
Abstract
Objective:
Minimally invasive cardiac surgery for mitral valve (MV) disease is a rising strategy. Axillary access is linked to reduced pain and faster recovery, but its efficacy and safety compared with median sternotomy for MV surgery (MVS) remain unclear. We conducted a meta-analysis comparing the clinical outcomes of MVS via axillary access and median sternotomy.
Methods:
Four databases were analyzed. The primary endpoint was perioperative mortality. Secondary endpoints included cardiopulmonary bypass (CPB) and cross-clamp times, rethoracotomy, wound complications, mechanical ventilation duration, stroke, hospital and intensive care unit (ICU) stay, and residual moderate mitral regurgitation. A random-effects model was used.
Results:
We included 2,129 patients from 4 studies, with 1,135 (53.3%) undergoing axillary access. Perioperative mortality was comparable between approaches (odds ratio [OR] = 0.34, 95% confidence interval [CI]: 0.09 to 1.23, P = 0.10). Axillary access was associated with longer CPB times (mean difference [MD] = 16.38, 95% CI: 6.42 to 26.34, P = 0.001), fewer wound complications (OR = 0.41, 95% CI: 0.21 to 0.80, P = 0.009), shorter ventilation time (MD = −4.93, 95% CI: −8.79 to −1.08, P < 0.01), and shorter hospital (MD = −0.78, 95% CI: −1.41 to −0.14, P = 0.02) and ICU stays (MD = −10.84, 95% CI: −19.54 to −2.14, P = 0.01). No difference was found in cross-clamp time, rethoracotomy, stroke, or residual mitral regurgitation.
Conclusions:
Axillary access for MVS shows comparable mortality to median sternotomy, with benefits in wound complications, ventilation, and recovery but longer CPB times. Further research is needed to confirm long-term safety and efficacy.
This is a visual representation of the abstract.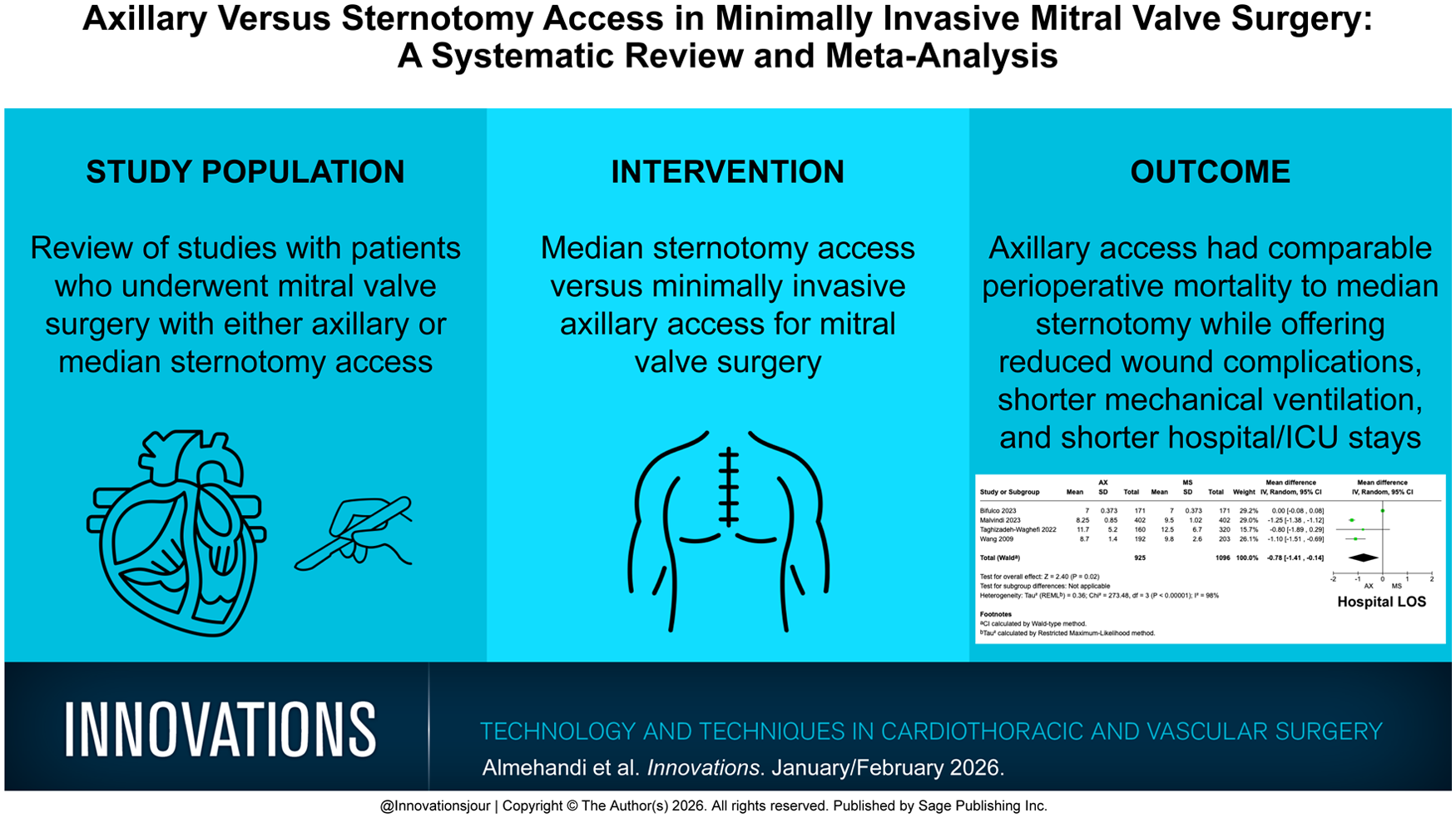
Central Message
Axillary access in minimally invasive MVS is associated with comparable perioperative mortality, shorter hospital and ICU stays, and fewer wound complications compared with median sternotomy, despite longer CPB times. These findings support axillary access as a safe and effective alternative, particularly for centers experienced in minimally invasive techniques.
