
Abstract
Background: Increasing demand for shoulder arthroplasty and an aging population may increase the rate of complications associated with advanced age such as postoperative delirium, but little is known on its burden in this cohort. Purpose: We sought to answer the following questions: (1) What is the epidemiology of postoperative delirium after shoulder arthroplasty? (2) What modifiable risk factors can be identified for postoperative delirium after shoulder arthroplasty? (3) Do risk factors differ in those younger than and in those older than 70 years of age? Methods: In a retrospective nationwide cohort study, we extracted data from the Premier Healthcare database on inpatient total and reverse shoulder arthroplasties from 2006 to 2016. The primary outcome was postoperative delirium; modifiable risk factors of interest were perioperative opioid use (high, medium, or low), peripheral nerve block use, and perioperative prescription medications. Mixed-effects models assessed associations between risk factors and postoperative delirium. Odds ratios and confidence intervals are reported. We applied a cutoff of 70 years of age because it was the median age of the cohort, as well as the age at which we observed that delirium prevalence increased. Results: A total of 92,429 total and reverse shoulder arthroplasties were identified (age range: 14–89 years). Overall delirium prevalence was 3.1% (n = 2909). Age-specific prevalence of postoperative delirium was lower in patients aged 50 to 70 years and higher in those aged 70 years and older, up to 8% among those older than 88 years. After adjusting for relevant covariates, only long-acting and combined short-acting and long-acting benzodiazepines (compared with no benzodiazepines) were associated with increased odds of postoperative delirium. Corticosteroids were associated with decreased odds of postoperative delirium. Conclusion: Our retrospective cohort study demonstrated that benzodiazepine use and older patient age were significantly associated with postoperative delirium in shoulder arthroplasty patients. The relationship between benzodiazepine use and delirium was particularly notable among those 70 years of age and older. Further investigation is indicated, given the known adverse effects of benzodiazepines in older adults and our findings of higher than expected use of these medications in this surgical cohort.
Introduction
One-third of surgeries in the United States are performed on people who are aged 65 years or older, and given our aging population, this percentage is expected to grow, increasing concern for age-specific complications such as postoperative delirium [2]. Postoperative delirium, an acute decline in cognitive function, is one of the most common surgical complications, occurring in an estimated 5% to 50% of elderly patients undergoing surgery; it is costly, is at times preventable, and may profoundly affect patients’ postoperative recovery [2,5,24,31].
Various factors—including unmodifiable factors such as advanced age and modifiable factors such as type of anesthesia or medications used such as benzodiazepines and some nonopioid analgesics—have been proposed as risk factors and been studied in the context of total hip or knee arthroplasty and hip fracture repair surgery [2,17,20]. Importantly, risk mitigation requires a focus on modifiable risk factors for postoperative delirium, such as the use of medications including benzodiazepines, gabapentinoids, ketamine, opioids, and neuraxial anesthesia [17,20]. To date, however, an extensive evaluation of the burden of postoperative delirium and related modifiable risk factors is not available for patients undergoing shoulder arthroplasty. Such an evaluation may provide useful information given the characteristics of this surgical population (eg, advanced age and comorbidities), different anesthetic approaches compared with other orthopedic surgeries, and the current trend toward outpatient shoulder arthroplasty in carefully selected patients [6]. Moreover, demand for shoulder arthroplasty is increasing [9].
Using national observational claims data from patients undergoing total and reverse shoulder arthroplasty, we aimed to study (1) the epidemiology of postoperative delirium and related (modifiable pharmacological) perioperative risk factors, (2) their impact on postoperative delirium, and (3) the difference, if any, between age groups, given the higher prevalence of postoperative delirium in older patients.
Methods
We conducted a retrospective cohort study using the applicable Strengthening the Reporting of Observational Studies in Epidemiology guidelines; it was approved as exempt by the institutional review board of our institution. Data were extracted from the nationwide Premier Healthcare database (Premier Inc, Charlotte, North Carolina), which contains detailed billing information on 20% to 25% of US hospitalizations [15,21]. The Premier Healthcare database is a “large, U.S. hospital-based, service-level, all-payer database that contains information on inpatient discharges, primarily from geographically diverse non-profit, nongovernmental and community and teaching hospitals and health systems from rural and urban areas” [21]. All inpatient total shoulder arthroplasty and reverse shoulder arthroplasty (TSA/RSA) procedures recorded in this data set from 2006 to 2016 were initially included in the study cohort. This was defined using International Classification of Diseases, Ninth Revision (ICD-9) codes for TSA (81.80) and RSA (81.88) [25,29]. A total of 92,429 cases were included after the following exclusion criteria were applied: unknown sex (n = 34), unknown discharge status (n = 109), emergency admission (patient required immediate medical intervention as a result of a severe, life threatening, or potentially disabling condition) (n = 732), outpatient procedure (n = 1199), and procedure performed at a hospital with fewer than 30 procedures during the study period (to ensure sufficient sample size per hospital; n = 2045). No patients were excluded on the basis of age.
