
Abstract
Keywords
Standardized endoscopic papillary muscle relocation (PMR), specifically addressing MV leaflet tethering, resulted in favorable periprocedural outcomes despite severe LV dysfunction. Minimally invasive PMR for patients with secondary MR type IIIb should be considered during routine interdisciplinary heart team discussion.Central Message
Introduction
Secondary mitral regurgitation (SMR) with restricted leaflet motion during systole (type IIIb) 1 is a common sequela of chronic heart failure (HF) resulting from progressive left ventricular (LV) distortion caused by ischemic or dilated cardiomyopathy. 2 Instead of being a mere bystander of LV remodeling, SMR type IIIb is associated with worsening of HF symptoms and excessive mortality itself.3,4 In symptomatic patients with SMR despite optimal medical therapy (OMT), percutaneous transcatheter edge-to-edge repair (TEER) represents a promising option for selected patients with suitable mitral valve (MV) anatomy. 5 Nevertheless, contradictory data regarding the prognostic benefit of TEER have been published.5,6 Most notably, patients with advanced LV remodeling, such as the Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients With Functional Mitral Regurgitation (COAPT) trial exclusion criteria of LV ejection fraction (LVEF) <20% and LV end-diastolic diameter (LVEDD) >70 mm, might not benefit from TEER.6–8
Isolated mitral annuloplasty results in an increased prevalence of recurrent mitral regurgitation (MR) 9 and did not demonstrate any prognostic benefit in comparison to OMT or MV replacement (MVR). 10 Therefore, additional subannular repair strategies, 11 specifically addressing LV geometry and papillary muscle orientation, have been developed to improve long-term durability after MV repair. 12 Standardized papillary muscle relocation (PMR), in addition to ring annuloplasty, 13 is feasible in a minimally invasive MV surgery setting. 14 Nevertheless, the periprocedural outcomes of patients with severely depressed LVEF remains unknown.
Methods
Patients
The local ethical committee approved the retrospective study, which complies with the Declaration of Helsinki. We herein analyzed the periprocedural outcome of 36 consecutive patients with SMR type IIIb who underwent minimally invasive standardized PMR at our institution between 2016 and 2021. According to preoperative transthoracic echocardiography, patients with severely reduced LVEF ≤35% (study group) were compared to patients with LVEF >35% (control group). After the evaluation and quantification of the severity of LV dysfunction and MR mechanism, all available therapeutic options, including TEER, transcatheter MV implantation (TMVI), surgical MV repair, and MVR, as well as LV assist device (LVAD) implantation and heart transplantation, were discussed in our institutional heart team.
Inclusion and Exclusion Criteria
Between 2016 and 2021, 98 consecutive patients with HF (LVEF <50%, LVEDD >55 mm) with symptomatic (New York Heart Association class ≥II) and severe (effective regurgitant orifice area [EROA] ≥0.2 cm2) type IIIb SMR (i.e., tenting height >10 mm) despite OMT, who were suitable for MV surgery, underwent standardized PMR in addition to ring annuloplasty. Due to the need for simultaneous coronary artery bypass grafting, 62 patients underwent sternotomy and were excluded from the current analysis. The remaining 36 patients were treated by a minimally invasive technique using 3-dimensional (3D) endoscopy. Patients with mixed MV disease, primary MR, or those requiring emergency surgery were excluded.
Surgical Setup and Standardized PMR Technique
Minimally invasive MV surgery was performed in a standard operating room via right anterolateral minithoracotomy using a soft-tissue retractor and 3D endoscopic guidance. A limited skin incision (<4 cm) periareolar (in men) or submammary (in women) was used to enter the fourth intercostal space. Peripheral cardiopulmonary bypass (CPB) was established via direct femoral cannulation. Preoperative peripheral Doppler ultrasound determined adequacy of femoral vessels. Transthoracic Chitwood clamp was used for aortic cross-clamp, and antegrade cardioplegia (i.e., del Nido) was administered into the aortic root. After exposure of the MV using a left atrial access and intraoperative confirmation of SMR type IIIb, standardized PMR was performed in addition to conventional ring annuloplasty using an ETlogix ring (Edwards Lifesciences, Irvine, CA, USA). 13 Therefore, 2 pledgeted 3-0 polytetrafluorethylene sutures were placed through the trunks of both papillary muscles and subsequently passed through the posterior mitral annulus and the adjacent annuloplasty ring. After filling the LV with cold saline, stepwise traction was applied on both sutures until leaflet tethering disappeared. To create a stable distance between the papillary muscles and the mitral annulus, both sutures were tightly knotted on the annuloplasty ring, while keeping the constant traction (Fig. 1).
