
Abstract
Background:
Pedicle screw placement during spine fusion is physically and mentally demanding for surgeons. Consequently, spine surgeons can become fatigued, which has implications for both patient safety and surgeon well-being.
Purpose:
We sought to assess the cognitive workload of surgeons placing pedicle screws using robotic-assisted navigation compared with fluoroscopic and computed tomography (CT)-assisted placement.
Methods:
We performed a nonrandomized prospective controlled trial to compare the cognitive workload of 3 surgeons performing single-level minimally invasive transforaminal lumbar interbody fusion (MI-TLIF) using robotic, CT, or fluoroscopic navigation on 25 patients (15 in the robotic navigation group and 10 in the nonrobotic group). Immediately after each procedure, surgeons submitted the National Aeronautics and Space Administration–Task Load Index (NASA-TLX), which has 6 subscales: mental demands, physical demands, temporal demands, performance, effort, and frustration. Four tasks associated with pedicle screw placement were assessed independently: (1) screw planning, (2) calibrating robot/obtaining imaging/registration, (3) pedicle cannulation, and (4) screw placement. Patient demographics and surgical characteristics were obtained and reviewed.
Results:
Surgeons’ self-reported cognitive workload was significantly reduced when using robotic-assisted navigation versus CT/fluoroscopic navigation. Workload was reduced for screw planning, pedicle cannulation, and screw placement. In addition, there were significant reductions in each subdomain for these 3 tasks, encompassing mental demand, physical demand, temporal demand, effort, and frustration with improved task performance.
Conclusions:
This study found significant reductions in mental workload with improved perceived performance for robotic-assisted pedicle screw placement compared with fluoroscopic and CT-navigation techniques. Lowering the cognitive burden associated with screw placement may allow surgeons to address the remainder of the operative case with less decision fatigue, prevent complications, and increase surgeon wellness.
Introduction
For surgeons, pedicle screw placement during spine fusion surgery is physically and mentally demanding, as inaccurately placed screws can result in significant postoperative complications due to the proximity of critical neurovascular structures. Placing pedicle screws is a repetitive task and spine surgery requires constant focus, attention, physical endurance, and meticulous fine motor skills [15]. Surgeons’ physical and mental fatigue can have implications on both patient safety and surgeon well-being. The ability to quantify and measure a surgeon’s workload is imperative to prevent potential patient complications as well as professional burnout, with as many as 38% of orthopedic surgeons and 30% of spine surgeons experiencing burnout in their career [1,11,19,21,22,25].
Fluoroscopy-based techniques, computed tomography (CT)-based navigation, and more recently robotic-assisted spine surgery (RASS) were introduced to help surgeons place pedicle screws accurately [14,15]. Studies have reported improved accuracy of screw placement with robotics compared with CT-navigation and freehand techniques [7,26]. In addition, these systems use software that allows the surgeon to plan and template screw trajectories preoperatively, which may reduce the mental demand of preoperative templating. Robotic surgery systems offer several purported advantages over CT-based navigation. The use of a robotic arm while placing pedicle screws reduces physical fatigue, improves ergonomics, and improves dexterity. Given the repetitive nature of placing pedicle screws, the use of RASS may reduce both physical and mental workload. Studies assessing the mental workload of surgeons using robotic systems have been well-reported in other surgical applications but remain relatively unknown in spine surgery [3,12,13,18,17,20].
While robotic systems enable safe and accurate screw placement, skepticism remains about whether robotic technology adds adequate value to justify the considerable capital cost [8,24]. Although few studies have quantified the impact of robotics beyond screw-placement accuracy, its true effect may exceed this narrow metric. The ability to execute preoperative plans with the assistance of a robotic arm could reduce the cognitive burden associated with placing pedicle screws, which in turn may allow surgeons to address the remainder of the case with less decision fatigue.
The purpose of this study was to assess the cognitive workload of surgeons during RASS compared with CT-based navigation and fluoroscopic screw placement. We hypothesized that the cognitive workload would be reduced for surgeons using robotic screw placement compared with other methods.
Methods
We performed a nonrandomized prospective controlled trial to assess and compare the cognitive workload of surgeons performing single-level minimally invasive transforaminal lumbar interbody fusions (MI-TLIF) using robotic, CT, or fluoroscopic navigation. The protocol was approved by the HSS Institutional Review Board (2020-2429). All patients and surgeons provided written informed consent prior to enrollment.