Introduction
Traditionally, isolated mitral valve surgery (MVS) has been performed with a median sternotomy (MS). However, patient needs for shorter hospital stays, fewer postoperative complications, and better cosmetic outcomes have driven interest in minimally invasive procedures. Growing evidence suggests that minimally invasive cardiac surgical techniques are associated with quicker recoveries, fewer complications, and reduced pain while improving esthetic outcomes.1–7
The axillary approach for minimally invasive MVS involves a single 4 to 6 cm incision typically made along the right anterior axillary line at the fourth intercostal space,8–11 although variations exist. For instance, Wang et al. describe a right vertical infra-axillary incision spanning the third to fifth intercostal spaces (7 to 10 cm), with positioning influenced by patient anatomy. 12 Collectively, these studies define the axillary region as encompassing both anterior axillary8,10,11 and infra-axillary incisions, situated between the midaxillary and preaxillary lines (Supplemental Fig. 1). 14 This differs distinctly from the anterolateral minithoracotomy, in which incisions are placed at the border of the pectoralis major muscle or near the right nipple, 12 a more medial/anterior location. Although the axillary approach (including its infra-axillary variant) prioritizes lateral access to minimize scarring and muscle disruption, the anterolateral technique traverses pectoral structures. For clarity, this article uses the term axillary to refer broadly to the axillary anatomical region, distinguishing it from nonaxillary anterolateral thoracotomies. 12
Despite its advantages, the adoption of the axillary technique has been slow due to its complexity, steep learning curve, and requirement for specialized instruments. Given the scarcity of meta-analyses comparing the postoperative outcomes of axillary access with MS in the context of MVS, this article aims to quantitatively analyze the available data and determine which approach provides possibly superior clinical outcomes.
Methods
Ethical approval of this analysis was not required as no human or animal subjects were involved. This review was registered with the National Institute for Health Research International Registry of Systematic Reviews (PROSPERO, CRD42024614501).
Search Strategy
We performed a comprehensive literature search to identify contemporary studies reporting short-term outcomes between patients who underwent MS and axillary access for minimally invasive MVS. Searches were run in August 2024 in the following databases: Ovid MEDLINE, The Cochrane Library (Wiley), Embase, and Web of Science. The MEDLINE complete search strategy is displayed in Supplemental Table 1.
Study Selection and Data Extraction
The study selection followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) strategy. After de-duplication, records were screened by 2 independent reviewers. Any discrepancies and disagreements were resolved by a third author. Titles and abstracts were reviewed against predefined inclusion and exclusion criteria. Studies were considered for inclusion if they were written in English and reported a direct comparison between patients who underwent MS and axillary access in minimally invasive MVS, including clinical outcomes of interest. Endoscopic cases, animal studies, abstracts, case reports, commentaries, editorials, expert opinions, conference presentations, review articles, and studies not reporting the outcomes of interest were excluded. The full text was pulled for the selected studies for a second round of eligibility screening. References for selected articles were also reviewed for relevant studies not captured by the original search. Risk of bias was assessed based on ROBINS-1. 13
Two reviewers independently performed data extraction. Accuracy was verified by a third author. The extracted variables included study characteristics (publication year, country, sample size, study design, presence or absence from population adjustment, and reported outcomes) as well as patient demographics (age, sex, body mass index [BMI], hypertension, coronary artery disease, stroke, diabetes, smoking, atrial fibrillation, New York Heart Association [NYHA] class, left ventricular ejection fraction, and EuroSCORE II).
Outcomes
The primary outcome was perioperative mortality. Secondary outcomes were cardiopulmonary bypass (CPB) and cross-clamp time, early (30-day) rethoracotomy, wound complications, duration of mechanical ventilation, stroke, and hospital and intensive care unit (ICU) stay.
Statistical Analysis
We conducted meta-analyses to compare the outcomes of MS and axillary access in minimally invasive MVS. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated for each outcome. An OR greater than 1 indicated that the outcome was more frequently present in the MS arm. Continuous variables were analyzed using mean difference (MD) and 95% CI. An MD greater than zero corresponded to larger values in the MS arm. Inherent clinical heterogeneity between the studies was balanced via the implementation of random effects models (DerSimonian–Laird). Results were displayed in forest plots. The alpha error was set to 0.05.
Between-study statistical heterogeneity was assessed with the Cochran Q statistic and by estimating I2. High heterogeneity was confirmed with a significance level of P < 0.10 and I2 of at least 50% or more. All statistical analyses were performed using Review Manager 5.3 (The Cochrane Collaboration, London, United Kingdom).
Results
Study Characteristics
A total of 3,323 studies were retrieved from the systematic search, of which 4 met the criteria for inclusion in the final analysis.8,12,15,16 Figure 1 shows the PRISMA flowchart for study selection. Included studies were published between 2009 and 2023, and all studies were observational single-center cohorts. Table 1 shows the details of the included studies. A total of 2,524 patients were included in the final analysis. The number of patients in each study ranged from 160 to 667.
