
Abstract
Villamonte-Calanche, Wilfredo, Marco Antonio Salazar-Zegarra, Franklin Miranda-Solis, and María Jerí-Palomino. Correlation of uterine blood flow in the first trimester of pregnancy and birth weight at term in high altitude. High Alt Med Biol. 00:00–00, 2026.
Objective:
To determine the correlation between total uterine artery flow (UtAQ) at the end of the first trimester of pregnancy and birth weight (BW) at term at 3,400 m altitude.
Methods:
Prospective study, conducted at 3,400 m altitude in 210 women who underwent routine ultrasound evaluation. The inclusion criteria were singleton pregnancy between 11 and 14 weeks + 1 day, crown-rump length between 45 and 84 mm, born and raised at high altitude (native), and without pathology. The outcome was BW, expressed as a Z score. Variables such as UtAQ, uterine artery (UtA) diameters, age, body mass index, and mean arterial pressure, among others, were evaluated.
Results:
After applying the inclusion criteria, 203 pregnant women were evaluated, out of a total of 210 women. The average diameter of UtA was 0.27 cm, and the total bilateral UtA blood flow was 305.8 ml/min. A significant correlation was found between BW and UtAQ (rho = 0.15, p = 0.033), with a higher association for the left UtA (rho = 0.19, p = 0.007). Similarly, BW was positively correlated with the average diameter of the UtAs (r = 0.21, p = 0.003) and the association was stonger for the left UtA (r = 0.19, p = 0.006).
Conclusion:
In low-risk singleton pregnancies among native women living at high altitude, a correlation was observed between UtAQ and term BW, with the highest association found between BW and the diameter and UtAQ of the left UtA.
Keywords
Introduction
High altitude (HA) is defined as an elevation greater than 2,500 m above sea level (Julian and Moore, 2019). Globally, ∼80 million people reside in HA regions. In Peru, a country in central and western South America, about 11 million people (∼30% of the population) live at HA (Tremblay and Ainslie, 2021). Cusco, a city situated at 3,400 m in the southeastern Andes of Peru, exemplifies such environments. In HA cities, atmospheric and ambient oxygen partial pressures decrease, a condition known as hypobaric hypoxia (HH). In Cusco, the atmospheric pressure is ∼520 mmHg, while at sea level it is 760 mmHg.
Birth weight (BW) is dependent on fetal growth and gestational age of pregnancy. It is an essential anthropometric measure related to neonatal morbidity and mortality. HH has a direct adverse effect on fetal growth (Giussani et al., 2007), leading to lower BW in HA cities (Giussani et al., 2001; Jensen and Moore, 1997). This lower BW is associated with less fat tissue storage than lean mass in the fetus during pregnancy (Ferrazzi et al., 2011). Genetic variations in Andean pregnant women that influence maternal vascular responses to pregnancy—such as uterine artery (UtA) diameter and transcriptional activity—may protect against the adverse effects of HH on BW (Bigham et al., 2014). As a result, BW in Andeans is more comparable to that at sea level.
Oxygen and nutrients are transported from the mother to the fetus via the UtA, which increases the total uterine artery flow (UtAQ) from a mean of 94.5 ml/min in the previous pregnancy to a mean of 542 ml/min in late gestation at sea level (Thaler et al., 1990). Increased UtAQ in the first trimester has been associated with greater BW compared to the rest of pregnancy (McKelvey et al., 2017). This increase is primarily attributed to the enlargement of the UtA diameter (Dickey and Hower, 1995; Palmer et al., 1992). However, the relationship between first-trimester UtAQ and term BW in native HA populations remains unknown.
We tested the hypothesis that UAt blood flow in the first trimester at HA correlates with BW, as demonstrated in the second and third trimesters of pregnancy (Julian et al., 2008; Moore et al., 2011). Therefore, the aim of this study was to determine the correlation between UAt blood flow in the first trimester of pregnancy in low-risk, HA native women (born and raised at HA) with the BW of their term neonates at an altitude of 3400 m.
Methods
Ethical considerations
This study was conducted following international ethical guidelines. The research protocol was reviewed and approved by the Research Ethics Committee of the Cusco Healthcare Network (Note No. 64-CE-GRACU-ESSALUD-2022). Each pregnant participant in the study signed an informed consent form, and confidentiality of the information was maintained.
