
Abstract
One of the dreaded disfiguring disease conditions among the Andoni tribesmen in the Nigerian Niger delta region is hydrocele, especially when its size is large (giant hydrocele) and it cannot be concealed. This case–control study was designed to evaluate the prevalence of depression among patients with giant hydrocele presenting to Bethesda Clinic Ngo, Andoni, Nigeria. A total of 52 patients were recruited into this study: 26 in the giant hydrocele group and 26 in the control group. Their age range was 23 to 78 years, with a mean age of 53.4 ± 15.5 years for the giant hydrocele group and 53.6 ± 14.2 years for the control group. The difference between the prevalence of depression among patients that presented with giant hydrocele (61.54%) and the controls (15.38%) was statistically significant (p = .0015). The authors conclude that depression is common among patients with giant hydrocele when compared with patients with other disease conditions.
Keywords
Introduction
Comorbid psychological conditions, particularly depression, often accompany physical illness. Rodin and Voshart (1986) reported the occurrence of mild to moderate symptoms of depression in up to one third of medical in-patients. Previous studies by MacHale (2002) and Marlow, Kegowicz, and Starkey (2009) further reported different prevalence rates of depressive illness in different disease conditions. They reported prevalence rates of about 25% in patients with diabetes and cardiac or neurological disease and 32% among patients with headache in Arizona. Such patients with comorbid depression, when compared with their nondepressed counterparts, have been found to exhibit poorer levels of functioning, less adherence to treatment plans and health maintenance, amplified physical symptoms of existing conditions, greater health care utilization, as well as higher levels of mortality and morbidity (Katon & Schulberg, 1992; Wulsin, Vaillant, & Wells, 1999). This adds to the complexity of clinical management of the disease conditions with resultant higher risk of problematic outcomes.
Disfigured people are not spared of depression and its associated problems (Tatum, 2010). One of the dreaded disfiguring disease conditions among the Andoni tribesmen in the Nigerian Niger delta region is hydrocele. This is the accumulation of fluid in the tunica vaginalis causing scrotal swelling. Its female equivalent is the hydrocele of the canal of Nuck, the portion of the processus vaginalis within the inguinal canal. It is small in size and very rare (Caviezel, Montet, Schwartz, Egger, & Iselin, 2009). Hydrocele in men becomes a problem when it cannot be concealed because of its disfiguring large size (giant hydrocele). A giant hydrocele was defined as one whose size is equal or bigger than the patient’s head or extending up to the knee (Akpo, 2005).
The physical disfigurement associated with giant hydroceles is associated with functional impairment, low self-esteem, negative self-image, and social isolation. Giant hydrocele also creates emotional distress (including depression) and reduced quality of life of the patients, especially in a society that emphasizes appearance, beauty, and physical attractiveness (Ahorlu, Dunyo, Asamoah, & Simonsen, 2001; Krishna, Harichandrakumar, Das, & Krishnamoorthy, 2005;Valente, 2009; Wulsin et al., 1999). Gyapong, Gyapong, Weiss, and Tanner (2000), attesting to the problems associated with hydroceles in Ghana, reported the inability of unmarried men with giant hydrocele to find spouses and married men exhibiting various degrees of sexual dysfunction. These predispose to fear of rejection in relationships, possible separation, and divorce (Valente, 2009). These patients are often disabled from active participation in community activities (Ahorlu et al., 2001) because of the ridicule from community members (Gyapong et al., 2000).
Despite these uncomplimentary findings, screening and treatment of depression in these patients, as with other medical and presurgical populations, is often limited (Royal College of Physicians & Royal College of Psychiatrists, 1995). This is because the symptoms of depression are often subtle and hard to verbalize (Holroyd et al., 2000). Other reasons include the fact that accurate diagnosis is difficult because of lack of a simple confirmatory test (Williams, Noël, Cordes, Ramirez, & Pignone, 2002) and the consideration by some physicians that psychological disorders are less clinically relevant than physical ailments (Wells et al., 1989). Considering the known impact of comorbid depression on patients, early identification and treatment through screening may favorably influence quality of life and health care outcomes. Indeed, evidence abounds of improved clinical outcomes resulting from treatment for depression (Paraskevaidis, Parissis, Fountoulaki, Filippatos, & Kremastinos, 2006).