Standardized PMR was implemented within our institutional clinical routine, and a group of 5 experienced MV surgeons performed the operations accordingly. Concomitant procedures such as atrial fibrillation (AF) ablation, left atrial appendage (LAA) closure, and tricuspid valve repair were performed according to our institutional standard without major changes during the study period.
Statistical Analysis
Baseline and follow-up data were retrospectively analyzed. Normally distributed continuous variables are presented as mean values and standard deviations. Otherwise, medians and interquartile ranges are used for continuous variables and absolute numbers and percentages for categorical variables. Unpaired t tests were used for between-group comparison of normally distributed numeric variables. Chi-squared tests were used for between-group comparison of categorial variables if the minimum expected cell size was at least 5. Otherwise, Fisher's exact tests and Mann-Whitney U tests were used. Results were considered statistically significant if the P value was <0.05. IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses. The data underlying this article will be shared on reasonable request to the corresponding author.
Results
Study Sample
A total of 98 consecutive patients with symptomatic type IIIb SMR (Fig. 2) despite OMT underwent surgical MV repair including standardized PMR at our institution between 2016 and 2021. Out of 36 patients, who we treated minimally invasively via right-sided minithoracotomy under 3D endoscopic guidance, 18 patients showed a severely reduced LVEF ≤35% (study group) and were compared to 18 patients with an LVEF >35% (control group).
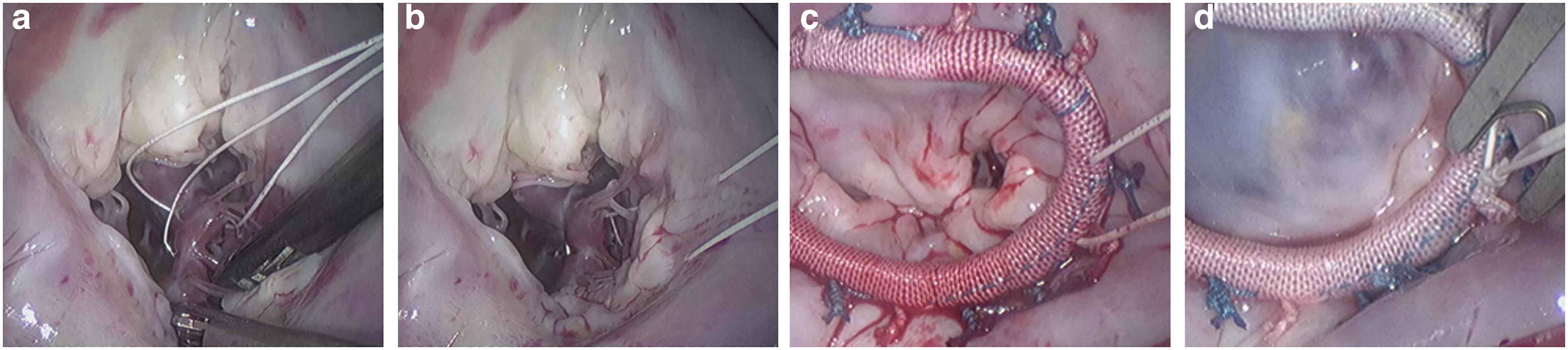
Standardized endoscopic papillary muscle relocation. Two pledgeted 3-0 polytetrafluorethylene sutures were (a) placed through the trunks of both papillary muscles and subsequently passed through (b) the posterior mitral annulus and (c) the adjacent annuloplasty ring. After filling the left ventricle with cold saline, stepwise traction was applied on both sutures until leaflet tethering disappeared. (d) To create a stable distance between the papillary muscles and the mitral annulus, both sutures were tightly knotted on the annuloplasty ring while keeping the traction.
