
Abstract
Background:
Increasing numbers of patients are undergoing total joint arthroplasty as a treatment for osteoarthritis, which can be an anxiety-provoking experience. Setting expectations through a preoperative physical therapy (pre-op PT) session can alleviate some of these stressors, potentially decrease hospital length of stay (LOS), and promote home discharge.
Purpose:
We sought to determine whether attending a pre-op PT session is associated with decreased hospital LOS and home discharge in total hip arthroplasty (THA) and total knee arthroplasty (TKA) patients.
Methods:
A retrospective cohort study was performed of 20,822 patients who underwent THA or TKA between January 2020 and December 2023. Pre-op PT attendance and covariates, including patient demographics and clinical data, were collected and analyzed for association with LOS and discharge disposition.
Results:
Unadjusted univariate analysis revealed that THA and TKA patients who received pre-op PT had a significantly lower average LOS and were more likely to be discharged home. Our multivariate regression model showed that pre-op PT was not significantly associated with LOS in both groups but was significantly associated with home discharge among THA patients.
Conclusions:
Our retrospective study of the effect of pre-op PT education on LOS and discharge disposition for elective THA and TKA patients found different results in univariate and multivariate analysis. Further study is needed to confirm the association found on multivariate analysis between pre-op PT and home discharge in THA patients.
Keywords
Introduction
The hip and knee joints are commonly affected by osteoarthritis, the most common type of arthritis [2]. Its prevalence has resulted in an increased rate of total hip arthroplasty (THA) and total knee arthroplasty (TKA). The numbers of THA and TKA procedures are expected to increase by more than 200% and 600%, respectively, by 2030 [7,20]. Total joint arthroplasty (TJA) is a major surgical procedure that can be physically and psychologically stressful for patients. Preoperative education for THA and TKA patients can reduce their anxiety and enhance postoperative outcomes [11]. While hospital length of stay (LOS) has decreased due to factors such as medications, technology, and advancements in procedures, preoperative education has also been shown to decrease hospital LOS [7]. An education session can improve patients’ expectations by providing useful information on the surgical procedure, discharge, rehabilitation, and postoperative care [10,15]. A study by DeMik et al [3] states that a reduction in LOS and an increase in home discharge are likely due to improvements in preoperative optimization and education before elective TJA.
As the number of these procedures increases, it is important to identify the strategies that improve patient outcomes [7]. At our institution, surgeons can refer patients for educational preoperative physical therapy (pre-op PT) [4], a 40-minute one-to-one session offered either in person or virtually. The objective of pre-op PT is to review postoperative surgeon preferences or precautions, hospital expectations, home preparation or modification, and discharge planning. Patients also can practice exercises, transfers, ambulation, stair negotiation, and the use of an assistive device if applicable. They are encouraged to ask the physical therapist questions on their postoperative course, and the therapist can obtain information for directing patient care. While the literature has conflicting evidence on whether preoperative education has a significant effect on hospital LOS [5,8], it has been shown to contribute to increasing rates of home discharge, as opposed to discharge to acute rehabilitation or skilled nursing facilities, after TJA [16].
The aims of this study were to evaluate how pre-op PT sessions prior to THA and TKA affect hospital LOS and discharge destination, with and without accounting for clinical and demographic covariates. We hypothesized that THA or TKA patients who participated in pre-op PT would have a reduced hospital LOS and be more likely to be discharged home than those who did not participate in these sessions.
Methods
We conducted a retrospective cohort study of patients who underwent primary, unilateral TJA from a single, orthopedic institution. A review was performed on patients who underwent THA or TKA from January 2020 to December 2022. Patients were excluded from the study if they had undergone revision or bilateral procedures or had LOS of greater than 7 days. After inclusion criteria were applied, a total of 20,822 patients were included in analysis, including 11,206 patients who underwent THA and 9616 patients who underwent TKA (Supplemental Fig. 1).
Of THA patients, the average age was 64 years, and the majority were women, White, non-Hispanic, and had commercial insurance. Of patients who received a TKA, the average age was 67 years, and the majority were women, White, non-Hispanic, and had Medicaid or Medicare.
