
Abstract
In this article, we focus on the important role of robot-assisted coronary surgery by reporting the successful case of a morbidly obese male (body mass index = 58 kg/m2) who presented to our center with severe coronary disease. A 54-year-old morbidly obese male presented with acute chest pain and was diagnosed with coronary artery disease. The culprit lesion was the left anterior descending (LAD) coronary artery. A percutaneous coronary intervention angiography attempted in a university hospital was not successful. Our heart team chose a hybrid robot-assisted revascularization (HCR) strategy based on the patient’s body size. The patient underwent left internal thoracic mammary artery to LAD bypass with uneventful postoperative recovery. Robotic HCR is a valuable strategy in morbidly obese patients undergoing coronary artery bypass grafting.
Introduction
To understand the importance of minimally invasive robot-assisted coronary artery bypass grafting (CABG) in morbidly obese patients with coronary artery disease, we describe the case of a 54-year-old male with morbid obesity (body mass index [BMI] = 58 kg/m2) and multiple comorbidities presenting with chest pain and treated with off-pump minimally invasive direct coronary bypass (MIDCAB) and percutaneous coronary intervention (PCI) in the context of hybrid coronary revascularization (HCR).
Case Report
A 54-year-old male with a BMI of 58 kg/m2 (194 kg) presented with acute chest pain. He also reported dyspnea after 50 feet of walking, which resolved 5 min after stopping activity. His medical history was remarkable for morbid obesity (with a max BMI of 67 kg/m2; Fig. 1), hypertension, hyperlipidemia, diabetes mellitus type 2, 4 episodes of pulmonary embolism from deep vein thrombosis of the lower extremities (in treatment with rivaroxaban), statin intolerance, inflammatory bowel disease, neuropathy, chronic opioid use, obstructive sleep apnea, hypothyroidism, asthma, hepatic steatosis, former smoker, and positive family history of cardiac disease. Previous operations included gastric sleeve in 2010 (lowest weight was 320 lb). The patient signed consent for publication of his medical information.
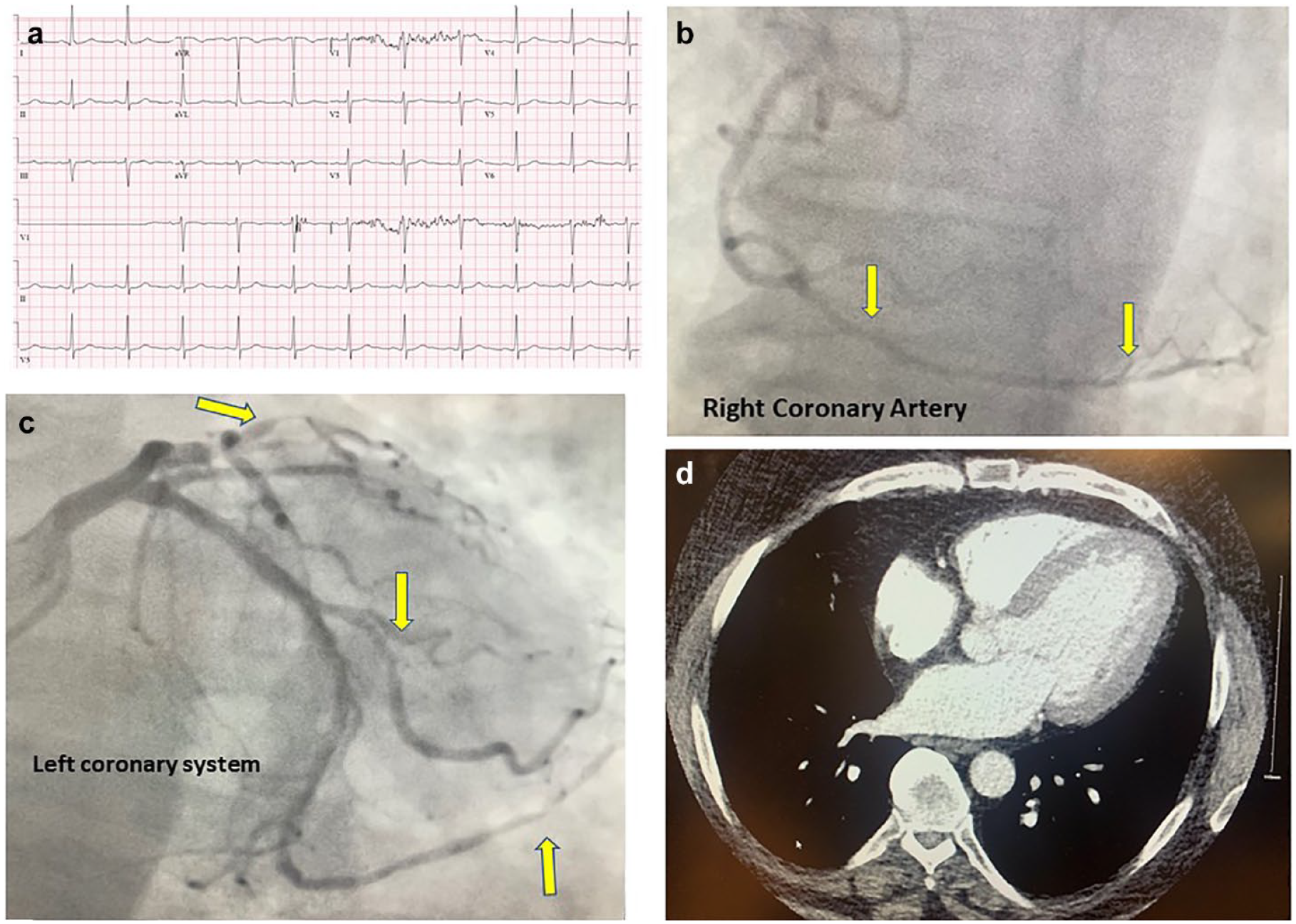
Investigation outcomes. (a) Electrocardiogram, (b) right coronary system, (c) left coronary system, and (d) computed tomography scan of the chest.