An a priori analysis plan was made to identify main outcomes, exposures, and other variables of interest. Patients with postoperative delirium, the primary outcome, were identified by either ICD-9 codes for delirium (290.3, 293, 293.1, 780.09) or billing for antipsychotics (specifically haloperidol, olanzapine, and quetiapine), as previously described [11,17,20]. International Classification of Diseases, Ninth Revision codes were not used alone because delirium is often not diagnosed, but billing for antipsychotics provides another mechanism of identifying patients with delirium, as these medications are commonly used for this condition. This method was chosen based on previous research showing that using ICD diagnosis codes or antipsychotic billing to define delirium increases sensitivity with little change in specificity, as compared with using ICD diagnosis codes alone, antipsychotic billing alone, and ICD diagnosis and antipsychotic billing together [11].
Modifiable perioperative risk factors were extracted from those mentioned in the American Geriatrics Society best practice statement on postoperative delirium [2]. These included perioperative opioid use (defined as opioid use on the day of surgery [D0] or the day after surgery [D1], categorized into high, medium, or low), peripheral nerve block use, and the following medications prescribed on either D0 or D1: benzodiazepines (short-acting and long-acting, the latter including intermediate-acting), meperidine, nonbenzodiazepine (sedative) hypnotics, ketamine, corticosteroids, and gabapentinoids (Supplemental Table 1). Opioid use on D0 or D1 was derived from charges for opioids and was expressed in oral morphine equivalents, calculated using the Lexicomp “opioid agonist conversion” and the GlobalRPH “opioid analgesic converter” calculator [14,16]. This was then categorized into 3 groups using percentiles; cutoffs for low, medium, and high use were based on the below 25th (low), 25th to 75th (medium), and above 75th (high) percentiles.
Patient-specific variables were gathered from the Premier database and included age, sex, and race (white, black, other). Health care–specific variables included insurance used for procedure (commercial, Medicaid, Medicare, or self-pay—including uninsured or unknown), hospital location (rural, urban), hospital bed size (below 300, 300–499, 500 or more beds), hospital teaching status, and hospital-specific volume of annual shoulder arthroplasties. Procedure-specific variables included year of procedure, admission type (elective, nonelective), surgery type (RSA or TSA), use of nonopioid analgesics not listed above (including nonsteroidal anti-inflammatory drugs, cyclooxygenase-2 inhibitors, and acetaminophen). Nonelective admission occurs when the first-available treatment is necessary but the patient does not meet the criteria for an emergency admission. In an elective admission, the patient can schedule surgery at their convenience. Comorbidity burden, including dementia, was determined using the Quan adaptation of the Charlson-Deyo comorbidity index [22]. History of substance use disorder, chronic pain conditions, and psychiatric conditions were also included as covariates as they may influence opioid use. These were defined using ICD-9 diagnosis codes, as previously described [12].
First, the general epidemiology of postoperative delirium in this surgical cohort was assessed through age-specific prevalence estimates (ie, the prevalence of delirium for each age in the cohort) and delirium prevalence stratified by all study variables. In addition, trends in prevalence of all candidate risk factors were graphed to assess the influence of changes over time on our multivariable models. Given the large sample size, group differences in our univariable analysis (comparing those with and without delirium) were assessed by applying standardized differences. Here, a standardized difference of 0.1 (or 10%) indicates a meaningful difference [4,30]. Second, mixed-effects (multivariable) models assessed associations between the (perioperative) risk factors of interest and postoperative delirium. Third, given the higher prevalence of postoperative delirium in older age groups, we performed the same multivariable analysis in a younger and older age groups by applying an interaction term to variables of interest. Here, a cutoff of 70 years was applied as this was the median as well as the age after which delirium risk started increasing. All available variables (as described above) were included in our multivariable models. For the multivariable analysis, adjusted odds ratios (ORs) and Bonferroni-adjusted confidence intervals (CIs) with P values are reported, considering the number of hypotheses tested for in the main analyses (27 hypotheses), thus reducing the risk of type I errors (false-positive associations). However, this step may increase the likelihood of type II errors (false-negative associations) [19]. For all models, PROC GLIMMIX in SAS v9.4 statistical software was used.
The following post hoc sensitivity analyses were performed to reduce or assess for the potential risk of misclassification bias and to increase the robustness of the algorithm used to extract cases of delirium:
Varying the definition of delirium. Here, delirium was defined using ICD-9 diagnosis codes, thus removing all cases that were identified by billing codes for delirium-related medications. Furthermore, the cohort was restricted only to hospitals that used ICD-9 codes for the identification of delirium, under the assumption that in those hospitals potential underreporting of delirium may be less pronounced.
Specifically adjusting for dementia. Given the likely strong association between dementia and delirium, dementia was removed from the Charlson-Deyo comorbidity index and added as a distinct covariate to account for potential bias.