Patients were included if they were 18 years old or older and were undergoing a single-level MI-TLIF. Patients were excluded if they had a contraindication to MI-TLIF, had history of a prior fusion at the operative level, were undergoing a multilevel fusion, or had a suspected infection or tumor. Surgeons were eligible if they were fellowship-trained attending spine surgeons and had prior experience with robotic navigation, CT-guided navigation, and fluoroscopic navigation. Residents and fellows were excluded to prevent differences in the learning curve and experience [1].
Patients were assigned to either (1) a robotic navigation group or (2) a nonrobotic group consisting of CT-guided navigation and fluoroscopic pedicle screw placement. Groups were assigned at the discretion of the surgeon and equipment availability and not through randomization. The nonrobotic group consisted of both CT and fluoroscopic placement, depending on the technique each surgeon commonly used in practice. Immediately following each procedure, the surgeon’s cognitive workload was assessed using a validated task load index (TLX) developed by the North American Space Association (NASA) [10].
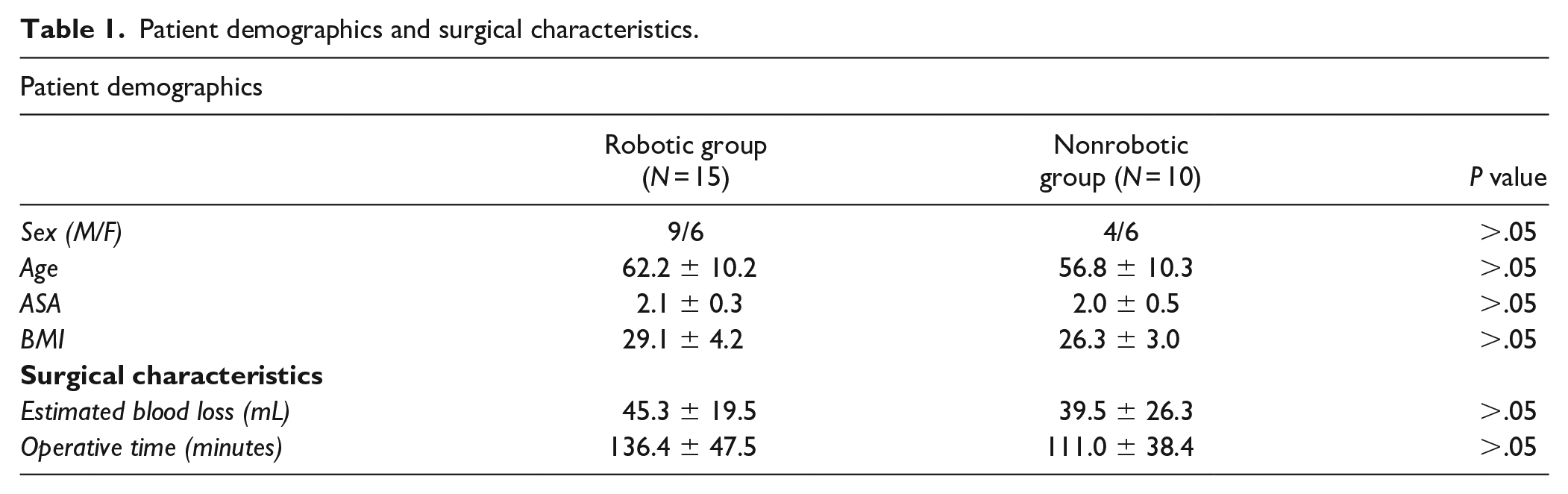
A total of 3 surgeons and 25 patients were available for analysis (Fig. 1). A total of 15 patients were enrolled in the robotic navigation group and 10 in the nonrobotic group. Each surgeon contributed 5 patients to the robotic navigation group, while 1 surgeon contributed 5 patients to the fluoroscopic group, and 1 surgeon contributed 5 patients to the CT-based navigation group. Given the between-group differences, enrollment was stopped early and a post-hoc power analysis confirmed 99.1% power with the final enrollment numbers. There were no demographic differences between groups, with an overall mean age of 60.1 ± 10.4 years and body mass index (BMI) of 28.0 ± 4.0 (Table 1).