Median age at the time of surgery was 63 (53 to 72) years in the whole cohort, and 61% of patients (22 of 36) were male (Table 1). Prevalence of ischemic cardiomyopathy was similar in both study and control groups (33.3% vs 44.4%, P = 0.31). Nevertheless, preoperative coronary angiogram confirmed no further need for coronary revascularization in all patients. Despite more severe impairment of LVEF (30% ± 4% vs 43% ± 6%, P < 0.001) and tricuspid annular plane systolic excursion (TAPSE; 18 ± 3 mm vs 23 ± 5 mm, P = 0.001), the severity of SMR indicated by EROA (0.28 ± 0.1 cm2 vs 0.33 ± 0.1 cm2, P = 0.084) and the degree of MV leaflet tethering indicated by tenting height (12 ± 3 mm vs 12 ± 1 mm, P = 0.60) and tenting area (309 ± 61 mm2 vs 301 ± 85 mm2, P = 0.84) were similar in the study and control groups. In addition, systolic pulmonary artery pressure (sPAP) and the prevalence of concomitant tricuspid regurgitation were comparable. Furthermore, no significant differences were present in the study versus control groups regarding patient demographics or prevalence of other outcome-relevant risk factors. Most patients were New York Heart Association functional class ≥III in both groups (89% vs 67%, P = 0.28) and had similar serum levels of creatinine and natriuretic peptide at baseline (Table 1).