The preoperative electrocardiogram was normal sinus rhythm (Fig. 1a), but the troponin level was high. Transthoracic echocardiography showed an ejection fraction of 65% and no regional wall abnormalities (Supplemental Video 1). A computed tomography scan for pulmonary embolism was normal (Fig. 1d). Coronary angiography found a culprit lesion of the proximal to mid left anterior descending artery (LAD) with 70% stenosis, 80% stenosis of first diagonal branch, 70% stenosis of second diagonal branch, 60% stenosis of proximal marginal branch (OM), and 60% stenosis of proximal right coronary artery (RCA) extending to the posterior descending artery (PDA; Fig. 1b-c). Previous spirometry revealed a mildly reduced forced expiratory volume in 1 second of 2.54 L or 63%. The patient was then admitted to a tertiary hospital and underwent an unsuccessful chronic total occlusion reperfusion of the LAD due to the excessive amount of coronary calcium. Therefore, the patient was transferred to our center for further management.
Management
The heart team opted for off-pump MIDCAB with robot-assisted harvesting of the left internal thoracic artery (LITA). In this context, MIDCAB can become problematic due to CO2 insufflation in the chest and to the diaphragm compressing the lungs. To prevent ventilation complications during MIDCAB, 2 reinforced femoral vein sheaths were introduced bilaterally in case urgent venous-arterial extracorporeal membrane oxygenation would be necessary. Eventually, femoral cannulation would have been performed percutaneously in order to avoid surgical isolation of the vessels in such a morbidly obese patient. The patient underwent MIDCAB with a Medistim (Oslo, Norway) flow of 157 mL/min (Supplemental Video 2), was extubated on day 1, and was discharged home on day 4. Medical treatment at discharge included aspirin 325 mg, rivaroxaban, angiotensin-converting enzyme inhibitor, ezetimibe, and beta-blocker. He underwent PCI of the PDA and OM at 1 month after the procedure, and the LIMA-LAD anastomosis was functional. At 1-month follow-up, he did not report any new anginal episode.
Discussion
Considering the overall case scenario, the following findings appear relevant:
Hybrid robot-assisted CABG can be a valid therapy in morbidly obese patients. The procedure permits the avoidance of sternotomy complications (for example, diastasis and infection), while presenting a lower rate of postoperative pain, shorter intubation time, as well as shorter hospital length of stay.1–4
Fast postoperative recovery is of extreme importance in this type of patient, and MIDCAB is of great help for fast extubation and prompt rehabilitation.
The combined advantages of sternal sparing, off-pump surgery, reduced ventilation time, and atrial fibrillation incidence are key factors for the good outcomes in this subset of patients.
Robotic HCR is a valid alternative in morbidly obese patients and must be considered from the heart team as an optional treatment.
In morbidly obese patients, after robotic LITA harvesting (great care is taken to avoid injury to the left phrenic nerve), a 4 cm left thoracotomy can be done at the fourth intercostal space with good exposure of the target LAD. Obese patients with chronic obstructive pulmonary disease (COPD) may have a difficult surgical exposure, and the need for an increased amount of CO2 insufflation can be tempting. However, one should keep in mind that CO2 insufflation is not complication free in patients with COPD.
Conclusions
Hybrid robotic-assisted revascularization is a useful strategy in morbidly obese patients undergoing CABG.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.