Adding a graph demonstrating age-specific use of benzodiazepines.
Results
Among the 92,429 TSA/RSA procedures (age range: 14–89 years) included in our analysis, the prevalence of postoperative delirium was 3.1% (n = 2909). When evaluating age-specific risks (Fig. 1), we observed a decreasing trend in patients younger than 70 years and an increasing trend in patients 70 years and older, with the age-specific prevalence reaching 8% for the oldest patients. While the rate of delirium increased at age 70, benzodiazepine use decreased at around the same age, but remained above 50% across all ages (Fig. 2). Regarding medication use over time (Fig. 3a-–d), pronounced trends were seen for peripheral nerve blocks (increasing trend), gabapentinoids (increasing trend), meperidine (decreasing trend), hypnotics (decreasing trend), corticosteroids (decreasing trend), ketamine (decreasing trend), and opioid use (decreasing trend). Interestingly, fewer clear trends were observed for benzodiazepines, with a high baseline use of short-acting benzodiazepines. In our study, 83.2% (n = 79,936) of patients received some form of benzodiazepines.
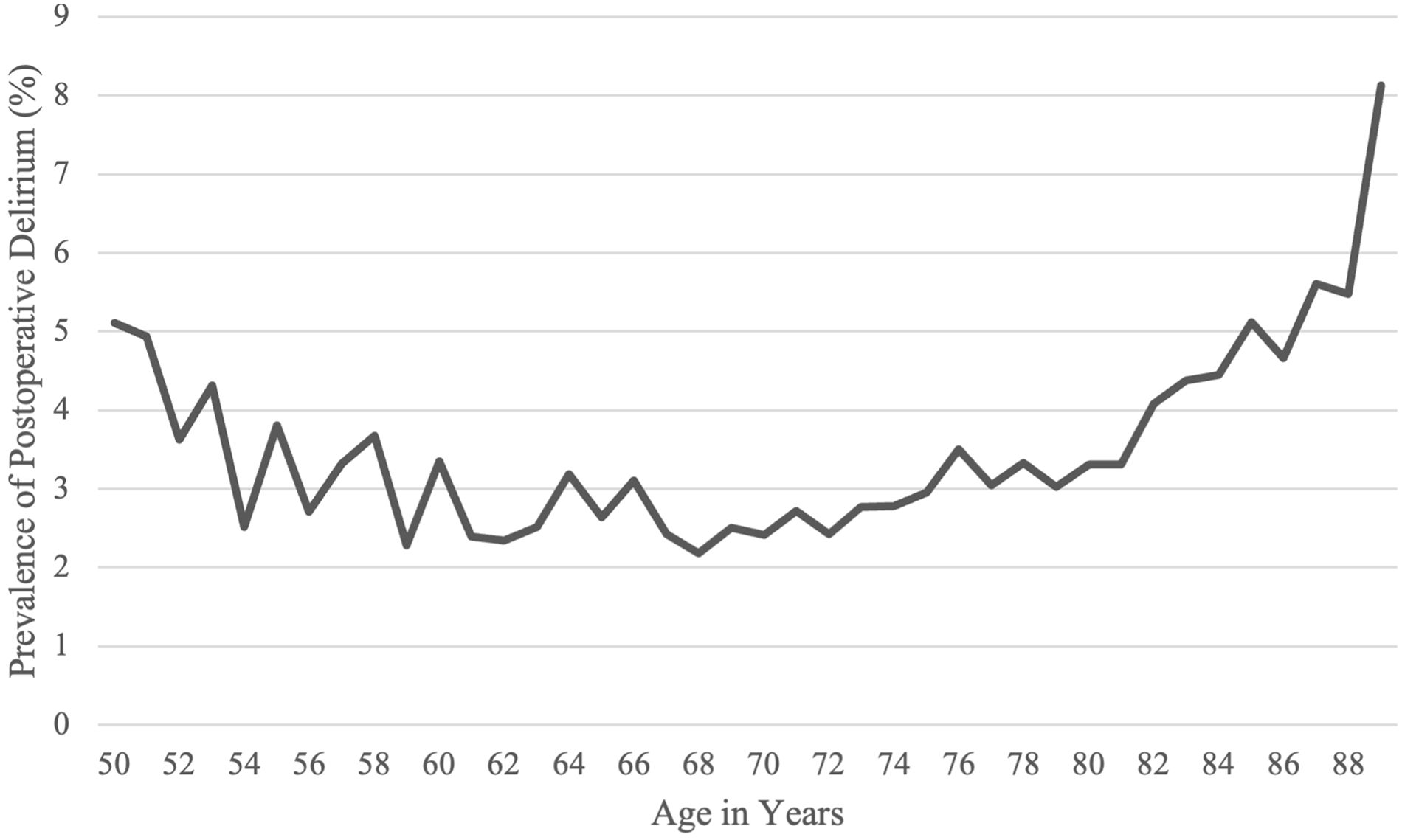
The graph shows age-specific prevalence of postoperative delirium.