Preoperative Patient Characteristics and Echocardiographic Parameters.
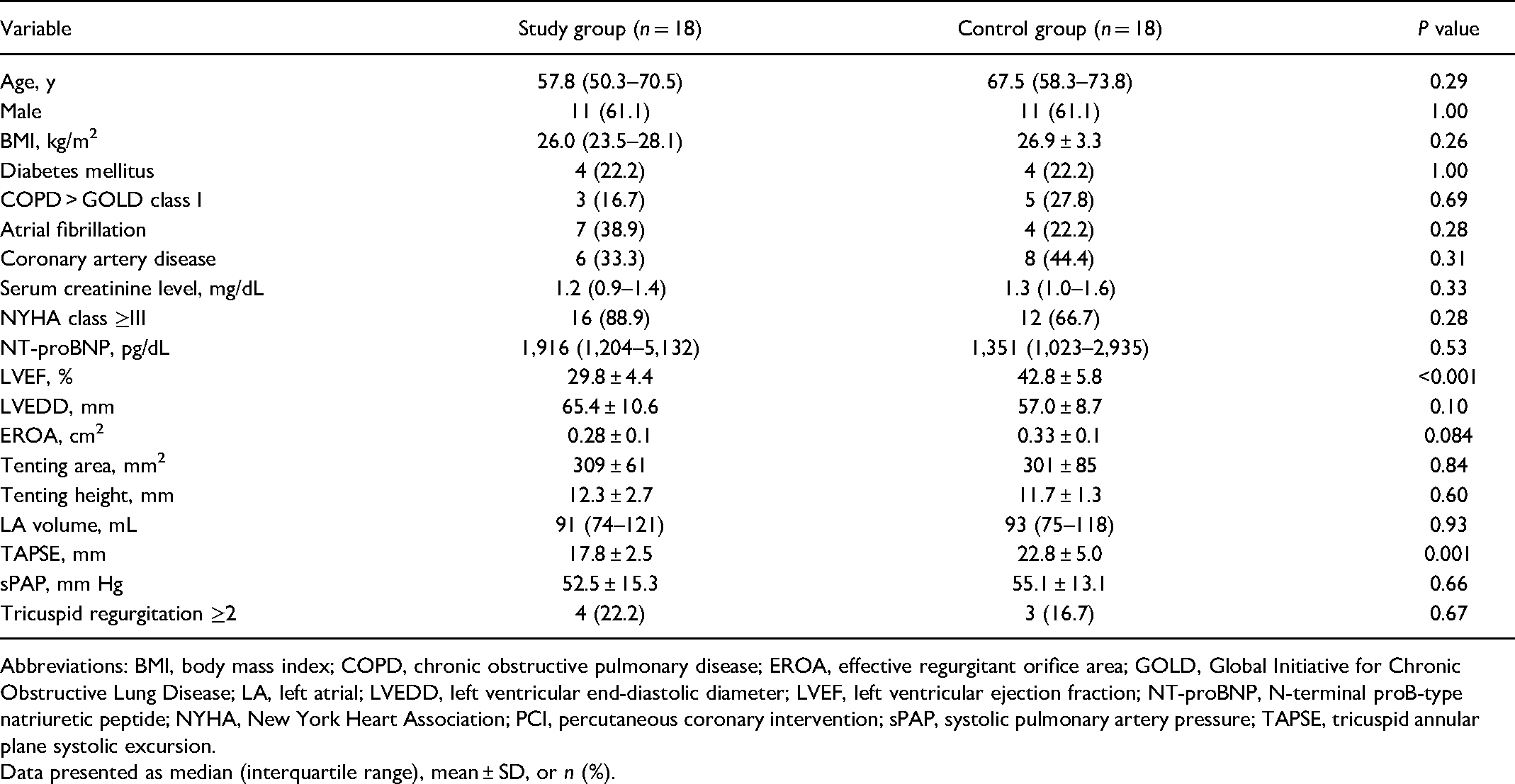
Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; EROA, effective regurgitant orifice area; GOLD, Global Initiative for Chronic Obstructive Lung Disease; LA, left atrial; LVEDD, left ventricular end-diastolic diameter; LVEF, left ventricular ejection fraction; NT-proBNP, N-terminal proB-type natriuretic peptide; NYHA, New York Heart Association; PCI, percutaneous coronary intervention; sPAP, systolic pulmonary artery pressure; TAPSE, tricuspid annular plane systolic excursion.
Data presented as median (interquartile range), mean ± SD, or n (%).
Periprocedural Outcomes
Conversion to sternotomy was required due to excessive pleural adhesions in 1 patient in each group. The prevalence of concomitant tricuspid valve repair, AF ablation, and LAA closure was similar in the study and control groups. Rigid complete annuloplasty rings, with similar median of manufacturer given ring sizes (28 mm [28 to 30 mm]), were used in all patients (IMR ETlogix annuloplasty ring). The duration of surgery, CPB, and cross-clamp were similar (Table 2). Of note, there was no need for perioperative extracorporeal membrane oxygenation (ECMO) support