
Abstract
Background:
While many studies have examined the impact of comorbidities on the success of same calendar day discharge (SCDD) in total joint arthroplasty (TJA), literature surrounding the impact of social determinants is lacking.
Purpose:
We sought to investigate the relationship between various social determinants and success of SCDD after primary total hip arthroplasty (THA) and total knee arthroplasty (TKA).
Methods:
We conducted a retrospective review of 1160 THA and 1813 TKA performed at a single academic institution between November 2020 and August 2022. Social factors including substance use, occupation, marital status, income, and participation in physical exercise were included. In addition, aspects of discharge planning were reviewed such as living situation and transportation details.
Results:
Overall, 952 (32%) patients had successful SCDD, whereas 2021 (68%) patients were discharged on postoperative day 1 (POD1) or greater. Successful SCDD patients were more likely to have health care (4.8% vs 2.5%) and active (5.4% vs 4.6%) rather than sedentary occupations, be married (79.6% vs 67.4%), have access to transportation (95.6% vs 92.9%), live in a higher median income area ($64,044 [16,183] vs $61,572 [14,594]), and exercise weekly (62.6% vs 23.9%). Interestingly, the successful patients had more stories in their homes (1.62 [0.56] vs 1.43 [0.53]), more stairs to enter their homes (5.19 [5.22] vs 4.60 [5.24]), lived farther from the hospital (43.3 [138.0] vs 32.0 [75.9] miles), and a higher prevalence of alcohol use (60.7% vs 44.7%) and tobacco use (19.3% vs 17.3%).
Conclusion:
These findings may help arthroplasty surgeons to better understand the social factors that contribute to successful SCDD in TJA patients, ultimately aiding in patient selection and preoperative counseling.
Introduction
Total knee arthroplasty (TKA) and total hip arthroplasty (THA) are among the most frequently performed orthopedic surgical procedures, and they consistently provide a significant improvement in patient quality of life [6,14]. As health care systems continue to aspire to increased efficiency and cost-effectiveness, there has been a growing interest in pursuing same calendar day discharge (SCDD) following total joint arthroplasty (TJA) [2,11]. Although the benefits of SCDD have been well documented (including reduced length of stay, lower costs, and comparable patient outcomes [3,16]), the identification of patient risk factors, which influence the success and failure of SCDD, remains essential for optimizing patient selection and minimizing complications [7,16].
Preoperative health optimization is crucial to ensuring positive surgical outcomes after TJA [4,13]. Several studies have examined the effect of comorbidities and specific demographics, such as age and body mass index (BMI), on SCDD [9,10]. Recognizing the importance of health optimization, the focus of this study shifts toward the impact of social determinants of health (SDOH) on successful TJA outcomes. Social determinants of health that have been found to be influential include socioeconomic status, occupation, and home support [1,5]. However, a comprehensive analysis of SDOH and their influence on SCDD TJA is lacking.
The primary aim of this study was to investigate the relationship between various SDOH and the success of SCDD after primary THA and TKA. We hypothesized that specific SDOH would be significantly correlated with the success of SCDD, thereby providing valuable insight into patient selection and the development of targeted interventions to improve TJA in the ambulatory surgical center.
Methods
Following institutional review board approval, we conducted a retrospective review of 2973 patients who underwent primary TKA or THA at a single academic institution between November 2020 and August 2022. All surgeries were performed by 3 adult-reconstruction fellowship-trained orthopedic surgeons. In addition, all patients had consistent preoperative and postoperative protocols based on the institution’s guidelines. The groups were subdivided into 2 cohorts based on the day of discharge: SCDD (N = 952) and discharge on post-op day 1 (POD1) or later (N = 2021). Patients were included if they were 18 years or older and had complete medical records containing relevant SDOH data. Patients were excluded if they had a revision surgery or if their charts had incomplete SDOH data.
