
Abstract
Given that the number of total joint arthroplasties (TJAs) performed worldwide is expected to continue to increase, and there are significant costs associated with these procedures, selecting candidates for same-day or 23-hour discharge is important in lowering costs and providing greater access. Younger, healthier patients are excellent candidates for same-day discharge after TJA. Preoperative medical assessment can help exclude patients who may not be candidates, such as patients with 1 or more comorbidities that increase the risk of intra- and postoperative complications and who may require a longer period of monitoring
Keywords
Introduction
The number of total joint arthroplasties (TJAs) performed worldwide is expected to continue to increase. Significant associated costs include hospital admission and postoperative rehabilitation at an acute, subacute, or outpatient rehabilitative facility or the patient’s home. Over the past decade, interest has increased in selecting patients who may be candidates for same-day discharge or discharge less than 23 hours after TJA.
Almost all TJA procedures are elective, providing a unique opportunity to evaluate patients preoperatively and to determine which can be safely discharged the same day or within 23 hours. As providers work conscientiously to provide access to TJA to as many patients as possible, while trying to contain costs, they must keep patient safety and procedure outcome top of mind. A key concept is preoperative medical optimization, which helps decrease intraoperative and postoperative complications. Reduction of complications benefits patients and is associated with lowered costs.
Complications
Although the rate of complications after TJA has fallen, thromboembolic events resulting in myocardial infarction, stroke, and pulmonary embolism are among the most common complications. A joint registry at the Mayo Clinic analyzed data over a 10-year period (1986-1995) and found the rate of myocardial infarction, pulmonary embolism, deep vein thrombosis, and death were 2.2%, 0.4%, 0.7%, 1.5%, and 0.5%, at 30 days after surgery, respectively [24]. Myocardial infarction was more frequent in men and patients 70 years of age and older. Perioperative stroke is rare but can be devastating and the rate of death at 1 year is elevated [29]. Surgical site infections, particularly periprosthetic joint infection (PJI), can result in sepsis and the need for revision. The overall risk of PJI is less than 1% [18]. A review of nearly 130 000 primary total knee arthroplasties reported a PJI rate of 0.5% at 1 year; male sex, younger age, diabetes, post-traumatic arthritis, patellar resurfacing, and discharge to rehabilitative care were associated with PJI risk [26].
Immunosuppression can also increase PJI risk. The American College of Rheumatology and the American Association of Hip and Knee Surgeons have published a guideline on the perioperative management of antirheumatic medications in patients with rheumatic diseases undergoing elective total hip arthroplasty (THA) or total knee arthroplasty (TKA). The goal was to reduce the risk of infection while holding immunosuppressive medications, balancing the risk of disease flare-ups [16]. In addition, postoperative delirium can occur, especially in patients who have decreased cognition preoperatively. Osteoporosis can increase the risk of periprosthetic fracture. Studies have also shown an increased risk of hip fracture 1 to 5 years after THA and TKA [32,39]. Studies looking at periprosthetic fracture during TKA have shown an incidence of 0.3% to 2.5% [9,33]. It is important to evaluate bone health preoperatively, especially as the number of elderly patients having TJA increases.
Selection
Young, healthy patients are excellent candidates for same-day discharge after TJA and typically prefer to be discharged on the day of surgery. Preoperative education can help prepare the patient for surgery and for the postoperative course. During the preoperative medical evaluation, additional education can be provided. A home assessment can be made during a preoperative physical therapy assessment to ensure that a safe discharge is possible. Any needed assistive devices or aides, such as a raised toilet seat or ambulation supports, can be recommended and the patient can purchase these products preoperatively. It is ideal for the patient to have someone stay with them on the night of surgery. When the patient has comorbidities, a preoperative assessment can guide whether the patient can be discharged safely on the day of surgery (Table 1). Some organizations have an age cutoff, such as 70 or 80 years, whereas other organizations favor consideration of physiologic and not biologic age.
Exclusion criteria for same-day total joint arthroplasty.