Study design and population
This study was a prospective observational cohort study conducted at the Research Institute of the Andina University of Cusco from July 2022 to August 2024. The study initially included 210 pregnant women. The inclusion criteria were low-risk, singleton pregnancies conceived spontaneously, born at altitudes greater than 2,500 m, with crown-rump length (CRL) between 45–84 mm and gestation of 11–14 weeks + 1 day. All participants delivered between 37 and 42 weeks at a hospital in Cusco city and experienced no pregnancy-related illnesses.
The sample size was calculated to detect a minimum correlation of 0.219 between UtA blood flow and BW, based on data reported by Hollis et al. (2003) The calculation was performed using Epidat 4.2, with a target statistical power of 80% and a 95% confidence level.
Analyzed variables
The UtAQ was calculated by summing the blood flow of each UtA, obtained using the formula π×r2×TA mean (Time-Averaged Mean Velocity) × 60, expressed in ml/minute. BW was converted to a Z score using the neonatal weight table (Villamonte-Calanche et al., 2019). Maternal age was considered as the number of years completed from birth to the time of evaluation. Ethnicity was determined based on the four surnames of the women’s parents (Chakraborty et al., 1989). If all surnames were of Quechua or Hispanic origin, they were defined as Quechua or Hispanic, respectively. If there was a combination of both, they were classified as mestizo. Menarche was defined as the age at which a woman had her first menstrual period. The total number of pregnancies included all prior pregnancies and the current one.
The number of living children was recorded, and miscarriages were defined as pregnancy losses occurring before 20 weeks of gestation. A history of preterm birth was noted if the woman had previously delivered a baby before 37 weeks of gestation. Blood pressure was measured according to the protocol described by Poon et al. (2012). Oxygen saturation and heart rate were measured twice on each index finger (right and left hand) using a digital oximeter, before blood pressure measurement; the average of the four readings was used. Weight and height were measured with minimal clothing using a Detecto® model 2,392 scale. Gestational age was reported in completed weeks, with 0.5 weeks added when appropriate, following the method recommended by Royston and Wright (1998). Hemoglobin levels were assessed in the first trimester using venous blood analyzed by a Sysmex XN-1000 hematology analyzer. A correction factor of –2.1 g/dl was applied to adjust for HA conditions at 3,400 m (WHO, 2024).
Procedure
Patients who voluntarily agreed to participate in the study and signed their consent form were asked to complete a questionnaire detailing their age, menarche, and other relevant information. Following this, their weight, height, and blood pressure were measured. Afterward, each participant was invited to use the restroom to empty their bladder and change into a gown. They were then positioned in lithotomy on a gynecological stretcher, and a 7.5 MHz transvaginal transducer, covered with a new prophylactic, was used for the ultrasound examination. The sonographic procedure was performed on a GE Voluson™ S10 ultrasound machine, configured for obstetric use. All ultrasound evaluations were conducted by the same operator (W.V.-C.), who was certified by the Fetal Medicine Foundation. After assessing fetal size and morphology, the transvaginal probe was placed in the lateral vaginal fornix. Color Doppler imaging was used to identify the UtA on both sides, near the internal cervical os. Pulsed Doppler was then activated, with the evaluation window set to 2 mm and an insonation angle maintained below 30° to ensure that more than three similar waves with a velocity greater than 60 cm/s were obtained. The TA mean and pulsatility index (PI) were measured automatically three times (Fetal-Medicine-Foundation, 2024). Next, the transducer was rotated to visualize the uterine artery longitudinally (Fig. 1). After optimizing the gain and image size on the screen, the UtA diameter was measured at the midpoint of diastole from the inner edge on one side to the inner edge on the opposite side. This measurement was repeated three times, and the average value was used. The intra-observer coefficient of variation was 6%.
