
Abstract
Background:
In the COVID-19 era, there has been increasing interest in same-day discharge (SDD) after total joint arthroplasty (TJA). However, patient perception of SDD is not well reported.
Purpose:
We sought to understand patients’ perceptions and preferences of postoperative care by surveying patients who have completed both an overnight stay (ONS) and an SDD after TJA.
Methods:
We emailed survey links to 67 patients who previously underwent either 2 total hip arthroplasties (THAs) or 2 total knee arthroplasties (TKAs).
Results:
Fifty-two patients (78%) responded to the survey. Thirty-four (65%) patients underwent staged, bilateral TKAs, and 18 (35%) patients underwent staged, bilateral THAs. Overall, 63% of patients preferred their SDD, 12% had no preference, and 25% preferred their ONS, with no difference in preference between TKA and THA groups. Those who preferred their SDD reported being more comfortable at home. Those who preferred their ONS felt their pain and concerns were better addressed. No differences were found in comfort, sleep quality, appetite, burden on family, return to function, feelings of being discharged too soon, overall experience, 30-day emergency department (ED) visits, or readmissions within 30 days between patients’ SDD and ONS. There was a small statistically significant difference between patients’ perception of safety between SDD and ONS.
Conclusion:
Our survey found that most patients reported a preference for SDD after TJA over ONS. Although there was a small difference in patient perception of safety, there were no differences in return to the ED or readmissions after SDD and ONS.
Introduction
Same-day discharge (SDD) after total joint arthroplasty (TJA) has garnered increasing interest, especially during the COVID-19 pandemic, when the risk of hospital-acquired infection was high and hospital resources were needed for COVID patients. Same-day discharge offers several additional benefits over traditional overnight stay (ONS) after TJA, including potential for faster rehabilitation, reduced reliance on hospital resources, the ability to more easily control the surgical care environment in more efficient ambulatory surgery centers, and reduced costs [1,2,10,11]. Most importantly, it has been proven to be safe in appropriately screened patients [5,6,9,13,14,17].
Many benefits of SDD have been assessed from the surgeon’s perspective. Goyal et al [6] randomized patients undergoing total hip arthroplasty (THA) to either SDD or ONS. They found that SDD patients reported higher pain scores on postoperative day 1, but that there was no difference in the number of reoperations, hospital readmissions, emergency department (ED) visits, acute office visits, or patient phone calls between groups. Pollock et al [14] performed a systematic review to evaluate the safety of SDD joint arthroplasty and concluded that SDD has similar complication rates to ONS and that SDD is safe in appropriately selected patients.
Patients’ perceptions of SDD after TJA are lacking. Patients who have undergone both SDD and ONS after TJA represent a unique cohort as they can make a direct comparison between experiences.
We sought to (1) examine the percentage of patients preferring SDD compared to ONS; (2) examine survey responses regarding why they selected a given preference; and (3) compare patient ratings of their experience of SDD and ONS. We hypothesized that most patients would prefer SDD over ONS.
Methods
After obtaining institutional review board approval, 67 patients were retrospectively identified who previously underwent either 2 THAs or 2 total knee arthroplasties (TKAs), of which the first surgery was done as an ONS in the hospital, and the second surgery was followed by an SDD. To qualify for SDD at our institution, patients needed to be ≤74 years old, have a body mass index (BMI) ≤33, have ≤2 stable chronic conditions, be a non-smoker, and have a caregiver available to stay with the patient for the first 3 postoperative days. The SDD surgeries were performed between October 2019 and August 2021 by 1 of 8 surgeons. The same surgeon performed both the SDD and the ONS surgery in every case. Each of these patients was offered a 32-question survey on their perceptions of each experience and their overall preferences. The survey was administered through an email link, and responses were recorded through a web-based program (Redcap) (Supplemental Table 1).