in either group. However, intra-aortic balloon pump was inserted in 1 patient in each group due to high periprocedural pharmacological inotropic support. Rethoracotomy for bleeding and rates of postoperative pacemaker implantation were similar between groups. Furthermore, there was no difference in postoperative mechanical ventilation time (5.7 vs 6.0 h, P = 0.43; Table 2). The incidence of low cardiac output syndrome, as well as length of intensive care unit stay, was similar in both groups. In-hospital and 30-day survival was 100% in both groups.
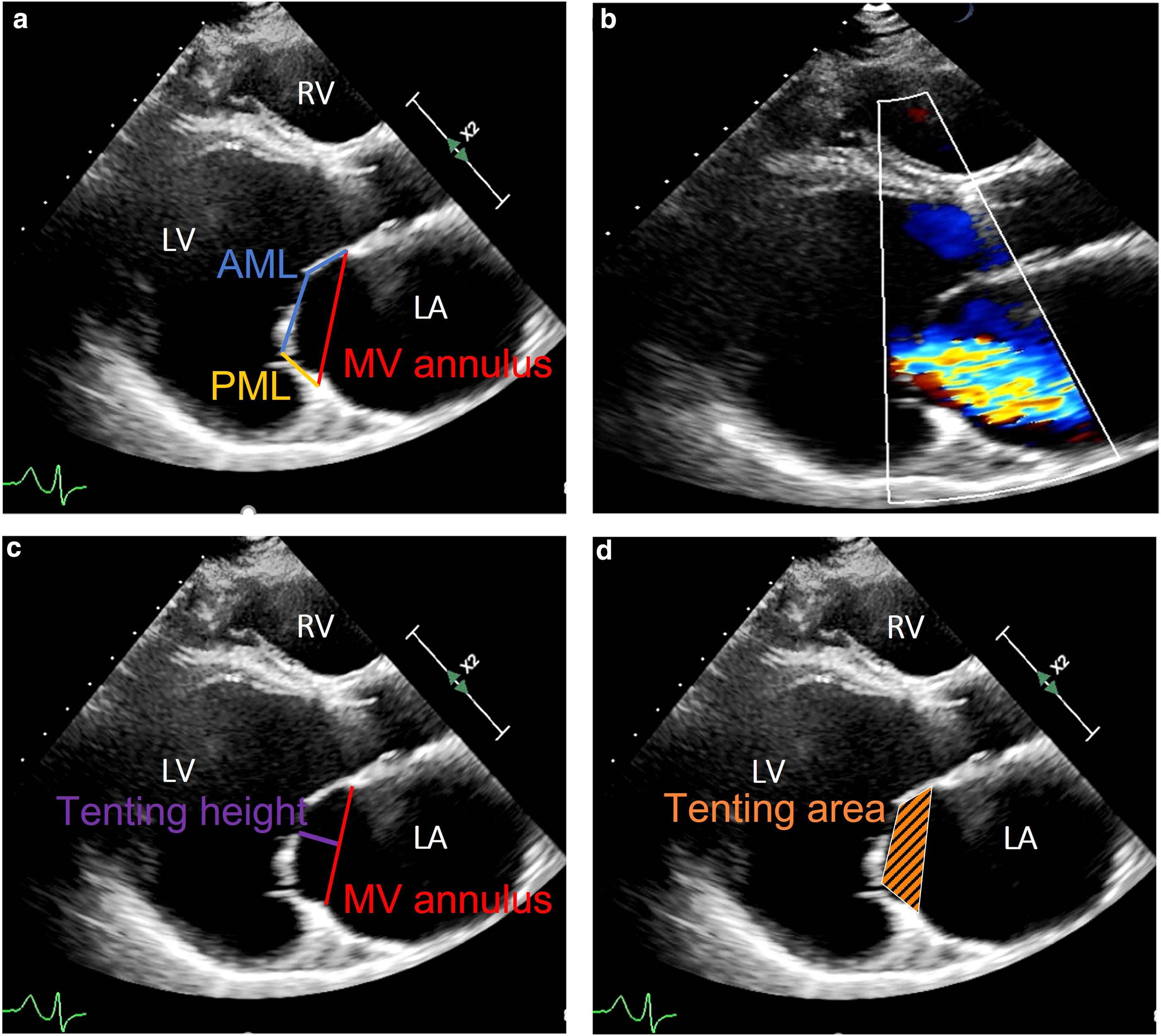
Advanced LV remodeling resulting in severe secondary mitral regurgitation type IIIb. (a) Preoperative echocardiography parasternal long axis view (AML, blue; PML, yellow; MV annular plane, red). (b) Color Doppler echocardiography reveals severe secondary mitral regurgitation type IIIb (effective regurgitant orifice area = 0.38 cm2) in parasternal long-axis view. Severe tethering of both mitral leaflets with (c) tenting height in purple (14 mm) and (d) tenting area in orange (3.2 cm2) in parasternal long axis view. AML, anterior mitral leaflet; LA, left atrium; LV, left ventricle; MV, mitral valve; PML, posterior mitral leaflet; RV, right ventricle.
Periprocedural Outcomes.