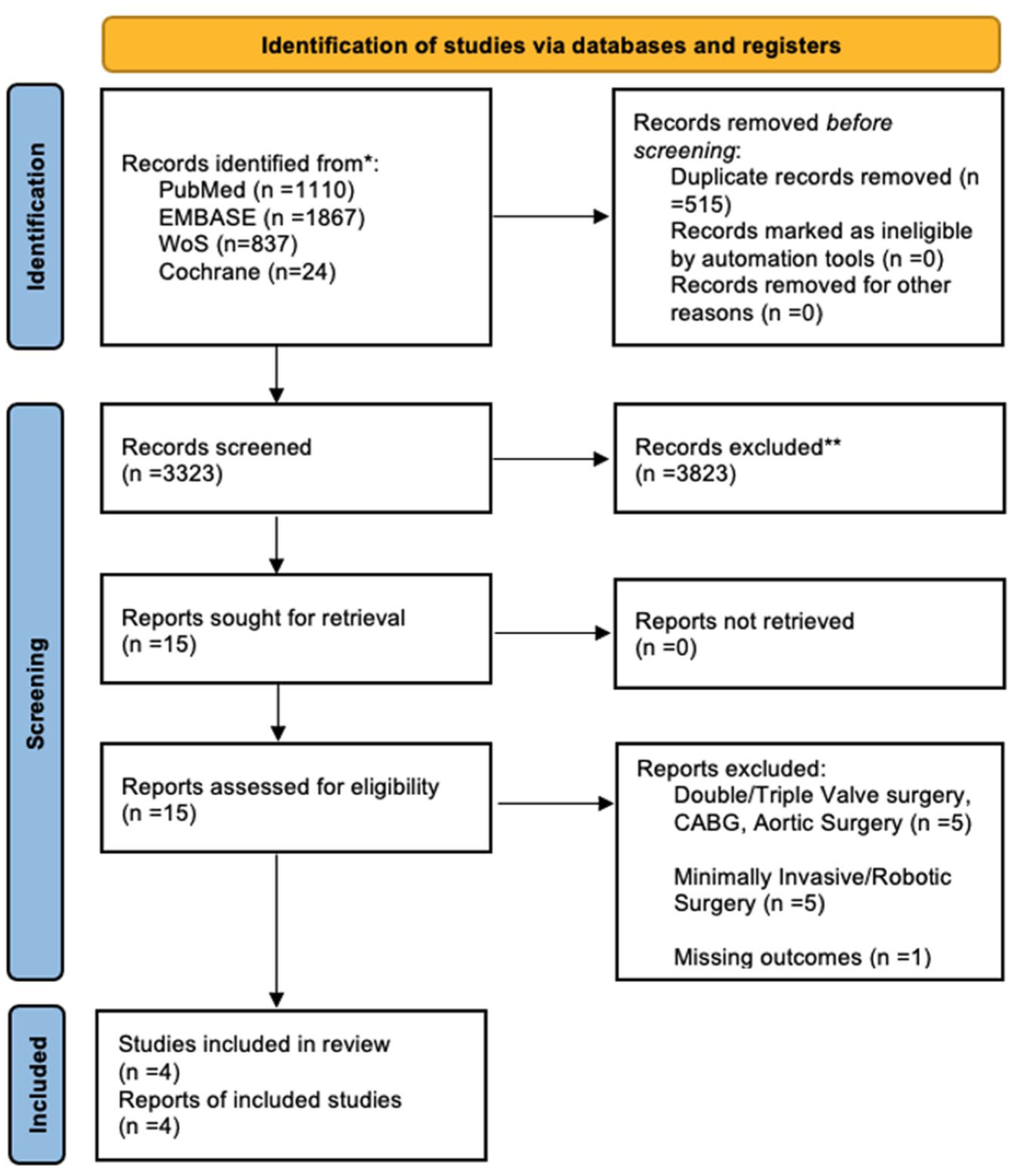
PRISMA flow diagram for study screening.
Summary of Included Studies.
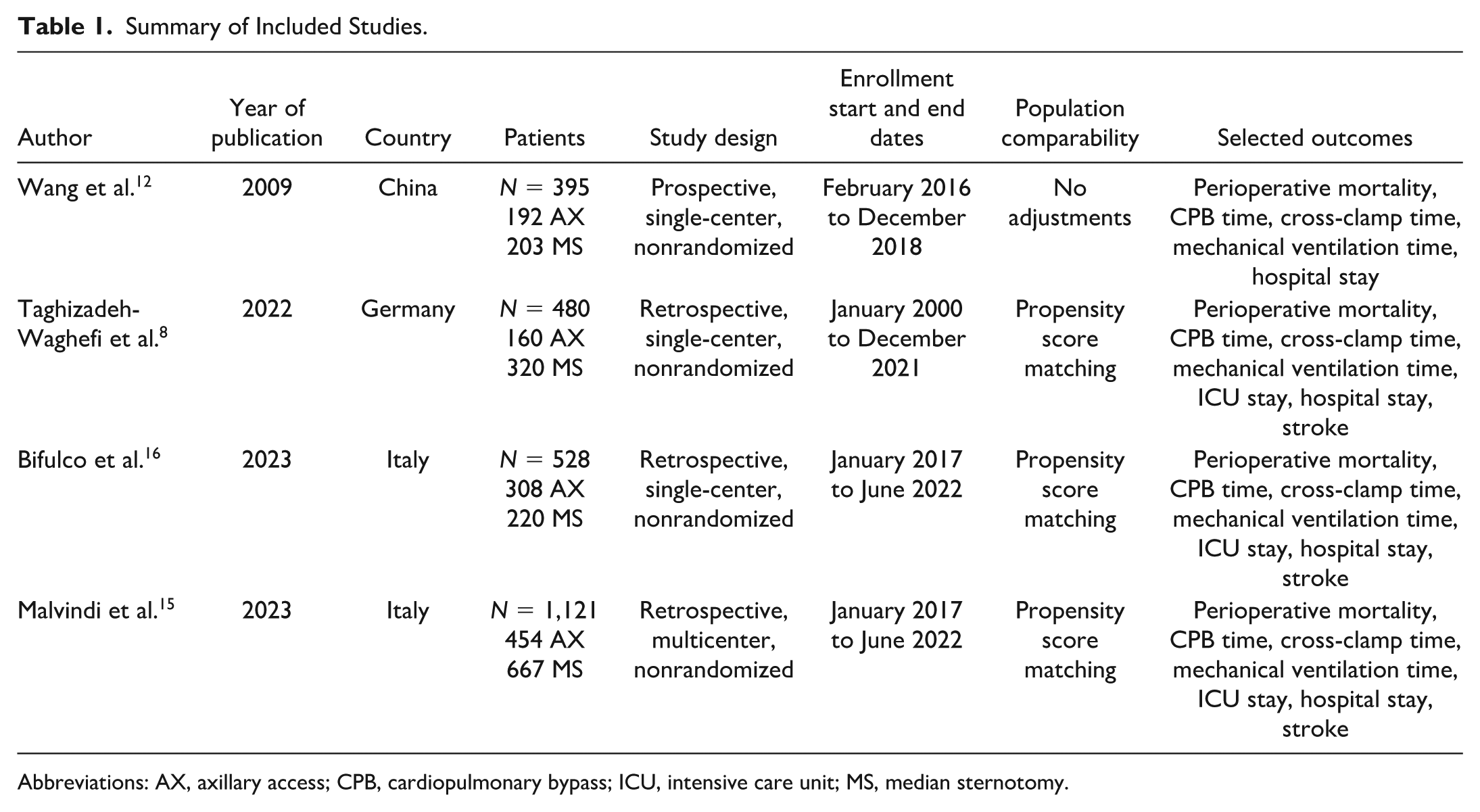
Abbreviations: AX, axillary access; CPB, cardiopulmonary bypass; ICU, intensive care unit; MS, median sternotomy.
