
Abstract
Introduction
Total joint arthroplasty (TJA), particularly of the knee and hip, is among the most common surgeries in the United States [13]. There are an estimated 790,000 total knee replacements and more than 450,000 total hip replacements performed in the United States every year [3].
Nationally, there has been an increase in same-day discharges and shorter length of stay (LOS) for inpatients following many types of surgery, including TJA [10]. Unnecessary days in an inpatient facility increase risks for complications like falls or healthcare-associated infections. This can also negatively impact the patient experience, increase costs, and, in recent years, prolong a patient’s risk of exposure to COVID-19 [20].
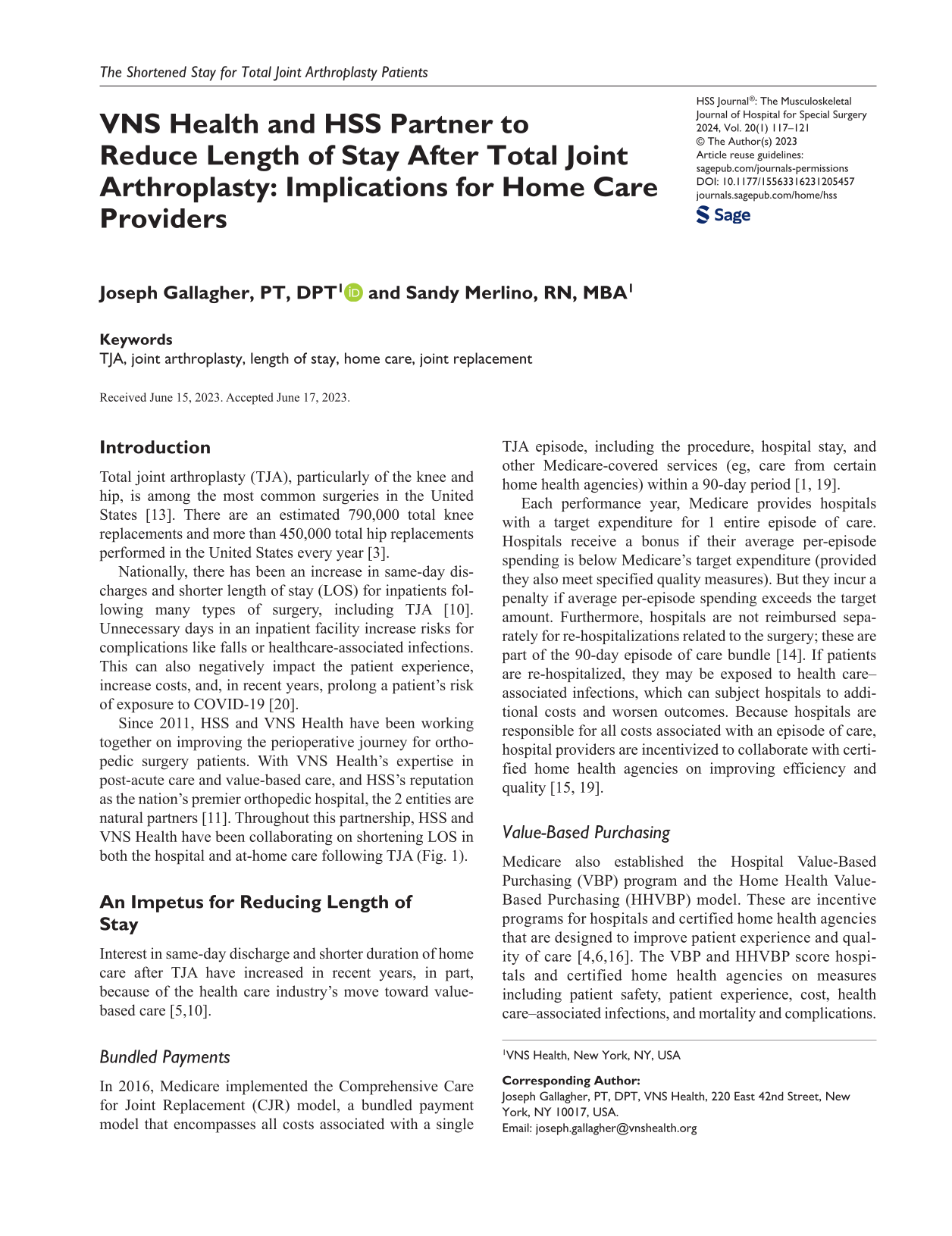
Since 2011, HSS and VNS Health have been working together on improving the perioperative journey for orthopedic surgery patients. With VNS Health’s expertise in post-acute care and value-based care, and HSS’s reputation as the nation’s premier orthopedic hospital, the 2 entities are natural partners [11]. Throughout this partnership, HSS and VNS Health have been collaborating on shortening LOS in both the hospital and at-home care following TJA (Fig. 1).