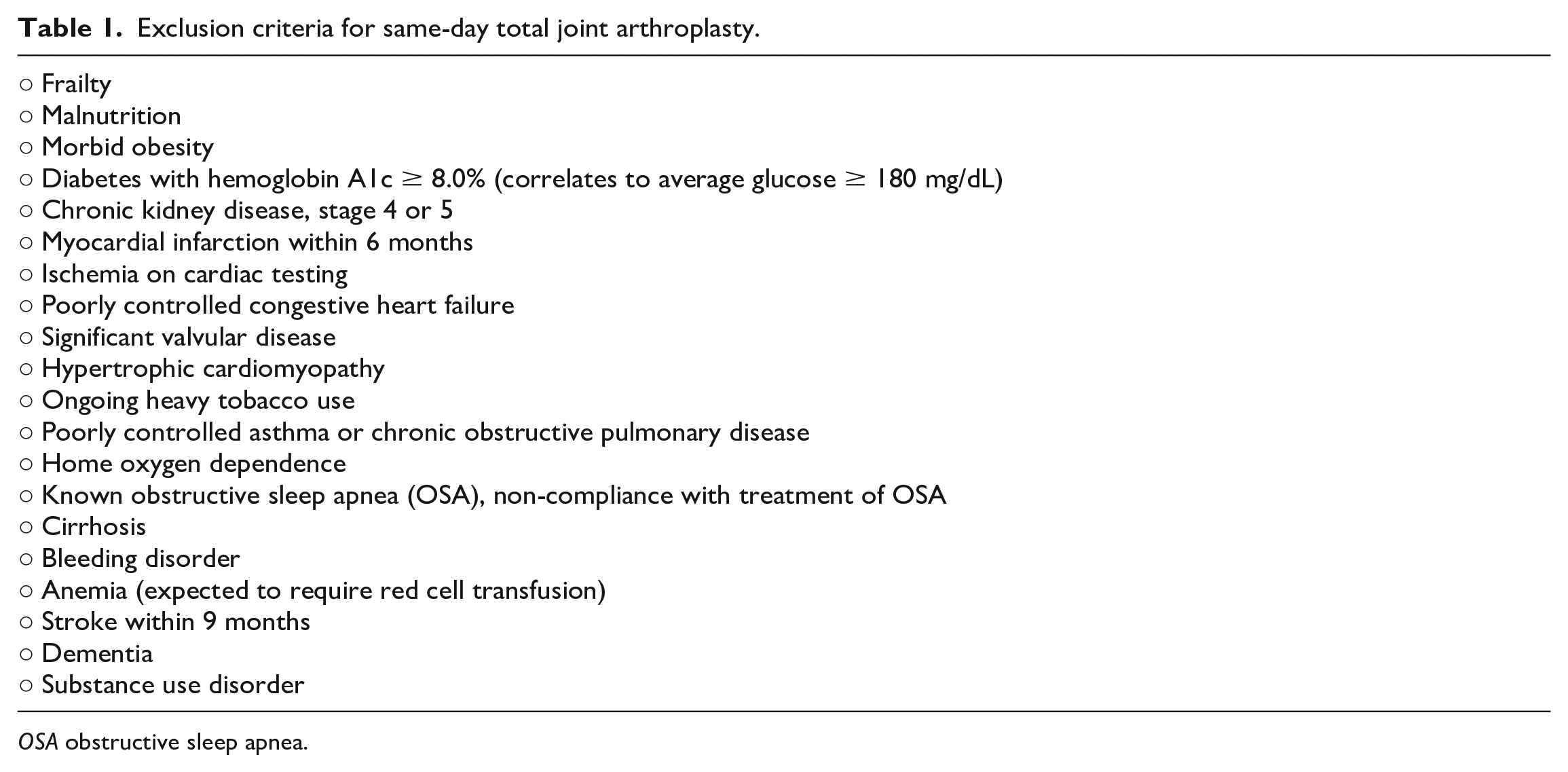
OSA obstructive sleep apnea.
Frailty
As the prevalence of hip and knee osteoarthritis increases with age, more patients with a greater number of comorbidities will be presenting for TJA. Frailty may be the best predictor of postoperative complications and poor outcomes. There are many frailty calculators, although none have been validated in TJA. The FRAIL calculator, validated in hip-fracture patients and simple to perform, includes 5 components: fatigue, resistance, ambulation, illness (more than 5 comorbidities), and weight loss (5% over 6 months) [15]. Scores range from 0 to 5 (0 = best to 5 = worst) and represent frail (3 to 5), prefrail (1 to 2), and robust (0) health statuses. Patients who score as “frail” are probably not ideal candidates for same-day TJA.
Obesity and Malnutrition
Although not all studies that evaluated obese patients demonstrated an increased risk of complications, most studies suggest that a body mass index (BMI) of 40 or greater does increase the risk of perioperative complications. A retrospective study of 98 410 primary TKA patients in the National Inpatient Sample with morbid obesity (BMI ≥ 40) found increased risk for perioperative infection (odds ratio [OR] = 1.3; confidence interval [CI] = 1.1-1.7), wound dehiscence (OR = 1.3; CI = 1-1.7), and genitourinary complications (OR = 1.3; CI = 1.1-1.5) [10]. Complications rates may be even higher for patients with a BMI of 50 or greater [1].