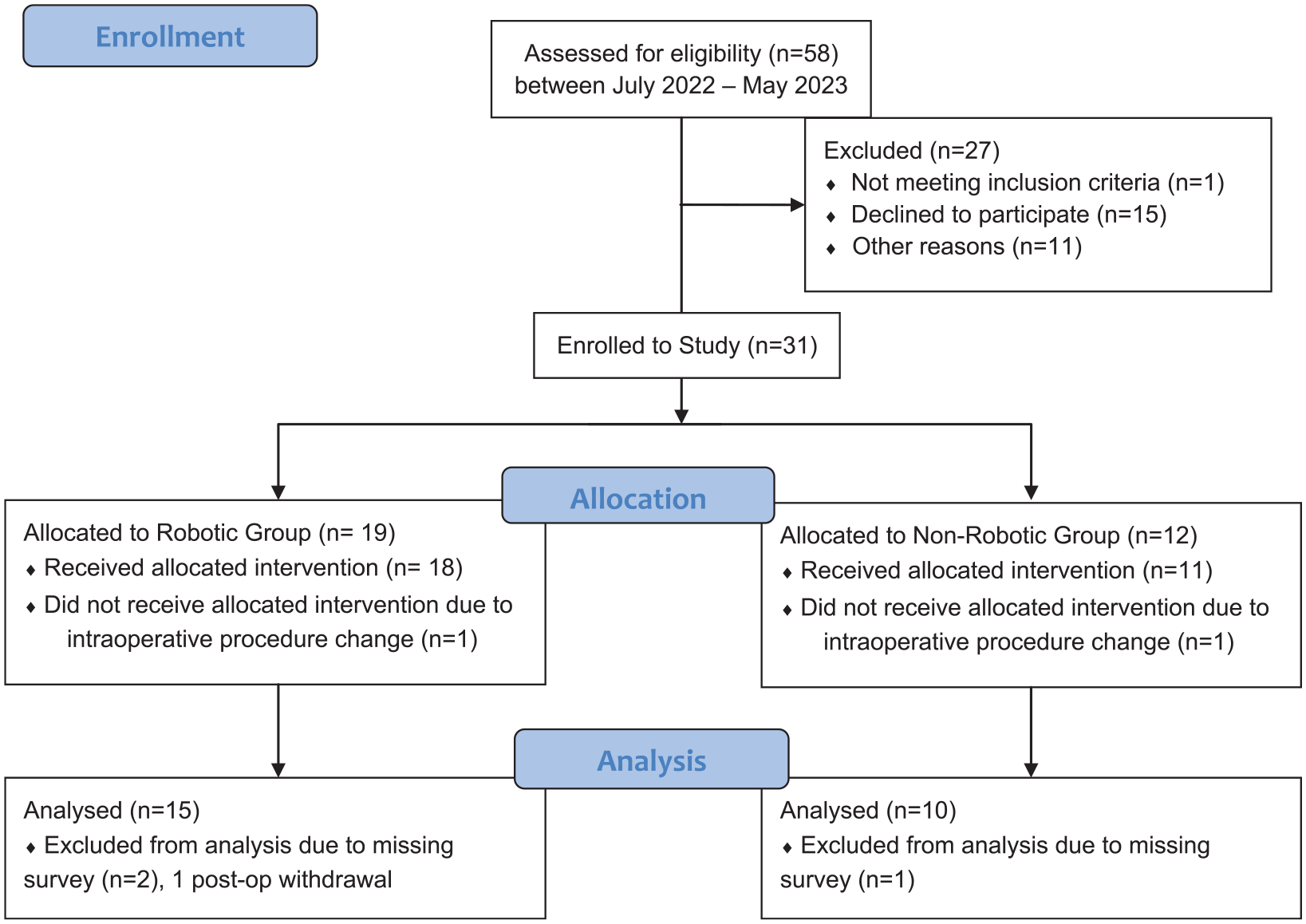
Enrollment flow diagram.
Patient demographics and surgical characteristics.
The NASA-TLX, initially developed in the 1980s to assess workload for use in aviation, estimates the overall mental workload required for a specific task; it was validated over a 3-year period including test-retest experiments [10]. The instrument has been translated into several languages and used across multiple industries to assess cognitive workload. Health care applications include a variety of robotic general surgery procedures, and recently the index was used to assess workload in primary and revision total knee arthroplasty [9,10,16,17,20]. The instrument rates 6 subscales: mental demands, physical demands, temporal demands, performance, effort, and frustration [10,17]. Mental demand is the comprehensive intellectual and perceptual work required to complete a task, while physical demand includes the actual physical effort involved in task completion. Temporal demand is the effect of time. Performance reflects the surgeon’s own appraisal of satisfaction following completion. Effort is a combination of both mental and physical demands, while frustration reflects the surgeon’s stress level [10,17].
For surgeons, 4 specific tasks associated with pedicle screw placement were created, including: (1) screw planning, (2) calibrating robot/obtaining imaging/registration, (3) pedicle cannulation, and (4) screw placement. Greater values indicate increased mental workload.