Patient Characteristics
Supplemental Table 3 summarizes the demographic data of the patient population in each study. The mean age of patients ranged from 37.5 to 67.2 years, and the proportion of female patients varied between 40.9% and 68%. Notably, the mean ages in both cohorts from Wang et al. 12 were significantly younger than those reported in the other 3 studies. This age difference was associated with distinct MV pathologies observed in their population. The mean BMI ranged from 24.9 to 26.5 kg/m². Hypertension prevalence ranged from 52.3% to 77%, and coronary artery disease was reported in 5% to 27.8% of patients. The percentage of patients with a history of stroke ranged from 1.6% to 4%, diabetes prevalence ranged from 6.8% to 21.6%, and smoking prevalence ranged from 9.8% to 20.5%. Atrial fibrillation was observed in 22.7% to 42.8% of patients, and 19.8% to 65.6% were classified as NYHA class ≥ III. Left ventricular ejection fraction ranged from 50% to 61.4%, and EuroSCORE II values ranged from 1.13% to 2.0%. MV regurgitation was a commonly reported pathology, ranging from 81% to 100% in 3 of 4 studies. In terms of MVS, with the exception of Wang et al., 12 most patients in the other 3 studies underwent MV repair ranging between 64% and 100%.
Consistent with the younger mean age of patients in its cohort, rheumatic valve disease predominated in the Wang et al. study cohort, accounting for 95.3% of cases in the axillary group and 94.6% in the sternotomy group, whereas degenerative disease represented only 4.7% and 5.4%, respectively. 12 This aligns with the expected epidemiology of MV disease, as rheumatic etiologies are more prevalent in younger populations compared with age-related degenerative pathologies. In the Wang et al. study population, mitral valve physiology—primarily mitral stenosis (28.6% to 30.1%), insufficiency (31.5% to 31.8%), and mixed lesions (38.4% to 39.6%)—reflected the complex presentations of rheumatic disease, contrasting with isolated degenerative pathologies seen in older cohorts and reinforcing the association between younger age and rheumatic etiology. 9 Finally, none of the axillary procedures reported in all 4 studies were done endoscopically.
Primary Outcome
Table 2 outlines the detailed results of the meta-analysis. Figure 2 shows the forest plot for perioperative mortality, which was reported by 4 studies including 2,021 participants. Perioperative mortality rates were comparable between the 2 groups (OR = 0.34, 95% CI: 0.09 to 1.23, P = 0.10).
Outcomes Summary.
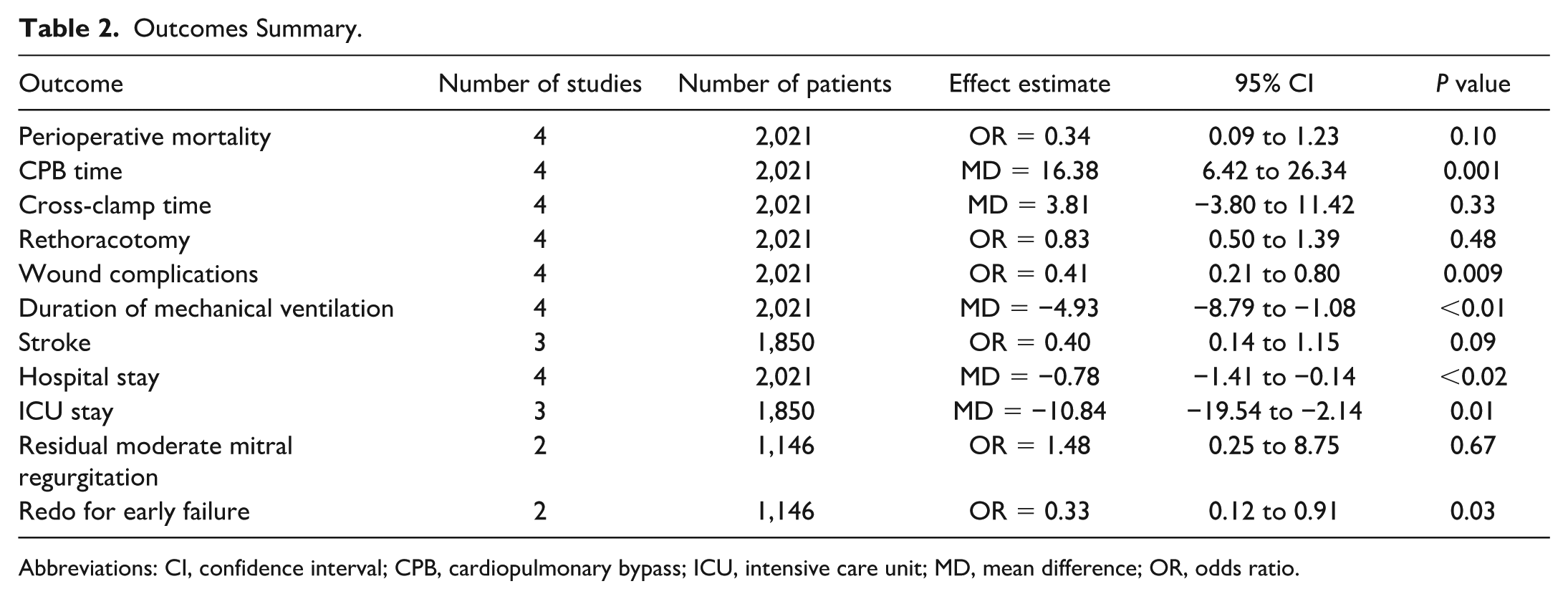
Abbreviations: CI, confidence interval; CPB, cardiopulmonary bypass; ICU, intensive care unit; MD, mean difference; OR, odds ratio.