The data collected included patient demographics (age, sex, race, ethnicity), BMI, surgery type (TKA or THA), emergency room or hospital admission in the year prior to surgery, and comorbidities described using American Society of Anesthesiologists (ASA) score and the Charlson Comorbidity Index (CCI).
We separated SDOH data points into 3 categories: social history, living situation and home descriptors, and baseline functional status. Social history included alcohol use, tobacco use, substance use, employment, exercise, and average income. The average income by zip code was collected using the 2010–2014 American Community Survey data [20]. As the US census typically collects information at the state level, the American Community Survey data set allows for a more granular data collection; therefore, it was better for zip code analysis [8]. The timeframe 2010–2014 was used to ensure a complete data set due to the multiyear nature of the American Community Survey. Living situations included marital status, cohabitation, access to transportation, and need for medication assistance. Home descriptors included the number of stories total in the house, the number of stairs to enter the house, first-floor bathrooms, and first-floor bedrooms. Home residence distances from each surgery site were calculated using Google Maps navigation systems and recorded in miles. Baseline functional status consisted of whether individuals exercised at any level, needed ambulatory aids, or had a history of falls within the year prior to surgery.
Statistical Analysis
All statistical analyses were performed using R Studio Software (Version 3.5.1). Continuous variables were analyzed using Student’s t tests or analysis of variance. Categorical data was analyzed using χ2 tests. Statistical significance was defined as P < .05.
Results
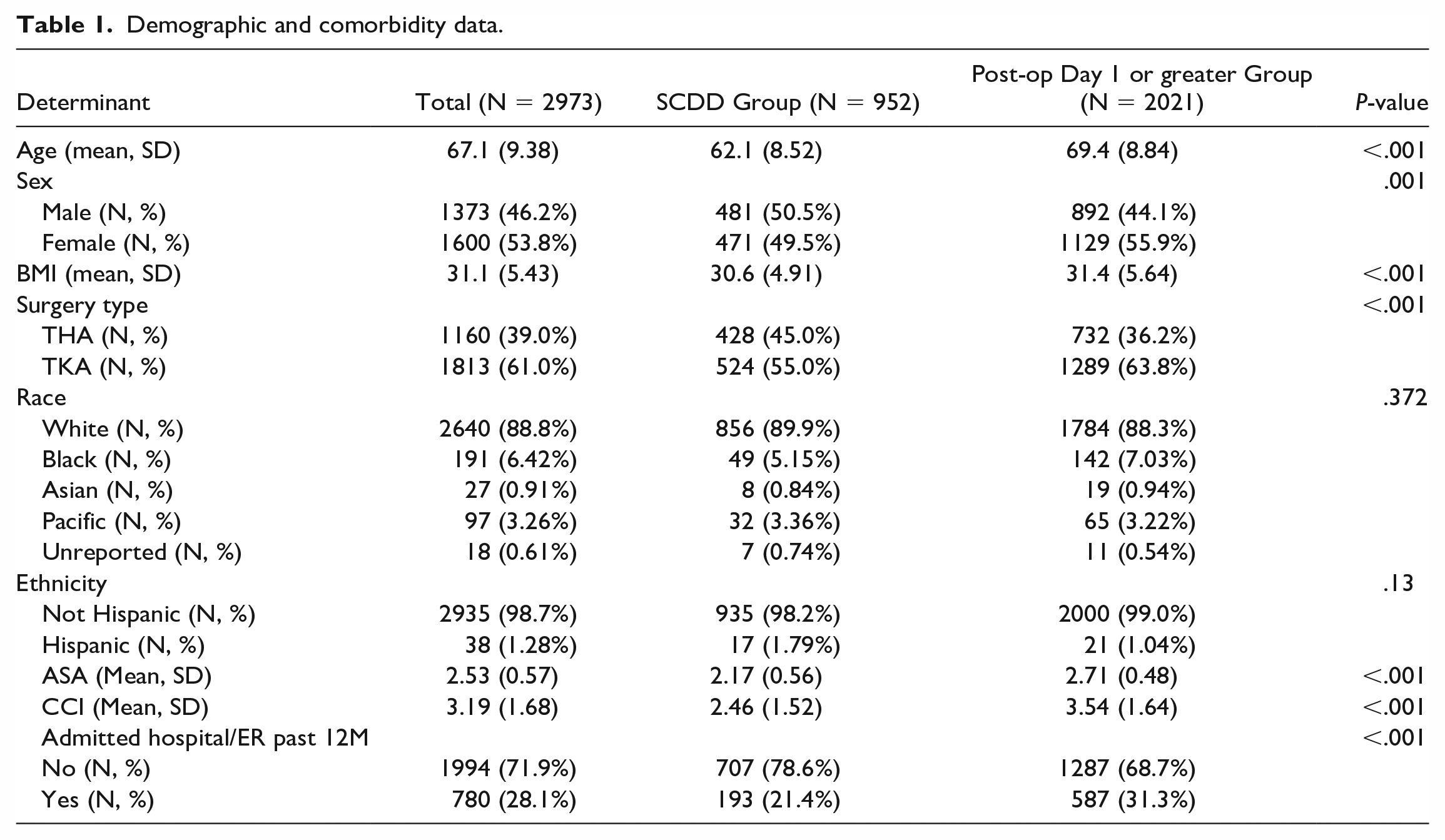
The SCDD group had a younger mean age (62.1 vs 69.4 years, P < .001), a higher proportion of men (50.5% vs 44.1%, P = .001), and a lower mean BMI (30.6 vs 31.4, P < .001) compared with the POD1 or greater group. There was no significant difference between the 2 groups in terms of race (P = .372) and ethnicity (P = .13). The SCDD group had a higher proportion of THA (45.0% vs 36.2%, P < .001) but a lower proportion of TKA (55.0% vs 63.8%, P < .001). The SCDD group had a lower mean CCI (2.46 vs 3.54, P < .001) and mean