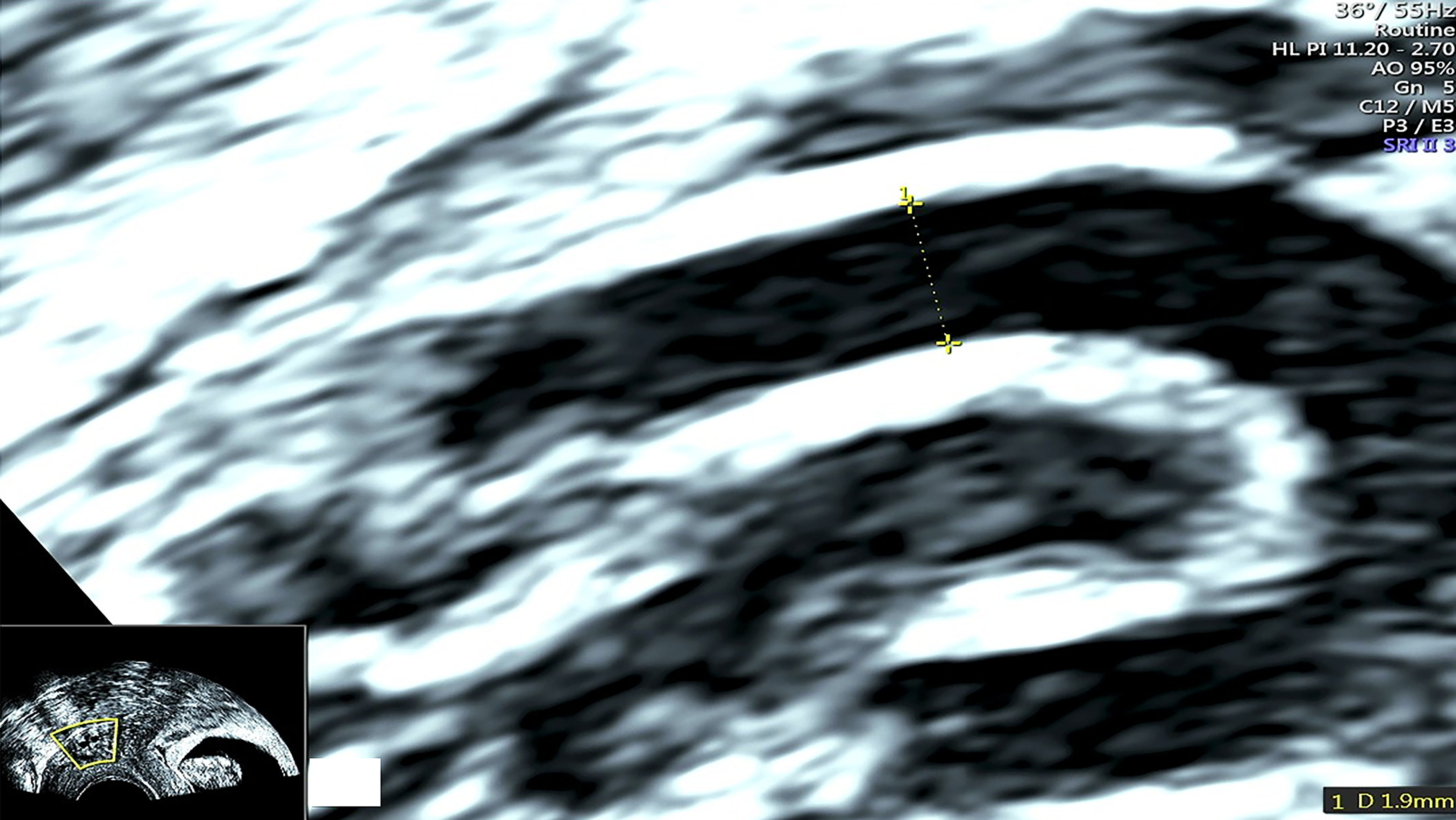
Measuring uterine artery diameter.
Finally, the medical records of the pregnant women were reviewed at the hospital where the delivery occurred to obtain delivery details and BW, which were recorded on a data collection form. All data were subsequently entered into a Microsoft® Excel electronic database.
Statistical analysis
All data were analyzed using the statistical package R, version 4.4.2. Categorical variables were described as absolute and relative frequencies. In contrast, quantitative variables were described using either the mean and standard deviation or the median and interquartile ranges, depending on whether the data followed a normal distribution, assessed using the Kolmogorov–Smirnov test. Fisher’s exact test or the Chi-square test was used for bivariate analysis between categorical variables. For quantitative variables, either the Student’s t-test or the Mann–Whitney test was applied. Additionally, a bivariate linear regression was performed, and the degree of correlation was assessed using Pearson’s or Spearman’s test, depending on the data distribution.
Results
Of the 210 pregnant women initially recruited, we excluded 7 (5 delivered before 37 weeks and 2 delivered at sea level). Finally, 203 pregnant women were evaluated, with an average age of 33.1 years. The median hemoglobin level was 12.4 g/dl. The body mass index was close to the upper limit of the overweight range, and the median crown-to-rump length was 69.2 mm. The average diameter of UtA was 0.27 cm, and the UtAQ was 305.8 ml/min (Table 1). A positive correlation was found between the term BW and UtAQ (rho = 0.15, p = 0.033) as well as between BW and the left UtA blood flow (rho = 0.19, p = 0.007). There was no correlation between right UtA blood flow (rho = 0.048, p = 0.5) and term BW (Fig. 2). Similarly, a positive correlation was observed between the average diameter of the UtA and term BW (r = 0.21, p = 0.003), which was maintained when evaluating the diameter of the left UtA (Fig. 3).
