
Abstract
Ellerton, John, Alison Sheets, Kyle McLaughlin, and Peter Paal. Rescue at Extreme Altitude: Managing the Ethical Considerations in the Language of Risk Management. An International Commission for Alpine Rescue Position Paper. High Alt Med Biol. 27:117–122, 2026.
Rescue from altitude has additional risks that require specialist knowledge, skills, and ability. Currently, rescue at extreme altitude (>5,500 m) is provided largely by ad-hoc teams responding to a need. The ethics of performing such rescues is controversial, and media coverage rarely considers the complexity of the environment. Organized mountain rescue teams have established processes to manage risk and their conduct to provide a professional service that changes the language of ethical decision-making into a practical, nuanced risk and crew resource management format. The International Commission for Alpine Rescue, along with the International Society of Mountain Medicine, has produced scientific papers on rescue at very high altitude and a position paper on the ethics of extreme altitude rescue. The aim is to improve the safety and outcomes of all rescues at altitude. The position paper, presented here, is targeted principally at those involved in extreme altitude rescue. Organized mountain rescue developed from ad-hoc rescue in response to a need; the same is likely to occur for extreme altitude rescue. Altitude is only one of the risk factors, and the knowledge of modern mountain rescue processes could aid in the advancement of extreme altitude rescue.
Introduction
Mountain rescue operations are being conducted at higher altitudes because of improved equipment, better communications, and increased knowledge. Rescues up to 5,000 m have become routine in many mountain areas and are becoming more common at extreme altitudes (>5,500 m). There are currently no established protocols for managing these rescues, and practice varies across the world.
The rescues at extreme altitudes may involve purely companion rescue, but often there are elements of a more complex system involving multiple agencies and transport modes. In addition, facilitation of a rescue effort may include administrative services and financial support from remote stakeholders such as an embassy, an insurance company, or the relatives of those involved. Not all such stakeholders may be familiar with the inherent risks and limitations involved in rescue.
With increasing altitude, multiple physical, physiological, psychological, meteorological, cultural, and economic factors complicate operations. However, there’s no reason to suggest that rescue will become inevitably impossible above any one numeric altitude. It’s the host of features that determine the risk, so a specific altitude alone cannot adequately define an unacceptable risk. Media interest in extreme rescue is significant. Their reports can focus on sensational aspects of the rescue at the expense of a nuanced and balanced appraisal. The ethics of decisions made under duress are often remotely dissected.
In response to these developments, the International Commission for Alpine Rescue (ICAR), along with the International Society of Mountain Medicine (ISMM) and practitioners in the field, set a goal of collecting knowledge on high-altitude rescues in order to improve the safety and effectiveness of the mission regardless of the entity—organized, ad hoc, improvised, military, governmental, sole providers, etc.—that performs the rescue. The scope of this position paper is the practical management of the ethics of rescue based on the input of experts, practitioners, and rescue specialists.
Methods
Between October 2022 and October 2025, the subject was discussed by members of ICAR at meetings and on its forums. A working group was formed, and members reached out to contacts outside ICAR who were known to be involved in rescue at altitude. They were invited to join the working group. The final draft was written by J.E. based on consensus and sent to all members of the working group for their comments. The Assembly of Delegates of ICAR endorsed the conclusions of the paper.
Limitations and Constraints
An important limitation of the paper is that legal and governmental obligations and duties, whether civil law or case (common) law-based, are excluded from our considerations. A legalistic approach to mountain rescue can be seen in a chapter in “Mountain Rescue and Technical Rescue” (Knutson, 2016). This contrasts with a philosophical approach taken by others (Iserson and Morenz, 2007). We acknowledge that both approaches operate together and that ideally a settled, coherent framework with enshrined governance should evolve. However, even a superficial enquiry in the international rescue field highlights ethical dilemmas and conflicts along with the imposition of political factors. For example, the fate of migrant boats in the Mediterranean has not been resolved (Mann, 2020). We justify applying this limitation by contending that organized mountain rescue has been more significantly influenced by a practical philosophical standpoint than by the application of Law.
We also acknowledge that this paper, despite its best intentions, has been most heavily influenced by an English-speaking group of mountain rescuers operating in an organized mountain rescue system. However, crucial points have been influenced from expedition, commercial, and indigenous rescue groups.