Demographic data including sex, body mass index (BMI), race, ethnicity, and age were collected at baseline. Clinical data collected included preoperatively collected Risk-Assessment Prediction Tool (RAPT) scores used to predict patient discharge disposition [14,19]; postoperatively collected Activity Measure for Post-Acute Care (AM-PAC) “6-Clicks” Basic Mobility Short Form to evaluate difficulty, assistance, and limitations in activities of daily living as it relates to hospital discharge destination [17]; Lower Extremity Functional Scales (LEFS) scores; payer group; surgery year; whether or not the patient chose to receive post-op PT through a postoperative telemedicine rehabilitation program; whether or not the patient had a preoperative social work visit; number of inpatient physical therapy visits; surgical or hospital complication diagnoses; and our independent variable of interest—whether or not the patient participated in a pre-op PT session.
The LOS was calculated from the time of admission to the time of discharge based on timestamps in the electronic health record (EHR) with partial hours being rounded down (eg, 30.5 hours = 30 hours). Discharge disposition was determined by the discharging physician and documented in the EHR.
Statistical Analysis
Descriptive statistics of the study population were summarized using means and standard deviations for continuous variables and frequencies and percentages for discrete variables. Demographic and clinical characteristics of those patients who underwent pre-op PT prior to their surgery were compared with those who did not. Independent samples t tests were performed to compare LOS between patients who did and did not have pre-op PT sessions. Chi-square tests were performed to compare pre-op PT with discharge destination (home/home with home care or to a rehabilitation/skilled nursing facility).
Multivariable linear regression was performed to analyze the effect of pre-op PT, accounting for all other collected demographic and clinical variables, on hospital LOS. Similarly, multivariable logistic regression was performed to analyze the effect of pre-op PT on discharge destination, accounting for all other collected variables. Complication was defined by presence of a surgical complication documented in the brief operative note or the occurrence of hospital complication any time during the hospital stay; this information was obtained from reviewing billing diagnoses. In the final models, factors that achieved a P value of .05 or less were considered statistically significant. All other factors that did not reach statistical significance were retained in the final model as covariates. To account for any multicollinearity due to a high degree of correlation between independent variables, variance inflation factors (VIFs) were calculated. For variables with VIF values of 5 or more, one of the redundant correlated variables was dropped from the model. Results of the linear regression analysis are reported as β coefficients and 95% confidence intervals to show how LOS changes as the independent variables vary. Results of the logistic regression analysis are reported as adjusted odds ratios (aOR) and 95% confidence intervals. All analyses were performed using SPSS version 23.0 (IBM Corporation).
Results
The THA patients who received pre-op PT (n = 8451) differed significantly from patients who did not receive pre-op PT (n = 2755) in average age, inpatient PT visits, LEFS scores, AM-PAC scores, race, ethnicity, surgery year, payer group, whether or not they were scheduled for telerehabilitation, discharge disposition, whether or not they received pre-op or post-op social work visits, and whether or not they had hospital complications (Supplemental Table 1). The TKA patients who received pre-op PT (n = 7243) differed significantly from those who did not receive pre-op PT (n = 2373) on the same factors as the THA group, excluding race and ethnicity and with the addition of average BMI and RAPT score (Supplemental Table 1).
Unadjusted univariate analysis showed that in both the THA and TKA groups, patients who received pre-op PT had statistically significantly lower average LOS than patients who did not receive pre-op PT (THA: 38.6 vs 44.6 hours, P < .001; TKA: 47.2 vs 51.5 hours, P < .001). In addition, univariate analysis showed that in both the THA and TKA groups, patients who were discharged home were more likely to have participated in pre-op PT than patients who did not (THA: 76% vs 68%, P = .008; TKA: 76% vs 70%, P = .02).