Malnourished patients have more adverse clinical outcomes, including increased 30-day readmissions and higher hospital mortality rate when adjusted for age [7,35]. Obese patients can be malnourished. Malnutrition defined using the Academy of Nutrition and Dietetics-American Society of Parenteral and Enteral Nutrition (AND-ASPEN) consensus tool predicts 1.4 times higher risk of prolonged length of stay and hospital readmission and 5 times higher risk of hospital death. The incidence of complications was much higher in patients who were both malnourished and obese [19]. Patients with morbid obesity and malnutrition are probably better cared for as inpatients.
Diabetes
Poorly controlled diabetes is a risk factor for several perioperative complications. Of 6000 patients with diabetes undergoing arthroplasty, a hemoglobin A1c of 7% or higher was associated with increased risk (OR = 1.22; CI = 1.01-1.47) for any complication, including return to the operating room, urinary tract infection, any infection, and acute kidney failure, plus an increased 90-day mortality rate (OR = 1.37; CI = 0.82-2.29) [19]. Many organizations have set a cutoff for an acceptable hemoglobin A1c of less than 7% to 8% for patients undergoing an elective orthopedic procedure. Patients should be optimized prior to surgery, but if surgery is to proceed for a patient who has poorly controlled diabetes, same-day TJA is not advisable.
Chronic Kidney Disease
Chronic kidney disease (CKD) is defined by the National Kidney Foundation as either a glomerular filtration rate of less than 60 mL/min/1.73 m2 or kidney damage for 3 months or longer. More specifically, stage 4 severe CKD corresponds to a glomerular filtration rate (GFR) of 15 to 29 mL/min/1.73 m2, whereas stage 5 severe CKD corresponds to a GFR of less than 15 mL/min/1.73 m2. Patients with end-stage renal disease (ESRD) require dialysis. Chronic kidney disease is thought to affect 13% of the US population and the incidence is expected to rise [20].
Postoperatively, patients with CKD are at risk for acute kidney injury (AKI), volume overload, and electrolyte disturbances. Chronic kidney disease has been recognized as a risk factor prior to surgery within the Revised Cardiac Risk Index [21]. Non–steroidal anti-inflammatory medications (NSAIDs) should be avoided in these patients, as there is a risk of AKI, which can make pain control more challenging. In a retrospective study of patients undergoing THA, the prevalence of CKD was found to be 6.1%, and these patients were found to have an increased risk of 90-day readmission (OR = 1.3; CI = 1.1-1.6), mortality (OR = 1.5; CI = 1.2-1.8), and superficial surgical site infection (OR = 1.3; CI = 1.2-1.8) [30]. Results were similar for patients with TKA [30]. Patients with ESRD have a longer length of stay, higher transfusion rate, and increased risk of PJI [22]. Chronic kidney disease is also a risk factor for major cardiovascular events (creatinine > 2 mg/dL).
It is critical to evaluate renal function preoperatively. For patients with CKD, it is important to review the risks of the procedure. Although this has not yet been well studied, it seems prudent to exclude patients with CKD stages 4 to 5 and ESRD from same-day TJA.
Cardiac Disease
Tests used to assess the risk of ischemic heart disease include echocardiogram, treadmill/nuclear stress test, coronary calcium computed tomography (CT), coronary CT angiogram, and coronary catheterization. Patients who have hip and knee osteoarthritis may not be able to generate 4 or more metabolic equivalents of task (METS) of activity, a level of activity associated with sufficient cardiopulmonary reserve to undergo an intermediate risk procedure without additional cardiac testing (TJA is considered intermediate risk).
For patients with significant cardiac risk factors, additional cardiac testing may be indicated and cardiac consultation may be warranted. If evaluation is notable for active ischemia, it is advisable to discuss with the patient’s cardiologist or internist the need for postoperative monitoring that may include troponin and electrolyte values, serial electrocardiography, and volume status. Patients with poorly controlled congestive heart failure will need to be monitored closely for volume status, oxygenation, and renal function. Significant valvular disease, such as moderate-to-severe aortic stenosis, requires closer hemodynamic monitoring. Hypertrophic cardiomyopathy can be associated with clinically significant arrhythmias and hemodynamic collapse. These patients are at risk for cardiovascular deterioration perioperatively and are best managed as inpatients.