Statistical Analysis
Statistical analysis was performed using SPSS Statistics software (v.23, IBM). Patient preference frequencies regarding ONS versus SDD were calculated. Within the groups preferring SDD or ONS, frequencies of survey responses for why they chose that preference were also calculated and ranked. Chi-square analysis was performed to compare surgery (TKA, THA) frequencies between those who preferred SDD and those who preferred ONS. Chi-square analysis was also used to compare the frequencies within the SDD or ONS preference groups regarding being discharged to early (yes/no), postoperative emergency room visit within 30 days (yes/no), and hospital readmission within 30 days (yes/no). In instances where there were fewer than 5 observations per response, results were confirmed using a Fisher’s exact test. A Mann-Whitney test for nonparametric data was used to determine if differences between the SDD and ONS preference groups were present regarding their ratings of pain control, sleep quality, appetite, comfort, safety, family burden, return to function, and their overall experience. Type-I error was set at α = 0.05 for all analyses. For all comparisons, effect size (ES) was calculated using either Phi (frequency-based comparisons) or Cohen’s d (rating-based comparisons) static, whereby ESs were interpreted as follows: 0–0.1 (N, negligible); 0.1–0.3 (S, small); 0.3–0.5 (M, moderate); 0.5–0.7 (L, large); >0.7 (VL, very large) [3,15,16].
Results
Fifty-two of the 67 patients responded to the survey (men = 28, women = 24, median age = 65 ± 2 years), for a response rate of 78%. Eighteen patients had two THAs, and 34 patients had two TKAs. As each patient’s SDD procedure was performed second, the length of time between the surgery and when patients completed the survey was longer for ONS (1629 ± 329 days) than for SDD (455 ± 41 days) (P < .001, ES = 2.50VL).