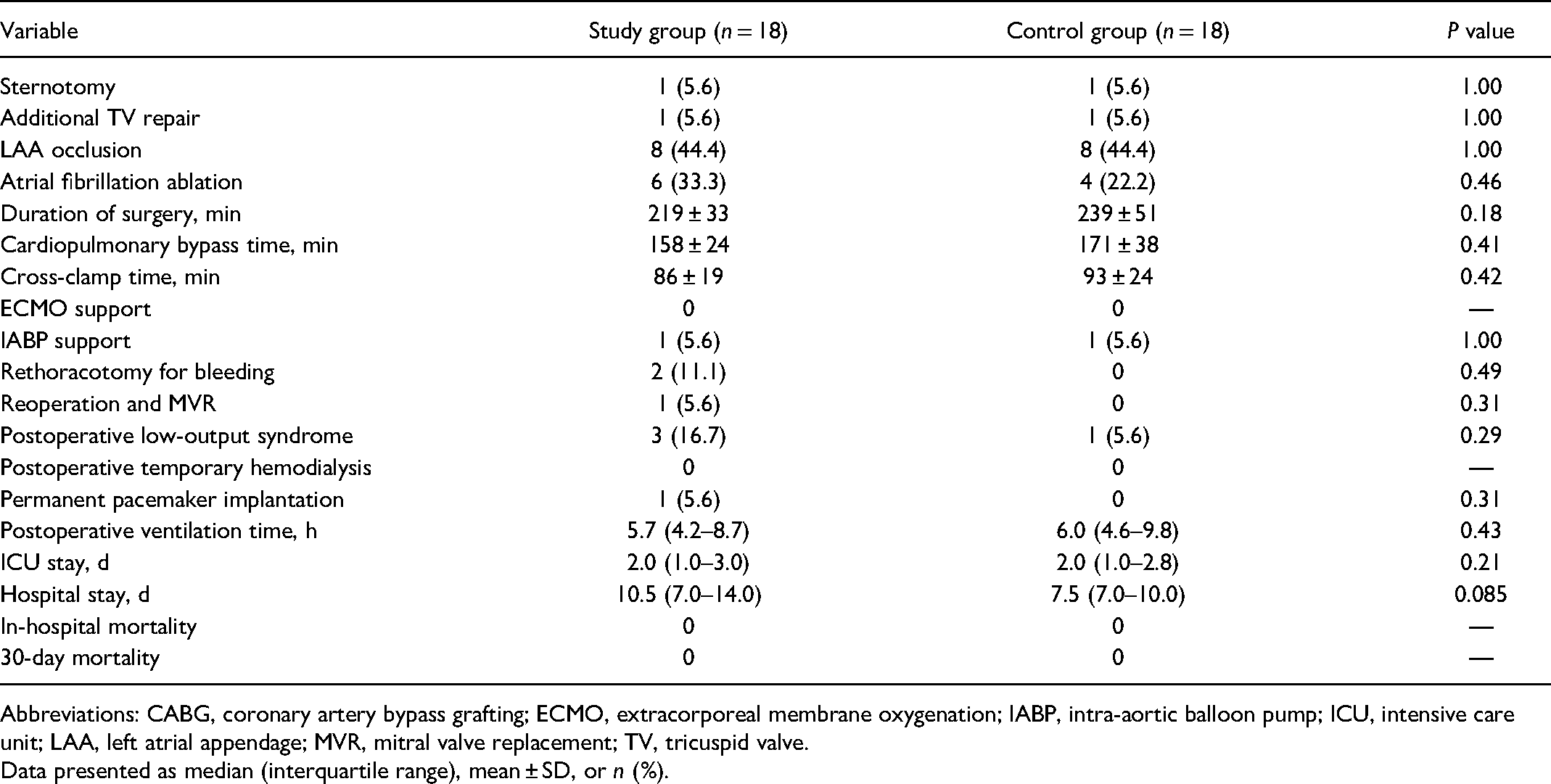
Abbreviations: CABG, coronary artery bypass grafting; ECMO, extracorporeal membrane oxygenation; IABP, intra-aortic balloon pump; ICU, intensive care unit; LAA, left atrial appendage; MVR, mitral valve replacement; TV, tricuspid valve.
Data presented as median (interquartile range), mean ± SD, or n (%).
Outcome Parameters at Discharge
One patient in the study group with severe preoperative LV dysfunction (LVEF <20%, LVEDD >75 mm) and excessive MV leaflet tethering required reoperation and chordal-sparing MVR due to persistent MR during the same hospital stay. In all remaining patients, no residual MR greater than mild was found at discharge. Residual MV tethering (tenting height and tenting area) at discharge was significantly reduced in comparison to baseline values in both groups (Table 3). No functional mitral stenosis or reduced MV orifice area were identified in any patient postoperatively. Postoperative right ventricular function, measured as TAPSE, was comparable in both groups (13.3 ± 3.9 mm vs 15.1 ± 3.1 mm, P = 0.14), although systolic LV function remained significantly reduced in the study group versus the control group (P = 0.001; Table 3).
Discharge Outcomes.