Admissions of HSS patients to VNS Health Home Care (left axis) and average length of stay in home care after total joint arthroplasty (right axis). VNS Health administrative data, Electronic Medical Record. HSS Hospital for Special Surgery, LOS length of stay.
An Impetus for Reducing Length of Stay
Interest in same-day discharge and shorter duration of home care after TJA have increased in recent years, in part, because of the health care industry’s move toward value-based care [5,10].
Bundled Payments
In 2016, Medicare implemented the Comprehensive Care for Joint Replacement (CJR) model, a bundled payment model that encompasses all costs associated with a single TJA episode, including the procedure, hospital stay, and other Medicare-covered services (eg, care from certain home health agencies) within a 90-day period [1, 19].
Each performance year, Medicare provides hospitals with a target expenditure for 1 entire episode of care. Hospitals receive a bonus if their average per-episode spending is below Medicare’s target expenditure (provided they also meet specified quality measures). But they incur a penalty if average per-episode spending exceeds the target amount. Furthermore, hospitals are not reimbursed separately for re-hospitalizations related to the surgery; these are part of the 90-day episode of care bundle [14]. If patients are re-hospitalized, they may be exposed to health care–associated infections, which can subject hospitals to additional costs and worsen outcomes. Because hospitals are responsible for all costs associated with an episode of care, hospital providers are incentivized to collaborate with certified home health agencies on improving efficiency and quality [15, 19].
Value-Based Purchasing
Medicare also established the Hospital Value-Based Purchasing (VBP) program and the Home Health Value-Based Purchasing (HHVBP) model. These are incentive programs for hospitals and certified home health agencies that are designed to improve patient experience and quality of care [4,6,16]. The VBP and HHVBP score hospitals and certified home health agencies on measures including patient safety, patient experience, cost, health care–associated infections, and mortality and complications. Their scores are compared with those of other hospitals and home health agencies, as well as to their own scores from the previous year. Medicare may reward organizations for efficiency and outcomes [7,16]—thus encouraging providers from across the continuum of care to work together on enhancing patient safety, improving outcomes, and boosting efficiency [5].
Reducing Length of Stay
Reduced LOS and improved outcomes have been primarily due to new approaches in 5 areas: discharge destination, at-home rehabilitation, preoperative preparation, clinical care, and communication.
Changing Discharge Destination
Discharge destination contributes significantly to both patient outcomes and the cost of care for TJA. The cost of a single inpatient rehabilitation episode can be more than 3 times greater than the cost of a home care episode [8]. Conversely, research has shown that decreases in inpatient rehabilitation have contributed to lower average costs per episode of care [19]. In addition, patients discharged to inpatient rehabilitation facilities after TJA have a greater likelihood of adverse events during recovery, including unplanned hospital readmission, complications, and even post-discharge morbidity [9,12].
Recognizing the importance of reducing costs and improving outcomes, in January 2013, VNS Health and HSS came together to address moving away from inpatient rehabilitation and toward home care as the default discharge destination post-TJA.
When VNS Health and HSS first began collaborating on shortening LOS, many TJA patients remained hospitalized for 3 to 5 days following surgery. A large percentage of these patients were then sent to an inpatient acute rehabilitation facility for 1 to 2 weeks or to a subacute facility for approximately 3 weeks and then were discharged to home care. VNS Health and HSS initiated an alternative approach that has enabled the majority of patients to bypass inpatient rehabilitation.
HSS began discharging patients when they were medically and functionally cleared to go home, regardless of the time of day. VNS Health committed to ensuring that these patients received care within 24 hours of hospital discharge. This has reduced time spent in the hospital following surgery; about half of patients go home the same day and the rest typically stay for only 1 night.
Reevaluating At-Home Rehabilitation
VNS Health piloted the “Intensive Rehab at Home” program. For the first week after discharge, physical therapists made daily home visits for physical therapy, providing a level of care consistent with inpatient programs. These home visits also reduced the risk of complications from inpatient facility stays that could potentially send patients back to the hospital.
