screening fears taken from a larger, 30-item PC attitudinal measure. Psychometric data for the entire scale can be found elsewhere (Consedine et al., 2007; Consedine et al., 2008). Participants used a 1 (Not at all true/Never) to 5 (Almost always true/Always) scale. Example items include “I worry that screening procedures will hurt me somehow,” “Prostate cancer is very frightening,” and “I am afraid of prostate cancer screening.” Initial reliability examinations suggested that one of the items reduced consistency and was dropped. The remaining items were averaged (α = .64) such that a higher score indicates greater anxiety regarding PC and screening.
Trait anxiety
Trait anxiety was measured with the anxiety subscale of the State–Trait Personality Inventory (Spielberger, 1986), a 30-item inventory in which participants used a 1 (Not at all) to 4 (Very much so) metric to assess their general emotional disposition. The 10 items accessing trait anxiety were summed to provide an aggregate general anxiety score (α = .76). Although there has been little work examining the properties of this instrument among subpopulations of African American men, one study including 40 Caribbean younger men detained at two English police stations (Gudjonsson, Rutter, & Clare, 1995) used the scale, and no reliability issues were reported.
Prostate cancer screening behavior
Men recorded the number of PSA tests in the prior 10 years. This metric was adopted because of low screening in subpopulations of immigrant Caribbean men (Consedine, Christie, et al., 2009; Consedine et al., 2006; Gonzalez et al., 2008; Lee et al., 2011; Shelton et al., 2005) mean that a 12-month metric would produce very large numbers of “nonscreeners” and would not allow for comparisons among “groups” of screeners (Consedine, Christie, et al., 2009). Although concordance between self-report and medical audit measures of cancer screening is adequate, discrepancies do exist (Jordan, Price, King, Masyk, & Bedell, 1999). Validation studies suggest that estimates of PC screening are generally higher using self-report versus charts (Hall et al., 2004), although another work found that nearly one third of men were not aware of that a PSA test had just been done (Chan, Vernon, Ahn, & Greisinger, 2004), suggesting charts may underestimate screening. For the current report, men were categorized into three groups—never screened, partially adherent (i.e., less than 1 screen/year for each year that a man ought to have been screening), and screening yearly for the duration that they ought to have been screening. In the current study, 28.3% of men reported never having had a PSA, 38.3% had screened but at partially adherent rates, and 33.3% reported yearly screening (see Table 2).
Sample Demographic Characteristics Stratified by Ethnic and Age Groupings

Note. PSA = prostate specific antigen; AA = U.S.-born African American; EA = U.S.-born European American; J = immigrant Jamaican. All marked effects are significant at .05.
Data Reduction and Analytic Strategy
Data reduction and analysis proceeded in three stages. First, to control for individual differences in reaction times (RT), RTs were standardized within each participant so that the resultant z scores indicate relative speed or Stroop interference; an average was calculated for each of the neutral, general threat, and prostate-specific threat lists. To facilitate comparisons, the two self-report indices (general and PC anxiety) were then ranked across the sample with the resultant score indicating whether a person reported consciously experiencing more or less of these two types of anxiety than others. Second, a descriptive MANOVA testing for ethnic and age differences in income and education was conducted; because both varied across groups these demographics were covaried in the final step examining ethnic and age-related differences in self-reported general and prostate-specific anxiety as well as reaction times during the experimental task. All post hoc tests were Tukeys. Finally, a multinomial logistic regression predicting PSA testing classification was run. In this model, background variables were entered with structural and history characteristics and the two PC anxiety variables. These analyses defined partially adherent men as the referent group in each comparison. Thus, the coefficients presented in Tables 3 represent the odds of being assigned to the non-referent group in relation to the referent (partially adherent screener) group—the nonscreeners in the first comparison or the adherent screeners in the second.
