
Abstract

Keywords
Introduction
Postoperative nausea (PON) occurs in 30% of surgical patients and may result in medical complications, increased length of stay, and decreased patient satisfaction [7]. Antiemetic medications require time to coordinate, administer, and take effect, and they may have adverse effects. If a patient does not respond to a first-line antiemetic, additional time is required to order and administer a second-line drug. Aromatherapy affords a complementary therapy that is easy to provide, with quick onset and few to no adverse effects. Aromatherapy can be self-administered, involving patients in their care, and may reduce exclusive reliance on drug therapy.
Advances in the management of inflammation and bleeding, new surgical and anesthetic techniques, and better pain control have generated faster and more efficient orthopedic surgery [9]. In step with this practice change, orthopedic nurses coordinate a quicker recovery with continuous emphasis on comfort and safe care transitions. Aromatherapy is a complementary therapy that may be used in support of these goals.
Using an implementation-science approach, orthopedic nurses at our institution introduced and evaluated the application of aromatherapy and found an association with increased patient comfort, which resulted in the augmentation of existing protocols to include aromatherapy as a standard inpatient practice. However, parallel cost-containment efforts associated with the COVID-19 pandemic required aromatherapy to be prioritized for spine surgery patients, who were thought to be more at risk for nausea given their exposure to general anesthesia.
More recently, our institution embarked on shifting joint replacement surgery from the inpatient to the ambulatory setting. Nurses observed PON as a barrier to patient throughput and identified aromatherapy as a potential strategy to reduce discharge delays and offer comfort and convenience during transition to home. Prior concerns about cost were no longer an issue; the opportunity to shorten length of stay incentivized an expanded use of aromatherapy in ambulatory surgery. In this article, we describe our institution’s introduction of aromatherapy to orthopedic inpatient practice and its expansion to the short-stay arthroplasty setting.
Aromatherapy for Postoperative Nausea: From Knowledge to Action
The Knowledge to Action (KTA) model provided a framework for our science-implementation project [12]; the model describes knowledge transfer as the interaction between knowledge creation and user implementation of created information. Knowledge creation informs practice change, and operationalization is achieved through a stepwise action cycle informed by continuous feedback (Supplemental Figure 1).
Knowledge creation involves inquiry, synthesis, and data collection to shape an implementation plan. In 2019, several nurses at our organization returned from a Magnet conference, where they learned about aromatherapy as a best practice. They formed a team to acquire more knowledge about this intervention and searched PubMed using MeSH terms: “Aromatherapy” [Mesh] OR aromatherapy OR aromatherapies AND “Postoperative Nausea and Vomiting” [Mesh] OR “postoperative nausea and vomiting “postoperative AND nausea AND vomiting” OR “postoperative nausea and vomiting” OR “postoperative AND nausea” OR “postoperative nausea.” Among the 31 studies retrieved was a systematic review [1] that cited a randomized trial (N = 339) [6] wherein researchers found a decrease in PON in the aromatherapy group. Investigators used a product called QueaseEASE that contains a blend of peppermint, lavender, ginger, and spearmint extracts and once opened, releases a scent that remains active for up to 72 hours. The nurse project team contacted the product vendor to find out more about cost, indications, and contraindications. Manufacturers of QueaseEASE also connected the nurse team with other Magnet-designated hospitals that use this product to provide postoperative comfort. The project nurses then presented a proposal for QueaseEASE use to our hospital pharmacy and therapeutics (P&T) committee, an interdisciplinary policymaking forum with expertise in both medicinal and complementary interventions. The committee endorsed the aromatherapy pilot and requested the project team return with results to inform future practice and financing.
