
Abstract
Ectopic parathyroid tissue in the mediastinum represents a rare and potentially serious clinical entity with challenging diagnostic and surgical management. The main surgical approach for this issue is open thoracotomy, which is a safe technique but carries risks and complications associated with such as extensive surgery. The purpose of this study is to demonstrate robotic thoracic surgery as an alternative and potentially advantageous method to treat patients with ectopic parathyroid adenomas compared with open and video-assisted thoracoscopic surgery approaches. A total of 13 reports in the literature were identified that provided details in terms of complications, surgical approach, and results of minimally invasive surgical resection of mediastinal ectopic parathyroid tissue.
Keywords
Central Message
Robot-assisted thoracoscopic surgery is an acceptable alternative approach for the management of symptomatic mediastinal ectopic parathyroid glands.
Introduction
Ectopic parathyroid glands have been classically described as occurring in numerous anatomic locations anywhere from the angle of the mandible to the mediastinum. 1 During embryogenesis, the superior parathyroid glands can descend into any position of the neck. The location of the inferior parathyroid glands is described compared with the thymus gland, and the increased distance in descent leads to greater final anatomical irregularity. To that extent, ectopic parathyroid adenoma arises from ectopic parathyroid tissue and could be the cause of primary hyperparathyroidism. Only 20% of parathyroid adenomas are described as ectopic in the mediastinum and constitute a more challenging surgical approach to resect. 2
Open approaches to excise an ectopic mediastinal parathyroid adenoma include lateral thoracotomy and the evolution of this procedure, which is partial sternotomy. Upper partial sternotomy is a surgical technique that is commonly used to extract ectopic parathyroid adenomas when they are located at the superior mediastinum of the chest. Potential drawbacks of the open approach are prolonged hospital stay, unappealing cosmetic results, delayed return to baseline activities, and potential wound-healing delays or complications among patients with diabetes and those who are immunocompromised. 3
In recent years, the introduction of minimally invasive ectopic parathyroid resection offered faster postoperative recovery, better cosmesis, and fewer complications than were associated with open surgery. In their case series, Alesina et al. concluded that resection of thoracic ectopic parathyroid via video-assisted thoracoscopic (VATS) approach is a safe alternative. VATS was associated with low complication rates and good cosmetic results. 4 The latest evolution of the minimally invasive thoracic approaches uses robot-assisted surgical technology (RATS). The aim of this study is to present the current literature regarding the application of RATS in the management of ectopic parathyroid adenomas located in the thoracic region.
Methods
The data presented in this study were obtained through a literature review of MEDLINE database (via PubMed). The search strategy used was as follows: ((ectopic parathyroid) OR (mediastinal masses) OR (mediastinal parathyroid adenoma)) AND (robotic assisted). A total of 47 results were retrieved including reviews, case series, and case reports. The inclusion criteria were patients with ectopic parathyroid adenomas, treated by a RATS technique, and articles published in English. The exclusion criteria were review articles, nonhuman samples, non-English language, and conference studies.
Results
In 13 reports (from 2004 to 2021), a total of 48 patients underwent excision of ectopic parathyroid adenomas using the RATS approach. There were 33 female and 15 male patients (age, 23 to 74 years).2,5–15 Operative time ranged from 22 to 210 min (in some studies, the robotic docking was included in the operative time). The rate of conversion to open surgery was 0%. Eighteen of 48 patients had undergone previously unsuccessful neck explorations, in which 1 or more parathyroid glands were resected or partial thyroidectomy was performed. Almost all patients underwent technetium (99mTc) sestamibi (MIBI) imaging, neck ultrasound, and computerized tomography (CT) scan to confirm the existence of an ectopic parathyroid adenoma. Table 1 summarizes the characteristics, adenoma location, port placement, patient position, and results of the included studies.
Basic Characteristics of the Included Studies.