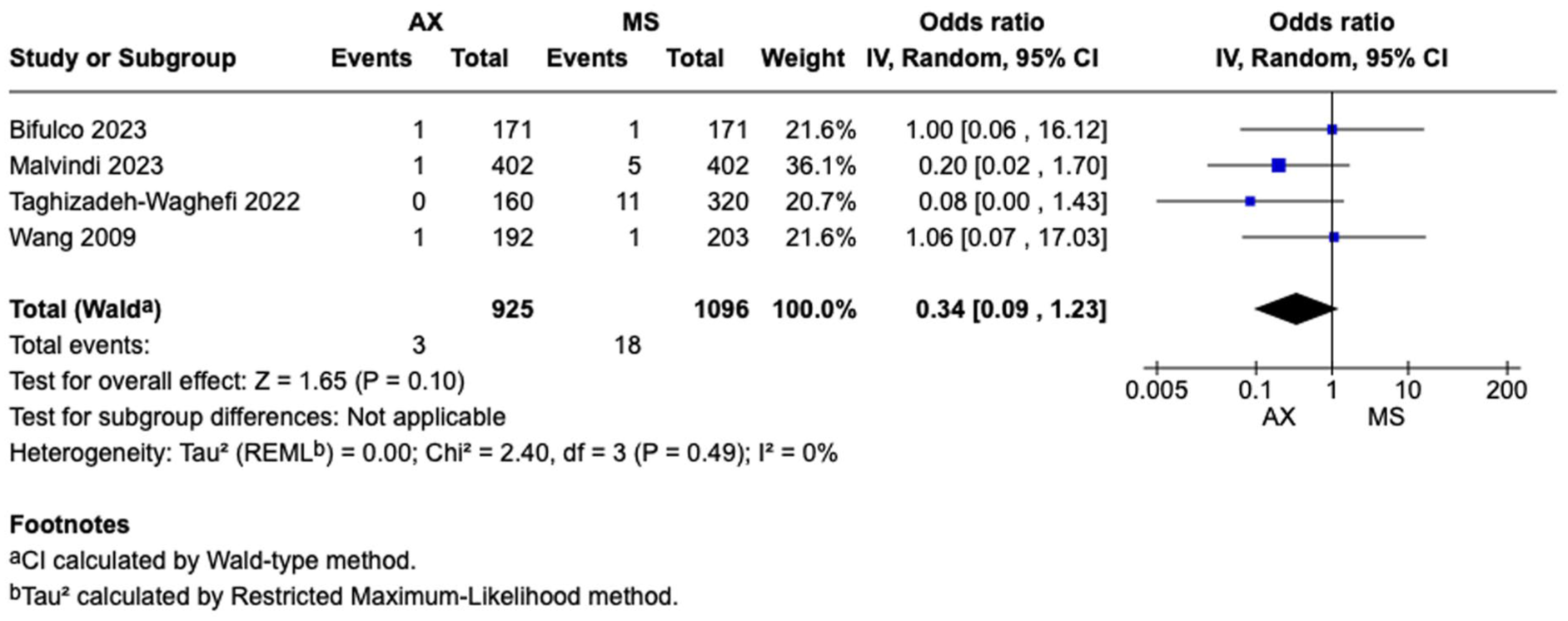
Forest plot for perioperative mortality. AX, axillary; CI, confidence interval; MS, median sternotomy; OR, odds ratio.
Secondary Outcomes
Figure 3 shows the forest plot for CPB time from 4 studies, including 2,021 participants. When compared with MS, the patients who underwent axillary access showed longer CPB times (MD = 16.38, 95% CI: 6.42 to 26.34, P = 0.001). Supplemental Figure 2 shows the forest plot for cross-clamp time from 4 studies, including 2,021 participants. There was no difference regarding cross-clamp time between the 2 strategies (MD = 3.81, 95% CI: -3.80 to 11.42, P = 0.33).
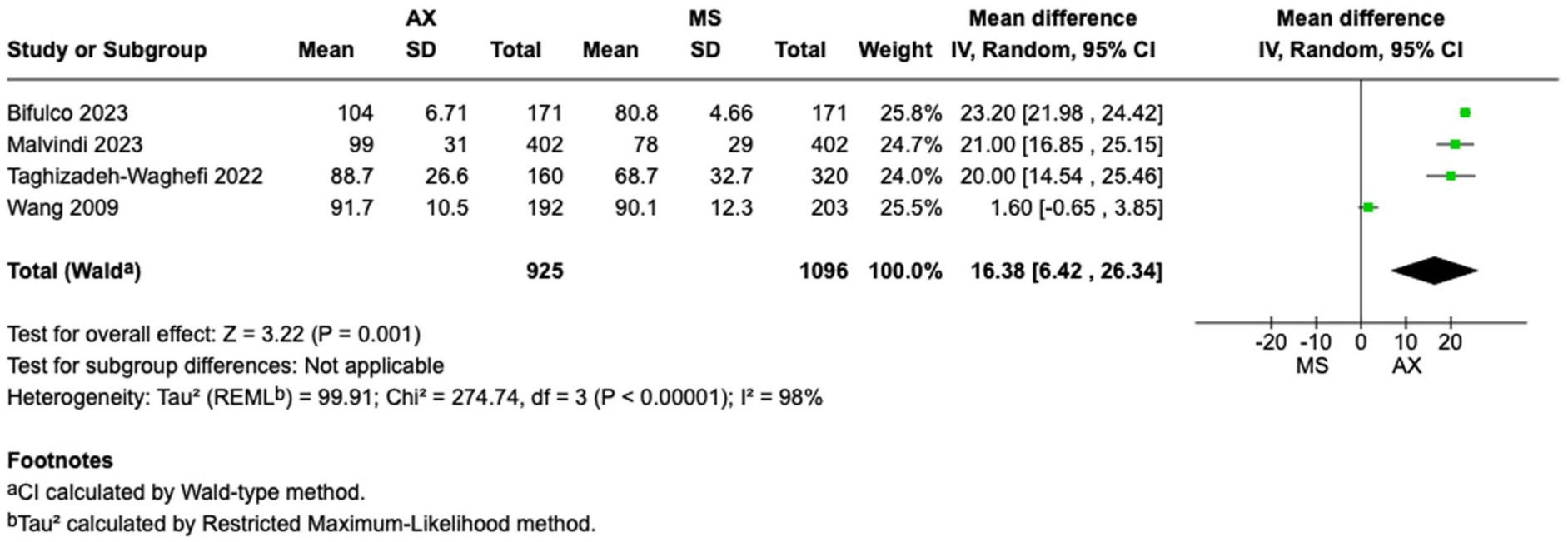
Forest plot for cardiopulmonary bypass time. AX, axillary; CI, confidence interval; MD, mean difference; MS, median sternotomy.
Supplemental Figure 3 shows the forest plot for rethoracotomy from 4 studies, including 2,021 participants. There was no difference regarding the incidence of rethoracotomy between the 2 strategies (OR = 0.83, 95% CI: 0.50 to 1.39, P = 0.48). Figure 4 shows the forest plot for wound complications from 4 studies, including 2,021 participants. When compared with MS, the patients who underwent axillary access showed reduced rates of wound complications (OR = 0.41, 95% CI: 0.21 to 0.80, P = 0.009). Supplemental Figure 4 shows the forest plot for stroke from 3 studies, including 1,850 participants. There was no difference regarding the incidence of stroke between the 2 strategies (OR = 0.40, 95% CI: 0.14 to 1.15, P = 0.09).