ASA score (2.17 vs 2.71, P < .001). The SCDD group had a lower rate of hospital or emergency room admission in the 12 months prior to surgery (78.6% vs 68.7% with no admissions, P < .001) (Table 1).
Demographic and comorbidity data.
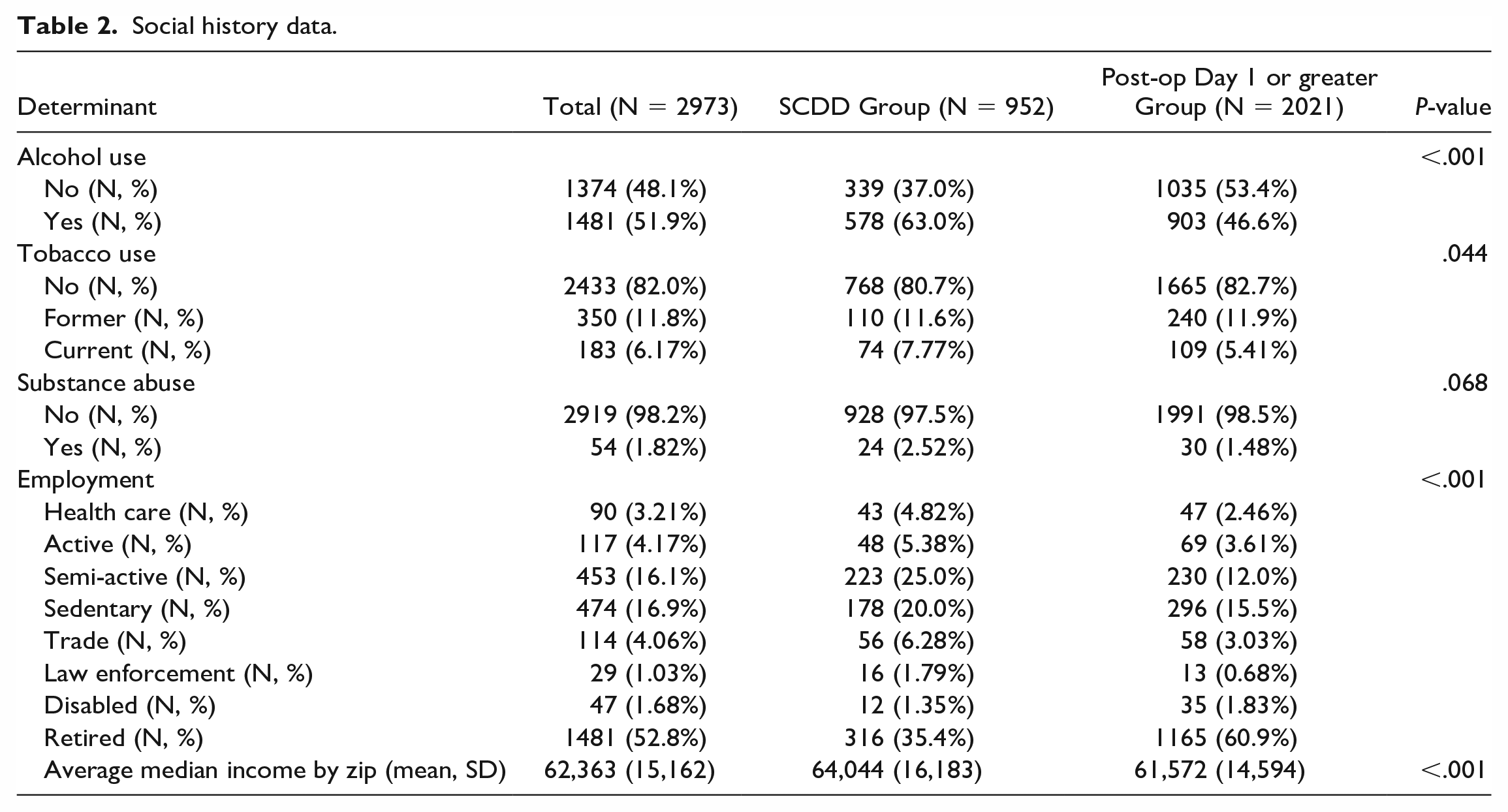
Regarding social history, the SCDD group showed a higher rate of alcohol use compared with the POD1 or greater group (63.0% vs 46.6%, P < .001). Tobacco use was slightly higher in the SCDD group, particularly among current users (7.77% vs 5.41%, P = .044). While substance use was not significantly different between groups (P = .068), it was slightly higher in the SCDD group (2.52% vs 1.48%). Regarding employment, the SCDD group had a higher proportion employed in health care (4.82% vs 2.46%, P < .001), and they were more likely to have active jobs (5.38% vs 3.61%, P < .001), semi-active jobs (25.0% vs 12.0%, P < .001), or trade jobs (6.28% vs 3.03%, P < .001). In contrast, a lower number of the SCDD group was retired compared with the POD1 or greater group (35.4% vs 60.9%, P < .001). The average median income by zip code was higher in the SCDD group ($64,044 vs $61,572, P < .001) (Table 2).
Social history data.