Multivariable linear regression of LOS among THA and TKA patients (Table 1), adjusting for all demographic and clinical covariates included in analysis, showed that pre-op PT was not statistically significantly associated with LOS (THA β = −0.39, confidence interval [CI] = −1.08 to 0.31, P = .278; TKA β = 0.03; CI = −0.77 to 0.84, P = .936). All other covariates, except for surgery year of 2021 among THA patients and BMI among TKA patients, were significantly associated with LOS.
Multivariable Linear Regression of LOS.
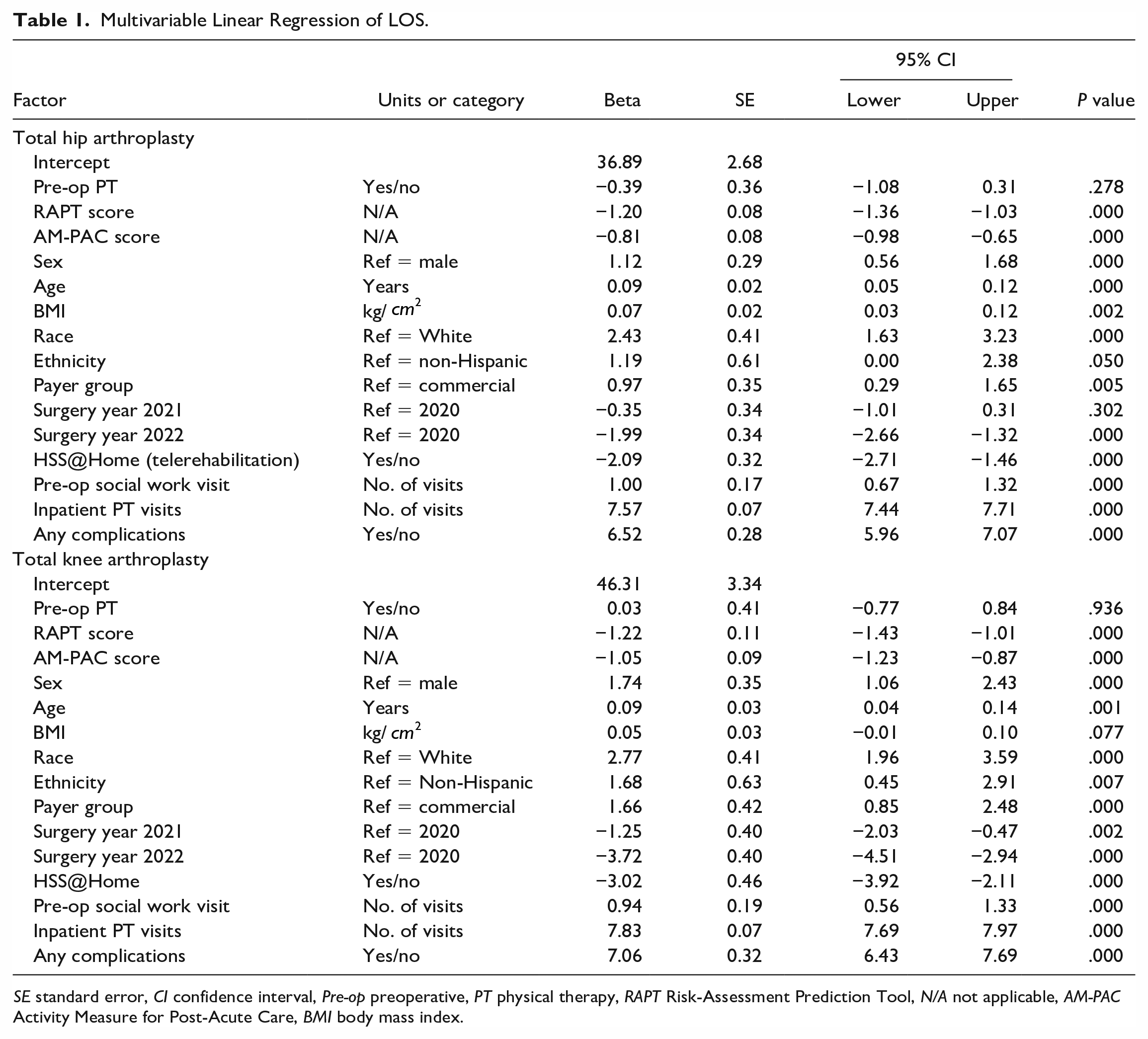
SE standard error, CI confidence interval, Pre-op preoperative, PT physical therapy, RAPT Risk-Assessment Prediction Tool, N/A not applicable, AM-PAC Activity Measure for Post-Acute Care, BMI body mass index.