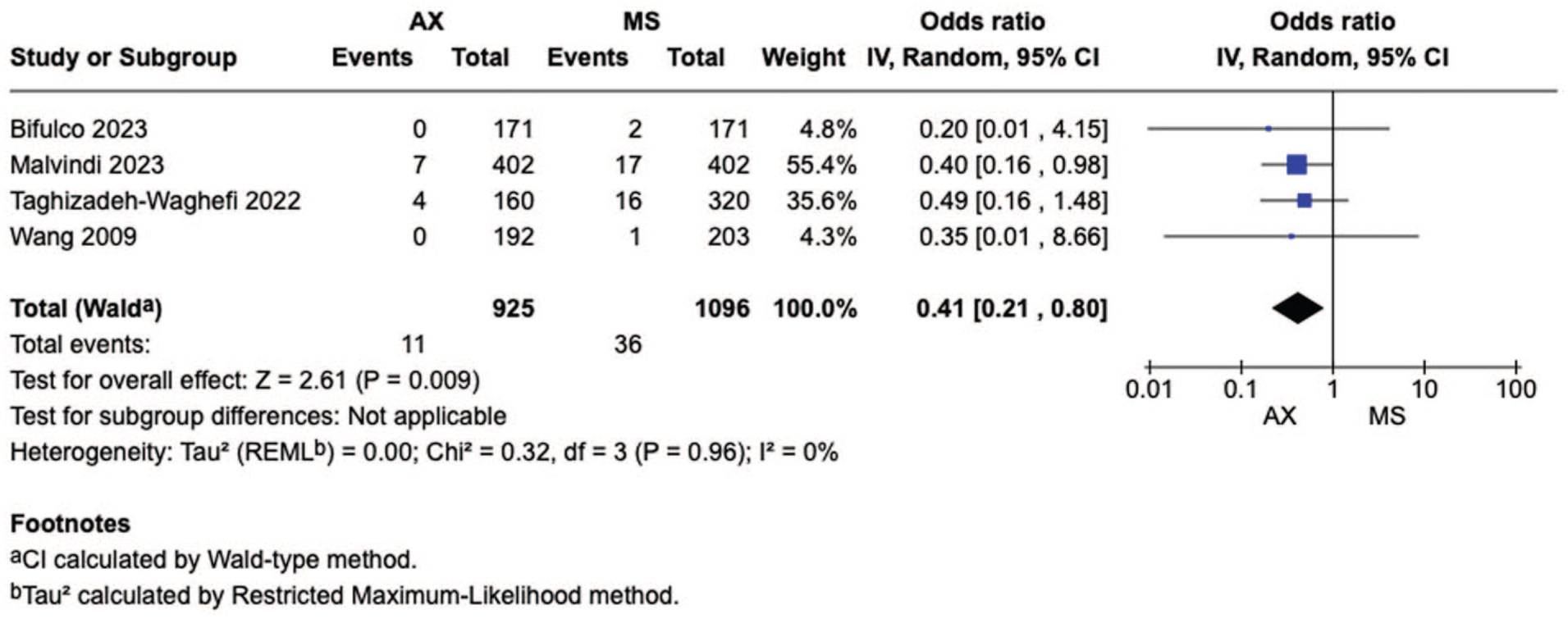
Forest plot for wound complications. AX, axillary; CI, confidence interval; MS, median sternotomy; OR, odds ratio.
Figure 5 shows the forest plot for ventilation duration from 4 studies, including 2,021 participants. When compared with MS, the patients who underwent axillary access showed shorter duration of ventilation (MD = −4.93, 95% CI: −8.79 to −1.08, P < 0.01). Figure 6 shows the forest plot for hospital length of stay from 4 studies, including 2,021 participants. When compared with MS, the patients who underwent axillary access showed shorter hospital stays (MD = −0.78, 95% CI: −1.41 to −0.14, P = 0.02). Figure 7 shows the forest plot for ICU length of stay from 3 studies, including 1,850 participants. When compared with MS, the patients who underwent axillary access showed shorter ICU stays (MD = −10.84, 95% CI: −19.54 to −2.14, P = 0.01).
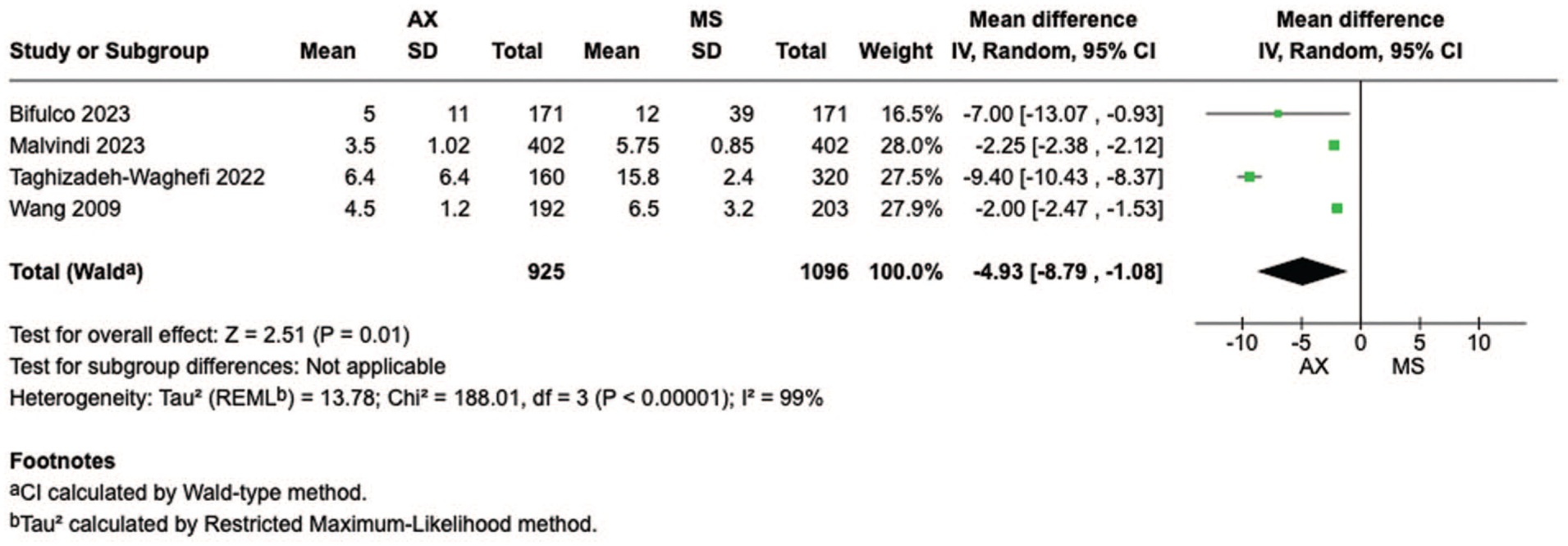
Forest plot for duration of ventilation. AX, axillary; CI, confidence interval; MD, mean difference; MS, median sternotomy.