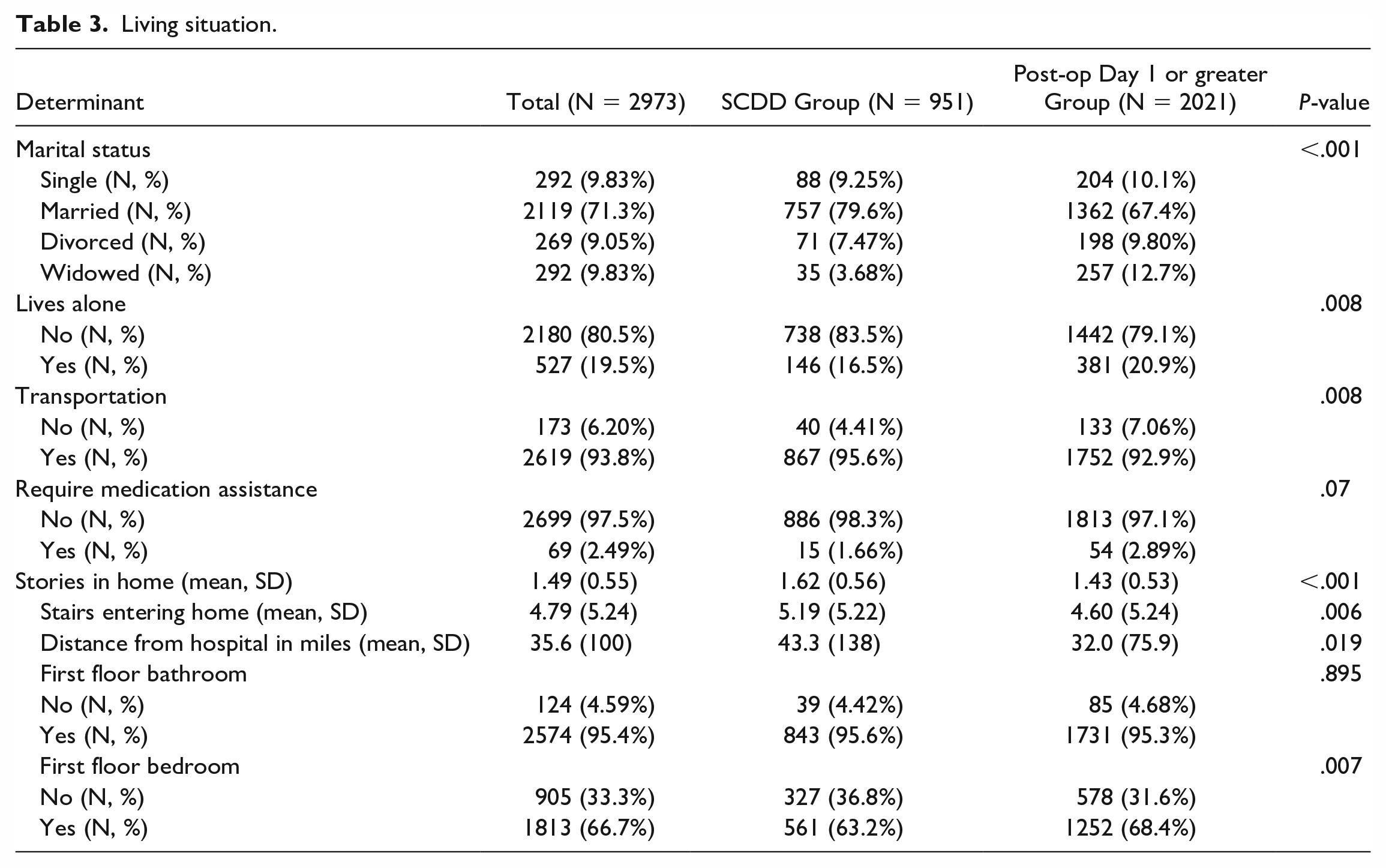
Living situation data revealed the SCDD group had more married individuals (79.6% vs 67.4%, P < .001) and fewer widowed individuals (3.68% vs 12.7%, P < .001). Fewer individuals in the SCDD group resided alone in comparison to the POD1 or greater group (16.5% vs 20.9%, P = .008). The SCDD group had a higher rate of transportation access (95.6% vs 92.9%, P = .008) and a lower rate of needing medication assistance compared with the POD1 or greater group (1.66% vs 2.89%, P = .07). The SCDD group lived in homes with a higher average number of stories (1.62 vs 1.43, P < .001) and more stairs entering the home (5.19 vs 4.60, P = .006). The SCDD group also lived a greater average distance from the hospital (43.3 vs 32.0 miles, P = .019). While there was no significant difference in having a first-floor bathroom (P = .895), fewer individuals in the SCDD group had a first-floor bedroom compared with the postoperative day one or greater group (63.2% vs 68.4%, P = .007) (Table 3).
