
Abstract
Background:
Fibroadenomas, common benign breast tumors in women of reproductive age, are increasingly managed with minimally invasive radiofrequency ablation (RFA) or surgical excision. However, their impact on breastfeeding outcomes remains underexplored. We aimed to assess breastfeeding ability and breast tissue changes in women treated with RFA or surgery compared to those with untreated fibroadenomas.
Methods:
In this retrospective cohort study, we evaluated 153 women with biopsy-confirmed fibroadenomas across five groups: RFA with prior breastfeeding (RFA-PreBF; n = 26), RFA with posttreatment breastfeeding (RFA-PostBF; n = 22), surgical excision with prior breastfeeding (Surgical-PreBF; n = 30), surgical excision with posttreatment breastfeeding (Surgical-PostBF; n = 20), and noninterventional with breastfeeding (Observation-BF; n = 55). Breastfeeding ability was assessed using a 5-point scale, and breast tissue changes were evaluated via ultrasound at 18 months, and all breastfeeding attempts occurred at a minimum of 12 months postprocedure. Fisher’s exact test compared complete lactation failure rates, and a power analysis validated the study design (Fig. 1).
Findings:
The combined RFA group (n = 48) had a higher complete lactation failure rate (14.6%) than the Observation-BF group (3.6%; Fisher’s exact test, p = 0.045). Similarly, the combined surgical group (n = 50) had a higher complete lactation failure rate (16.0%) than the Observation-BF group (p = 0.034). When pooled, the combined intervention group (n = 98) showed a complete lactation failure rate of 15.3% versus 3.6% in the Observation-BF group. Residual tissue correlated with lactation impairment in the RFA group (Spearman’s ρ, p < 0.05). Ultrasound showed no tumor recurrence, with cystic changes in some cases not linked to breastfeeding impairment. Power analysis confirmed 80% power to detect a medium effect size (f = 0.25, Fig. 1), supporting the study’s robustness.7 RFA-PreBF (n = 26), RFA-PostBF (n = 22), Surgical-PreBF (n = 30), Surgical-PostBF (n = 20), and Observation-BF (n = 55). Breastfeeding ability was assessed using a 5-point scale, and breast tissue changes were evaluated via ultrasound at 18 months. Fisher’s exact test compared complete lactation failure rates, and a power analysis validated the study design (Fig. 1).
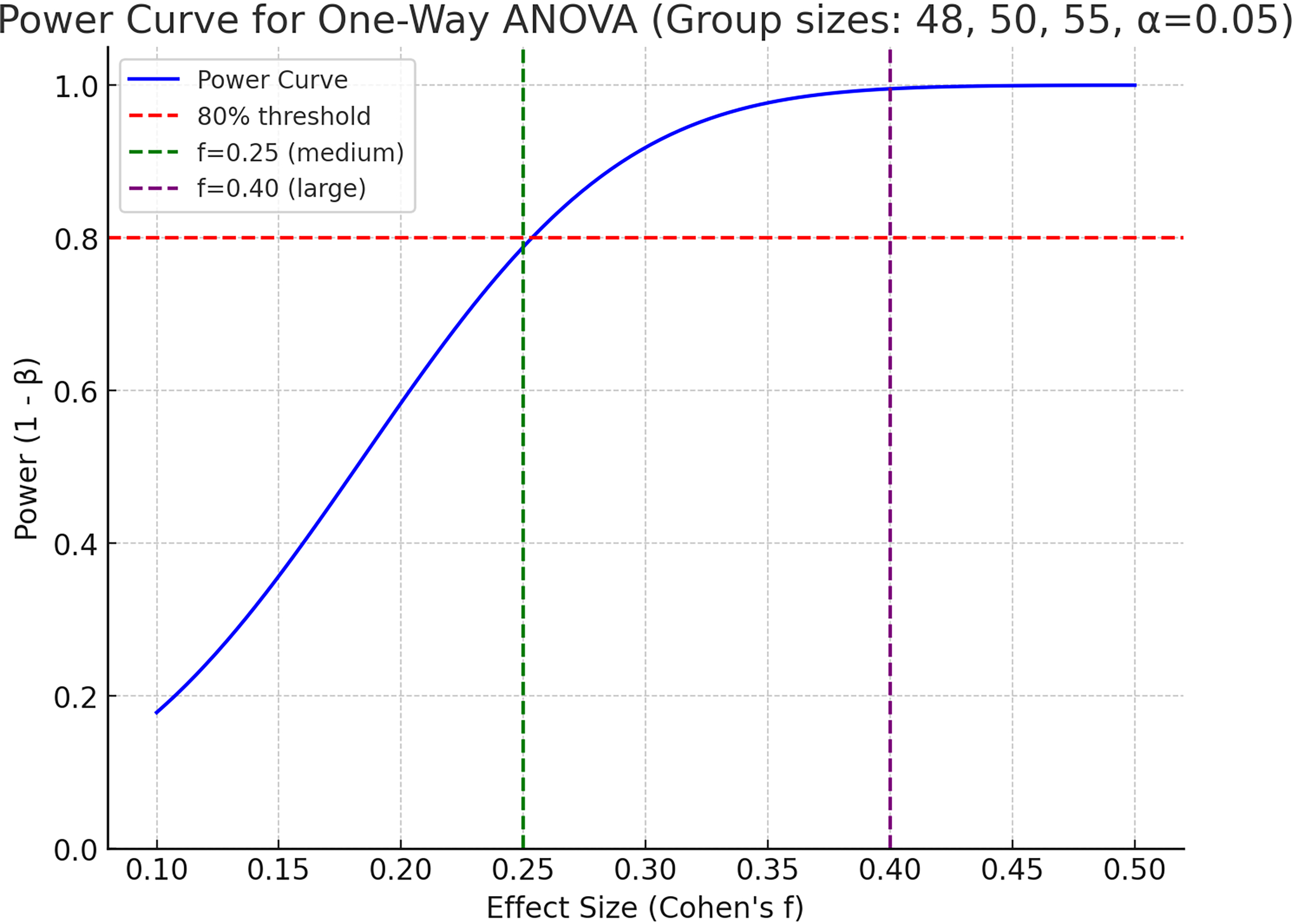
Power Analysis Curves for Breastfeeding Outcome Differences. Power curves illustrate the study’s statistical power to detect differences in Complete Lactation Failure rates across groups (RFA, surgical excision, and observation) using one-way ANOVA (α = 0.05). The study achieved 80% power for a medium effect size (f = 0.25) with group sizes of 48, 50, and 55. Power estimates for other effect sizes are shown: f = 0.20 (60%), f = 0.22 (69%), f = 0.28 (89%), f = 0.30 (93%), f = 0.35 (98%), f = 0.40 (99.6%).
Interpretation:
RFA and surgical excision are effective for fibroadenoma management but increase the risk of complete lactation failure compared to untreated fibroadenomas. Careful patient selection, precise procedural techniques, and vigilant posttreatment monitoring are essential to optimize breastfeeding outcomes, particularly for women planning future pregnancies.
Keywords
Get full access to this article
View all access options for this article.