The association of depression with different medical conditions has been a popular subject of study in many parts of the world (MacHale, 2002). Several screening instruments such as the Beck Depression Inventory, the Center for Epidemiological Studies–Depression, the Hamilton Depression Scale, and the Zung Depression Rating Scale (Sharp & Lipsky, 2002) have been used in these studies, but in a recent systematic review by Nease and Malouin (2003), the PRIME-MD Patient Health Questionnaire (PHQ-9) was adjudged as the best depression screening tool available for primary care. Searches of the literature, both manual and electronic, reveal no objective study done on depression in patients with giant hydrocele in Nigeria. Second, considering the aesthetic and therapeutic goals of the treatment of giant hydrocele, it is imperative to objectively assess the level of depressive symptoms and give the patient holistic care.
Although there are several disease conditions that predispose to depressive symptoms, we want to test the null hypothesis that depression among patients with giant hydrocele is neither prevalent nor related to the disease condition. It is believed that the findings of this study would bring more attention to the problems posed by this disease condition and also help provoke the required public health response.
Method
Study Location
This study was conducted at Bethesda Clinic, Ngo. Ngo is a rural Niger delta town. It is the headquarters of Andoni Local Government Area in Rivers State of Nigeria. Ngo is situated in the marshland drained by creeks that empty into the Atlantic Ocean. It is one and half hour’s boat ride from Port Harcourt, the capital of Rivers State. A journey by land to the locality takes a longer period and ends with a 30-minute boat ride. This is one of the most remote towns in Rivers State and hence lacks basic amenities such as electricity, pipe-borne water, transport, good schools, and well-equipped health care facilities.
Bethesda Clinic is 10-bedded and is the only clinic visited by a consultant family physician weekly. It therefore enjoys the monopoly of good patronage compared with the government health centers in the local government area that are run by community health extension workers. It was established in 1995 and has been the only health facility rendering surgical services in the local government area, which has a population of about 211,000. Many rare surgical cases not found in other parts of Rivers State of Nigeria were therefore encountered. The clinic has a full complement of an efficient primary care medical team as health care providers. The practice is general practice/primary care oriented; therefore, a wide range of patients (surgical, medical, gynecological, and pediatrics patients) are seen. It is patronized mainly by the very poor and educationally disadvantaged fish farmers living in fishing settlements in the creeks.
Design
This is a case–control study that spanned over a period of 10 years (1998-2008).
Participant Selection
The study population was made up of men who reported to Bethesda Clinic Ngo with complaints of hydrocele. The diagnosis of hydrocele was confirmed when on physical examination a large, smooth, cystic, and painless scrotum that transilluminated when torchlight was pressed against it was felt. The details of the study were thoroughly explained to all the participants. They were examined to ensure that the size of their hydroceles met the criteria of being described as giant hydrocele before recruitment for the study.
Sample Size
The study was designed considering an alpha error of 5% and a statistical power of 80%. Using the prevalence of 10% recorded in a similar study on depression in primary care in Nigeria by Amoran, Lawoyin, and Lasebikan (2007), the minimum sample size calculated was 15 (Interactive Statistical Calculation Pages, 2010). All the patients with giant hydrocele (26) seen in the clinic during the study period were recruited to increase the power of the study further.
Sampling Method
A convenient sample of all consenting men with giant hydrocele who attended the clinic during the period of study was recruited for the study. For each presenting patient in the giant hydrocele group, a matched control for age (±2 years) was recruited during the study period. These controls consisted of consenting patients from the same environment who presented to the clinic with complaints such as fever, diarrhea, skin rashes, and cough. They were examined to ensure that they did not have hydroceles.
Inclusion criteria
All consenting adult male patients (18 years of age and older) who presented with giant hydrocele to the clinic.
Exclusion criteria
Patients seen and recruited by any other member of staff apart from the consultant family physician.
Patients identified to be using antidepressants or tranquilizers were excluded since these drugs will give false negative results in the interview.