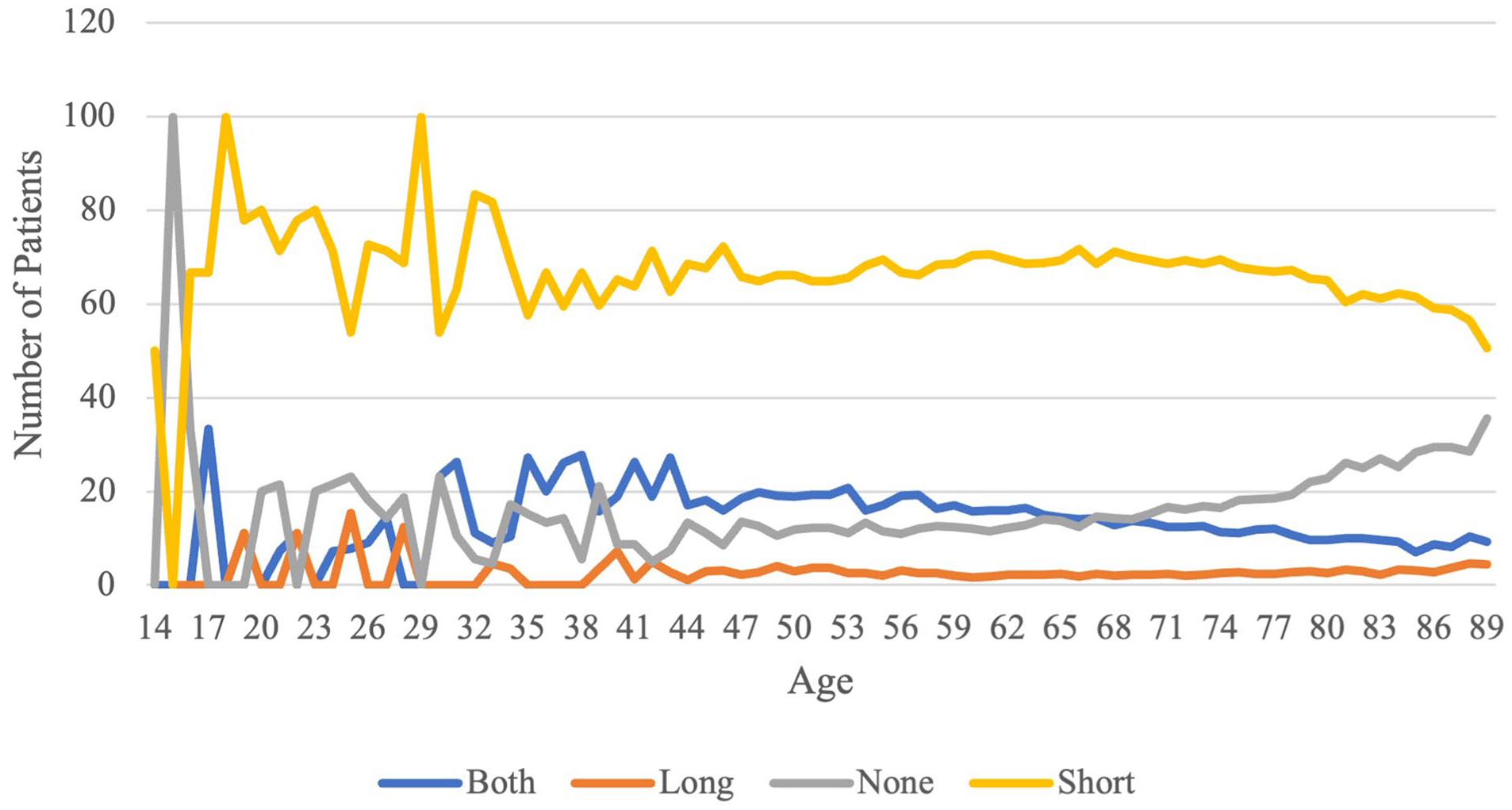
The graph shows age-specific rates of benzodiazepine use.