As an organized rescue service, we have learnt that dogmatic statements as to how to do things are not the best way of helping fledging rescue systems. Giving information for it to be discussed and adapted to meet the local situation suits the complexities of rescue. Hence the reader will not find simple instructions in this paper; indeed, organized mountain rescue may not find new information but will find much to contemplate.
Our deliberations are restricted to mountain rescue. Other environmentally extreme rescues have similar dilemmas. Examples include the Thai “football team” cave rescue, maritime incidents, and natural and man-made disasters. Further consideration of these may be beneficial in the future.
Discussion
Moral and ethical considerations
Moral and ethical considerations distinguish the difference between “good and bad” or “right and wrong.” Moral values, such as empathy and compassion, connect people from different cultures, each with their different ethical rules. People will have their own obligatory ethical rules and supererogatory (encourage to do but non-obligatory) norms. It is clear in the literature that there is disagreement, and few, if any, simple statements can be made that could guide a person or organization in rescues at altitude (Miller, 2020. Miller, 2022. Jecker and Derse, 2017. Jecker, 2015). It is frequently stated that there is an accepted ethical duty to rescue if there is minimal cost or inconvenience to the potential rescuer (Rulli and Millum, 2016). The “Duty of Easy Rescue” can be illustrated in a scenario where a bystander, passing a shallow pond no deeper than their knees, sees a child at risk of drowning. In this situation, the potential benefit of saving a life outweighs the inconvenience of getting their clothes soiled and losing time. The literature suggests that this ethical rule is universal in all cultures. A mountain-equivalent scenario could be: You are clipped on a fixed line descending to a camp and see a person also descending but at risk of falling, as they are unable to clip on as their hands are non-functioning from having lost their gloves. You ask them if they want to be clipped on, which they do. You clip them on and put your spare gloves on their hands. You follow them down, doing the same action as anchor points are reached. Your journey is prolonged by a few minutes, and you can recover the gloves you lent at the camp.
There are several discussion points before we can accept the “Duty of Easy Rescue.”
(1) How much cost—physically, mentally, financially, or risk—is minimal, and does that change depending on what you are doing? Authors have argued that: If the potential rescuer has voluntarily and knowingly accepted an assumed level of risk equal to the risk of performing a rescue and the original pursuit of the rescuer is less morally important than the rescue itself, then the duty of rescue persists. Imagine the mountain scenario above: What if you are ascending to the summit and the rescue involves descending instead? For a bystander, some authors argue that there is no compulsion or obligatory duty to turn back even though the original goal of summiting is less important than saving another person’s fingers or reducing the risk of falling with its range of outcomes. The uncertainty of making a tangible difference to the outcome is considered a reasonable consideration in determining your actions. Even the realization of the risk you have now encountered could be adequate for you to decline becoming involved; you had not been fully informed of the risk before the incident.
(2) What is the scope of the duty? Even minimal cost multiplied by many is not insignificant, particularly when a resource is limited. During the period May 1975–2006, atleast one death occurred on Everest on 31% of days when mountaineers reached the summit (Firth et al., 2008). It is difficult not to conclude that the burden of minimal inconvenience, as described in the “Rule of Easy Rescue,” has been breached. You would hope society would act in such a situation. However, society’s perspective may be that one “problem” can’t be prioritized over other similar emergencies. Could the cost be spent more effectively on other programs that improve more lives in the community? Cost benefit analysis may lead to downgrading of rescue operations to a social value judgement that, though carrying a strong symbolic value to the community, is not an obligation. Rescue is not a human right (Findler, 2021). Other authors have pointed out that a potential rescue is not a single act performed by an individual. Instead, it involves a series of actions, such as an extrication, assessment, treatments, and evacuation, among others. Some of these actions may lie within a “Duty of Easy Rescue,” others may be part of a harder rescue, and other actions may be beyond reason (Reichling, 2022). For some persons on the fixed line, not summiting may be a blow to their ego; for subsistence mountain workers, it may be financially crippling. These complexities are difficult to convey in a binary decision and at the root of why the organized rescue community is reluctant to judge others on their rescue decisions.