As part of the knowledge-creation phase, project nurses developed a data collection tool that contained patient demographics, type of surgery and anesthesia, number of postoperative days, and patient satisfaction. The numeric rating scale (NRS) was used to measure nausea intensity. Widely used to measure pain, the NRS can be used to measure PON. In a psychometric study (N = 479) using a 4-level NRS and visual analog scale (VAS), researchers correlated (r = .79) nausea scores between instruments [13]. In a second study, researchers evaluated nausea using NRS and VAS before and after rescue antiemetics and found 86% agreement with reported changes in nausea intensity [2]. Nurses and patients in the study reported the 5-point NRS as easy to understand and use. The nurse project team at our organization employed a 5-point scale with nausea levels of 1 = none, 2 = mild (able to tolerate food and medication), 3 = moderate (lack of appetite), 4 = great (nausea ongoing; no appetite), and 5 = severe (nausea with dry heaves). A single, dichotomous patient satisfaction measure was added to the data collection plan. Patients using aromatherapy were asked whether they were likely to use aromatherapy again if they experienced nausea.
The KTA cycle guides knowledge transfer, including adapting knowledge to the local context, monitoring fidelity to procedural changes, and evaluating outcomes. An aromatherapy pilot at our institution began on 3 orthopedic inpatient units between August 19, 2019 and February 19, 2020. Before implementing the pilot, point of care nurses on the 3 units were educated on the use, safety, and benefits of aromatherapy; data collection procedures; and placement, application, and storage of the aromatherapy dispenser. While the pilot was in progress, weekly huddles and onsite in-services reinforced details on the delivery process, optimized data collection, and verified use of aromatherapy.
Patients cared for by direct care nurses involved in the project were included. Patients with an allergy, a sensitivity to scents, or an aversion to aromatherapy ingredients were excluded from participation, as were those with dementia, confusion, epistaxis, sinusitis, and developmental delay. Level of nausea was elicited during routine postoperative assessment. Patients with nausea were offered antiemetic medication or aromatherapy. Nausea intensity ratings were re-evaluated 5 minutes after aromatherapy administration. Nurses asked patients about their satisfaction with aromatherapy and monitored patients for adverse reactions.
Of 105 patients who self-administered aromatherapy during the project trial, the mean age was 58 years and most were female (73%). Predominant orthopedic procedures consisted of spine (44%), hip (20%), and knee (28%) surgeries. Findings noted a higher percentage (53%) of nausea scores in one of the 3 inpatient units, which routinely admits a greater proportion of spine surgery patients. Half of patients received general anesthesia and half received local anesthesia; 98% received opioid pain control during their postoperative course. Requests for aromatherapy were most frequent during the immediate postoperative period and the first postoperative day.
Before receiving aromatherapy, 22% (n = 23) of patients had mild nausea and 79% (n = 82) reported moderate or greater. Postaromatherapy scores showed an association with decreased PON intensity, with χ2 analysis demonstrating an associated significant change (P < .001) between prearomatherapy and postaromatherapy intervention (Table 1). Nine participants (8.5%) showed no change in score and the remaining patients showed improvement (91.5%).
Preoperative vs postoperative change in nausea.