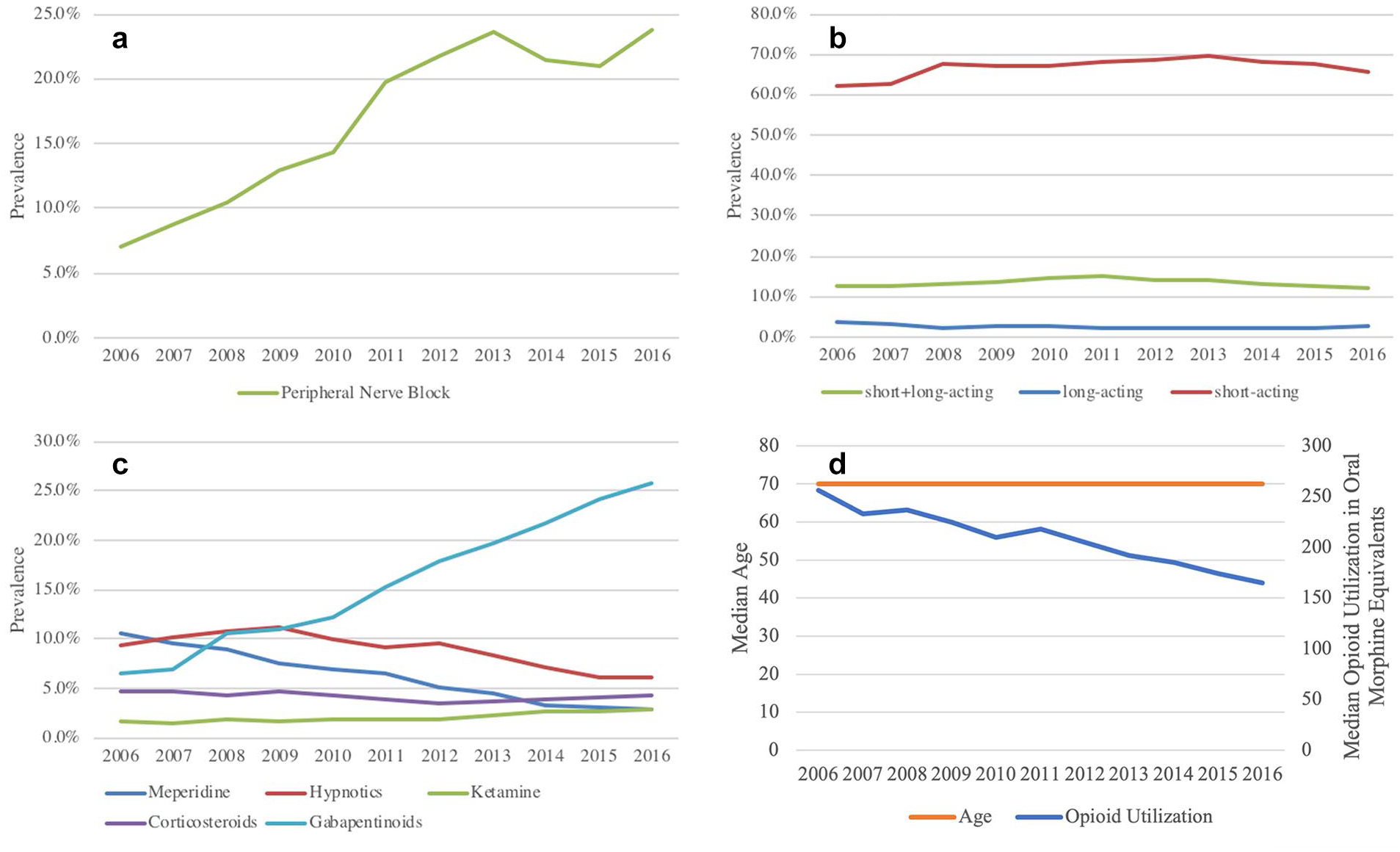
The graphs show trends of the following exposures of interest: (a) use of a peripheral nerve block, (b) use of benzodiazepines, (c) use of meperidine, hypnotics, ketamine, corticosteroids, and gabapentinoids, and (d) median age and median opioid utilization.
In the univariable analysis, higher postoperative delirium risks were seen in female patients (3.6%), those on Medicaid (5.5%), those treated in large (3.8%) and teaching (3.7%) hospitals, those with a nonelective admission (6.1%), those undergoing TSA (3.9%), those receiving long-acting benzodiazepines (both alone and in combination with short-acting benzodiazepines, prevalence up to 8.8%), those receiving either gabapentinoids (3.9%) or acetaminophen (3.9%), and those with a higher comorbidity burden (up to 8%), all with standard differences >0.1 (Supplemental Table 2).
After adjustment for relevant covariates in the multivariable analysis, increased odds for postoperative delirium were seen for older age (OR = 1.01, 99.82% CI = 1.00–1.02; P < .0001), long-acting benzodiazepine use (OR = 2.24, 99.82% CI = 1.67–2.99; P < .0001), and combined use of short-acting and long-acting benzodiazepines (OR = 1.87, 99.82% CI = 1.51–2.32; P < .0001). Decreased odds for postoperative delirium were seen for corticosteroid use (OR = 0.72, 99.82% CI = 0.53–0.99; P = .0013). No significant associations were seen in other remaining risk factors of interest (Table 1; Supplemental Table 3). When stratifying by age, the effect of benzodiazepines remained significant in both groups. Only long-acting benzodiazepines (<70 years: OR = 2.30, 99.82% CI = 1.41–3.75; ≥70 years: OR = 2.23, 99.82% CI = 1.54–3.21; P < .0001) and combined use of short-acting and long-acting benzodiazepines (<70 years: OR = 2.03, 99.82% CI = 1.42–2.91; ≥70 years: OR = 1.72; 99.82% CI = 1.31–2.24; P < .0001) were significant. When stratifying by age, gabapentinoids significantly increased the odds for postoperative delirium in those younger than 70 years (OR = 1.29, 99.82% CI = 1.05–1.59; P = .0002). The use of corticosteroids was not significant for either age group (P = .0400): age younger than 70 years (OR = 0.74; 99.82% CI = 0.47–1.17) or age 70 years or older (OR = 0.70, 99.82% CI = 0.46–1.08; Table 2 and Supplemental Table 4).