Multivariable logistic regression analysis of discharge disposition (Table 2), adjusting for all demographic and clinical covariates included in analysis, showed that pre-op PT was significantly associated with an increased odds of discharge to home in THA patients (aOR = 2.16, CI = 1.13 to 4.14, P = .02) but not in TKA patients (aOR = 1.49, CI: 0.86 to 2.58, P = .151).
Multivariable Logistic Regression of Discharge to Home.
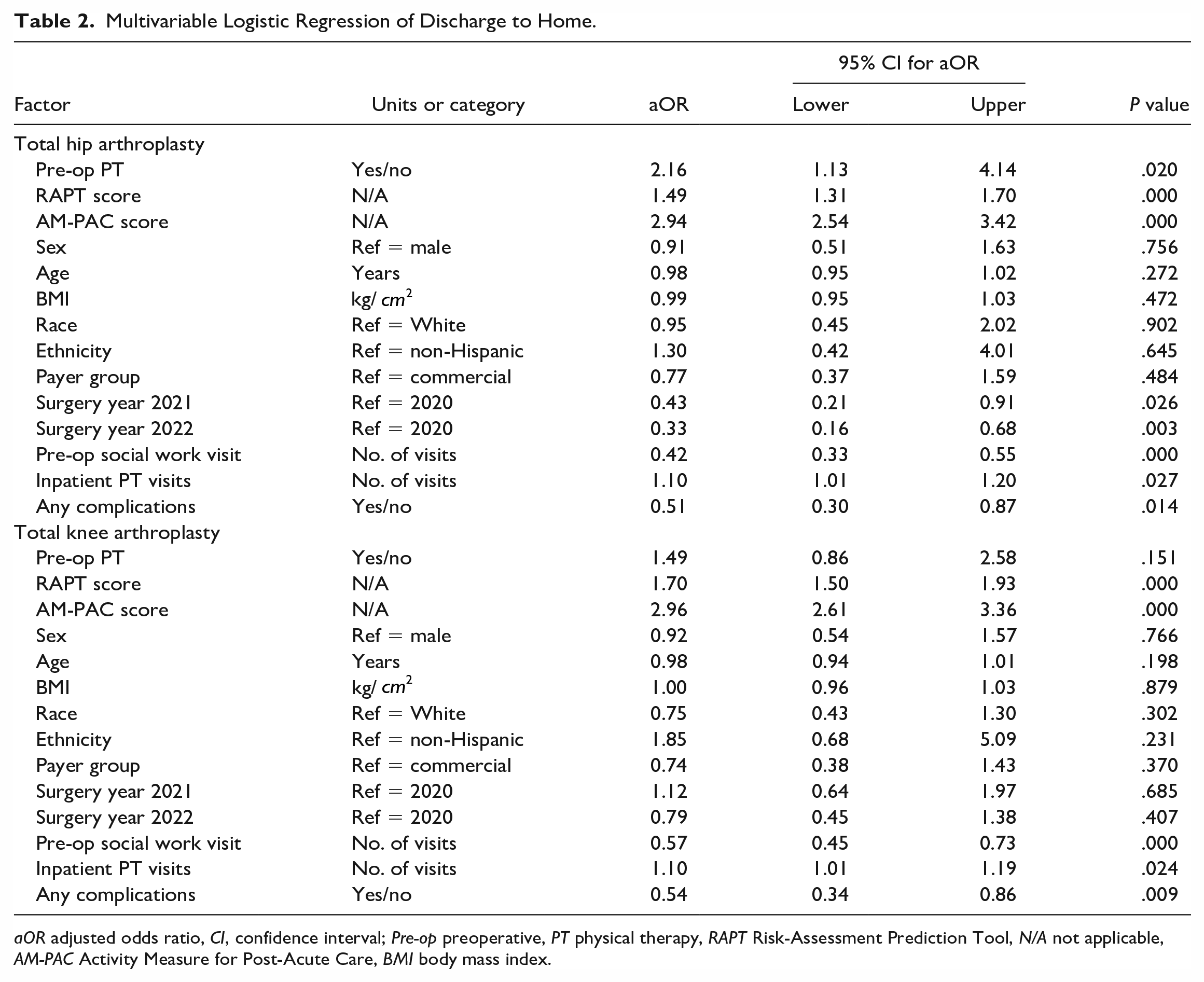
aOR adjusted odds ratio, CI, confidence interval; Pre-op preoperative, PT physical therapy, RAPT Risk-Assessment Prediction Tool, N/A not applicable, AM-PAC Activity Measure for Post-Acute Care, BMI body mass index.