Data Collection
This was done with the aid of a questionnaire in English language. This is a commonly spoken language by the people because of the influence of multinational oil workers involved in the drilling of crude oil in the environment. The questionnaires were administered by the most senior nurse in the clinic who was trained for 2 weeks on its administration. It was made up of two parts: the first part recorded the patients’ biodata, which included age, educational status, marital status, and occupation. The second part was the PRIME-MD PHQ-9. This is an instrument that scored each of the nine Diagnostic and statistical manual of mental disorder, 4th edition (American Psychiatric Association, 1994) criteria for major depression. The scored criteria included the presence of anhedonia, low mood, sleep disorder, tiredness, poor appetite, feeling bad about self, inability to concentrate, hopelessness, and suicide ideation occurring within the previous 2 weeks. The scores range from 0 (not at all) to 3 (nearly every day). The scoring, which takes an average of 2 to 5 minutes to complete, has been found to have good reliability and validity and has a relatively high positive predictive value for major depression (Nease & Malouin, 2003). PHQ-9 scores of 5 and above indicate various degrees of depression. These characteristics as well as its brevity make the PHQ-9 a useful clinical and research screening tool in primary care when compared with others. Scores of 5 to 9, 10 to 14, 15 to 19, and 20 represented mild, moderate, moderately severe, and severe symptoms of depression, respectively.
In this study, to allow meaningful comparison of patients with and without depression in some variables, scores on the PHQ-9 depression scale were collapsed into dichotomous measures. As in previous studies (Kroenke, Spitzer, & Williams, 2001; Marlow et al., 2009; U.S. Department of Veterans Affairs, 2009), patients with scores of ≥5 were diagnosed as depressed and those <5 free of depression. The technical justification for doing so was to construct 2 × 2 tables to enable statistical analysis. The reliability of the PHQ-9 as used in this study was good, with a Cronbach’s α coefficient of .82.
Data Analysis
Data collected were stored in Microsoft Word spreadsheet and analyzed using percentages, McNemar and Pearson’s chi-square test, and odds ratio with the aid of Statistical Package for Social Sciences, Version 15. All calculations were done at 95% confidence limit and p value less than .05 was taken as significant.
Ethical Consideration
Ethical approval of the study protocol was obtained from the management committee of Bethesda Clinic, Ngo Andoni, Rivers State of Nigeria. Written and informed consent was obtained from the participants after the aim and objectives of the study had been explained to them.
Results
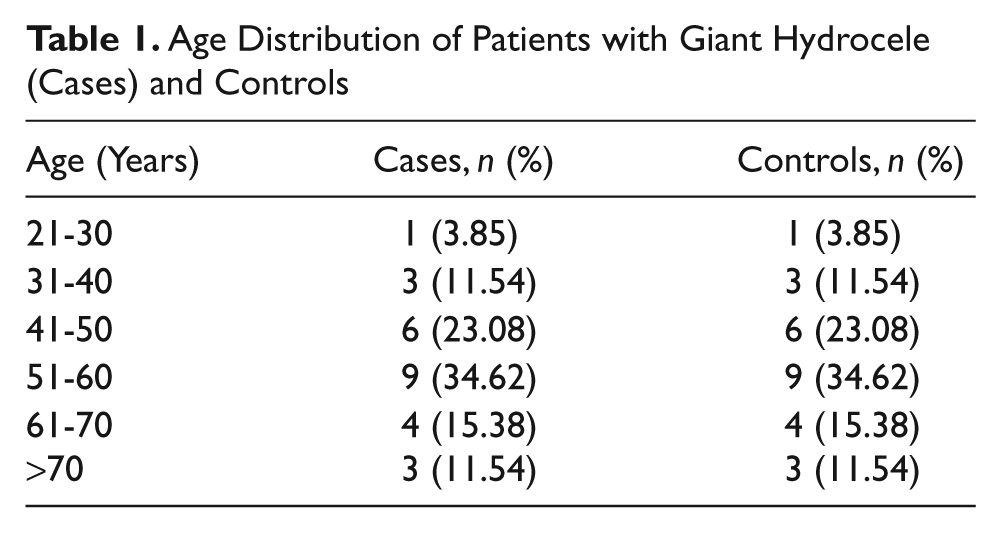
A total of 83 patients with hydrocele were seen during the study period out of which 26 (31.33%) were classified as giant hydrocele. In all 52 patients entered into this study: 26 in the giant hydrocele group and 26 in the control group. Their age range was 23 to 78 years. The mean age of participants in the giant hydrocele group was 53.4 ± 15.5 years and 53.8 ± 11.3 years in the control group. Giant hydrocele was most prevalent in the 51 to 60 years age bracket (34.62%) and least in the 21 to 30 years age bracket (3.85%; Table1).