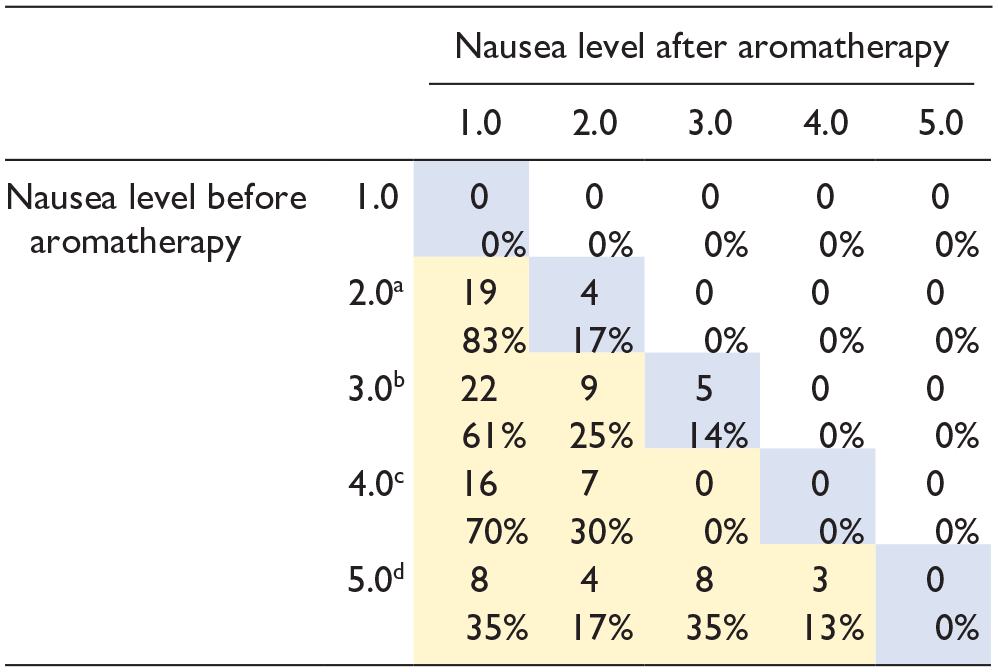
19/23 (83%) of patients who were level 2 prearomatherapy were level 1 postaromatherapy.
31/36 (86%) of patients who were level 3 prearomatherapy were level 2 or 1 postaromatherapy.
23/23 (100%) of patients who were level 4 prearomatherapy were level 3 or lower postaromatherapy.
23/23 (100%) of patients who were level 5 prearomatherapy were level 4 or lower postaromatherapy.
Using McNemar’s test, paired binary outcomes were compared demonstrating significant (P < .001) change in the mild (1-2) nausea scores prearomatherapy and postaromatherapy across the orthopedic units. Level 1-2 response improved from 22% to 85% after aromatherapy (Supplemental Table 2a). Improvement was seen by all individual orthopedic services (Supplemental Table 2b).
We observed no adverse reactions to the aromatherapy; in fact, 98% of patients reported a likelihood to use aromatherapy again, whereas 2% were not satisfied (ie, 1 patient reported a headache and 1 reported worsening nausea that was not attributed to the aromatherapy). All nurses who participated in the pilot were satisfied with the application of the aromatherapy protocol.
Part of the KTA cycle is to sustain knowledge gained through application and evaluation. In early 2021, the project team brought results from the pilot to the P&T committee, which endorsed aromatherapy for clinical practice and suggested Institutional Review Board approval to allow findings to be disseminated. Although providing aromatherapy as a comfort measure is within the Nursing Scope of Practice [10], the interdisciplinary members of the P&T agreed to include aromatherapy in the standard order set to cue nurses to make use of this comfort option and to control inventory. Cost constraints limited application of aromatherapy to the standard order sets of the spine patient population, but providers of other orthopedic services could add an individualized separate order if indicated.
Extending Aromatherapy to Short-Stay Arthroplasty
Successful implementation of aromatherapy in the inpatient population coincided with our organization’s decision to provide arthroplasty surgery in an ambulatory setting, dedicating a patient care unit to include this patient population and an interprofessional Ambulatory Arthroplasty Task Force to ensure excellent care over a shorter patient stay. In the fall of 2022, the task force observed PON as a barrier that delayed patient progress with physical therapy. Previous success in nausea reduction during the earlier aromatherapy trial led to discussion on whether ambulatory arthroplasty patients might benefit from aromatherapy.
In October 2022, nurses from the original aromatherapy transfer project collaborated with members of the task force to expand aromatherapy access to patients undergoing ambulatory joint replacement. Up until this point, prescribers could order aromatherapy for individual arthroplasty patients, but it was not technically part of the standard order set. In November 2022, project nurses worked with informatics professionals to add aromatherapy to standard prescriber orders for ambulatory arthroplasty patients. Informaticists also incorporated documentation fields for aromatherapy indication and administration within the electronic medical record (EMR). During EMR reconfiguration, the implementation team contacted nurse educators to review existing lesson plans and update the few nurses not already trained before the unit was converted to a short-stay status.