Multivariate Predictors of Screening Classification
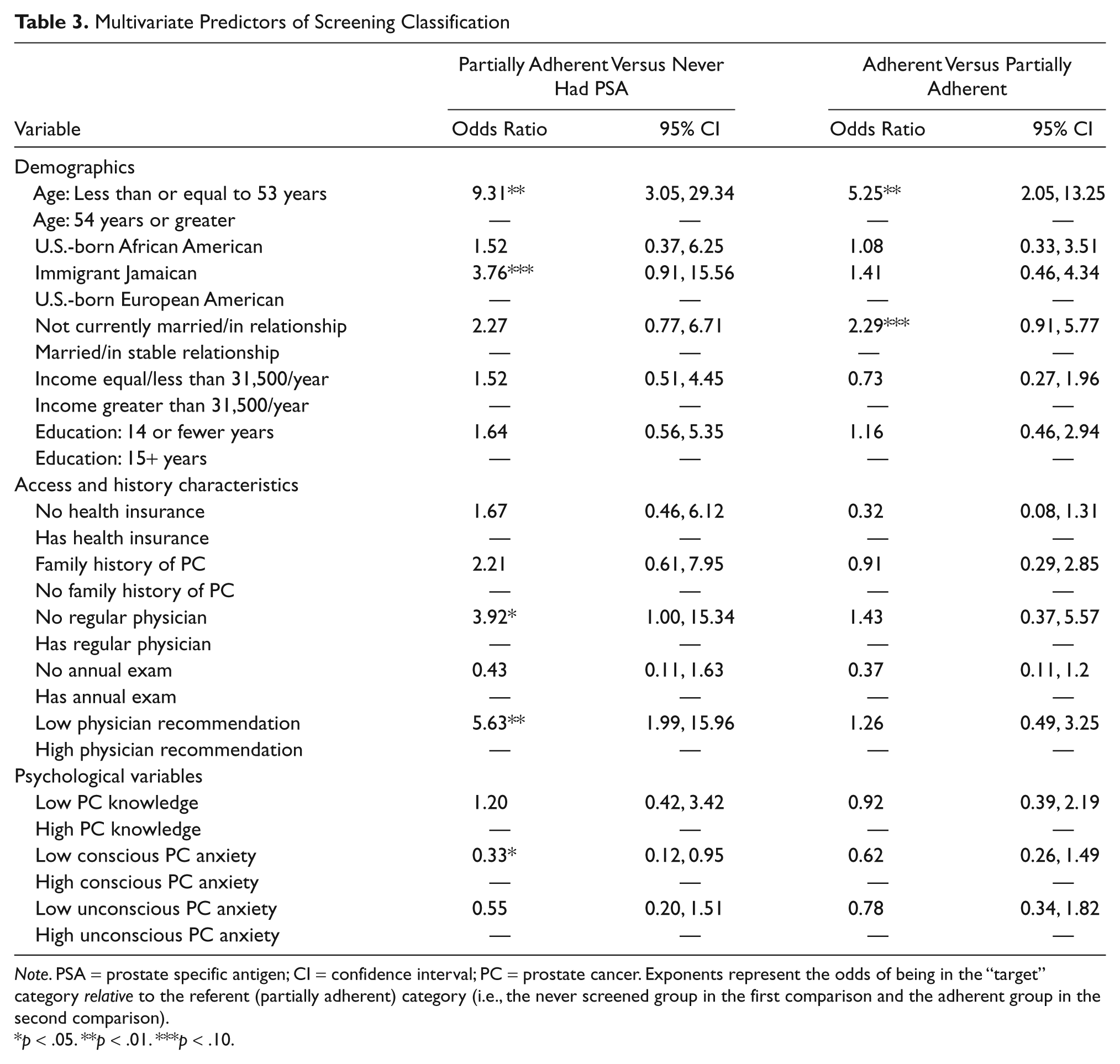
Note. PSA = prostate specific antigen; CI = confidence interval; PC = prostate cancer. Exponents represent the odds of being in the “target” category relative to the referent (partially adherent) category (i.e., the never screened group in the first comparison and the adherent group in the second comparison).
p < .05. **p < .01. ***p < .10.