Discussion
The benefits of pre-op PT education prior to TJA are well documented [7,12,15,18]. Patients report feeling better prepared, feeling more able to manage their pain, and having improved psychological status after receiving education about the upcoming surgery. Currently, there is a dichotomy in published research on the effects of pre-op PT on LOS, with some studies showing a significant difference in LOS with the implementation of pre-op PT and others finding no effect [5,8]. At our institution, the goals of pre-op PT are to help patients feel prepared for their upcoming surgery, to establish postoperative expectations and goals, and to improve patient outcomes [4]. With a large sample size of 20,822 patients who underwent primary TJA across 3 years—including approximately 75% of these patients who received a pre-op PT session—our study suggests pre-op PT may affect LOS and discharge disposition. We found that in both the THA and TKA groups, patients who received the pre-op PT session had a significantly lower average LOS and were more likely to be discharged home than patients who did not receive pre-op PT. However, our multivariate regression model showed that, when accounting for demographic and clinical covariates, pre-op PT was not statistically significantly associated with LOS and was significantly associated only with discharge disposition in the THA group.
This study has limitations. First, a limiting factor to comparing pre-op PT versus non-pre-op PT patient populations is that much of the demographic data differed between the 2 groups. For example, patients who participated in pre-op PT on average were older and were more likely to have commercial insurance (Supplemental Table 1). While this limits the inferences we can draw about pre-op PT, these factors were accounted for in our multivariate regression models. Second, it should be noted that this analysis did not consider the patient’s surgical time of day. At our institution, patients can be seen by the PT team until 9
In 2022, our institution led an initiative to increase support for same-day discharge for TJA patients who met appropriate discharge criteria. This initiative likely created a historical bias, contributing to the decrease in hospital LOS for all patients in 2022. In addition, cost analysis suggests that third-party reimbursement has driven shorter LOS, specifically same-day discharge, as it can lead to significant cost savings [1].
Our findings point to interesting insights into factors affecting postsurgical LOS and discharge disposition. Our regression analysis suggested that being female, older, with a higher BMI and Medicare or Medicaid insurance was statistically significantly associated with a longer LOS, regardless of pre-op PT education. As expected, patients who experienced a complication, either during or after surgery, also had a longer LOS; these issues may correspond to increased medical management and restrictions such as weightbearing or surgical precautions that require greater education and mobility practice. These findings are consistent with prior studies on increased LOS [6,21]. Older patients and patients on Medicare/Medicaid were less represented in our pre-op PT group. Our findings are also consistent with the literature on RAPT and AM-PAC scores predicting home discharge, as higher scores for these assessment tools reflect decreased risk of requiring inpatient rehabilitation and reduced functional impairment, respectively [9,14,17].
Our finding that THA patients—but not TKA patients—were more likely to be discharged home if they received pre-op PT while accounting for covariates may be attributed to postoperative pain; prior studies suggest that TKA patients experience higher levels of acute pain postoperatively compared with THA patients [13]. Patients with increased pain may have unsafe mobility, preventing them from achieving milestones required for safe home discharge.