Although aromatherapy was technically available for use, disruptions during implementation slowed application of practice. The dedicated unit and personnel relocated within the organization to a similarly organized workspace. During this time, there were also EMR technical disruptions that interfered with ordering aromatherapy. Nurse informaticists made necessary adjustments to better access to standard orders. Nurse educators promoted the use of aromatherapy where indicated, reinforcing clinical advantages during shift-change huddles. These challenges notwithstanding, the use of aromatherapy began to slowly increase.
As previously stated, the expansion of aromatherapy to the ambulatory setting was the second aim of a 2-part implementation initiative. The effectiveness of aromatherapy on PON intensity and duration was established during the first phase of the knowledge transfer. The outcomes of the second phase involving expansion to the ambulatory joint replacement patient, focused on the effects of aromatherapy on patient throughput. The team used the analytics resources of the Ambulatory Arthroplasty Task Force to identify metrics to estimate impact, specifically delays in physical therapy clearance (goals met) due to PON and length of stay.
Among the 3605 patients scheduled for ambulatory arthroplasty surgery between October 1, 2022 and May 5, 2023, 68 patients received aromatherapy. Eight doses were given over the first 4 months, which increased to an average of 18 doses per month as logistical issues associated with informatics and unit relocation were rectified. Among the 68 patients who received aromatherapy, 26 patients experienced nausea as barrier to discharge clearance by physical therapy. The absence discharge delays for the remaining 42 patients are potentially due to earlier administration of aromatherapy. Of the 294 patients experiencing nausea as barrier to physical therapy clearance, 26 patients who received aromatherapy were discharged an average of 3 hours earlier compared to patients who did not receive aromatherapy (Table 2).
Aromatherapy impact on length of stay (LOS).

Discussion
Several studies have investigated the effects of aromatherapy on PON, including 2 Cochrane systematic reviews [5]. The 2012 review [5] analyzed 6 randomized and 3 case-control studies (N = 402). Researchers of the experimental studies compared isopropyl alcohol to antiemetic drug therapy, and the latter was determined to be more effective. In the 2018 review [5], 5 more trials and 2 case-control studies were added, for a total of 16 (N = 1036) studies. Six of the studies in this second systematic review measured PON intensity and did not find aromatherapy to be effective in reducing nausea severity compared with placebo (P = .28). Aromatherapy products varied across studies (ie, alcohol vs essential oils), and the ability to pool data was limited due to heterogeneity of outcomes and varying measurement of time points.
In a third systematic review conducted in 2019, researchers reported a significant decrease (P < .05) in nausea severity in 3 out of 5 randomized studies where ginger or essential oil blends were used [1]. In both the Cochrane [5] and Asay [1] systemic reviews, 11 studies reported significantly (P < .05) less antiemetic medication needed postoperatively. This outcome was not measured during our project. Consistent with our findings, patients ranked aromatherapy positively in 4 studies cited in the systematic reviews. None of the previously mentioned research encountered adverse effects of aromatherapy, which is consistent with our experience.
Our approach to knowledge transfer was supported by shared governance structures within our organization to successfully change practice. Aromatherapy was approved by the Medical Board and is part of the routine postoperative order set for spine surgery patients. It can also be ordered if requested by patients from any orthopedic surgical service. Expansion of aromatherapy to the short-stay arthroplasty patient is in progress.