Overall, a greater proportion of patients (63%) preferred their SDD compared to 25% of patients preferring ONS (P < .001, ES = 0.48M) and 12% who had no preference (P < .001, ES = 0.67L) (Fig. 1a). There was no significant difference in preference for SDD or ONS between the TKA group and the THA group (Fig. 1b).
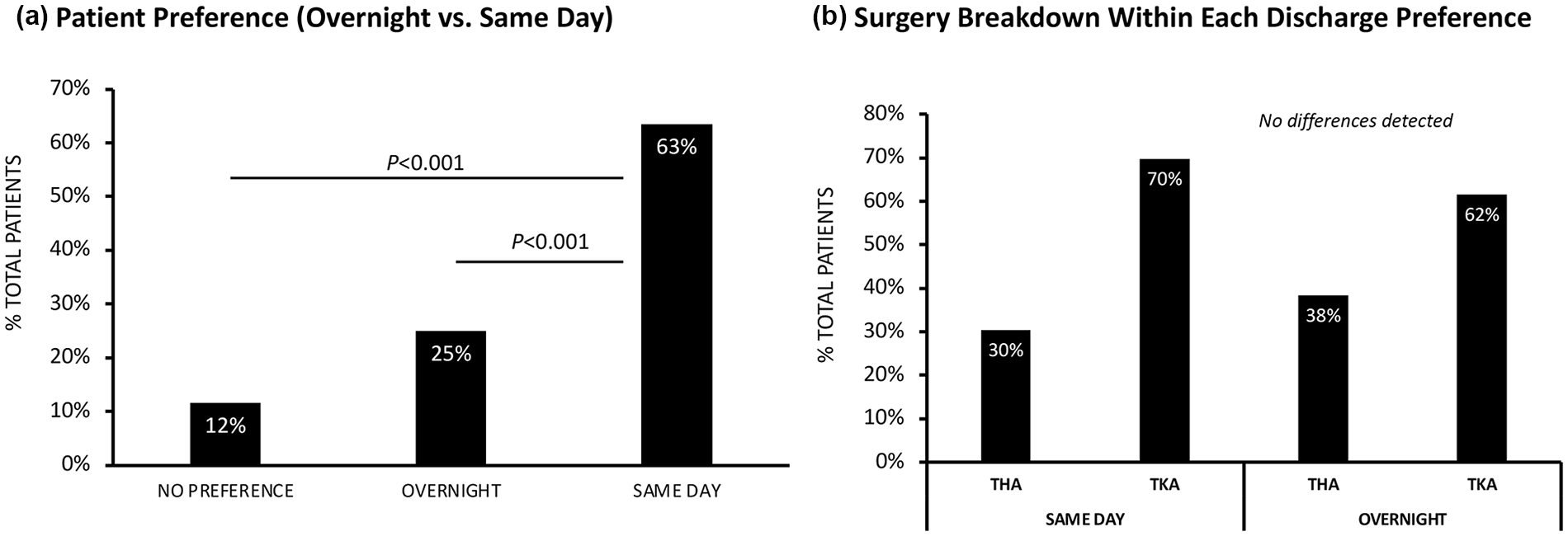
Patient preference of overnight stay vs same-day discharge. Data are presented as (a) frequency of the total patient population preferring same-day discharge, preferring overnight stay, or with no preference; and (b) frequency of surgery type within each discharge preference. TKA total knee arthroplasty, THA total hip arthroplasty.
Response frequencies for reasoning behind preference selection of either ONS or SDD are shown in rank order in Fig. 2. Of those who preferred ONS, better pain management (54%) and having concerns more readily addressed in the hospital (54%) were the top selections (Fig. 2a). Of those who preferred SDD, being “more comfortable at home” was the top response for contributing to their preference with “able to sleep better” and “limited exposure to illness, ie, COVID-19” tied as the next highest-ranking factors for SDD preference (52%) (Fig. 2b).
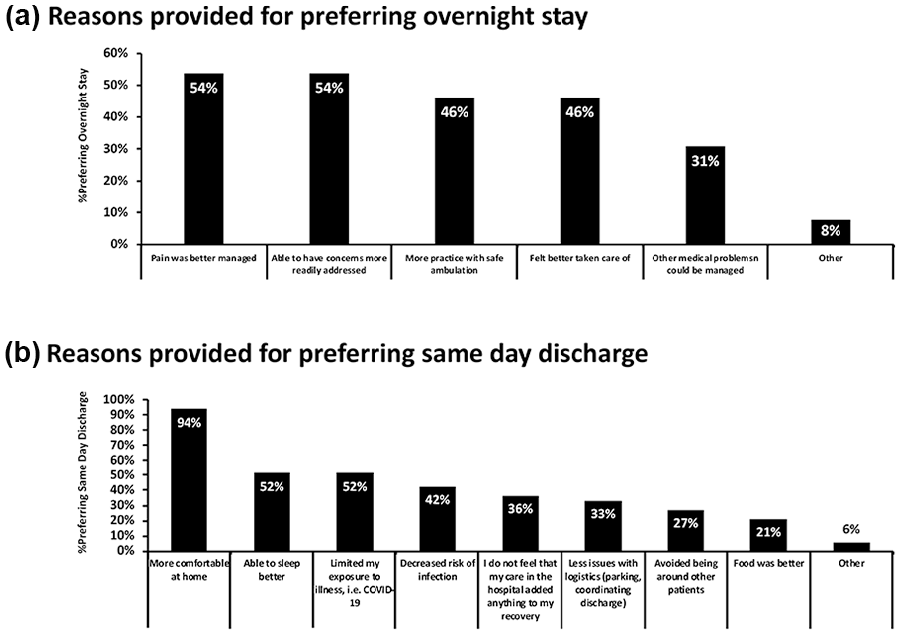
Rational for patient discharge preference. Data are presented as frequencies for (a) reasons provided for those who preferred overnight stay; and (b) reasons provided for those who preferred same-day discharge.