The people
Mountain workers are a heterogenous group that includes porters, camp assistants, local and international guides, and support staff. They are the backbone of high-altitude tourism. They span the whole breadth of socio-economic, status, religious, and educational spectrums. Almost half the deaths on Everest are in the subsistence mountain workers. In addition, an untold number will have suffered morbidity. Yet their voice and opinions are rarely heard; their work is extremely precarious, and justice (representation, dignity, and recognition) is almost certainly tainted by their post-colonial and indigenous mountain status (Wilson and Dashper, 2023). Inequality in health care and rescue provision has been questioned (T. Küpper et al., 2012).
Customers, at first sight, would seem to be less heterogenous. Most are tourists buying a product. Many will originate from more affluent regions and may be engaged in a goal-driven or a ‘once in a lifetime’ challenge. Motivation, fueled by money, time, social media presence, and a host of other factors, may cloud their mountain appreciation and situational awareness. Forming a relationship with the mountain and its workers, as demonstrated by the writings of John Muir and Nan Shepherd, may not be prioritized (Muir, 1901. Shepherd, 2011). Indeed, it has been said that even moral duties can be suspended at extreme altitude, and the age of fellowship of the rope is past (Findler, 2021). The spectrum of personal and group behavior that results is as wide as is imaginable. Indeed, when you consider the multitude of non-tourist clients engaging in pilgrimage to altitudes, then perhaps a better understanding of societal needs could be made (Basnyat, 2014).
Professionals with relevant technical and medical skills have more stringent duties to perform a rescue compared to a bystander. This seems an accepted norm and applies to all such persons in proximity to a rescue and persists whether the professional is present in a voluntary or paid capacity. The degree of commitment may vary depending on whether the relationship is deemed to be contractural. For example, a paid mountain guide and a commercial guiding company will have a ‘Duty of Care’ for their client, which could include a duty to rescue. This may be defined in a contract or by a regulatory body (BAMG, 2016. AMGA, 2013). The limitations may or may not be defined explicitly. For example, the American Mountain Guides Association says in its Code of Ethics and Conduct:
“Managing risk and the welfare of our clients is our prime concern. Where possible and practical, we should provide assistance to persons having difficulty by offering help that is appropriate under the circumstances. In providing assistance to others, we should avoid compromising the welfare of our clients.”
There is very little peer-reviewed literature on how stringent or how risky a rescue has to be before an obligation becomes supererogatory (“beyond the call of duty”) for professionals.
One would expect that, at a minimum, the duty would be measured against a like-minded group of peers and cognizant of the effects that equipment and training have on risk. Extrapolating from examples given in the non-mountain environment; performing an “easy” rescue on a prepared fixed-line route even at extreme altitude, where risk can be managed and a significant improvement in outcome is probable, might be regarded as the norm though supererogatory. However, performing a multi-agency rescue on an unclimbed peak in the next valley, where risk and inconvenience would be considered greater, would, to many observers, be beyond the call of duty. Health Care Providers involved in “ad hoc” rescues may have unfamiliar duties of care and be confronted with problems outside of their usual scope of practice. Their usual moral responses are challenged by a plethora of additional factors that may give rise to internal conflict and distress (Zientek, 2020).
Organized mountain rescue
Organized mountain rescue typically arises in response to anticipated or actual recurring search and rescue needs in a specific geographical area (Agazzi, 2021). Whether voluntary or paid, they will have an established “Duty of Care” both at an individual and organizational level. Society’s contracts with rescue organizations, whether written or not, often prioritize risk assessment over moral values. Situational, geographical, and politico-societal factors contribute to practical considerations, making self-guided development crucial. The characteristics of a modern organized mountain rescue organization are summarized in Table 1.