Administration of the NASA-TLX involves 2 steps. Prior to rating the task itself, the participant rates the importance of the 6 subscales using pairwise comparisons to build an understanding of their own workload. Following each case, surgeons were asked to rate each task. A weighted score for each participant is then calculated based on their preferences for workload. The instrument is then given, and individuals rate the task for each of the 6 subdomains from 0 to 100 with 5-point gradations.
In addition, both patient characteristics and surgery characteristics were collected. Patient characteristics included the American Society of Anesthesiology (ASA) Score and BMI. Surgical factors included operative time (time from incision to closure). Intraoperative events were also recorded.
Statistical Analysis
We estimated a sample size of 30 patients (15 in each group with 3 participating surgeons), with preliminary analyses planned at 1/3 and 2/3 enrollment with a post-hoc power analysis performed following final confirmation of enrollment (α = .05, β = .2).
Statistical analysis was performed with GraphPad PRISM v7.04. The primary outcome was the mental workload of surgeons following robotic and CT-navigation pedicle screw placement using the NASA-TLX score. An as-treated analysis was performed. Two-way analyses of variance were used, followed by post-hoc testing between groups to assess mean differences between pedicle screw placement techniques. Secondary outcomes included patient and surgical factors associated with increased mental workload such as BMI and operative time. Fisher’s exact test was utilized as appropriate.
Results
We found no differences in operative characteristics (Table 1), although there was 1 reported registration failure, which required re-calibration of the robotic platform. No other intraoperative events were noted.
We found a significantly reduced cognitive workload in surgeons using robotic-assisted navigation versus CT/fluoroscopic navigation (20.2±12.1 vs 45.3±15.5, respectively; P < .001). Workload was reduced for screw planning (20.6±10.9 vs 45.02±13.0, respectively; P < .001), pedicle cannulation (11.9±9.6 vs 51.5±14.7, respectively; P < .001), and screw placement (14.8±10.2 vs 49.6 vs 11.6, respectively; P < .001). In addition, there were significant reductions in all 6 subdomains for these 3 tasks (Fig. 2a, b, d).