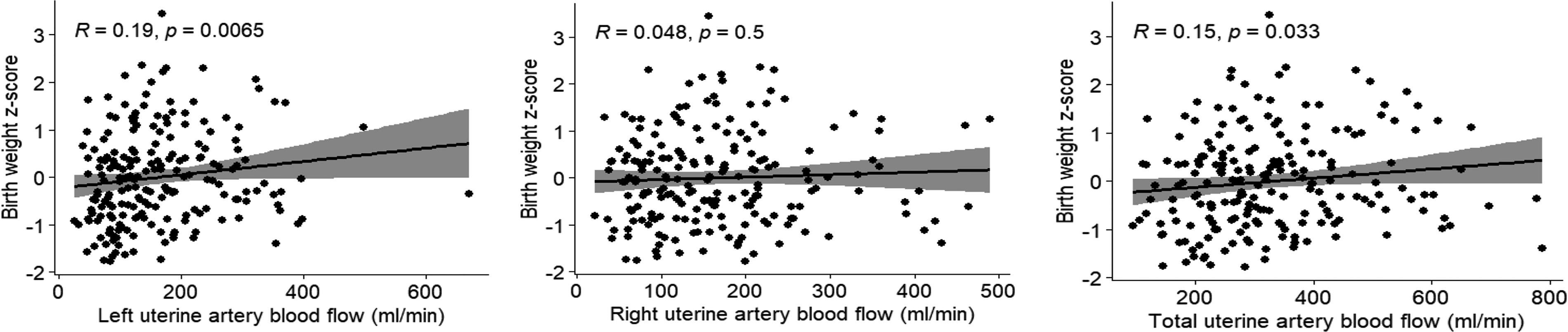
Correlation of total blood flow of the uterine arteries with birth weight at 3400 m altitude.
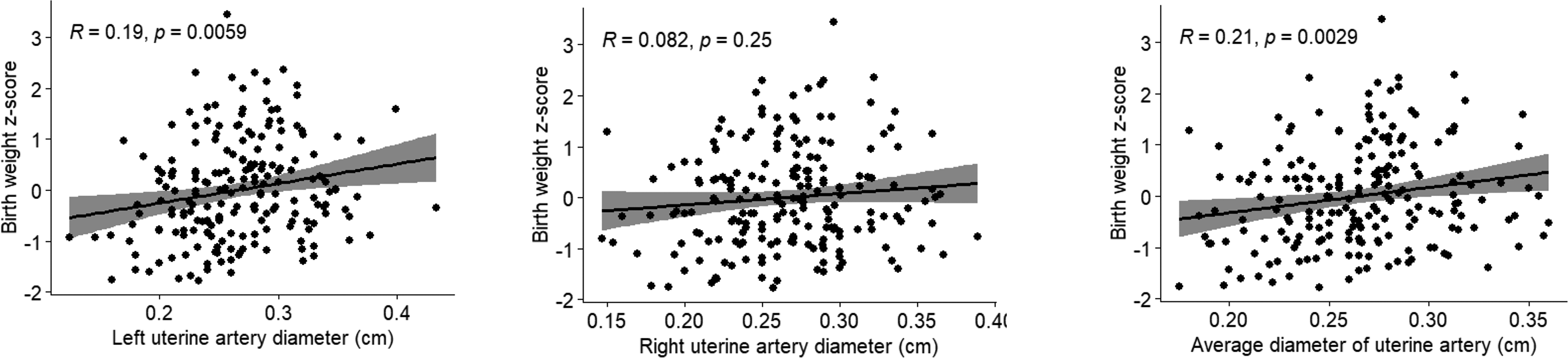
Correlation of the diameter of the uterine arteries with birth weight at 3400 m altitude.