A summary of patient ratings for each category for their SDD and ONSs can be found in Table 1. There were no differences in patient-reported comfort levels, sleep quality, appetite, burden on family, return to function, feelings of being discharged too soon, overall experience, ED visits, or readmissions between patients’ SDD and ONSs reported with the survey. There was a statistically significant difference between patient perception of safety between SDD versus ONS (SDD: 4.29 ± 0.25—ONS: 4.60 ± 0.16; P = .031, ES = 0.74VL).
Experience ratings during overnight stay compared to same-day discharge.
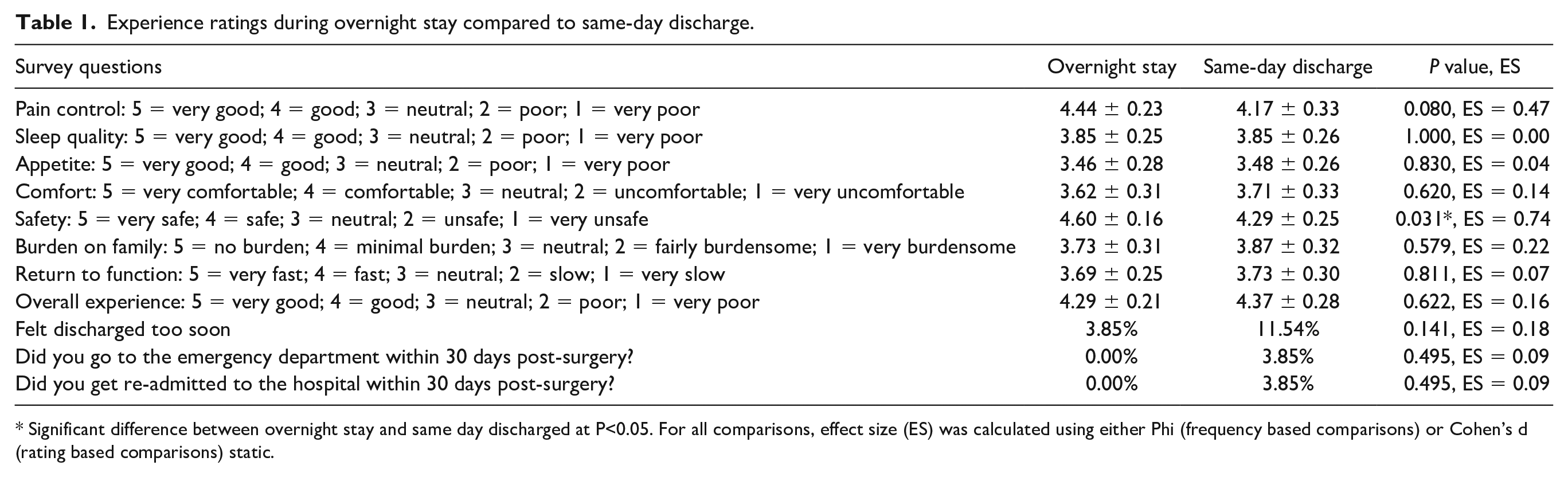
Significant difference between overnight stay and same day discharged at P<0.05. For all comparisons, effect size (ES) was calculated using either Phi (frequency based comparisons) or Cohen’s d (rating based comparisons) static.
Discussion
With this survey, we sought to determine preferences for SDD or ONS in a population of patients who had undergone TKA or THA in both settings. Interestingly, we observed that, in line with our hypothesis, most patients preferred SDD after having experienced ONS and that the rationale was related to home comfort and limited exposure to illness. The results of this survey suggest that, similar to surgeons, patients prefer SDD over ONS.