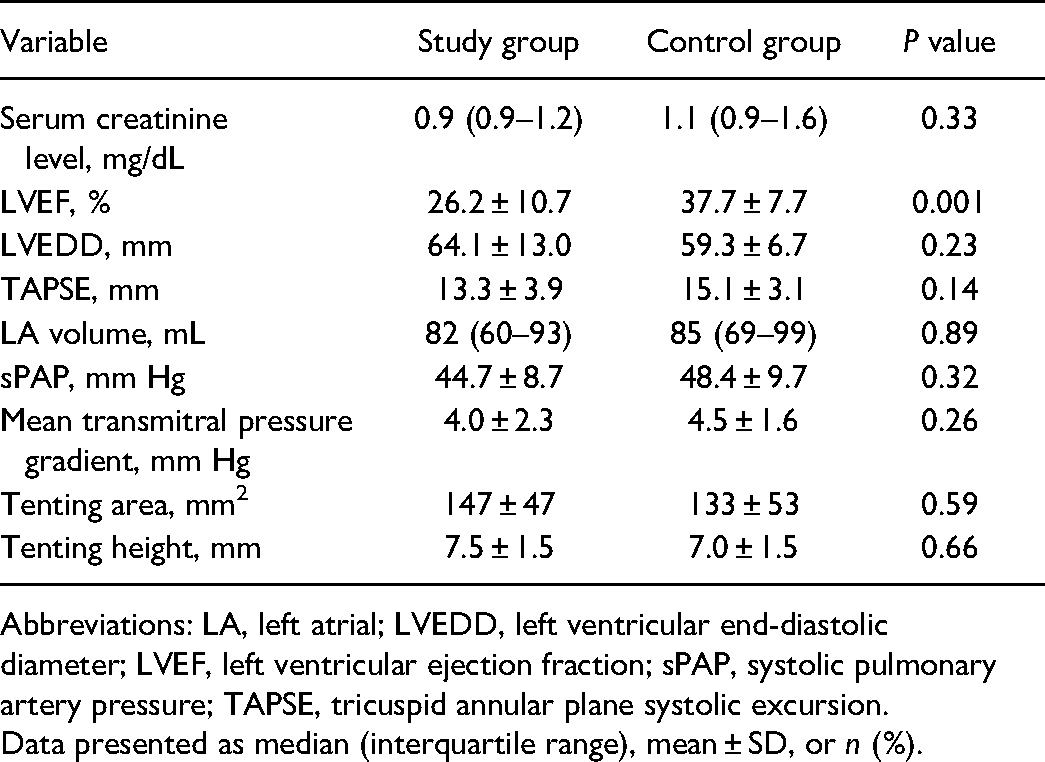
Abbreviations: LA, left atrial; LVEDD, left ventricular end-diastolic diameter; LVEF, left ventricular ejection fraction; sPAP, systolic pulmonary artery pressure; TAPSE, tricuspid annular plane systolic excursion.
Data presented as median (interquartile range), mean ± SD, or n (%).
Discussion
SMR type IIIb, which is prevalent in about one-third of patients with advanced HF, 15 is associated with a dismal outcome and remains a promising therapeutic target. 16 Despite contradictory data regarding the prognostic effect of TEER in patients with HF who have concomitant SMR,5,6 TEER was upgraded in the current guidelines for the management of valvular heart disease. 17 Accordingly, in symptomatic patients despite OMT, who have no indication for coronary revascularization and exhibit appropriate anatomical features (LVEF between 20% and 50%, LV end-systolic diameter <70 mm, sPAP <70 mm Hg), TEER is reasonable (Class IIa, Level B). In contrast, MV surgery has only a Class IIb, Level C indication in the clinical setting described above. 17 Due to an excellent periprocedural safety profile and less invasiveness as compared to conventional open heart surgery, TEER emerges to be the first-line treatment option for SMR in patients with HF.
Isolated mitral annuloplasty is associated with an unacceptably high rate of recurrent SMR up to 60% 9 and does not show any beneficial prognostic effect in comparison to OMT. 10 To improve repair durability and to avoid the drawbacks of MVR, subannular repair strategies have been established. In particular, standardized PMR is feasible in a minimally invasive MV surgery setting, although the periprocedural outcome of patients with severely depressed LVEF remains unknown.