Population Characteristics and Results of 203 Low-Risk Term Singleton Pregnancies at 3400 m Altitude
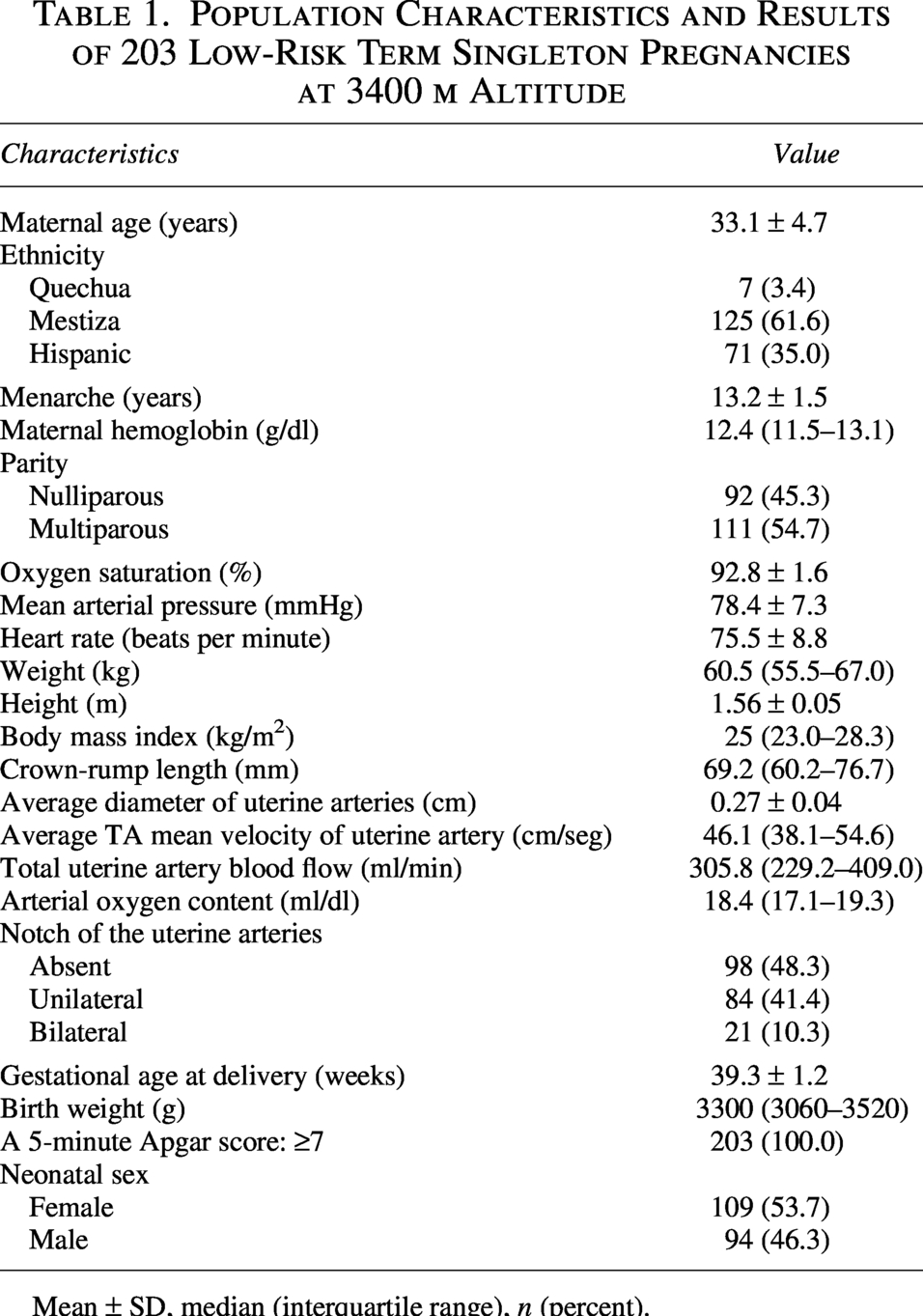
Mean ± SD, median (interquartile range), n (percent).
Discussion
At an altitude of 3,400 m, term BW was correlated with UtAQ, particularly with the flow and diameter of the left UtA. Doppler flowmetry in pregnant women at this altitude showed higher UtAQ (305.8 ml/min) and the absence of a diastolic notch (low level of flow resistance) in 48.3% of cases. Similar findings were observed from 20 weeks until the end of gestation in an Andean population in Bolivia (Julian et al., 2009). The relationship between ancestry and HH influences UtA dilation, as well as other physiological factors, such as a lower endothelin-to-nitric oxide metabolite ratio, which promotes increased blood flow in UtA.