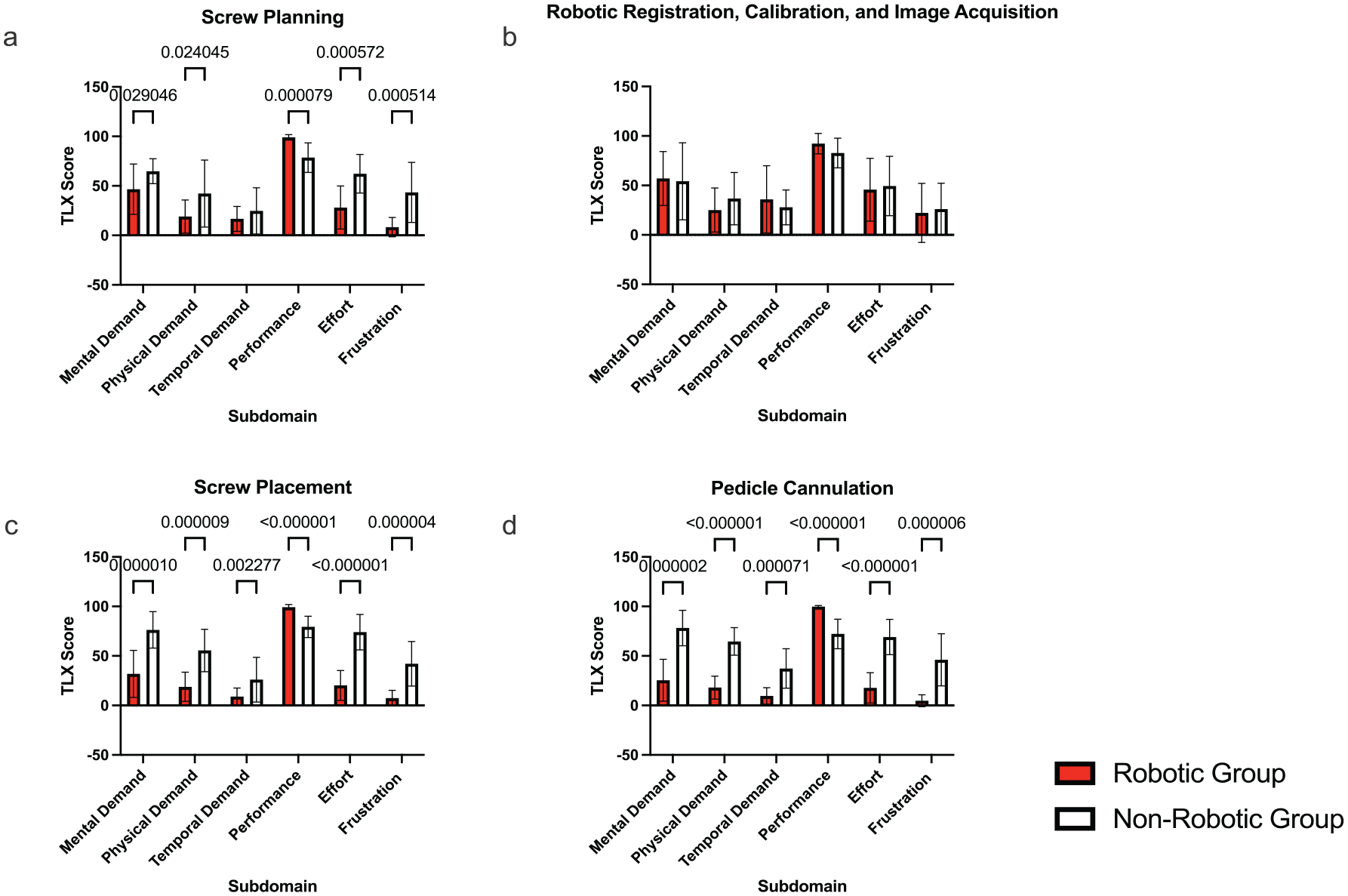
North American Space Association–Task Load Index (NASA-TLX) scores by task. (a) Screw planning. (b) Robotic registration, calibration, and image acquisition. (c) Screw placement. (d) Pedicle cannulation.
There was no difference in mental demand for robotic calibration imaging acquisition and registration versus CT/fluoroscopic navigation (33.6±17.5 vs 35.0±22.5, respectively; P > .05) and subsequently no differences in the subdomains between groups (Fig. 2c).
Summed across the entire case, there was an overall reduction in cognitive workload in each subdomain with improved performance placing pedicle screws using robotic navigation concurrently with reduced frustration, effort, mental demand, temporal demand, and physical demand (Fig. 3).
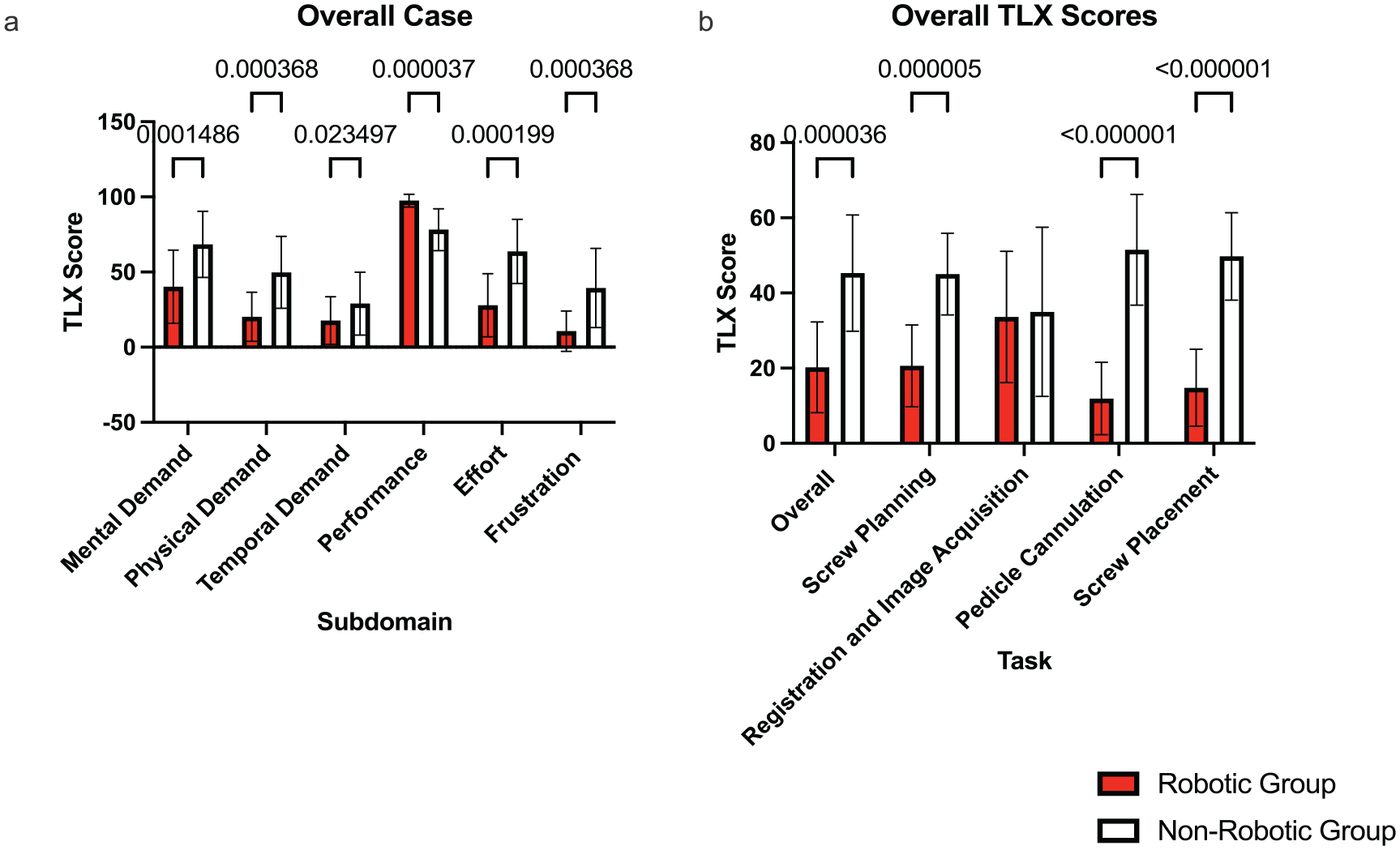
Overall North American Space Association–Task Load Index (NASA-TLX) Scores. (a) Overall NASA-TLX scores for each subdomain (mental demand, physical demand, temporal demand, performance, effort, and frustration). (b) Overall NASA-TLX scores for each task (overall case, screw planning, registration and image acquisition, pedicle cannulation, and screw placement).
There were multiple correlations between patient and surgical factors and workload for each task (Supplemental Figs. 1-4). For the robotic group, there was a negative correlation with BMI and screw planning (P < .05) (Supplemental Fig. 1). In addition, when placing screws with robotic assistance, increased operative time was correlated with decreased workload for the overall case (P < .02), screw planning (P < 0< .001), pedicle cannulation (P < .02), and screw placement (P < .0001) (Supplemental Fig. 3). Finally, for the robotic cases, increased blood loss was correlated with decreasing workload (P < .05).
However, when placing screws with either CT or fluoroscopic guidance, increasing operative time was correlated with increased workload for the overall case (P < .02), registration and image acquisition (P < .001), pedicle cannulation (P < .05), and screw placement (P < .05) ( Supplemental Fig. 4 ).
Discussion