Study Population
We aimed to compare the periprocedural outcome of minimally invasive standardized PMR in patients with HF who have LVEF ≤35% and LVEF >35% in the treatment of symptomatic SMR type IIIb. After echocardiographic and clinical assessment, all symptomatic patients with SMR type IIIb were discussed in our institutional interdisciplinary heart team, including the evaluation of TEER, TMVI, surgical MV repair, and MVR strategies, as well as LVAD implantation and heart transplantation. Despite the obvious differences in the severity of LV dysfunction, baseline patient characteristics including comorbidities, as well as mitral leaflet tethering parameters, were similar in both groups.
In-Hospital Outcomes
Except for 2 patients who underwent conversion to sternotomy due to excessive pleural adhesions, all remaining patients were successfully treated minimally invasively via right-sided minithoracotomy under 3D endoscopic guidance. Concomitant procedures, procedural duration times, and CPB and cross-clamp times were similar in both groups. Our data demonstrate that in contrast to other described subannular MV repair strategies (e.g., papillary muscle approximation or the “ring plus string” technique),18,19 standardized PMR can be reproducibly performed in a minimally invasive MV surgery setting, independent of the severity of LV dysfunction. Periprocedural complication rates were comparably low in both groups. Of note, despite the severe degree of LV dysfunction, there was no weaning failure from CPB or need for perioperative ECMO support. This finding underlines the importance of a thorough heart team discussion, to select appropriate surgical candidates. Obviously, a reasonable comparison with previously published TEER cohorts is quite limited due to methodological issues because patients enrolled in the COAPT and Multicentre Study of Percutaneous Mitral Valve Repair MitraClip Device in Patients With Severe Secondary Mitral Regurgitation (MITRA-FR) trials were either inoperable or at very high surgical risk. Nonetheless, procedural safety and in-hospital mortality in our series seem to be lower as compared to previously published surgically treated SMR cohorts.9,20,21
Apart from cosmetic advantages, patients with HF who have severe LV dysfunction might particularly benefit from rapid extubation protocols, decreased transfusion rates, and the absence of sternal wound infections after endoscopic MV repair.22,23 In addition, all further surgical interventions that might be required due to advancing HF (i.e., LVAD implantation, heart transplantation) are technically less challenging after previous minimally invasive surgery as compared to conventional sternotomy. Furthermore, due to the implementation of enhanced recovery after cardiac surgery protocols, 24 as well as the adaption of advanced percutaneous cannulation techniques, 25 perioperative complication rates after minimally invasive MV surgery will potentially further decrease.
Although long-term durability of endoscopic PMR is yet to be established, very favorable periprocedural results might suggest that minimally invasive MV surgery can safely be extended to patients with HF who have severe LV dysfunction.
Study Limitations
This is a limited-size single-center study with a nonrandomized study design. Furthermore, only perioperative outcomes were addressed. We included no additional control group of patients with SMR after TEER or OMT alone, which would be required for a more extensive comparison. Therefore, the comparability of our results with the alternative SMR treatment modalities is limited.
Conclusions
Standardized endoscopic PMR results in favorable periprocedural outcomes, even in patients with severe LV dysfunction. Compared to patients with less severe LV dysfunction, the perioperative results were similar, suggesting that minimally invasive surgery can be safely extended to this patient population. Further studies with an increased follow-up period in a larger patient population are needed to evaluate the future role of minimally invasive standardized PMR as a treatment option for patients with HR who have SMR type IIIb.
Supplemental Material
Visual abstract - Supplemental material for Early Outcomes of Endoscopic Papillary Muscle Relocation for Secondary Mitral Regurgitation Type IIIb in Patients With Severe Left Ventricular Dysfunction
Supplemental material, sj-pptx-1-inv-10.1177_15569845221115419 for Early Outcomes of Endoscopic Papillary Muscle Relocation for Secondary Mitral Regurgitation Type IIIb in Patients With Severe Left Ventricular Dysfunction by Jonas Pausch, Oliver D. Bhadra, Tatiana M. Sequeira Gross, Xiaoqin Hua, Lenard Conradi, Hermann Reichenspurner and Evaldas Girdauskas in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.