This retrospective study is not without limitations. First, by surveying patients who had undergone both ONS and SDD after THA or TKA, we received well-informed opinions of patients who can make a direct comparison between their experiences, but there also may have been a recall bias in our sample given the time delay between the surgery and the survey. However, these patients also had the benefit of experiencing an ONS before their SDD and thus had a sense of what to expect (rather than being randomized as in a prospective clinical trial). Second, there are no established minimum clinically important differences to assess for survey responses. Third, there is a selection bias in this study, as the patients in the study were all from a selected population that was safe for SDD, which might represent different opinions from the general patient population in the TJA clinics. In addition, the sample size for this survey was determined by the number of patients in our records who had experienced both ONS and SDD and were willing to complete the survey (convenience/availability sample). In addition, as the survey questions were novel, we were unable to have a reference for the normal population variance or minimum clinically important differences to detect, both critical for formal power analysis. This limitation also prevented us from being adequately powered for any subsequent multivariate analysis. However, the data provided here may be utilized for future power analyses based on the survey developed. In addition, the ES calculations provided may provide information on the expected magnitude of difference between the SDD and ONS conditions.
Same-day discharge after TJA is on the rise in the United States for numerous reasons, and proper selection of patients and improvements in perioperative multidisciplinary care coordination have allowed for this transition. More recently, the rise has further been aided by the COVID-19 pandemic. Many studies have reported that SDD is safe in properly selected patients, with a complication rate that is similar to that of ONS [2,4,5,8,9,14,17].
While SDD safety has often been assessed from a surgeon’s perspective, in terms of complication and readmission rates, safe discharge requires patients to perceive safety and preparedness [7,18]. Our survey sought to determine patient perceptions of SDD relative to ONS after TJA and is the first to assess perceptions in patients who have experienced both ONS and SDD after TJA. This is the only population who can make a direct comparison between experiences, and by studying these patients specifically, we believe the most well-informed preferences are being collected.
Few studies have reported on patient perceptions of an SDD experience. Meneghini and Ziemba-Davis [12] surveyed 110 consecutive patients undergoing inpatient TJA and found that only 54% thought SDD after TJA was an option. Despite that, 62.6% of their patients thought that home was the best place to recover, and only 34.4% would feel uncomfortable with SDD. These results are similar to our survey data, in which 63% of patients said they preferred their SDD, and 25% preferred their ONS experience.
Adelani and Barrack [1] asked patients undergoing inpatient primary TKA in 2017 if they thought SDD arthroplasty would be possible. The most cited concerns regarding SDD were pain control, ability to get to the bathroom, and having a fall. We also found that the respondents who preferred their ONS had similar concerns regarding pain control, being able to have concerns addressed, and safety.
In our survey, 63% of patients preferred SDD, and another 12% had no preference. There was also a small but statistically significant difference between patient perception of safety regarding SDD versus ONS on a 5-point scale, where 5 was “very safe” (4.29 ± 0.25 vs 4.60 ± 0.16, P = .031). Despite these concerns, there were no statistically significant differences in patient ratings of pain control, return to function, or feelings of being discharged too soon. There was also no difference in number of postoperative visits to the ED or readmission between experiences.
Patient education will continue to be the biggest factor in improving patient satisfaction after SDD. Future studies will look at ways to improve patients’ perception of safety, pain control, and the availability of staff to address their concerns.