Results from multivariable models; odds ratios depicting effect estimates for the postoperative delirium risk factors of interest.
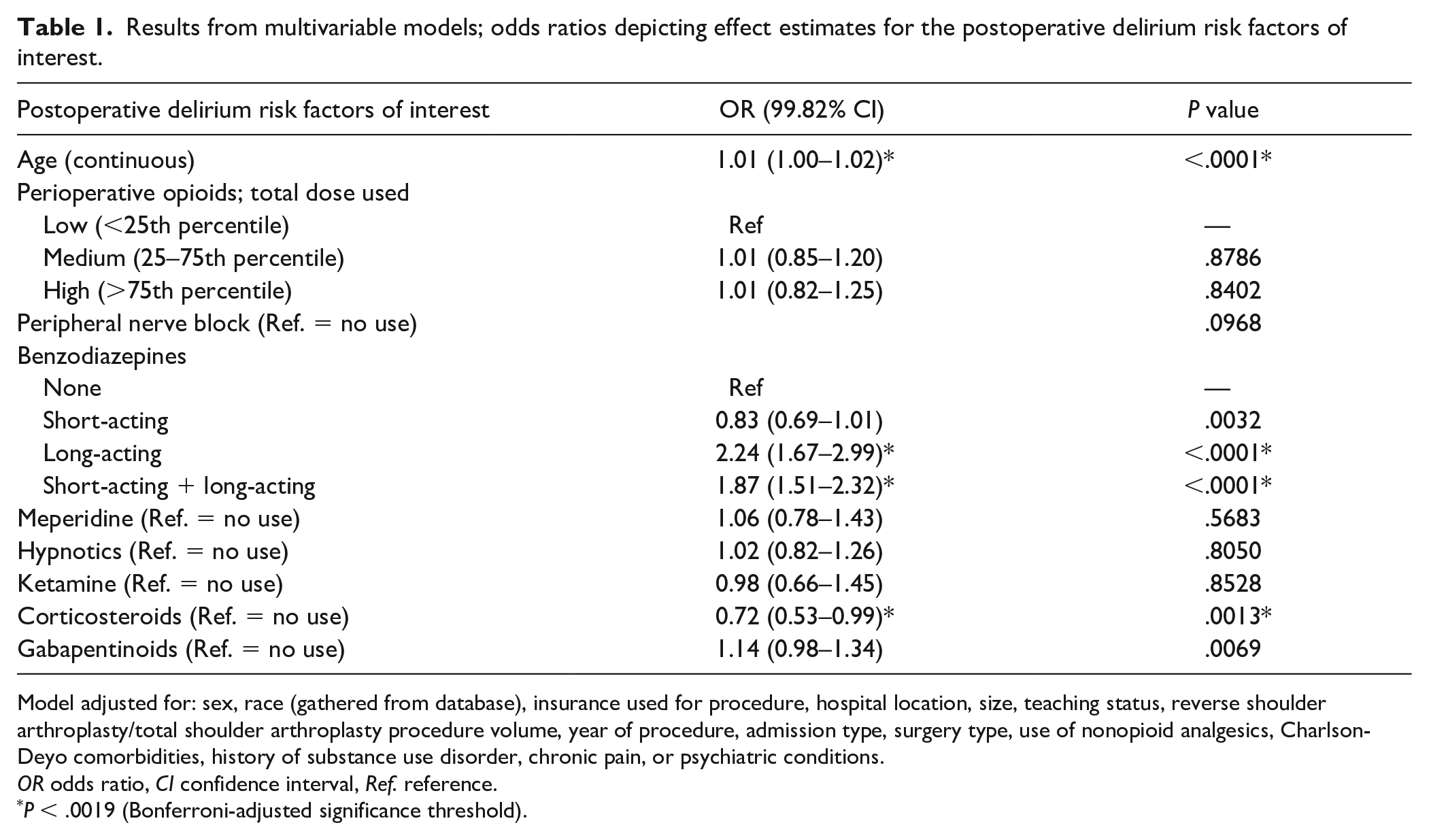
Model adjusted for: sex, race (gathered from database), insurance used for procedure, hospital location, size, teaching status, reverse shoulder arthroplasty/total shoulder arthroplasty procedure volume, year of procedure, admission type, surgery type, use of nonopioid analgesics, Charlson-Deyo comorbidities, history of substance use disorder, chronic pain, or psychiatric conditions.