Age Distribution of Patients with Giant Hydrocele (Cases) and Controls
Among the patients that presented with giant hydrocele, 61.54% reported symptoms of depression as compared with 15.38 % of the controls. This difference in prevalence was statistically significant (p = .0015; Table 2). Significant difference in the prevalence of depression was also found among the patients that had severe depression (PHQ-9 20) with p value of .05 (Table 3). Depression was commoner among the patients with giant hydrocele who were single/separated, had nonformal education, and were fish farmers (Table 4).
The Prevalence of Depression Among Patients With Giant Hydrocele (Cases) and Controls
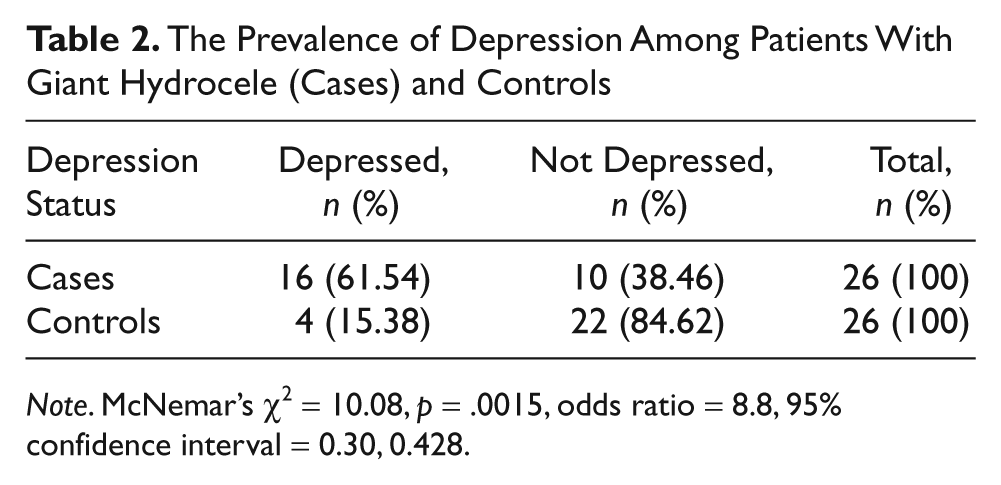
Note. McNemar’s χ2 = 10.08, p = .0015, odds ratio = 8.8, 95% confidence interval = 0.30, 0.428.
Prevalence of Symptoms of Depression Among Patients With Giant Hydrocele and Controls

Note. PHQ = Patient Health Questionnaire.
Sociodemographic Characteristics of the Study Population

Others include traders, unemployed, artisans, and civil servants.
Discussion
Giant hydrocele is a rare disease condition found in remote areas where health care facilities are rudimentary and the people poor. The prevalence of giant hydrocele was low in the younger age groups and high in the 51 to 60 years age bracket probably because of the time-dependent nature of the disease. A progressive increase in the prevalence of giant hydroceles with age is an expected finding but the contrary was the observation in this study. This could have resulted from the small number of elderly patients older than 61 years of age probably because of the low life expectancy in the area (Mathers et al., 2004).
The prevalence of depression among patients with giant hydrocele in this study is 61.54%, much higher than the 15.38% prevalence observed among the controls. Lower prevalence figures of between 5% and 10% were recorded among patients in previous primary care studies by Amoran et al. (2007) and the U.S. Preventive Services Task Force (2002). This high prevalence of depression among the patients with giant hydrocele could have been culturally induced. Gyapong et al. (2000) had opined that the cosmetically disfiguring large size of hydrocele causes stigmatization and functional impairment. This is known to affect family functioning negatively and also attract ridicule from community members.