We found significant reductions in surgeons’ mental workload in pedicle screw placement for surgeons using robotic-assisted compared with fluoroscopic and CT-navigation techniques. While multiple studies have assessed accuracy in pedicle screw placement, the assessment of surgeons’ mental workload when utilizing robotic techniques is underreported. This study demonstrates the utility of robotic platforms in lowering spine surgeons’ mental workload while placing pedicle screws. Lowering the cognitive burden associated with screw placement may allow surgeons to address the remainder of the operative case with less decision fatigue and fewer complications while increasing surgeon wellness.
This study has limitations. While it was performed prospectively, it was not randomized, which introduces a potential selection bias; this was mitigated with no demographic differences between the treatment groups. Another potential source of selection bias is our exclusion of freehand screw placement, as a surgeon may prefer this technique. The inclusion of this technique would have been difficult for a MI-TLIF procedure, as freehand pedicle screw placement would require muscular dissection of the screw entry points—not routinely performed in this procedure. In addition, we did not include biometric data. Recently, wearable technology has been used to measure heart rate variability (HRV), which is a measure of overall health [11]. A higher HRV is associated with decreased mental fatigue during task completion, and a lower respiratory rate and normal sleep are associated with decreased mental fatigue [11]; the association of these biometrics with cognitive workload as measured by the TLX in spine surgery is an area for future study. Furthermore, while our recruitment numbers varied by surgeons and there was no internal control, enrollment was stopped early given between-group differences, with a post-hoc analysis confirming appropriate power with the final analysis. Also, the NASA-TLX is a self-report instrument and is therefore susceptible to recall bias, a limitation we mitigated through asking participants to complete it immediately after performing the procedure. Finally, some of the authors have a financial relationship with the makers of the robotic platform used for this study, although it was conducted without financial or other direct support from the manufacturer.