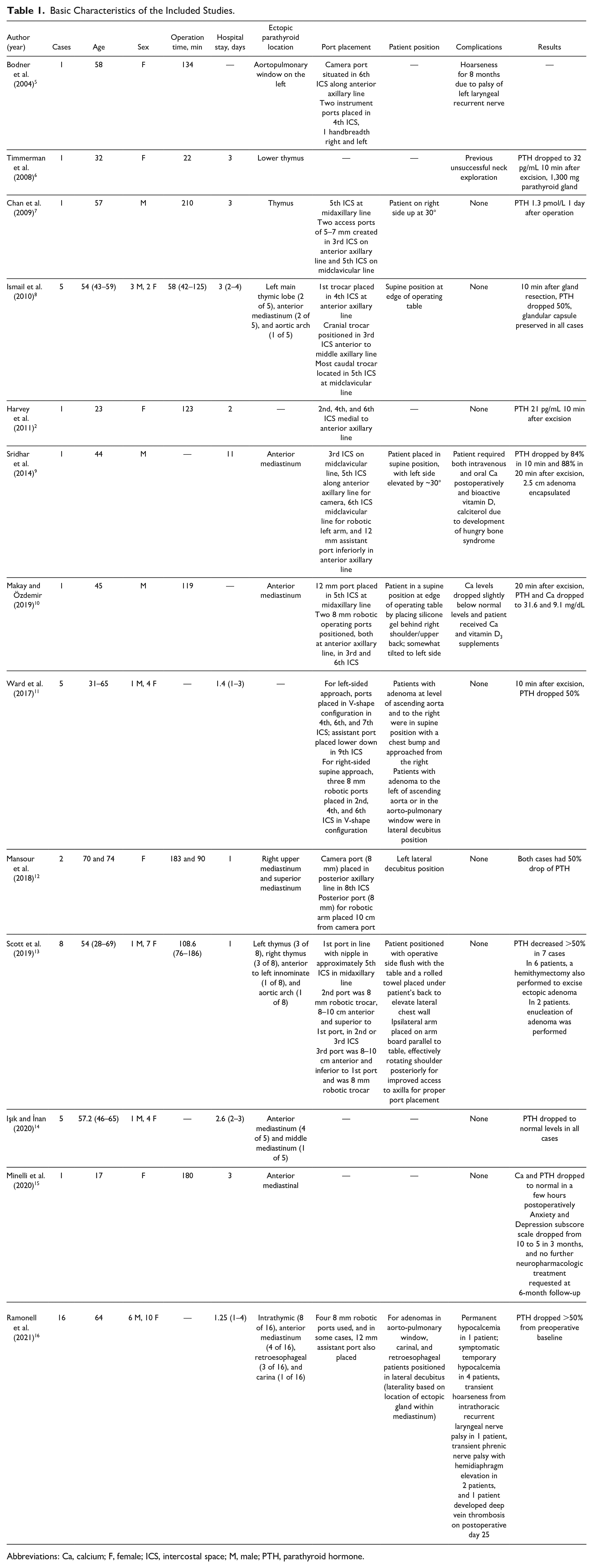
Abbreviations: Ca, calcium; F, female; ICS, intercostal space; M, male; PTH, parathyroid hormone.
Complications
Common complications that occurred following RATS ectopic parathyroid resection were hypocalcemia and recurrent laryngeal nerve damage. Bonder et al. described a patient who had transient hoarseness that resolved 8 months after the operation due to palsy of the left laryngeal recurrent nerve. 5 Sridhar et al. presented a case in which the patient developed hungry bone syndrome caused by postoperative parathyroidectomy hypocalcemia, which was resolved by administering intravenous and oral calcium (Ca), combined with bioactive vitamin D. 8 Makay et al. reported a patient in whom Ca levels dropped slightly below normal and was treated by calcium and vitamin D3 supplements. 10 Ramonell et al. reported that in a series of 16 patients, complications were deep vein thrombosis (1 of 16), hypocalcemia (1 of 16), symptomatic temporary hypocalcemia (4 of 16), and transient hoarseness from intrathoracic recurrent laryngeal nerve palsy (1 of 16). 16 In addition, Ramonell et al. reported that transient phrenic nerve palsy with hemidiaphragm elevation occurred in 2 of 16 patients. Both patients with hemidiaphragm elevation were asymptomatic and diagnosed incidentally on a routine postoperative chest x-ray at the 2-week postoperative visit. 16
Discussion
The most important factor for successful surgical resection of symptomatic parathyroid ectopic tissue is the precise preoperative localization. The exact location of the ectopic parathyroid adenoma could be found in many different anatomical locations including intrathymic, retroesophageal, carina, or aortopulmonary window compartment. Preoperative chest CT scan combined with MIBI demonstrates high accuracy in identifying the location of parathyroid tissue. 13 The study from Işık et al. emphasizes the importance of preoperative localization of the parathyroids, especially in small-sized adenomas for which the exploration is even more challenging. 14 They found that the combination of ultrasound and MIBI scintigraphy as a preoperative imagining method had a sensitivity of up to 95% for determining the location of the adenoma. Among the included studies, a CT scan was performed preoperatively in all cases except for 2 patients in the Işık et al. 14 study, while MIBI was used to locate the adenoma in 13 of 14 studies.