In conclusion, the responses to our survey suggest that a majority of patients who experienced both SDD and ONS after TJA preferred SDD over ONS, with the strongest factors related to home comfort, sleep, and reduced exposure to contracting an illness. Although we found a small difference in patient perception of safety (~7%), there were no differences in return to the ED or readmissions after SDD and ONS. As SDD continues to be a topic of interest in TJA, these findings provide insight into patients’ preferences and outcomes. Further study is needed.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231218249 – Supplemental material for Patient Perceptions of Same-Day Discharge Versus Overnight Stay After Total Joint Arthroplasty: Results of a Survey
Supplemental material, sj-docx-1-hss-10.1177_15563316231218249 for Patient Perceptions of Same-Day Discharge Versus Overnight Stay After Total Joint Arthroplasty: Results of a Survey by Daniel F. O’Brien, Thomas C. Sullivan, Bradley S. Lambert, Timothy S. Brown, Stephen J. Incavo and Kwan J. Park in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316231218249 – Supplemental material for Patient Perceptions of Same-Day Discharge Versus Overnight Stay After Total Joint Arthroplasty: Results of a Survey
Supplemental material, sj-docx-2-hss-10.1177_15563316231218249 for Patient Perceptions of Same-Day Discharge Versus Overnight Stay After Total Joint Arthroplasty: Results of a Survey by Daniel F. O’Brien, Thomas C. Sullivan, Bradley S. Lambert, Timothy S. Brown, Stephen J. Incavo and Kwan J. Park in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316231218249 – Supplemental material for Patient Perceptions of Same-Day Discharge Versus Overnight Stay After Total Joint Arthroplasty: Results of a Survey
Supplemental material, sj-docx-3-hss-10.1177_15563316231218249 for Patient Perceptions of Same-Day Discharge Versus Overnight Stay After Total Joint Arthroplasty: Results of a Survey by Daniel F. O’Brien, Thomas C. Sullivan, Bradley S. Lambert, Timothy S. Brown, Stephen J. Incavo and Kwan J. Park in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316231218249 – Supplemental material for Patient Perceptions of Same-Day Discharge Versus Overnight Stay After Total Joint Arthroplasty: Results of a Survey
Supplemental material, sj-docx-4-hss-10.1177_15563316231218249 for Patient Perceptions of Same-Day Discharge Versus Overnight Stay After Total Joint Arthroplasty: Results of a Survey by Daniel F. O’Brien, Thomas C. Sullivan, Bradley S. Lambert, Timothy S. Brown, Stephen J. Incavo and Kwan J. Park in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316231218249 – Supplemental material for Patient Perceptions of Same-Day Discharge Versus Overnight Stay After Total Joint Arthroplasty: Results of a Survey
Supplemental material, sj-docx-5-hss-10.1177_15563316231218249 for Patient Perceptions of Same-Day Discharge Versus Overnight Stay After Total Joint Arthroplasty: Results of a Survey by Daniel F. O’Brien, Thomas C. Sullivan, Bradley S. Lambert, Timothy S. Brown, Stephen J. Incavo and Kwan J. Park in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316231218249 – Supplemental material for Patient Perceptions of Same-Day Discharge Versus Overnight Stay After Total Joint Arthroplasty: Results of a Survey
Supplemental material, sj-docx-6-hss-10.1177_15563316231218249 for Patient Perceptions of Same-Day Discharge Versus Overnight Stay After Total Joint Arthroplasty: Results of a Survey by Daniel F. O’Brien, Thomas C. Sullivan, Bradley S. Lambert, Timothy S. Brown, Stephen J. Incavo and Kwan J. Park in HSS Journal®
Supplemental Material
sj-docx-7-hss-10.1177_15563316231218249 – Supplemental material for Patient Perceptions of Same-Day Discharge Versus Overnight Stay After Total Joint Arthroplasty: Results of a Survey
Supplemental material, sj-docx-7-hss-10.1177_15563316231218249 for Patient Perceptions of Same-Day Discharge Versus Overnight Stay After Total Joint Arthroplasty: Results of a Survey by Daniel F. O’Brien, Thomas C. Sullivan, Bradley S. Lambert, Timothy S. Brown, Stephen J. Incavo and Kwan J. Park in HSS Journal®
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Bradley S. Lambert, PhD, reports relationships with Major League Baseball and Delfi Medical Innovations, Inc. Timothy S. Brown, MD, reports relationships with AO Foundation and Stryker. Stephen J. Incavo, MD, reports relationships with Kyocera Medical Corporation, MicroPort Orthopedics Inc., and Engage Surgical. Kwan J. Park, MD, reports relationships with Zimmer Biomet. The other authors report no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived from all patients included in this study.
Level of Evidence
Level IV: Survey
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.