Recent studies analyzing robotic navigation focus on screw accuracy and the surgeon learning curve. This is the first multisurgeon study to specifically analyze cognitive workload. Of the 4 tasks assessed, the 3 surgeons rated improved performance in screw planning, screw placement, and pedicle cannulation when using robotic navigation compared with nonrobotic techniques. This increase in performance was accompanied by reductions in mental demand, physical demand, temporal demand, effort, and frustration. Importantly, nonrobotic methods of pedicle placement still resulted in increased perceived performance but at the cost of increased mental workload. There were no differences found in workload associated with robotic calibration, image acquisition, and registration between groups. Multiple workflows exist on how to best manage this process, which may be a source of frustration.
Traditional measurements of workload have utilized the NASA-TLX and have been adapted to spine and neurosurgical procedures. Gabrovsky et al [5] reported reducing workload and enhancing performance with the use of a digital microscope for spine cases (mostly decompression procedures). In their series, a TLIF had a NASA-TLX performance score of 60, and scores of effort and frustration were each 40. Comparatively, we report an overall case performance score of 97.6±4.3 with effort and frustration scores of 27.9±21.0 and 10.7±13.4, respectively, when using the robotic platform to place pedicle screws. In addition, Gabrovsky et al [4] reported reduced NASA-TLX scores for robotically placed screws compared with fluoroscopically placed screws with a score of approximately 20 after the initial learning curve, similar to the overall scores that we report. High performance with both methods may be due to the surgeons’ familiarity with the equipment and overcoming the initial learning curve; all surgeons in our study had previously implemented robotic navigation into their practices.
Interestingly, there was a decreased workload associated with increased operative time when using robotic navigation although this was not the case when using CT or fluoroscopic-based techniques. Decreasing intraoperative cognitive burden may also have positive impacts on intraoperative stress levels, surgeon well-being, and longevity [2,19]. The decreased workload may allow surgeons to more effectively communicate with the operative team and improve overall performance [2]. Burnout, which is associated with increased workload and reported in up to 30% of spine surgeons [1], can contribute to alcohol abuse, depression, and lower quality of life, and therefore identifying technologies with the potential of decreasing it is imperative [6,19].
Enhancing the usability of robotic platforms, especially in methods that do not draw attention from the surgical field, is ongoing; tool-mounted interfaces have shown the potential to reduce workload [23]. Further enhancements may focus on aspects of the procedure other than screw placement, which may additionally reduce workload. Given the high cost of robotic platforms, the ability of a surgeon to perform cases continually at a high level is imperative and may help further justify the high initial capital expenditure for hospital systems. While the use of robotic techniques can lower a surgeon’s cognitive workload, it does not take away the difficulty of placing pedicle screws, and this fact should not be misconstrued as a conclusion from this study. In addition, in MI-TLIF, screw placement is just one part of the procedure, and further research is required to determine which aspect of the procedure leads to the highest workload. This will be important in designing processes and systems that can reduce surgeon workload while accomplishing their goals. The robotic platforms are an enabling technology that allows surgeons to fully draw on their experience; surgical training and a full understanding of the relevant anatomy are still required to prevent complications.
In conclusion, this study found significant reductions in the mental workload of spine surgeons, with improved perceived performance, when using robotic-assisted pedicle screw placement compared with fluoroscopic and CT-navigation techniques. Lowering the cognitive burden associated with screw placement may allow a surgeon to address the remainder of the procedure with less decision fatigue, prevent complications, and enhance surgeon wellness.