Results
The sample demographics broken down by age and ethnicity are reported in Table 2. An ethnicity by age MANOVA on income and education revealed a significant effect for ethnicity, Wilks’s Λ = 9.62, p < .01, ηp2 = .10, on both income, F(2, 174) = 11.98, p < .01, ηp2 = .12, and education, F(2, 174) = 9.01, p < .01, ηp2 = .09. Tukey HSD post hocs showed that U.S.-born African Americans reported lower income than either U.S.-born European Americans or Jamaicans, while both U.S.-born African Americans and Jamaicans reported fewer years of education than U.S.-born European Americans. Factors that varied as a function of ethnicity or age were covaried in subsequent models.
Age and Ethnic Differences in Self-Reported Versus Stroop-Ascertained General and Prostate-Specific Anxiety
An initial mixed model MANCOVA with age group and ethnicity as between-subject factors, type of anxiety (general vs. prostate specific) and type of measurement (self-report vs. Stroop-ascertained) as within-subject factors, and income and education as covariates was conducted. There was an effect for ethnicity, F(2, 169) = 3.79, p < .04, ηp2 = .04, a marginal effect for age, F(1, 169) = 3.25, p = .073, ηp2 = .02, and an effect for income, F(1, 169) = 13.92, p < .01, ηp2 = .08; education was not significant and was dropped from the model. Next, a model in which age and ethnicity were between-subject factors, type of anxiety (general vs. prostate specific) and type of measurement (self-report vs. Stroop ascertained) within-subject factors, and income as a covariate was run. There was an effect for ethnicity, F(2, 170) = 5.30, p < .01, ηp2 = .06, although the effect for age remained marginal, F(1, 170) = 3.47, p = .064, ηp2 = .02, and income remained significant, F(1, 170) = 16.53, p < .01, ηp2 = .09.
Effects indicated that anxiety was higher in the Jamaicans versus African American and European American samples. There were, however, several higher order interactions. First, age interacted with type of anxiety (self-report vs. Stroop) such that unconscious anxiety (as assessed with Stroop) was higher in the older group while self-reported anxiety was greater in the younger group, Wilks’s Λ = 0.919, p < .01, ηp2 = .08. This interaction was, however, further qualified by a significant three-way interaction between age, type of anxiety, and type of measurement (self-report vs. Stroop), Wilks’s Λ = 0.974, p < .05, ηp2 = .03. Inspection of the interaction plot (see Figure 1) provides some support for the expectation that self-reported anxiety should be lower among the older cohort. Men in the younger group had greater self-reported anxiety, particularly for general anxiety than indicated by their Stroop score while the pattern was reversed in the older portion of the sample; older men’s Stroop scores indicated they were consistently underreporting anxiety, particularly general anxiety.

Interaction plot showing mean self-reported and Stroop-ascertained general and prostate screening anxiety in younger versus older men
For its part, the main effect for ethnicity was qualified by a two-way interaction with anxiety type (general vs. PC specific), Wilks’s Λ = 0.957, p < .05, ηp2 = .04. The interaction suggested that the general tendency for Jamaican men to report greater anxiety overall was more pronounced in the context of prostate anxiety. Finally, a three-way interaction between ethnicity, anxiety type, and type of measurement, Wilks’s Λ = 0.917, p < .01, ηp2 = .08, appeared to indicate that while U.S.-born African Americans showed few discrepancies between self-report and Stroop-ascertained anxiety, distinct patterns were evident in the other two groups (see Figure 2). Specifically, while the Jamaican men appeared to report greater PC anxiety than was indexed by their Stroop score, they underreported general anxiety. Conversely, the sample of U.S.-born European American men reported less PC anxiety than their Stroop score indicated but overreported general anxiety.