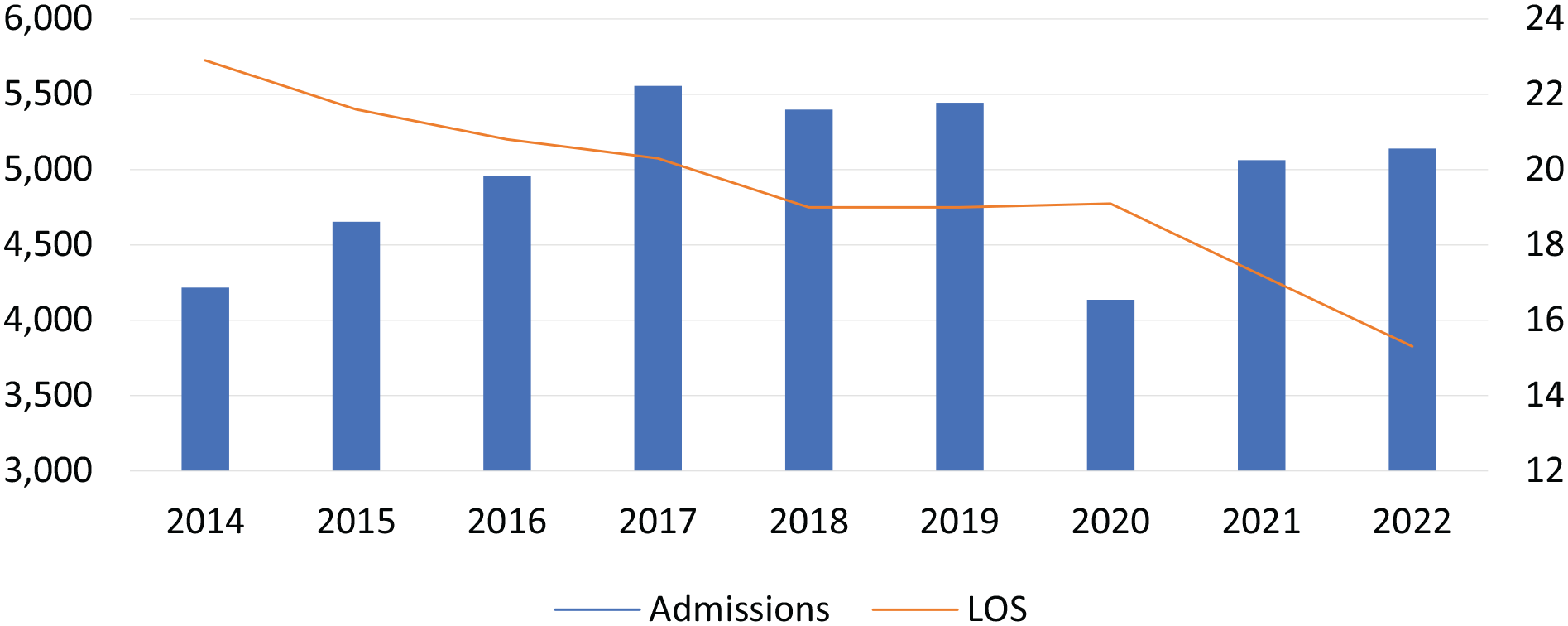
When reimbursement models changed in 2016, VNS Health remained flexible and reevaluated the program. Assessing whether all patients required a daily intensive rehabilitation regimen, they shifted toward a patient-centric plan of care to provide patients with what was needed to restore them to their optimal level of function. They offered a plan of care tailored to a patient’s environment and physical needs; this meant going from daily physical therapy for approximately 4 weeks to an average of 6 visits over a 2-week period (Fig. 2). Even with significantly fewer visits, patient outcomes remained the same.
Average number of registered nurse (RN) and physical therapy (PT) visits per VNS Health Home Care Admission between 2017 and 2022. VNS Health administrative data, Electronic Medical Record.
Involving Home Care Teams in Preoperative Planning
Preoperative assessments have long been part of the perioperative process. Realizing the value of including input from home care services in preoperative planning, HSS invited VNS Health to partner with them at this early stage. The evaluation begins with the surgical team at HSS. Once surgery is scheduled, pre-surgical screening is completed and the discharge planning process is initiated; a home care referral to VNS Health typically takes place 2 weeks in advance of surgery.
VNS Health and HSS also prepare patients to adopt the right mindset about postoperative care, which can be confusing based on their previous understanding. For example, some patients who have spoken with people who had TJA procedures in the past may expect to be discharged to inpatient rehabilitation. When told they will be discharged directly home, they may express concern that they will be skipping an important step in recovery. Other patients who have spoken with TJA patients who went right home after surgery may be confused to learn that they will still need to participate in inpatient rehabilitation. By proactively preparing patients for rehabilitation and providing reassurance, VNS Health and HSS are taking steps to improve patient experience and satisfaction.
Translating Clinical Advancements Into Home Care Innovations
Minimally invasive surgeries, rapid recovery protocols for pain management, and implementation of new surgical and anesthesia techniques (eg, neuraxial anesthesia) have increased outpatient TJAs and shortened LOS at hospitals nationwide [17,18]. VNS Health and HSS constantly look for opportunities to maximize clinical advancements beyond the hospital setting. One of the greatest collaborations began in 2021, as it became commonplace for surgeons to perform minimally invasive procedures and seal outer wounds with surgical glue and atraumatic dressings, such as Mepilex, rather than traditional staples or stitches. Previously, dressings could be changed only by nursing home care staff. But with Mepilex, HSS staff could teach VNS Health’s physical therapists to safely remove dressings, thereby increasing efficiency.