OR odds ratio, CI confidence interval, Ref. reference.
P < .0019 (Bonferroni-adjusted significance threshold).
Results from multivariable models with separate effect estimates per age group; odds ratios depicting effect estimates for the postoperative delirium risk factors of interest.
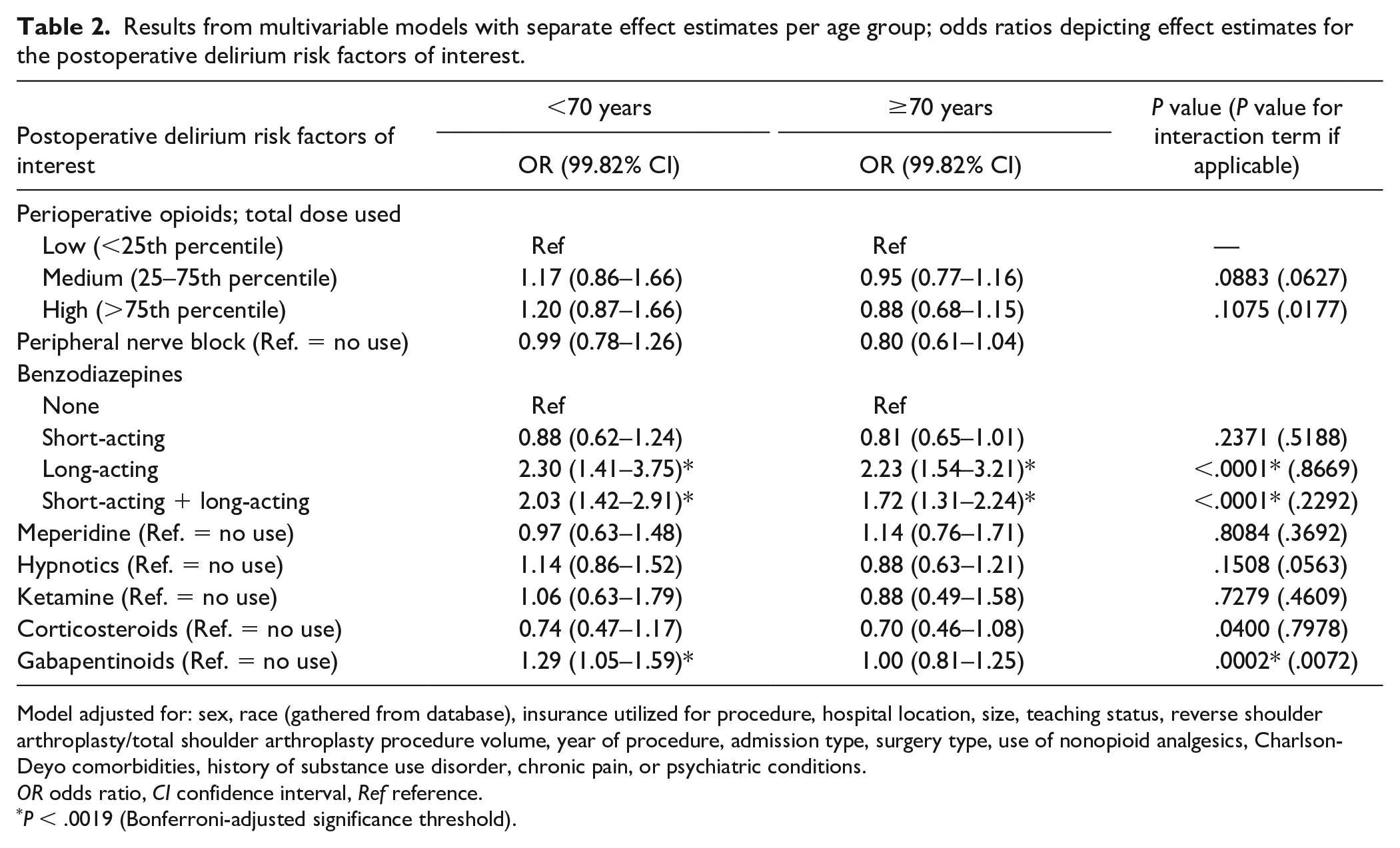
Model adjusted for: sex, race (gathered from database), insurance utilized for procedure, hospital location, size, teaching status, reverse shoulder arthroplasty/total shoulder arthroplasty procedure volume, year of procedure, admission type, surgery type, use of nonopioid analgesics, Charlson-Deyo comorbidities, history of substance use disorder, chronic pain, or psychiatric conditions.
OR odds ratio, CI confidence interval, Ref reference.
P < .0019 (Bonferroni-adjusted significance threshold).