Living situation.
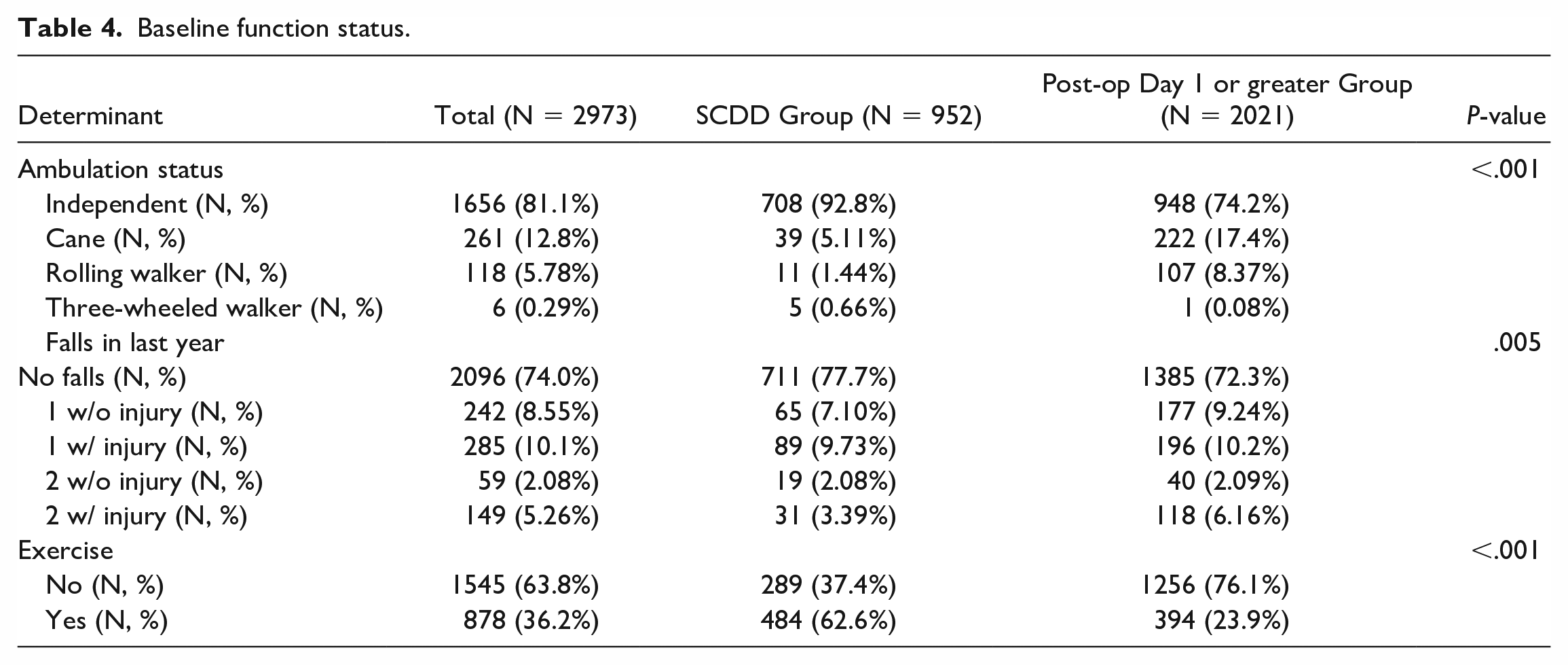
The SCDD group showed a higher rate of independent ambulation (92.8% vs 74.2%, P < .001) and a lower rate of ambulation assistance with canes (5.11% vs 17.4%, P < .001) or rolling walkers (1.44% vs 8.37%, P < .001). The SCDD group had experienced fewer falls in the year prior to surgery (77.7% vs 72.3% with no falls, P = .005). Furthermore, exercise in any form was more common in the SCDD group (62.6% vs 23.9%, P < .001) (Table 4).
Baseline function status.