The Characteristics of an Organized Mountain Rescue Team Include Most of the following
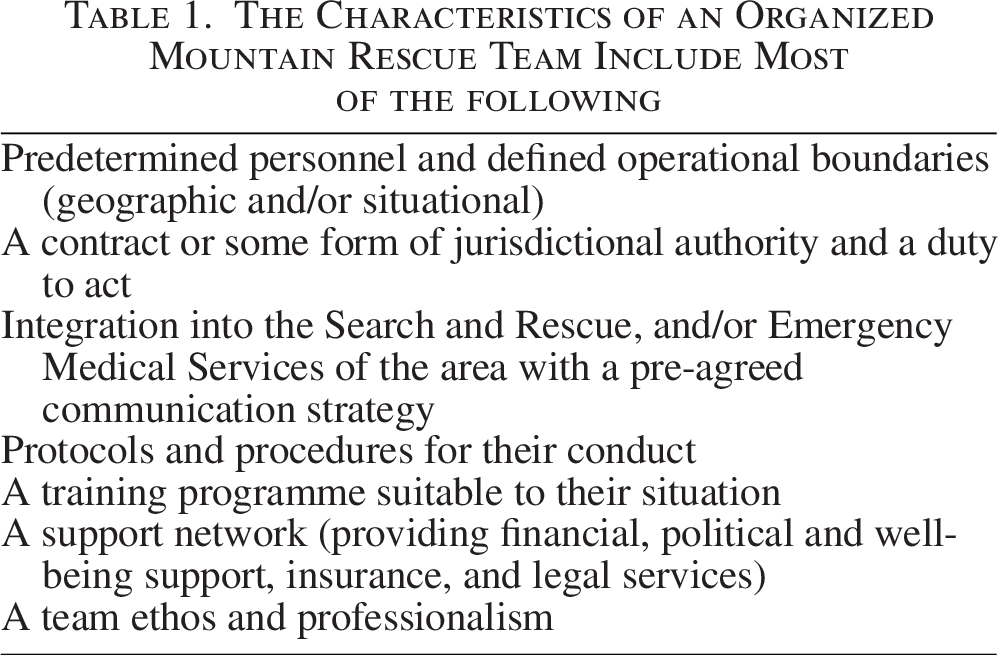
Organized mountain rescue sees the development of rescue from altitude, including extreme altitude, as no different than its historic progress. Though often in a vastly different socio-political environment, developing teams could assimilate the learned experience of organized mountain rescue, as altitude per se is just an additional risk factor to the mission’s overall complexity.
Challenges of rescue at altitudes
Altitude’s inherent challenges, including cold temperatures, extreme weather, and lower oxygen levels, affect rescue missions for both victims and rescuers. Helicopter performance diminishes in thinner air, and terrestrial rescue may be impossible. Planning, training, design, acclimatization, and equipment can partially mitigate these constraints (McLaughlin et al, 2025a; McLaughlin et al, 2025b).
At high altitudes, people push against environmental challenges with a strong motivation to keep going. Mental toughness, the ability to overcome failures or obstacles by staying positive and competitive, is a key psychological trait among high-altitude mountaineers (Crust et al., 2016). Cognitive function is reduced in an unacclimatized person acutely exposed to extreme altitude; it improves, to some extent, on acclimatization, though evidence is very limited (Griva et al., 2017. Bliemsrieder et al., 2022). A person’s ability to carry out a risk assessment is not known (Jackman et al., 2023). Understanding the psychological state of both victim and rescuer is important, as their state can impact on their resilience and decision-making. Evidence of the psychology states of the subsistence mountain workers is entirely absent (Dawadi et al., 2020).
More people are travelling to extreme altitude. For example, the number scaling Everest has increased from an average of under 100 persons a year before 2000 to over 300 per year by 2010 and since 2021 to over 500 persons a year (Himalayan Database, 2024). New challenges can be envisaged as the speed of ascent increases and schedules become more convoluted (Benavides, 2025).
With improvement in cellular and satellite communications, calls for help and rescues are reported during or shortly after the event. Extreme altitude rescue is reported, at least in its initial phase, in a binary fashion. For example, in 2023, news was made by a heroic Nepalese sherpa carrying a stricken Malaysian climber from the balcony on Everest (8,400 m) back to the South Col and then, with others, using a stretcher to lower him to Camp 3 (7,162 m), where a helicopter, using a longline technique, completed the evacuation (Reuters, 2023). Subsequent statements from the guiding companies have added nuances to this remarkable rescue and demonstrate a control and command function (Muzaffar, 2023).