Prior research in the ambulatory setting is focused on the clinical effect of aromatherapy on the presence of PON, rather than its impact on patient throughput [3,4,8,11]. In a randomized trial (N = 1151) conducted in the ambulatory surgical setting, researchers reported a significant (P < .001) decrease in PON for ginger or blended essential oil groups compared with placebo [8]. Researchers in a separate quality-improvement study (N = 50), conducted in a 23-hour stay setting reported significantly (P = .001) less PON intensity after administration of blended aromatherapy [3]. Several researchers reported the number of antiemetics used by patients receiving aromatherapy varied depending on if medication was provided during the postoperative period vs as a rescue dose after aromatherapy [5,6,11]. Although shortened length of stay was cited as a potential benefit of aromatherapy, it was not listed in primary or secondary outcomes.
Aromatherapy is a recognized complementary intervention to provide comfort to patients experiencing PON. In the first phase of implementation, we found that patients experienced diminished nausea; in the second phase, preliminary data suggest an associated reduction in length of stay.
The intention of this staged project was to demonstrate the process of knowledge transfer to practice. The planning, coordination, and evaluation are basic operational milestones in applying research to the field. The knowledge transfer approach is a systematic means to evidence-based practice. The intervention process lacked the control and number of participants present in more rigorous research, but our intention was more about replication of best practice and sharing our experience with what has been reported elsewhere in prior research.
A question that arose during both phases of implementation was whether aromatherapy should be given pre-emptively to all surgical patients. In the first phase of our project, we measured risk factors for PON and found them not to be correlated with PON. A larger correlation study might reveal an association, in which case aromatherapy might be initiated sooner to patients identified as high risk. Exploring the impact of self-administration might also reveal that the patients’ ability to control dosing could influence symptoms.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231213097 – Supplemental material for A Knowledge-Transfer Project to Reduce Postoperative Nausea and Improve Patient Throughput in Orthopedics
Supplemental material, sj-docx-1-hss-10.1177_15563316231213097 for A Knowledge-Transfer Project to Reduce Postoperative Nausea and Improve Patient Throughput in Orthopedics by Patricia Quinlan, Adero Gaudin and Jake White in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316231213097 – Supplemental material for A Knowledge-Transfer Project to Reduce Postoperative Nausea and Improve Patient Throughput in Orthopedics
Supplemental material, sj-docx-2-hss-10.1177_15563316231213097 for A Knowledge-Transfer Project to Reduce Postoperative Nausea and Improve Patient Throughput in Orthopedics by Patricia Quinlan, Adero Gaudin and Jake White in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316231213097 – Supplemental material for A Knowledge-Transfer Project to Reduce Postoperative Nausea and Improve Patient Throughput in Orthopedics
Supplemental material, sj-docx-3-hss-10.1177_15563316231213097 for A Knowledge-Transfer Project to Reduce Postoperative Nausea and Improve Patient Throughput in Orthopedics by Patricia Quinlan, Adero Gaudin and Jake White in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316231213097 – Supplemental material for A Knowledge-Transfer Project to Reduce Postoperative Nausea and Improve Patient Throughput in Orthopedics
Supplemental material, sj-docx-4-hss-10.1177_15563316231213097 for A Knowledge-Transfer Project to Reduce Postoperative Nausea and Improve Patient Throughput in Orthopedics by Patricia Quinlan, Adero Gaudin and Jake White in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316231213097 – Supplemental material for A Knowledge-Transfer Project to Reduce Postoperative Nausea and Improve Patient Throughput in Orthopedics
Supplemental material, sj-docx-5-hss-10.1177_15563316231213097 for A Knowledge-Transfer Project to Reduce Postoperative Nausea and Improve Patient Throughput in Orthopedics by Patricia Quinlan, Adero Gaudin and Jake White in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316231213097 – Supplemental material for A Knowledge-Transfer Project to Reduce Postoperative Nausea and Improve Patient Throughput in Orthopedics
Supplemental material, sj-docx-6-hss-10.1177_15563316231213097 for A Knowledge-Transfer Project to Reduce Postoperative Nausea and Improve Patient Throughput in Orthopedics by Patricia Quinlan, Adero Gaudin and Jake White in HSS Journal®
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was not required for this commentary.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.