
Abstract
Objective:
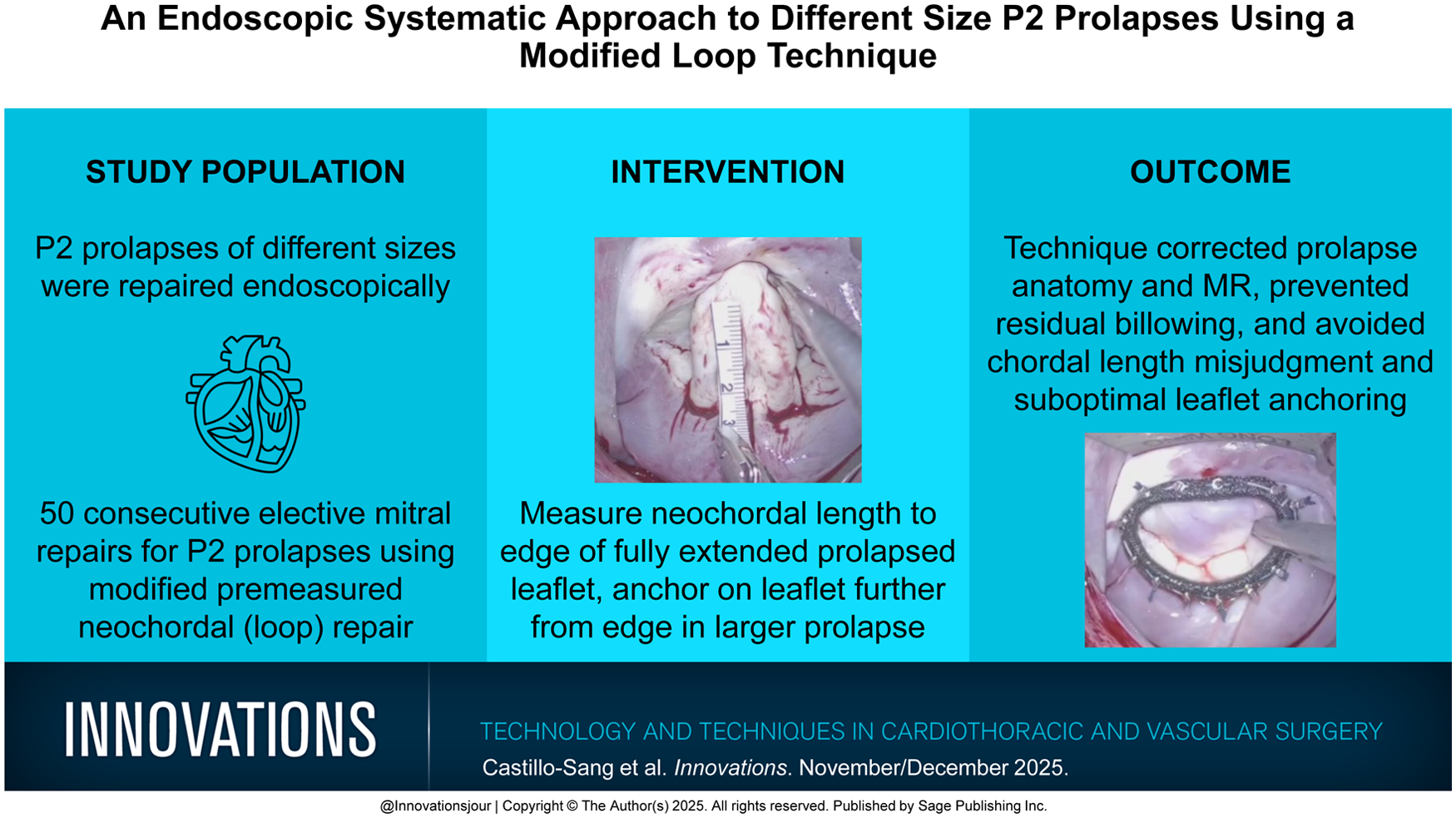
A P2 prolapse comes in all sizes, and the original description of mitral loop repair (premeasured neochords) does not account for prolapse size. This technique “blind spot” can result in residual billowing or prolapse, especially in larger leaflets. Ventricular remodeling after repair can cause neochordal pseudo-elongation that worsens this residual prolapse, leading to regurgitation. We sought to study the effect of P2 prolapse size on neochordal anchoring location on the prolapse. To account for the P2 prolapse size in loop technique, we measured this intraoperatively (edge-to-annulus distance) and anchored the neochords incrementally farther from the leaflet edge in larger prolapses. Neochordal length was measured from the flattened prolapsed leaflet edge to the papillary muscle anchoring point.
Methods:
Of 180 endoscopic repairs for degenerative mitral disease, 95 involved P2 neochords and 50 were premeasured (loop technique). We studied the relationship between P2 prolapse size and leaflet neochordal anchoring in 50 P2 prolapses through surgical footage review. Echocardiography at discharge and 3 months provided immediate and short-term follow-up.
Results:
All 50 repairs were successful without residual billowing or regurgitation above mild when anchoring neochords based on prolapse size. The P2 prolapses were grouped by size into 4 grades: grade 1 (<1.5 cm, n = 15), grade 2 (1.5 to 2 cm, n = 18), grade 3 (2 to 3 cm, n = 10), and grade 4 (>3 cm, n = 7). Each prolapse grade had consistent neochordal leaflet anchoring away from the edge: grade 1 = 3 mm, grade 2 = 5 to 8 mm, grade 3 = 1 to 1.5 cm, and grade 4 = 1.5 to 2 cm.
Conclusions:
Our adaptation of the loop technique to include P2 prolapse size prevents residual billowing or prolapse and prevents suboptimal leaflet anchoring.
Keywords
Get full access to this article
View all access options for this article.