Tobacco Use
Tobacco use affects wound healing, increases risk for cardiovascular disease, can reduce the rate of bone fusion, and may impair osseous integration. One study of almost 80 000 THAs and TKAs found that smoking increased the risk of wound complications at 1.8% compared to 1.1% for nonsmokers (P < .001) [11]. A 2011 meta-analysis of THAs and TKAs noted smoking was associated with an increased risk of all complications, including mortality, infection, and revision; the overall risk for death was 1.69 (OR = 1.69; CI = 1.08-2.64) [36]. All patients planning to undergo TJA should be referred to a smoking-cessation program. Patients should understand the deleterious effects of tobacco use on bone and wound healing. Patients who continue to use tobacco products heavily may not be ideal candidates for same-day TJA.
Chronic Pulmonary Disease
Patients with poorly controlled asthma and moderate-to-severe chronic obstructive pulmonary disease (COPD) need to be monitored postoperatively and are not good candidates for same-day TJA. Asthma is characterized by reversible airway obstruction, inflammation, and hyperresponsiveness [23]. Significant risk can be linked to a history of glucocorticoid use, hospital admission for acute respiratory failure, or a need for intubation. Patients with well-controlled asthma have the overall low risk and may be candidates for same-day TJA [40].
Patients should be instructed to take their asthma medications until surgery. Patients with mildly active disease may benefit from β2 agonists and systemic steroid treatment for a few days prior to surgery. Patients with severe or poorly controlled asthma are not ideal candidates for same-day TJA.
Chronic obstructive pulmonary disease describes chronic lung disease, including emphysema and chronic bronchitis. Airflow is blocked, making it more difficult to ventilate. Some patients are oxygen dependent. Patients with COPD have a 2.7- to 4.7-fold increased risk of postoperative pulmonary complications [3,34], most commonly atelectasis or pneumonia. Patients with mild or moderate COPD are candidates for same-day TJA, if it is well-managed and they are relatively asymptomatic, with normal room air pulse oximetry and no active respiratory infection. Pulmonary consultation and pulmonary function testing can help with this determination. Patients who are oxygen dependent or who have poorly controlled COPD are better managed as inpatients.
Obstructive Sleep Apnea
Obstructive sleep apnea (OSA) is a breathing disorder characterized by periodic upper airway collapse, often caused by a narrowed airway due to fatty deposits in the pharyngeal walls. Patients have hypopnea or apnea, resulting in hypoxia. An estimated 10% to 20% of the adult surgical population has OSA, and many are undiagnosed [13,28]. The incidence of hypoxia may be greater in an orthopedic population undergoing TJA, as many patients are obese, which is the greatest risk factor for OSA. Complicating care is that opioids are often prescribed postoperatively, which can worsen hypoxia associated with OSA.
A commonly used preoperative screening tool is STOP-Bang [4]. This tool considers snoring, daytime fatigue, observation of stopping to breathe while sleeping, hypertension, BMI over 35 kg/m2, age over 50 years, neck circumference greater than 16 inches, and male sex. The risk of OSA is calculated as low, intermediate, or high. Serum bicarbonate (HCO3) of 28 or greater increases the specificity of STOP-Bang screening in predicting moderate-to-severe OSA. The ideal assessment should be preoperative polysomnography, but this is often not practical.
Patients with known OSA who are noncompliant with either continuous positive airway pressure (CPAP) or an oral device or who have undiagnosed OSA and a “high” risk on screening are at increased risk of perioperative complications, including death. Comorbidities need to be considered if surgery is going to proceed. For patients considered at very high risk, it may be best to undergo a formal preoperative evaluation and begin CPAP preoperatively. Although some patients may be candidates for discharge within 23 hours, observation overnight to monitor hemodynamics, including hypoxia, is the safer option. The initial 24 hours after opioid administration marks the period of highest risk for acute respiratory insufficiency [6]. Unfortunately, postoperative days 3 through 7 still pose a high risk of worsening of sleep-disordered breathing [5]. The Anesthesia Patient Safety Foundation recommends continuous monitoring with pulse oximetry and at times capnography in high-risk patients [17].
Gastrointestinal and Liver Disease
Chronic liver disease and cirrhosis greatly increase the risk of perioperative complications, including the risk of infection as well as postoperative liver and or renal failure. Chronic liver disease may be suspected if laboratory testing reveals elevated international normalized ratio (INR), elevated liver function tests, low albumin, and decreased platelet count. A history of alcoholism, variceal bleeding, hepatitis B or C, or ascites can aid in diagnosis. Two scores have used to assess preoperative risk are the Child-Turcotte-Pugh (CTP) score and the Model for End-Stage Liver Disease (MELD) [12,27,31]. Patients with a low CTP or MELD score may be candidates for same-day TJA, if specific tests values are not of concern, such as a very low platelet count.