Discussion
To the best of our knowledge, this study is the first comprehensive investigation into the social determinants that correlate with successful SCDD after primary THA and TKA. While prior studies have reported on the impact of basic demographics and comorbidities on successful SCDD, they did not fully address social factors [9,15,16]. Our findings suggest that social factors that may affect SCDD success for THA and TKA patients include occupation, marital status, transportation access, regional median income, and engagement in physical activity. Surprisingly, alcohol use and tobacco use were associated with successful SCDD.
This study has several limitations that warrant consideration. The retrospective design may introduce biases, which could be addressed in future research by adopting a prospective design with larger cohorts. In addition, this research was conducted at a single institution, potentially limiting generalizability. However, our cohort of almost 3000 patients had a diverse range of social determinants. Future multicenter studies may help validate our findings in different settings and populations while also exploring additional SDOH and their associations with successful SCDD. Moreover, this study focused on SCDD success as the primary outcome, which does not fully capture TJA recovery complexity. Despite these limitations, our findings may help orthopedic surgeons in understanding the social factors that contribute to successful SCDD in TJA patients, ultimately aiding in patient selection and preoperative counseling.
As anticipated, patients with successful SCDD were more likely to be younger, married, wealthier, and more physically active. These characteristics are associated with better overall health, which may contribute to a smoother and more rapid postoperative recovery. Moreover, being married and having a higher income could indicate a stronger social support system, providing the necessary assistance during the recovery process. Similar findings have also been found in other areas of medicine. Previous research by Shen et al [17] analyzed 244 patients with chronic rhinosinusitis and found worse baseline symptom severity in patients with lower average income and those who were not married. In addition, regular physical exercise prior to surgery can also improve muscle strength and joint function, which may facilitate a quicker return to normal activities following TJA. This conclusion is supported by Hoogeboom et al [12], who found evidence for improved outcomes in patients who exercised prior to and soon after surgery. Therefore, it is not surprising that patients with these characteristics had a higher likelihood of successful SCDD.
This study also found that successful SCDD patients had more stories in their homes, more stairs to enter their homes, and lived farther from the hospital. One might have expected that these factors would be associated with a lower likelihood of successful SCDD due to patient concerns with possible increased physical demand during their recovery once they return home. However, it is possible that these factors could be indicative of a higher socioeconomic status in SCDD patients. Higher socioeconomic status, as suggested by Adler and Newman [1], is often linked to better health outcomes due to increased access to health care, preventive care, and healthier lifestyles resulting in improved outcomes.
Surprisingly, our analysis suggested that successful SCDD patients were more likely to have a history of alcohol consumption and tobacco use. Although we found a positive association with successful SCDD, alcohol and tobacco use are typically considered risk factors for poorer health outcomes [18,19]. We speculate that healthier patients may consume more alcohol than less healthy patients, who may restrict alcohol intake for health concerns, but further study is needed on the underlying factors affecting the association of alcohol and tobacco use with successful SCDD in the context of TJA. Our results suggest that certain factors, which may seem counterintuitive at first, may still contribute to the success of SCDD in TJA patients.