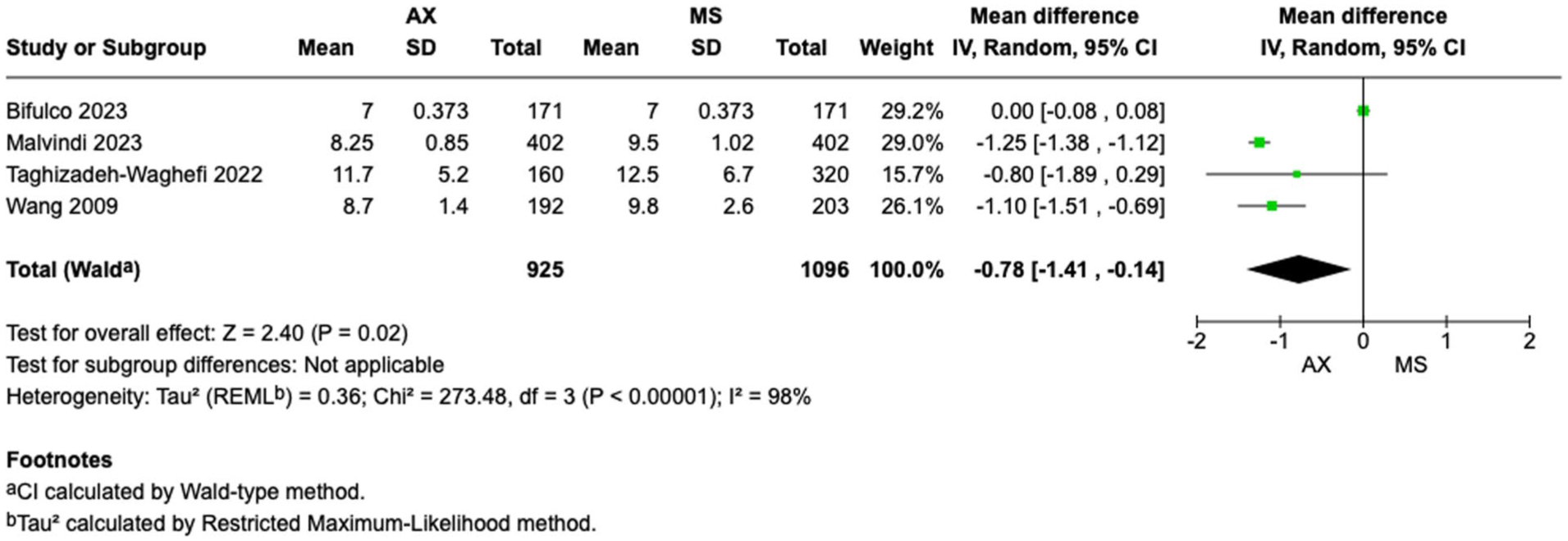
Forest plot for duration of hospital stay. AX, axillary; CI, confidence interval; MD, mean difference; MS, median sternotomy.
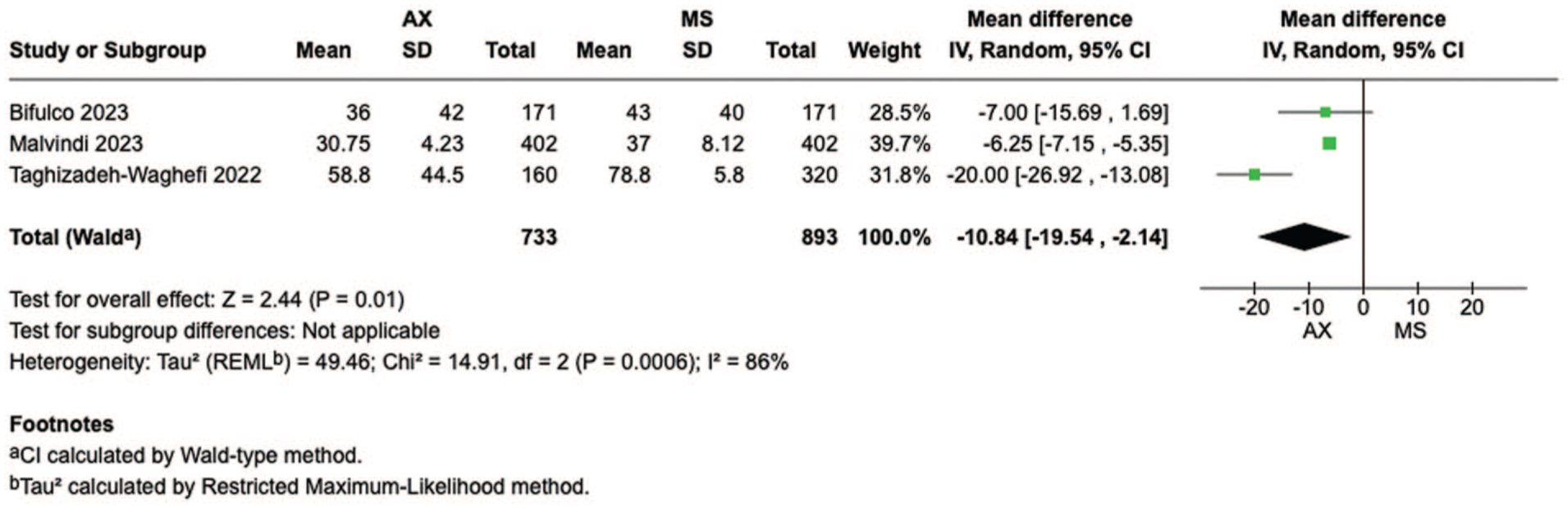
Forest plot for duration of intensive care unit stay. AX, axillary; CI, confidence interval; MD, mean difference; MS, median sternotomy.