In conclusion, our retrospective analysis suggests that THA and TKA patients participating in pre-op PT at our institution had reduced hospital LOS, but when accounting for demographic and clinical covariates, we did not find a significant association between pre-op PT and LOS in both groups. There was a significant association between pre-op PT and discharge home for THA patients, but not for TKA patients. Future studies should account for additional factors such as time of surgery and investigate other potential benefits of pre-op PT, such as patient satisfaction.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231208423 – Supplemental material for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay
Supplemental material, sj-docx-1-hss-10.1177_15563316231208423 for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay by Monika Brossier, Jessica Schwartz-Dillard, Danielle McInerney, Jerome Brent Smith, Joseph Nguyen, Mary Murray-Weir and Danielle Edwards in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316231208423 – Supplemental material for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay
Supplemental material, sj-docx-2-hss-10.1177_15563316231208423 for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay by Monika Brossier, Jessica Schwartz-Dillard, Danielle McInerney, Jerome Brent Smith, Joseph Nguyen, Mary Murray-Weir and Danielle Edwards in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316231208423 – Supplemental material for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay
Supplemental material, sj-docx-3-hss-10.1177_15563316231208423 for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay by Monika Brossier, Jessica Schwartz-Dillard, Danielle McInerney, Jerome Brent Smith, Joseph Nguyen, Mary Murray-Weir and Danielle Edwards in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316231208423 – Supplemental material for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay
Supplemental material, sj-docx-4-hss-10.1177_15563316231208423 for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay by Monika Brossier, Jessica Schwartz-Dillard, Danielle McInerney, Jerome Brent Smith, Joseph Nguyen, Mary Murray-Weir and Danielle Edwards in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316231208423 – Supplemental material for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay
Supplemental material, sj-docx-5-hss-10.1177_15563316231208423 for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay by Monika Brossier, Jessica Schwartz-Dillard, Danielle McInerney, Jerome Brent Smith, Joseph Nguyen, Mary Murray-Weir and Danielle Edwards in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316231208423 – Supplemental material for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay
Supplemental material, sj-docx-6-hss-10.1177_15563316231208423 for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay by Monika Brossier, Jessica Schwartz-Dillard, Danielle McInerney, Jerome Brent Smith, Joseph Nguyen, Mary Murray-Weir and Danielle Edwards in HSS Journal®
Supplemental Material
sj-docx-7-hss-10.1177_15563316231208423 – Supplemental material for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay
Supplemental material, sj-docx-7-hss-10.1177_15563316231208423 for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay by Monika Brossier, Jessica Schwartz-Dillard, Danielle McInerney, Jerome Brent Smith, Joseph Nguyen, Mary Murray-Weir and Danielle Edwards in HSS Journal®
Supplemental Material
sj-docx-8-hss-10.1177_15563316231208423 – Supplemental material for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay
Supplemental material, sj-docx-8-hss-10.1177_15563316231208423 for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay by Monika Brossier, Jessica Schwartz-Dillard, Danielle McInerney, Jerome Brent Smith, Joseph Nguyen, Mary Murray-Weir and Danielle Edwards in HSS Journal®
Supplemental Material
sj-docx-9-hss-10.1177_15563316231208423 – Supplemental material for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay
Supplemental material, sj-docx-9-hss-10.1177_15563316231208423 for Preoperative Education Prior to Hip or Knee Arthroplasty Is Associated With Home Discharge but Not Reduced Length of Stay by Monika Brossier, Jessica Schwartz-Dillard, Danielle McInerney, Jerome Brent Smith, Joseph Nguyen, Mary Murray-Weir and Danielle Edwards in HSS Journal®
Footnotes
Acknowledgements
The authors wish to thank Sharlynn Tuohy, Sherry Backus, and Gwen Weinstock-Zlotnick.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived for all patients included in this study.
Level of Evidence
Level III, Retrospective Cohort Study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.