In conclusion, this study highlights the impact of social determinants on the success of SCDD following primary THA and TKA surgery. We found that patients who are younger, married, wealthier, and more physically active tend to have more successful SCDD outcomes. In addition, factors such as living in larger homes with more stories and stairs, as well as residing further from the hospital, were positively correlated with successful SCDD. These results emphasize the importance of considering social determinants when preparing patients for potential SCDD following primary THA and TKA. By recognizing these factors, orthopedic surgeons can potentially improve the success rate of SCDD through appropriate patient selection and thorough preoperative counseling.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231204231 – Supplemental material for Social Risk Determinants for Successful Same Calendar Day Discharge in Total Joint Arthroplasty
Supplemental material, sj-docx-1-hss-10.1177_15563316231204231 for Social Risk Determinants for Successful Same Calendar Day Discharge in Total Joint Arthroplasty by Rex W. Lutz, Danielle Y. Ponzio, Hope S. Thalody, Harrison A. Patrizio, Miranda M. Czymek, Michael Ast, Zachary D. Post and Alvin C. Ong in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316231204231 – Supplemental material for Social Risk Determinants for Successful Same Calendar Day Discharge in Total Joint Arthroplasty
Supplemental material, sj-docx-2-hss-10.1177_15563316231204231 for Social Risk Determinants for Successful Same Calendar Day Discharge in Total Joint Arthroplasty by Rex W. Lutz, Danielle Y. Ponzio, Hope S. Thalody, Harrison A. Patrizio, Miranda M. Czymek, Michael Ast, Zachary D. Post and Alvin C. Ong in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316231204231 – Supplemental material for Social Risk Determinants for Successful Same Calendar Day Discharge in Total Joint Arthroplasty
Supplemental material, sj-docx-3-hss-10.1177_15563316231204231 for Social Risk Determinants for Successful Same Calendar Day Discharge in Total Joint Arthroplasty by Rex W. Lutz, Danielle Y. Ponzio, Hope S. Thalody, Harrison A. Patrizio, Miranda M. Czymek, Michael Ast, Zachary D. Post and Alvin C. Ong in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316231204231 – Supplemental material for Social Risk Determinants for Successful Same Calendar Day Discharge in Total Joint Arthroplasty
Supplemental material, sj-docx-4-hss-10.1177_15563316231204231 for Social Risk Determinants for Successful Same Calendar Day Discharge in Total Joint Arthroplasty by Rex W. Lutz, Danielle Y. Ponzio, Hope S. Thalody, Harrison A. Patrizio, Miranda M. Czymek, Michael Ast, Zachary D. Post and Alvin C. Ong in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316231204231 – Supplemental material for Social Risk Determinants for Successful Same Calendar Day Discharge in Total Joint Arthroplasty
Supplemental material, sj-docx-5-hss-10.1177_15563316231204231 for Social Risk Determinants for Successful Same Calendar Day Discharge in Total Joint Arthroplasty by Rex W. Lutz, Danielle Y. Ponzio, Hope S. Thalody, Harrison A. Patrizio, Miranda M. Czymek, Michael Ast, Zachary D. Post and Alvin C. Ong in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316231204231 – Supplemental material for Social Risk Determinants for Successful Same Calendar Day Discharge in Total Joint Arthroplasty
Supplemental material, sj-docx-6-hss-10.1177_15563316231204231 for Social Risk Determinants for Successful Same Calendar Day Discharge in Total Joint Arthroplasty by Rex W. Lutz, Danielle Y. Ponzio, Hope S. Thalody, Harrison A. Patrizio, Miranda M. Czymek, Michael Ast, Zachary D. Post and Alvin C. Ong in HSS Journal®
Supplemental Material
sj-docx-7-hss-10.1177_15563316231204231 – Supplemental material for Social Risk Determinants for Successful Same Calendar Day Discharge in Total Joint Arthroplasty
Supplemental material, sj-docx-7-hss-10.1177_15563316231204231 for Social Risk Determinants for Successful Same Calendar Day Discharge in Total Joint Arthroplasty by Rex W. Lutz, Danielle Y. Ponzio, Hope S. Thalody, Harrison A. Patrizio, Miranda M. Czymek, Michael Ast, Zachary D. Post and Alvin C. Ong in HSS Journal®
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Danielle Ponzio, MD, declares a relationship with Depuy. Michael Ast, MD, declares relationships with BD, Bioventus, Conformis, Convatec, ConveyMed, HS2, Orthoalign, Ospitek, Osso VR, Parvizi Surgical Innovations, Smith & Nephew, Stryker, and Surgical Care Affiliates. Zachary Post, MD, declares relationships with Orthodevelopment and Depuy. Alvin Ong, MD, declares relationships with Smith & Nephew and Stryker. The other authors declare no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived for all patients included in this study.
Level of Evidence
Level IV: prognostic study
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.