Two months later, a Pakistani porter was fixing ropes in the bottleneck area of K2 at about 8,200 m. He fell and was injured. He died a few hours later at the scene. Climbers went to his assistance. Some climbers then continued to the summit, including a Norwegian climber and her Nepalese guide. By summiting, they established the record for the shortest time to complete all 14 summits above 8,000 m. The mountaineer has reported receiving death threats and has retired from mountaineering. She has said: “I’m sure that if it was possible that we saw a chance to carry him down from there, everyone would have tried that. But it was impossible” (Drake, 2023). A subsequent investigation by the regional government criticized the expedition company for the equipment given to the porter, for hiring him as he was inexperienced, and for not having insurance in place. The company was banned for 2 years from operating on the mountain (Benavides, 2023).
As mountaineers, we have been here before. David Sharp’s death high on Everest in 2006 divided mountaineers, with Ed Hillary saying: “you have a duty, really, to give all you can to get the man down, and getting to the summit becomes very secondary.” Others disagreed with that view; they contended that rescue was impossible or futile, and it was everyone for themselves in the Death Zone. Hard on the heels of this story was the miracle of Lincoln Hall; left for dead, he survived a night out in Everest’s death zone and was rescued the following morning. The UIAA Declaration on Mountain Ethics and the Tyrol declaration were published in 2009 (UIAA, 2016). The relevant section says: “All participants in mountain sports … need to be ready to help others in the event of an emergency or accident and also be ready to face the consequences of a tragedy.” The last phrase could mean foregoing a summit bid, but there are other interpretations. The 2024 UIAA Declaration on Hiking, Climbing, and Mountaineering expresses ethical principles in the following sentiments: “We will always try to help others… in distress; … We ensure that injured parties are safe from objective dangers; … we alert rescue services …; we do not sensationalize these events but treat them with respect. …; We give all possible assistance to local inhabitants in need” (UIAA, 2024).
Practical application
In the context of rescue at extreme altitudes, we can consider the published circumstances surrounding the David Sharp incident mentioned above and imagine how an organized rescue system might manage the situation. (Supplemental Data) The aim is to encourage discussion, particularly in emerging rescue organizations.
Conclusion
Rescue from extreme altitude has additional risk that requires specialist knowledge, skills, and ability.
Media coverage of rescue at extreme altitude has flourished; it is often unhelpful and rarely takes into consideration the complexity of the environment.
The ethics of performing a rescue at altitude, and particularly at extreme altitude have been discussed but are incomplete. The limitations described by a “Duty to Rescue” may well be breached in high-frequency rescue hotspots.
Organized rescue has established general rules and protocols to manage risk and their conduct to provide a professional and unbiased service. These rules are increasingly explicitly written. Many organizations may not have reached this stage but most recognize that the ethics of rescue are incorporated in their operations. When appropriate, specific consideration of altitude should be a routine part of this process and is essential for teams working at extreme altitude.
ICAR is producing papers based on the literature and expert opinion to inform on the current technical and medical aspects of rescue at very high and extreme altitude. These will be freely available.
Organized mountain rescue almost always developed from improvised “ad hoc” community needs. The impetus for the change may have involved the burden of rescue becoming significant as well as other factors such as regulations and increasing sophistication.
Improvised rescue at altitude may benefit from the influence of organized rescue principles. Policy makers, commercial enterprises, professional associations, developing rescue systems, as well as guides, expedition members, and clients could benefit from the knowledge of organized rescue and adapt systems for their purposes.
Footnotes
Acknowledgments
The concept of the paper was conceived by John Ellerton. The first draft was produced by the authors. ICAR MedCom and ISMM members were involved in the formulation and discussion of the paper. The authors particularly acknowledge the contributions of Giancelso Agazzi, Italy; Hermann Brugger, Italy; Sebastián Donato, Argentina; Marika Falla, Italy; Maurizio Folini, Italy; Niels Holthof, Switzerland; Raimund Lechner, Germany; Andrew Luks, USA; Kazue Oshiro, Japan; Monica Piris, UK; Dick Price, New Zealand; George Rodway, USA; Steve Roy, Canada; Will Smith, USA; Giacomo Strapazzon, Italy; Iztok Tomazin, Slovenia; and Ken Zafren, USA.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for the production of the paper.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.