Supplemental Figure 5 shows the forest plot for residual moderate mitral regurgitation from 2 studies, including 1,146 participants. There was no difference regarding the incidence of residual moderate mitral regurgitation between the 2 strategies (OR = 1.48, 95% CI: 0.25 to 8.75, P = 0.67).
Supplemental Figure 6 presents the forest plot for redo procedures due to early failure, derived from 2 studies encompassing a total of 1,146 participants. The analysis demonstrated a significantly higher incidence of early redo operations in the MS group compared with the axillary approach. Specifically, the axillary group was associated with a significantly lower odds of early failure requiring reoperation (OR = 0.33, 95% CI: 0.12 to 0.91, P = 0.03), indicating a potentially protective effect of the axillary technique in this context.
Discussion
The findings from this study indicate that, as compared with MS, the axillary approach for MVS is associated with similar perioperative mortality, longer CPB times, but shorter ICU and hospital stays. In addition, no significant differences were observed between the 2 strategies in terms of cross-clamp time, rethoracotomy rates, or stroke incidence. These results highlight the efficacy and safety of axillary access, providing a favorable balance of perioperative outcomes in appropriately selected patients.
Despite promising evidence, the adoption of minimally invasive MVS by surgeons has been gradual, largely due to concerns about longer operative times, technical demands, and the learning curve required to maintain repair durability.17–19 Although the literature suggests that axillary access offers direct visualization of the MV apparatus, facilitating an optimal surgical field without significantly increasing procedural complexity,20,21 our findings align with prior studies showing that minimally invasive MVS is often associated with prolonged CPB and cross-clamp times.22–24 Reports indicate that ischemic times frequently exceed 90 to 110 min, and CPB times often surpass 2 h in these procedures.25–27 However, the learning curve is an important factor, as evidence suggests that with experience, operative efficiency improves.28,29 For instance, complex MV repairs have been successfully performed using a minimally invasive approach, yielding durable long-term outcomes, including survival and recurrence rates comparable with conventional sternotomy—an observation consistent with our findings in patients undergoing reoperations for moderate MV regurgitation. 30
However, the success of the minimally invasive approach is highly dependent on surgical expertise and patient selection. In high-volume centers where surgeons are well-trained in these techniques, outcomes can be outstanding. However, when dealing with high-risk patients—particularly those with poor left ventricular function, significant coronary artery disease, or requiring multiple valve interventions—the minimally invasive approach may not offer the same advantages as MS, especially given the limited available evidence regarding outcomes of minimally invasive MVS in this patient population. 31 In addition, the complexity of MV repair itself must be considered. A bileaflet MV repair, for instance, is more technically demanding via a minimally invasive approach, often requiring longer operative times and potentially leading to different outcomes compared with an open, direct approach. 32 These nuances emphasize the need for careful patient selection and surgical expertise to maximize the benefits of minimally invasive techniques.
Conversely, some studies have raised concerns regarding prolonged single-lung ventilation, capillary leakage, and systemic inflammatory responses in minimally invasive approaches, which may contribute to pulmonary complications such as unilateral pulmonary edema and transient respiratory dysfunction. 22 However, our findings did not support these concerns, as the axillary approach was associated with shorter ventilation times, suggesting a potential advantage in respiratory recovery.
Finally, our pooled analysis highlighted comparable stroke rates between axillary and sternotomy groups, supporting the safety of axillary access in terms of neurologic outcomes. Moreover, in our included studies, patients were cannulated via a femoral approach with retrograde bypass, yet there was no difference in stroke rates between the 2 groups. This aligns with growing evidence that peripheral cannulation can be a viable alternative to central cannulation without adding risk to the stroke incidence. 33 However, it is important to take note of potential selection bias, as surgeons may preferentially choose axillary or minimally invasive approaches for patients with favorable anatomy and lower perceived risk. This may partially account for the comparable stroke rates observed. Future prospective studies or propensity-matched analyses could help better delineate the effect of access strategy on neurologic outcomes.
Limitations
This meta-analysis offers valuable insights into axillary MVS, but several limitations should be noted. All included studies were observational, raising the risk of selection bias and residual confounding, even with propensity score matching—especially because patients undergoing minimally invasive surgery are often healthier and lower risk than those undergoing sternotomy. Furthermore, variations in the learning curve for axillary access across centers may have influenced outcomes and limited generalizability.
The included studies did not consistently distinguish between MV repair and replacement, despite their differing complexities and prognoses. Furthermore, long-term outcomes, such as repair durability and survival, were not uniformly reported, making it difficult to assess the extended benefits of the minimally invasive approach beyond the immediate postoperative period. Lastly, the lack of patient-reported outcome measures, including quality of life and postoperative pain, limits the ability to fully evaluate its impact from a patient-centered perspective. Future research should address these gaps to better define the role of axillary MVS in different patient populations.
Conclusions
Axillary access for MVS appears to be a safe alternative to MS, with similar perioperative mortality, longer CPB times, but shorter ICU and hospital stays. Although it offers potential benefits in experienced centers, its role in high-risk patients remains uncertain. Further research is needed to assess long-term outcomes and patient selection criteria.
Supplemental Material
sj-docx-1-inv-10.1177_15569845251400765 – Supplemental material for Axillary Versus Sternotomy Access in Minimally Invasive Mitral Valve Surgery: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-inv-10.1177_15569845251400765 for Axillary Versus Sternotomy Access in Minimally Invasive Mitral Valve Surgery: A Systematic Review and Meta-Analysis by Abdullah Almehandi, Mohammed Ramadhan, Yahya Ali, Abdulaziz Almhanedi, Abdulrahman Osama Al-Naseem, Ahmad Gonnah, Ahmad Awad, Johannes Fischer, Hristo Kirov, Torsten Doenst, Rakan I. Nazer and Tulio Caldonazo in Innovations
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: T.C. was funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) Clinician Scientist Program OrganAge funding number 413668513, by the Deutsche Herzstiftung (DHS, German Heart Foundation) funding number S/03/23, and by the Interdisciplinary Center of Clinical Research of the Medical Faculty Jena.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.