Bleeding Disorders and Anemia
Most candidates for same-day TJA are not expected to require blood products postoperatively. Patients at risk for bleeding need to be monitored postoperatively as inpatients and are not candidates for same-day TJA. Disorders of hemostasis can be due to platelet dysfunction (primary hemostasis) or clotting factor deficiency (secondary hemostasis). The best way to ascertain whether a patient has a bleeding disorder is to take a thorough history, not by ordering routine laboratory testing, such as platelet count or prothrombin time/partial thromboplastin time. Questions about prolonged bleeding with prior tooth extractions or surgeries, heavy and prolonged menses, or easy bruising can help target who would benefit from laboratory testing preoperatively.
Arthroplasty has the potential for significant blood loss due to soft-tissue trauma and the inability to cauterize bleeding bony surfaces. Anemia is common in patients undergoing elective orthopedic procedures and can be found in over 40% of patients preoperatively [37]. Preoperative anemia and postoperative blood transfusion are associated with poorer outcomes, including longer length of stay, infection, and higher 90-day readmission rate. The use of tranexamic acid has greatly reduced blood loss associated with orthopedic surgery and arthroplasty [8,38]. Whenever possible, the cause of preoperative anemia, such as iron deficiency, anemia of chronic disease, and gastrointestinal bleeding, should be understood. Optimization of anemia preoperatively is the goal, when possible (ie, oral, or intravenous iron or treatment of chronic gastrointestinal bleeding). More study is needed, but for same-day TJA, it may be prudent for patients to have a preoperative hemoglobin of 11.0 g/dL (higher for more complex procedures).
Stroke
A prior stroke or transient ischemic attack increases the risk of a subsequent stroke after surgery, although the overall risk of postoperative stroke is low. It is advisable to wait at least 30 days, but ideally 9 months, after an ischemic stroke to proceed with elective noncardiac, nonvascular procedures [14]. The highest risk of a postoperative stroke is within 30 days of a prior stroke. Prior stroke is also a risk factor for major adverse cardiovascular events. Consequently, patients with a stroke history are not ideal candidates for same-day TJA.
Neurologic Disease Including Dementia
Patients with neuromuscular disorders including Parkinson’s disease, multiple sclerosis, myasthenia gravis, and muscular dystrophies may find it challenging to achieve postoperative rehabilitation goals. Many of these patients may also be at risk for pulmonary decompensation, including aspiration. The severity of the neuromuscular disorder must be considered when evaluating for the suitability of a same-day TJA.
Preoperative dementia is one of the strongest risk factors for postoperative delirium. Delirium is the most common surgical complication among older adults, with an incidence of 15% to 25% after major elective surgery and 50% after high-risk procedures, such as hip-fracture repair [25,27]. Ideally, it is best to screen patients preoperatively for decreased cognition. One delirium risk stratification instrument is Age, WORLD backwards, Orientation, iLlness severity, Surgery-specific risk (AWOL-S) that assesses age greater or less than 80 years; the ability to spell the word “world” backwards; orientation as assessed by correctly stating the city, state, county, hospital name, and floor; a nursing assessment of illness severity; and surgery-specific risk [41]. For patients whose screening indicates risk for postoperative delirium, inpatient admission is prudent so that they can be monitored and their medications adjusted as needed.
Substance Misuse
Preoperative misuse of alcohol, opioids, or illicit drugs such as cocaine can affect pain control after TJA. Prescribing an opioid postoperatively to patients misusing alcohol, illicit drugs, or opioids can increase the risk of death. A study of 153 consecutive patients admitted to an orthopedic unit noted more medical and behavioral complications among those who smoked or consumed alcohol heavily [42].
A validated screening tool for alcohol dependence is the Alcohol Use Disorders Identification Test-Concise (AUDIT-C) [2]. It is simple to use and can help identify patients who may be at risk of withdrawal postoperatively. All US states have a prescription drug monitoring program (PDMP) in which prescribers can view controlled substances recently filled at pharmacies, such as opioids. Toxicology screens can detect illicit drugs.
If substance misuse is suspected, a preoperative program designed to help the patient abstain from or reduce substance use is prudent. Same-day TJA may not be appropriate for patients who continue to misuse substances at high doses.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231212880 – Supplemental material for Comorbid Factors and Selection for Same-Day Total Joint Arthroplasty
Supplemental material, sj-docx-1-hss-10.1177_15563316231212880 for Comorbid Factors and Selection for Same-Day Total Joint Arthroplasty by Linda A. Russell in HSS Journal®
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was not required for this review article.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.