Interaction plot showing mean self-reported and Stroop-ascertained general and prostate screening anxiety in three ethnic groups
Self-Reported Versus Stroop-Ascertained Prostate-Specific Anxiety: Links to Prostate Screening
Finally, a multinomial logistic regression predicting the odds of being categorized as (a) a nonscreener, (b) a partially adherent screener, or (c) an adherent screener was run. The model was significant, −2 log likelihood = 277.875, Nagelkerke R2 = 0.47. Being categorized to the “never screened” group relative to the “partially adherent screening” group (left panel, Table 3) was marginally more likely among Jamaican men (odds ratio [OR] = 3.76, p = .07, 95% confidence interval [CI] = 0.91, 15.56), younger men (OR = 9.31, p < .01, 95% CI = 2.98, 29.05), men with a personal physician (OR = 3.92, p < .05, 95% CI = 1.00, 15.34), or those reporting stronger physician recommendation to screen (OR = 5.63, p < .01, 95% CI = 1.99, 15.96); men reporting low conscious anxiety were less likely to be classified as nonscreeners relative to partially adherent screeners (OR = 0.34, p < .05, 95% CI = 0.12, 0.95), but there was no relation between nonconscious anxiety and screening behavior. The model contrasting partial-adherence and recommendation-adherent screeners was weaker; adherence to screening was only significantly more likely among younger men (OR = 5.25, p < .01, 95% CI = 2.08, 13.25), with no other factors, including either conscious or unconscious prostate anxiety predicting this distinction.
Discussion
As expected, results from the current report cohere in providing preliminary demonstrations of several key observations. First, as expected, older men reported less PC and general anxiety than indexed by their Stroop scores. However, examinations of the discrepancy between self-reported and Stroop-ascertained anxiety metrics also provided support for the expectation that Jamaican men would self-report comparatively greater PC anxiety than indicated by their Stroop but underreport general anxiety; the expected effect was not found among African Americans and the reverse pattern was evident among European Americans. Finally, only consciously reported anxiety predicted PC screening classification, although only for the never versus suboptimal screening comparison; men reporting more anxiety were less likely to initiate screening. Overall, these data suggest that while patterns of conscious versus unconscious anxiety vary across age and ethnic groups, researchers can be reasonably confident in the utility of straightforward assessments of consciously experienced anxiety. Below, these findings are revisited in light of prior work and theory regarding the links between anxiety reporting, ethnicity, and the mechanisms linking anxiety to health behavior.
Prostate Anxiety Reporting in Diverse Age and Ethnic Groups
Data from the current study suggest that the correspondence between self-reported and Stroop-indexed PC and general anxiety varied across age and ethnic groups. As expected, while older (vs. middle aged) men reported relatively lower trait and PC-specific anxiety, their Stroop scores indicated greater anxiety. Although effects were stronger with the general anxiety metric, age-related results were consistent across PC-specific versus general metrics insofar as older men appeared to consistently underreport anxiety. Similarly, while there was some ethnic variation in the degree of the discrepancy (below), the overall pattern was consistent with the thesis that groups with normatively more restrictive socialization histories (i.e., Caribbean Blacks and older adults) develop regulatory patterns producing reductions in the frequency with which anxiety is consciously experienced. Thus, insofar as increased reaction times can be considered an index of anxiety unbiased by self-report, the current findings suggest that older men are uncomfortable with experiences of both PC-specific and general anxiety.
Such an interpretation is consonant with theories suggesting that restrictive socialization produces an aversion to certain experiences and a tendency to route anxiety from consciousness (Magai et al., 2004). Dismissive attachment—a style of functioning characterized by affect “minimization” (Magai, Hunziker, Mesias, & Culver, 2000)—is common among older adults (Mickelson, Kessler, & Shaver, 1997), and older adults with dismissing attachment have increased reaction times for anger and anxiety stimuli (Jain & Labouvie-Vief, 2010). Although the implications of this finding remain unclear, researchers should remain mindful of the fact that while older men report greater PC anxiety (Dale et al., 2005), they still report less anxiety than their Stroop scores indicate. Prior work has shown that Stroop-indexed sensitivities predict emotional distress regarding a subsequent diagnosis (MacLeod & Hagan, 1992), and it may be that PC diagnoses will ultimately pose a more serious challenge to groups of men who underreport.