HH leads to reduced fetal growth, which is reflected in a lower-term BW in HA cities compared to neonates at sea level. However, the impact of HH varies across populations. In Cusco, for instance, the average BW of term neonates is 121 g lower than at sea level (Villamonte et al., 2011). It contrasts with findings in Colorado, USA, where BW decreases by an estimated 121 g for every 1,000 m of elevation (Jensen and Moore, 1997). Fetal biometry data suggest that the altitude-associated reduction in BW is evident between 25 and 29 weeks of gestation, and becomes more evident by term (Krampl et al., 2000). Both the present and previous studies, in populations native to or newly arrived in HA, suggest that reduced UtA blood flow precedes detectable reductions in fetal growth, implying a potential causal relationship (Julian et al., 2008; Julian et al., 2009). The diminished blood flow is attributed to a reduced oxygen supply to the uteroplacental circulation, mainly because a smaller UtA diameter. Contributing factors include a relative deficiency of vasodilators compared to vasoconstrictors, such as endothelin (Julian et al., 2008), and increased blood viscosity (Kametas et al., 2004), often linked to elevated hemoglobin levels (Huamani et al., 2022). Consequently, UtAQ during the second half of pregnancy tends to be lower in HA populations than at sea level (Zamudio et al., 1995). This effect is notably more pronounced in populations of European descent residing at HA than native Andean populations (Jensen and Moore, 1997).
At sea level, systemic vasodilation, a 40% increase in blood volume, and an increase in cardiac output occur during pregnancy. The increase in vessel growth is likely the factor responsible for the increase in UtA diameter by the sixth week of gestation (Burchell, 1967)—before the completion of placentation—the increase in UtAQ during pregnancy results from an increase in vascular diameter and blood flow velocity. Vascular dilation predominates in the first half of gestation, while flow velocity becomes the dominant factor in the second half (Palmer et al., 1992). The increase in the diameter of UtA continues through the 20th week, after which it remains unchanged at sea level and in HA populations (Julian et al., 2008). However, a greater increase in UtA diameter has been observed in HA populations compared to those at sea level. It may help explain the larger fetal anthropometric measurements recorded between 15 and 22 weeks of gestation in Cusco, relative to sea-level populations (Villamonte et al., 2013).
Higher UtAQ during the first trimester has a greater impact on term BW than in later stages. For instance, a 100 ml/min increase in UtAQ during this period results in an additional 25 g of BW compared to the same increase in UtAQ at 24 weeks (Ferrazzi et al., 2011). Similarly, neonates with intrauterine growth restriction exhibit a reduction in UtAQ of ∼12% at 28 weeks and 37% at 38 weeks of gestation (Konje et al., 2001). By the end of pregnancy, a fetus weighing around 3,500 g requires a UtAQ of ∼841 ml/min, or about 235 ml/min per kilogram of fetal weight (Battaglia and Meschia, 2013; Moore et al., 2022). In the second half of pregnancy, UtAQ is inversely related to the PI of UtAs. Between 27 and 38 weeks, neonates with normal PI have higher UtAQ compared to neonates with appropriate or small-for-gestational-age with PI values above the two standard deviations (Ferrazzi et al., 2011). Additionally, higher UtAQ is associated with a longer gestational duration; for example, a 100 ml/min increase in UtAQ increases gestational duration by 0.98 days (McKelvey et al., 2017).
Notably, the diameter of the UtA on the placental side is, on average, 10.8 ± 2.4% larger than the contralateral artery (Konje et al., 2001). As a result, UtAQ on the placental side is approximately double that of the opposite side by term, a pattern that is also evident in the second half of gestation (Battaglia and Meschia, 2013; Rigano et al., 2010). A limitation of our study is the absence of data on placental location, which may account for the observed predominance of higher UtAQ in the left UtA.
In conclusion, there is a positive correlation between UtAQ and the diameter of the UtA—especially on the left side—and term BW in low-risk and high-altitude native pregnant women at 3,400 m altitude. These findings will serve as a basis for developing research projects to develop predictive models of fetal growth restriction during pregnancy at HA.
Authors’ Contributions
Contribution to conception or design: W.V.-C. and M.J.-P. Data collection: W.V.-C., M.A.S.-Z., F.M.-S., and M.J.-P. All the authors contributed to data analysis, prepared and revised the article, and have approved the final version.
Footnotes
Acknowledgments
The authors thank Professor Lorna Moore for her kind suggestions in preparing this article.
Author Disclosure Statement
All authors declare no conflicts of interest.
Funding Information
Andina University of Cusco.