RATS has a clear advantage over traditional open approaches such as sternotomy or thoracotomy, which are associated with high morbidity and long recovery time.8,12 RATS parathyroidectomy is considered effective, 12 safe, and accurate, 7 while patients report fast recovery, 12 fewer complications, decreased pain, 17 and better cosmetic effect. 9 Robotic surgical complex filters a surgeon’s natural tremor, downscaling operator movements, 7 offering a stable operative field, and providing flexible instruments that help surgeons gain access to narrow anatomical spaces such as the mediastinum. 8 Due to its 3-dimensional vision, RATS provides a stable operative field, more dexterity, and magnification. Given its magnified vision, RATS could provide a precise distinction between the parathyroid tissue and other adjacent anatomical structures that are important to preserve including the phrenic nerve, thymus gland, and other big vessels such as the carotid artery sheath, external jugular vein, and brachiocephalic vein. 8 Moreover, the da Vinci robotic system (Intuitive Surgical, Sunnyvale, CA, USA) provides flexible instruments with 7-degree freedom that help surgeons to excise the ectopic adenoma by easily navigating through the narrow anatomical structures of the mediastinum.2,8 The aforementioned features of robotic surgery could provide a significant advantage over the VATS approach given its ability to precisely operate in the superior mediastinum and technically challenging fields and conditions, including redo surgeries.2,8 It significantly enhances surgeon ergonomic positioning, helping them operate more comfortably for longer periods of time. 7 Furthermore, the RATS approach could be an alternative to sternotomy, especially in morbidly obese patients with multiple comorbidities who could potentially not tolerate an open sternotomy or thoracotomy procedure. 9 To that extent, the authors would like also to comment on the flexibility and freedom of the robotic instruments. The VATS approach and its rigid instruments may pose a major restriction to dissection of adenomas in deep mediastinum locations. In contrast, a robotic approach with its instrument flexibility facilitates dissection in deep tissue planes.
On the other hand, the main criticism of RATS includes the cost-effectiveness and the long learning curve. 7 Park and Flores analyzed the operative cost of RATS, VATS, and thoracotomy approaches to pulmonary lobectomy. 18 They presented 269 patients who underwent thoracotomy and lobectomy, 87 who underwent VATS, and 12 who underwent RATS procedures. The operation length was similar in all cases, while the mean hospital stay was 6 days for patients who underwent thoracotomy and 4 days for those with either VATS or RATS procedures. In their study they found that the cost of thoracotomy lobectomy was on average higher than VATS by $8,368 USD, while the use of robotic technology during VATS lobectomy was associated with increased cost for the minimally invasive approach, adding on average $3,981 USD compared with VATS alone. 18 Despite the fact that the da Vinci system has enormous purchase, service, and surgical instrument costs compared with the VATS technique, the robot has proven to be equally effective in the long term, helping hospitals reduce costs by providing reduced hospitalization for the patients, minimizing the risk of disease recurrence, being associated with fewer postoperative complications that may need further medical treatment. Indeed, similar conclusions have been made based on mediastinal minimally invasive operations. Imielski et al. compared the cost-effectiveness of RATS, VATS, and open surgery in thymectomy. Their study concluded that minimally invasive techniques such as VATS and RATS were associated with lower associated costs and improved postoperative recovery. 19 In general, the current literature supports that VATS and robotic thoracic surgery procedures are associated with increased cost and a greater learning curve.
RATS has also been found to have a high training cost for surgeons and nurses and that a long learning curve is needed for surgeons to operate safely and effectively using robotic surgical systems. 2 Ectopic parathyroid is a rare entity in general; thus, thoracic surgeons are not widely exposed to numerous cases for proper training. The learning curve is not easily attainable. However, due to similar applications of the technique for other thoracic operations such as thymectomy and lobectomy, surgeons are finally going to be able to corroborate their expertise.
Conclusions
The current literature supports RATS as a safe and efficient alternative for the resection of ectopic parathyroid glands in the mediastinum, providing surgeons with greater comfort and helping them operate with more precision due to flexible instruments. The findings of our study support the use of RATS as an alternative to VATS and the open thoracotomy approach for the removal of thoracic ectopic parathyroid adenomas. It is difficult to fully calculate the long-term cost-effectiveness of the robotic system because it depends on the volume of RATS operations performed by each medical center. Based on our experience in a hospital environment where the robotic system already exists and is utilized by many departments (i.e., urology, general surgery, gynecology, etc.), we recommend that thoracic surgeons with prior experience in robotic surgery implement it also for ectopic parathyroidectomy located in the thoracic region. Future studies are needed to assess the cost-effectiveness and favorable postoperative outcomes of the RATS mediastinal ectopic parathyroid tissue resection approach. Studies that compare RATS to VATS or open approach are essential to elucidate further differences in short-term and long-term postoperative outcomes of the mediastinal ectopic parathyroid tissue removal.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.