Correspondence between self-reported and Stroop-indexed PC and general anxieties also varied across ethnic groups. Consistent with prior work suggesting the need to discriminate among ethnic subpopulations (Consedine, Magai, & Conway, 2004), analyses showed that while discrepancies were minimal among African Americans, Jamaican men reported greater PC anxiety than indicated by Stroop but underreported general anxiety while the reverse pattern was evident among European Americans (see Figure 2). The elevation in self-reported PC anxiety parallels high PC incidence and mortality rates among Caribbean groups (Phillips et al., 2007) and is consistent with prior descriptive work (Consedine, Adjei, et al., 2009). Thus, while some minorities, particularly those from the Caribbean, may underreport negative affectivity in general (Consedine, Magai, et al., 2011), this tendency can clearly be overcome where the health threat is sufficiently salient. Given the positive impact PC anxiety has on screening behavior (below), it is ironic that in this study it was the European American sample that appeared to underreport PC anxiety, perhaps suggesting that this may represent a fertile avenue for intervention in this group.
Conscious Versus Unconscious Anxiety and PC Screening
The final aim of the current report was to contrast the ability of conscious versus Stroop-ascertained, unconscious PC screening anxiety to predict the frequency of PC screening. Consistent with expectation and theory emphasizing the motivational functions associated with the felt experience of emotions (Consedine, Magai, Krivoshekova, et al., 2004)—that is, the notion that people behave in ways that reduce consciously experienced anxiety—pitting these two metrics against one another revealed that greater consciously experienced anxiety predicted increased odds of being a nonscreener (vs. suboptimal). Such a finding is consistent with work suggesting that anxiety regarding screening predicts less frequent screening (Consedine et al., 2008) as well as with other work suggesting that PC screening–related anxieties are predominantly relevant to the initiation of screening (i.e., the never versus suboptimal screening contrast) rather than to the understanding of a pattern of “maintenance” wherein men are screening over time.
That consciously experienced but not unconscious anxiety predicted behavior also provides indirect support for the assertion that identifying the source of health-related emotional experiences is critical when seeking to predict the links between those and behavior. Reaction times consistent with some degree of specificity have been demonstrated in several groups (Carrigan et al., 2004; Drobes et al., 2006); the fact that over- and underreporting of anxiety appeared to be domain specific with Jamaican men reporting greater PC (but not general) anxiety than their Stroop indicated combined with the fact that the only conscious PC anxiety predicted behavior is likewise indicative of domain specificity. In some views, because emotions arise in response to a specific stimulus (i.e., there is a stimulus that elicits the anxiety) the resultant behavior typically occurs in relation to that stimulus (Consedine, Ladwig, Reddig, & Broadbent, 2011; Consedine & Moskowitz, 2007). This is not to say that producing anxiety-reducing behaviors is the function of anxiety but, rather, that in most instances the functional behaviors that reduce objective threat appear to be mediated by a motivational mechanism involving the reduction of consciously experienced anxiety. Particularly when the emotion promotes avoidance of the eliciting stimulus, identifying the exact source of emotions in health contexts is critical because it is these specific aspects that people are motivated to behave with respect to (Consedine et al., 2008).
However, the fact that unconscious anxiety did not predict PC screening classification does not eliminate the possibility that unconscious anxiety influences health decisions. Self-report and Stroop PC anxiety scores were minimally related, suggesting, at the very least, that there may be multiple pathways. Anxiety may influence behavior nonconsciously by affecting ability or motivation regarding the anticipation of possible future dangers (Etkin et al., 2004) or through rehearsal and preparatory coping (Matthews, 1990); screening might be considered a coping behavior that occurs prior to diagnosis. However, while prior Stroop work has shown that greater interference occurs in the relevant samples (Carrigan et al., 2004), it remains unclear how unconscious processes might affect behavior. In addition to indexing threat value, reaction times may index avoidant coping (Andersen, Smith, Meischke, Bowen, & Urban, 2003), or as in some studies of self-reported anxiety (Consedine et al., 2006), the relation between unconscious anxiety and behavior may be curvilinear (see Jessop et al., 2004). Alternately, it may be that reaction times (as a method) imprecisely estimate cognitive–affective processes and that researchers need to use more complex examinations that incorporate error patterns (White, Ratcliff, Vasey, & McKoon, 2010).