Since there is no known previous report on the prevalence of giant hydrocele, we are constrained to compare the prevalence in this study with other forms of visibly disfiguring diseases such as Graves’s ophthalmopathy. The prevalence of depression among patients with giant hydrocele in this study is considerably higher than the 45% prevalence recorded among patients with Graves’s ophthalmopathy (Kahaly, Hardt, Petrak, & Egle, 2002; Paik & Yang, 2009). A higher prevalence among the hydrocele patients could have emanated from the involvement of sex organ with associated sexual problems (Babu, Mishra, & Nayak, 2009). Generally, disfigurement from disease conditions exposes patients to numerous psychosocial stressors that predispose to depression, especially in a society that emphasizes appearance, beauty, and physical attractiveness (Valente, 2009).
Considering the impact of giant hydrocele on patients, statistical significance was expected between the prevalence of mild, moderate, and moderately severe depression in the study and control groups. This was not found probably because of the existence of factors common to the study and control groups peculiar to the locality of the study that could predispose to depression. These factors include abject poverty resulting from the environmental degradation from oil exploration resulting in joblessness and the militant activities by youths struggling for resource control with much loss of lives.
The higher prevalence of depression among the single/separated patients with hydrocele in this study is in agreement with findings in earlier studies (Gyapong et al., 2000). A study by Babu et al. (2009) similarly revealed that the most worrisome effect of hydrocele for patients and their wives was their inability to have a satisfactory sexual life. They also highlighted the impact on marriageability, some women expressing that marrying a hydrocele patient is the “last choice.” These findings are sources of depression among the married and single/separated patients.
It is important for primary care physicians to be aware of the high prevalence of symptoms of depression among patients with giant hydrocele and to consider treating not just the hydrocele but both problems, if depression is confirmed to exist as well. MacHale (2002) advised that physicians need to remember this high prevalence of depression in these patients when prescribing drugs such as such as beta-blockers, antianxiety agents, digoxin, methyldopa, and narcotics, which may possibly worsen depression. It should be known that depression is a treatable disorder, and its potential adverse effects on surgical treatment outcomes such as poorer prognosis and longer recovery times for these patients should not be underestimated (Burg, Benedetto, Rosenberg, & Soufer, 2003; Cherr, Wang, Zimmerman, & Dosluoglu, 2007).
Many questions warranting further research remain. Does the prevalence of symptoms of depression vary with different sizes of hydroceles? Do depressed patients with giant hydroceles enjoy good family function assessed with appropriate instruments, as compared with nondepressed patients with giant hydroceles?
Limitations
This study has several limitations. The description of depression among patients with giant hydrocele in this article is limited since the sample size is small because of the rarity of the disease and the fact that the sample of participants was composed of patients from Andoni in the south geographical zone of Nigeria.
There were no PHQ-9 screening result in the patients’ records to ascertain whether they had a preexisting diagnosis of a depressive disorder (e.g., major depressive disorder, dysthymic disorder, or depressive disorder not otherwise specified) prior to the onset of the disease condition.
Conclusion and Recommendations
The findings in this study demonstrate that there is a high prevalence of symptoms of depression in patients who present to primary care physicians with giant hydrocele. Given the impact of depression on outcomes, health care utilization, and basic quality of life, it is clearly advantageous for clinicians to have a practical and efficient means of screening for depression. It is therefore recommended that the biopsychosocial approach to medical care be embraced by all primary care physicians to enhance medical outcomes. Alternatively, a multidisciplinary approach, including surgeon, family physicians, and psychiatrist, is critical for patients with giant hydrocele to achieve good therapeutic outcomes.
Additional research is needed from multiple centers to understand the experience of depression among patients with giant hydrocele from differing cultural backgrounds. The knowledge generated from these explorations will increase the potential for providing acceptable and appropriate health care to patients with giant hydrocele at risk for depression as well as patients in other circumstances.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.