
Abstract
Objective:
Robot-assisted thoracoscopic (RATS) lung resection is a widely used treatment modality. We hypothesized that geographic and sociodemographic factors would affect trends in RATS use versus video-assisted thoracoscopic (VATS) for lung resection in the United States.
Methods:
Retrospective study of patients who underwent either RATS or VATS lung resection from 2016 to 2020 within the National Inpatient Sample. Cohorts were stratified by extent (lobectomy vs sublobar) and technique (RATS vs VATS) of resection and compared with respect to sociodemographic, hospital-level, and geographic factors.
Results:
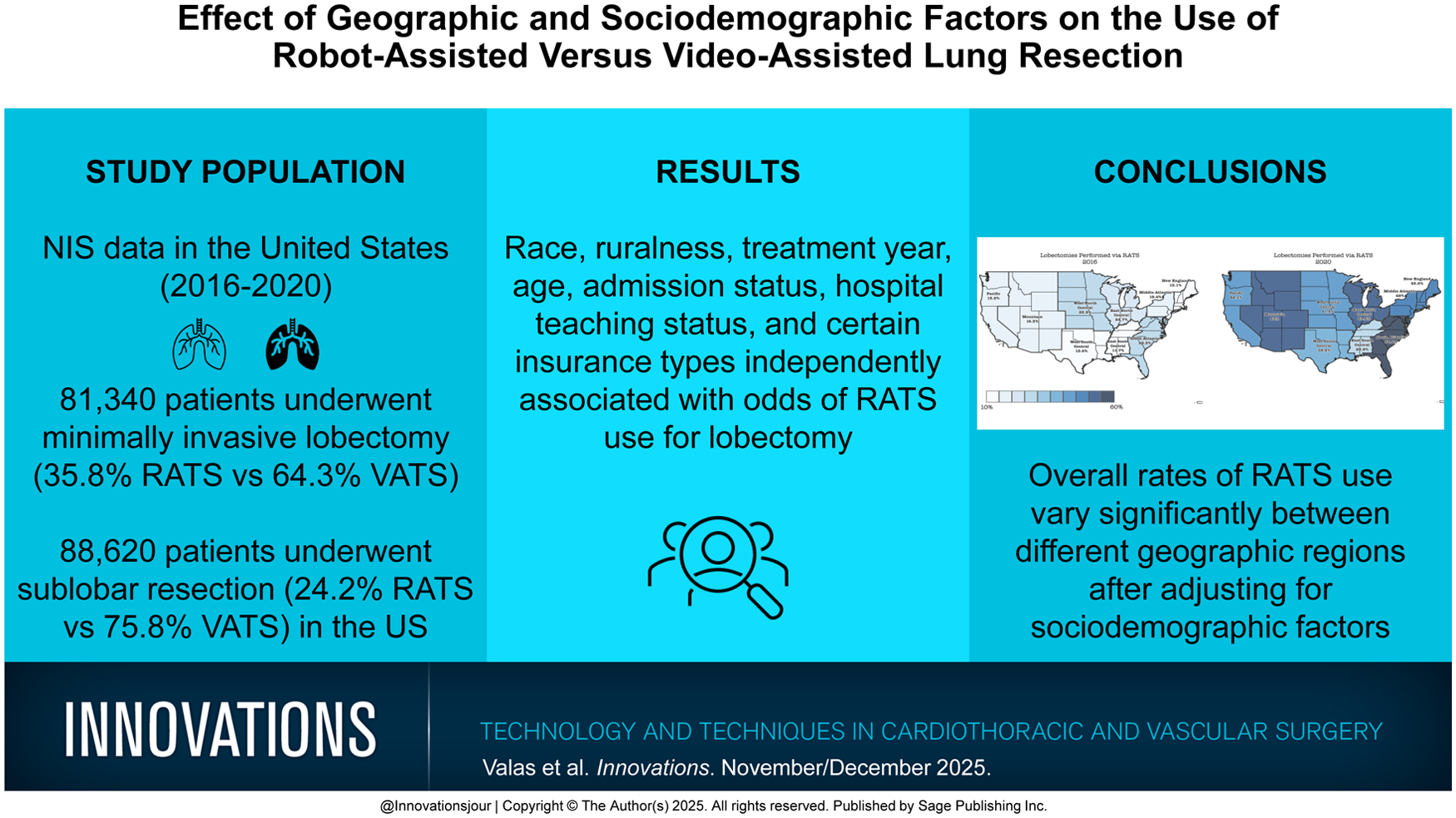
From 2016 to 2020, 81,340 patients underwent lobectomy (35.8% vs 64.3% for RATS vs VATS) and 88,620 underwent sublobar resection (24.2% vs 75.8% for RATS vs VATS). RATS lung resection rates varied by year and geographic division (P < 0.05). The odds ratio (OR) of RATS for lobectomies (reference = East South Central) ranged from 1.64 (95% confidence interval [CI]: 1.35 to 2.0) for Pacific to 3.88 (95% CI: 3.23 to 4.67) for East North Central. For sublobar resection, they ranged from 1.64 (95% CI: 1.31 to 2.06) for Pacific to 3.27 (95% CI: 2.69 to 4.02) for South Atlantic. Race, ruralness, treatment year, age, admission status, hospital teaching status, and certain insurance types were independently associated with the odds of RATS lobectomy use (P < 0.05). Findings were similar for sublobar resection use, except for insurance status (P > 0.05) and hospital bed size (P < 0.05).
Conclusions:
Geographic division remained independently associated with the odds of RATS lung resection after adjusting for sociodemographic factors. The overall rates of RATS use ranged from 16.9% to 44.7% for lobectomy and from 11.5% to 30.6% for sublobar lung resection between geographic regions.
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.