Implications, Limitations, and Concluding Remarks
Although these data represent a useful clarification regarding developing an understanding of the likely mechanisms by which anxiety processes are linked to health behaviors, several considerations should be borne in mind. Most obviously, it should be recalled that the current sample was a convenience one and comprised entirely of men; the extent to which the current findings will generalize to middle aged and older women or with respect to other health domains remains unclear. Gender-wise, men and women are differentially socialized regarding emotions, with men tending to experience and express reduced levels of emotions such as fear and sadness (Madden, Barrett, & Pietromonaco, 2000); discrepancies may be lower among female samples and/or the means by which conscious and unconscious anxiety processes affect behavior may vary across groups.
Second, as with all Stroop studies, while interference scores may tell us something about the degree of unconscious threat associated with a set of stimuli, the specific meaning that men assign to such stimuli remains unclear. The challenges inherent in creating matched length/word frequency lists are substantial and meant that while most words are cancer specific, a significant proportion of the terms used may not be prostate specific. Indeed, inspection of the PC word listing used in the Stroop component of the study (see Table 1) reveals a mix of general cancer-related, cancer anatomy, treatment, and consequence type words, and it may be that the mixed focus of this listing contributes to the inability of unconscious metrics to predict behavior. More broadly, it remains somewhat unclear exactly what the interference score is indexing. Prior work has shown that the smokers in a quit program with greater interference scores were more likely to relapse (Waters et al., 2003). Thus, rather than unconscious anxiety acting to promote avoidance of smoking, it was associated with nonavoidant behavior. It may be that cigarette-related stimuli increased reaction times among a portion of the sample because they were worried about failing in their quit attempt rather than because the stimuli were anxiety provoking per se. Although assessing the unconscious meaning of stimuli may remain problematic for some time, future work should look to reduce the heterogeneity of anxiety constructs assessed with instrumentation such that a clear picture of the underlying source is provided.
These limitations noted, the current report provides evidence suggesting that, at least in the case of PC screening, the influence of avoidance-producing emotions operates predominantly through conscious channels. While there was variation in the magnitude of the discrepancies between conscious and nonconscious PC anxiety metrics as a function of age and ethnicity, conscious anxiety continued to predict screening behavior notwithstanding whether under- or overreporting appeared to have occurred. Hence, although unconscious mechanisms cannot be ruled out, they seem less likely, and it seems more probable that anxiety is linked to screening behaviors through motivational mechanisms in which persons enact behaviors that reduce their experience of felt anxiety.
Demonstrating that it is the felt experience of PC screening anxiety that predicts screening is clinically important for several reasons. First, it suggests that interventions to reduce screening anxiety may be a fertile avenue in attempts to increase screening. One way in which this might be accomplished is by communicating the fact that many men are afraid of PC screening. Initiating a dialogue regarding the fact that many men are afraid may help destigmatize men’s experience. Physician-initiated discussions may help patients see their provider as empathic and thus help establish a partnership that shifts the patient’s focus toward the management of anxiety rather than the avoidance of it. The fact that conscious anxiety was significant in the never screened versus suboptimal screener contrast but not in the contrast between suboptimal and adherent contrast—an “initiation” versus “maintenance” distinction (Consedine, Christie, et al., 2009)—is also important. It may suggest that fears are typically worse in anticipation and that such information may be of value to men. When physicians are discussing PC screening with men they might mention that fears are typically less than expected; such knowledge may provide men with a means of coping such that attendance is enhanced.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Cancer Institute (1P20 CA 91372)