Improving Interorganization Communication
VNS Health and HSS rely on frequent and thorough communication. The organizations share a secure, HIPAA-compliant transport layer security (TLS) tunnel for sharing patient information, which allows staff from both organizations to communicate easily and view critical data without delay.
Staff from VNS Health and the HSS Center for the Advancement of Value in Musculoskeletal Care hold weekly meetings to review all patients currently in their 2 weeks of home care and discuss barriers to discharge from home care. They also use these meetings to ensure that there is goal alignment between both organizations’ visions and values, as well as to develop and improve clinical pathways and performance. These meetings are invaluable for both organizations. For example, during past meetings, VNS Health and HSS collaborated on managing bundled payment programs on value-based care initiatives, contributing to millions of dollars in annual savings. They spread the application of value-based health care principles organization-wide, providing clinical and data-driven evidence to support and promote value in health care.
The 2 organizations also hold quarterly steering committee meetings, where leadership from both organizations share information, review key performance indicators, and discuss opportunities for clinical initiatives and collaboration.
Outcomes
Shortening LOS continues to be successful in lowering costs and maintaining or improving patient outcomes (Supplemental Figs. 3 and 4). As the average LOS decreased between 2014 and 2022, there were also improvements in outcome-based quality improvement metrics, including bed transferring, toilet transferring, ambulation, and hospital readmissions.
Research by HSS in 2015 found no difference in post-surgical complications among knee replacement patients who were discharged to inpatient rehabilitation vs discharged directly to home care [11]. The 2-year outcomes for function, pain, and patient improvement were also similar between the 2 groups.
Partnership During COVID-19
As with many projects, some of the greatest accomplishments are not anticipated at the onset. When New York became one of the nation’s COVID-19 epicenters in March 2020, VNS Health and HSS relied on their established framework of collaboration to take action to manage changes in hospital operations.
In the first few months of the pandemic, most elective orthopedic surgeries were postponed. HSS transitioned from being an orthopedic specialty hospital to an acute care facility, first serving orthopedic trauma cases and nonelective orthopedic surgeries to anyone who needed hospitalization with COVID-19 or other medical issues. During this time, VNS Health and HSS worked seamlessly and swiftly to optimize care—allowing hundreds of New Yorkers to receive acute medical care and safely transition to certified home health agency or hospice services.
VNS Health and HSS were also able to partner on other COVID-19 initiatives, such as making sure that home care workers across New York could receive vaccinations at HSS and VNS Health.
Elective TJAs rebounded relatively quickly, with numbers of cases reaching historic averages by June 2020 [2]. Since COVID-19 was still prevalent, hospitals were even more determined to send patients home rather than to inpatient facilities to conserve medical resources and decrease exposure to COVID-19. VNS Health and HSS were ahead of the game in this regard, as they had already achieved excellence in patient throughput and providing top-quality care at home.
The initiative to shorten LOS while maintaining and improving patient outcomes is far from complete; it likely will evolve along with the health care landscape. Yet within the past 12 years of working together, VNS Health and HSS have learned important lessons in innovative thinking, flexibility, preparation, communication, and teamwork that continue to contribute to shorter LOS and improve patient outcomes.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231205457 – Supplemental material for VNS Health and HSS Partner to Reduce Length of Stay After Total Joint Arthroplasty: Implications for Home Care Providers
Supplemental material, sj-docx-1-hss-10.1177_15563316231205457 for VNS Health and HSS Partner to Reduce Length of Stay After Total Joint Arthroplasty: Implications for Home Care Providers by Joseph Gallagher and Sandy Merlino in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316231205457 – Supplemental material for VNS Health and HSS Partner to Reduce Length of Stay After Total Joint Arthroplasty: Implications for Home Care Providers
Supplemental material, sj-docx-2-hss-10.1177_15563316231205457 for VNS Health and HSS Partner to Reduce Length of Stay After Total Joint Arthroplasty: Implications for Home Care Providers by Joseph Gallagher and Sandy Merlino in HSS Journal®
Supplemental Material
sj-pdf-3-hss-10.1177_15563316231205457 – Supplemental material for VNS Health and HSS Partner to Reduce Length of Stay After Total Joint Arthroplasty: Implications for Home Care Providers
Supplemental material, sj-pdf-3-hss-10.1177_15563316231205457 for VNS Health and HSS Partner to Reduce Length of Stay After Total Joint Arthroplasty: Implications for Home Care Providers by Joseph Gallagher and Sandy Merlino in HSS Journal®
Footnotes
Acknowledgements
The authors thank Samantha Gassel of CareContent, Inc., and Stephen Lee and Martha Schueneman of VNS Health for their contributions to the researching and writing of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: VNS Health paid CareContent, Inc., for the writing and research of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was not required for this commentary.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.