Supplemental Material
sj-docx-1-hss-10.1177_15563316241281064 – Supplemental material for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial
Supplemental material, sj-docx-1-hss-10.1177_15563316241281064 for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial by Kyle W. Morse, Tejas Subramanian, Eric Zhao, Omri Maayan, Yousi Oquendo, Catherine Himo Gang, James Dowdell, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316241281064 – Supplemental material for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial
Supplemental material, sj-docx-2-hss-10.1177_15563316241281064 for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial by Kyle W. Morse, Tejas Subramanian, Eric Zhao, Omri Maayan, Yousi Oquendo, Catherine Himo Gang, James Dowdell, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316241281064 – Supplemental material for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial
Supplemental material, sj-docx-3-hss-10.1177_15563316241281064 for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial by Kyle W. Morse, Tejas Subramanian, Eric Zhao, Omri Maayan, Yousi Oquendo, Catherine Himo Gang, James Dowdell, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316241281064 – Supplemental material for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial
Supplemental material, sj-docx-4-hss-10.1177_15563316241281064 for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial by Kyle W. Morse, Tejas Subramanian, Eric Zhao, Omri Maayan, Yousi Oquendo, Catherine Himo Gang, James Dowdell, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316241281064 – Supplemental material for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial
Supplemental material, sj-docx-5-hss-10.1177_15563316241281064 for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial by Kyle W. Morse, Tejas Subramanian, Eric Zhao, Omri Maayan, Yousi Oquendo, Catherine Himo Gang, James Dowdell, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316241281064 – Supplemental material for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial
Supplemental material, sj-docx-6-hss-10.1177_15563316241281064 for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial by Kyle W. Morse, Tejas Subramanian, Eric Zhao, Omri Maayan, Yousi Oquendo, Catherine Himo Gang, James Dowdell, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®
Supplemental Material
sj-docx-7-hss-10.1177_15563316241281064 – Supplemental material for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial
Supplemental material, sj-docx-7-hss-10.1177_15563316241281064 for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial by Kyle W. Morse, Tejas Subramanian, Eric Zhao, Omri Maayan, Yousi Oquendo, Catherine Himo Gang, James Dowdell, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®
Supplemental Material
sj-docx-8-hss-10.1177_15563316241281064 – Supplemental material for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial
Supplemental material, sj-docx-8-hss-10.1177_15563316241281064 for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial by Kyle W. Morse, Tejas Subramanian, Eric Zhao, Omri Maayan, Yousi Oquendo, Catherine Himo Gang, James Dowdell, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®
Supplemental Material
sj-docx-9-hss-10.1177_15563316241281064 – Supplemental material for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial
Supplemental material, sj-docx-9-hss-10.1177_15563316241281064 for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial by Kyle W. Morse, Tejas Subramanian, Eric Zhao, Omri Maayan, Yousi Oquendo, Catherine Himo Gang, James Dowdell, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®
Supplemental Material
sj-pdf-10-hss-10.1177_15563316241281064 – Supplemental material for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial
Supplemental material, sj-pdf-10-hss-10.1177_15563316241281064 for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial by Kyle W. Morse, Tejas Subramanian, Eric Zhao, Omri Maayan, Yousi Oquendo, Catherine Himo Gang, James Dowdell, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®
Supplemental Material
sj-pdf-11-hss-10.1177_15563316241281064 – Supplemental material for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial
Supplemental material, sj-pdf-11-hss-10.1177_15563316241281064 for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial by Kyle W. Morse, Tejas Subramanian, Eric Zhao, Omri Maayan, Yousi Oquendo, Catherine Himo Gang, James Dowdell, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®
Supplemental Material
sj-pdf-12-hss-10.1177_15563316241281064 – Supplemental material for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial
Supplemental material, sj-pdf-12-hss-10.1177_15563316241281064 for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial by Kyle W. Morse, Tejas Subramanian, Eric Zhao, Omri Maayan, Yousi Oquendo, Catherine Himo Gang, James Dowdell, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®
Supplemental Material
sj-pdf-13-hss-10.1177_15563316241281064 – Supplemental material for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial
Supplemental material, sj-pdf-13-hss-10.1177_15563316241281064 for Robotic-Assisted Navigation in Single-Level Transforaminal Lumbar Interbody Fusion Reduces Surgeons’ Mental Workload Compared With Fluoroscopic and Computed Tomographic Techniques: A Nonrandomized Prospective Controlled Trial by Kyle W. Morse, Tejas Subramanian, Eric Zhao, Omri Maayan, Yousi Oquendo, Catherine Himo Gang, James Dowdell, Sheeraz Qureshi and Sravisht Iyer in HSS Journal®
Footnotes
CME Credit
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KWM reports relationships with NIH, OREF, SRS, Johnson & Johnson, GE Health, and Sustain Surgical. SQ reports relationships with Viseon, Tissue Differentiation Intelligence, HS2, Minimally Invasive Spine Study Group, Stryker, SpineGuard, Globus Medical, Surgalign, Lifelink.com, Spinal Simplicity, Contemporary Spine Surgery, NASS, Annals of Translational Medicine, HSS Journal, Society of Minimally Invasive Spine Surgery (SMISS), Lumbar Spine Research Society (LSRS), Cervical Spine Research Society (CSRS), Association of Bone and Joint Surgeons (ABJS), and International Society for the Advancement of Spine Surgery (ISASS). SI reports relationships with Innovasis, HS2, Stryker, Healthgrades, and Globus Medical. The other authors declare no potential conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received the following financial support for the research, authorship, and/or publication of this article: This study used REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center For Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384. KWM was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under award number T32-AR078751. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was obtained for all patients included in this study.
Level of Evidence
Level II, Nonrandomized prospective controlled trial.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.