The various sensitivity analyses did not alter our main conclusions (Supplemental Tables 5 and 6).
Discussion
In this retrospective cohort study of 92,429 TSA and RSA procedures, we observed a postoperative delirium prevalence of 3.1%, with age-specific trends in those younger than 70 years than in those 70 years or older, without a clear plateau. Postoperative delirium was associated with the use of long-acting benzodiazepines and combined use of short-acting and long-acting benzodiazepines. Interestingly, the use of benzodiazepines stayed relatively stable over time, and there was high baseline use of specifically short-acting benzodiazepines.
This study has limitations. First, given the observational nature of the methods, we can infer only associations and not causation. Second, delirium in this study is defined by ICD codes and billing codes for antipsychotics; thus, clinical information about delirium timing, severity, and subtype (hypoactive vs hyperactive) was not accessible. This reflects challenges in clinical practice; there is no standardized screening for delirium and cases may not be recognized [2,7,20]. While the rate of delirium in our study is in the range found in shoulder arthroplasty and in hip and knee arthroplasty (<1–14%), this limitation applies to most retrospective research on postoperative delirium, suggesting that the research likely underestimates its prevalence [11,17,18]. Nevertheless, to improve the sensitivity and specificity of delirium detection, we performed multiple sensitivity analyses to eliminate potential confounders. Third, billing for ketamine, opioids, and benzodiazepines might not equate to actual administration. However, this misclassification bias should be independent of delirium prevalence, and given the short timeframe investigated (within 48 hours of surgery), we believe this should be closely linked. Finally, this research focused on a subset of medications, primarily given postoperatively, and additional research is needed to isolate the effects of intraoperative anesthetics in patients undergoing shoulder arthroplasty.
The literature on postoperative delirium has reported a wide range of prevalence (between 3% and 50%) in older patients undergoing various surgical procedures [3,17]. For example, in lower extremity total joint arthroplasties, the prevalence of postoperative delirium has been reported to range from 2.6% to as high as 14.3% [17,18]. Given the higher median age of patients undergoing shoulder arthroplasty (compared with lower extremity joint arthroplasty), we were surprised to find a lower delirium prevalence in the current study. Much of the postoperative delirium literature focuses on outcomes after hip fracture repair [1,26]. A lower rate of delirium may be seen in the TSA and RSA population, as may lower rates of known risk factors for postoperative delirium including transfusions, intensive care unit admissions, and poor preoperative health [13,27].
Few studies have directly addressed the burden of postoperative delirium in patients undergoing TSA/RSA. One study assessing the impact of depression on outcomes after shoulder arthroplasty found a link between depression and postoperative delirium but in a cohort with a less than 1% prevalence of delirium [18]. While the prevalence of 3.1% found in our study may be a more accurate burden (as we did not rely solely on ICD codes but also used proxies such as billing for antipsychotics), this still may reflect an underestimation, as there is no universal screening for postoperative delirium after shoulder arthroplasty, and hypoactive delirium in particular may be easily overlooked [11,17,20]. Future studies should focus on the utility of screening in certain high-risk groups given the aging surgical population and growing demand for TSA/RSA [9].
Our analysis indicated a sharp increase in postoperative delirium in patients aged 70 years and older, reaching up to 8% without a clear plateau. This finding suggests the potential benefit of risk-reduction strategies in older patients targeting polypharmacy, the use of high-risk drugs, and underlying impaired cognition [2,3,20].
While we studied various risk factors, the most consistent association was seen for the use of long-acting benzodiazepines and combined use of short-acting and long-acting benzodiazepines with increased odds of postoperative delirium, an association that has been noted in lower extremity arthroplasty [17,20]. Notably, given the age composition of this surgical cohort, the majority of patients received some form of benzodiazepines. The use of benzodiazepines in elderly patients is surprising, given the known risk of benzodiazepine use in the elderly. Benzodiazepine use—regardless of short or long half-life—has been linked to an increased risk of falls, hip fracture, and cognitive impairment; thus, the association with postoperative delirium is of particular importance [3,8]. Indeed, the 2019 edition of the American Geriatrics Society Beers Criteria for Potentially Inappropriate Medication Use in Older Adults recommends that benzodiazepines be avoided in elderly patients [2,3]. This contrasts with our findings of a relatively high use of specifically short-acting benzodiazepines in this surgical cohort with no clear trend in decreasing use over time. While there is a slow decrease with age beginning around age 70, the rate continues to remain above 50%. Given the stated recommendation, this finding deserves additional study, specifically focusing on indications and characterization of prescribing patterns in this elderly surgical population and the effects of preoperative benzodiazepine use. The use of long-acting benzodiazepines in this surgical cohort requires further scrutiny, using data sources with more information on potential indications.
The association of long-acting benzodiazepines and combined short-acting and long-acting benzodiazepines with increased odds of postoperative delirium is present in both age groups. Benzodiazepine use among all patients should be monitored in those undergoing for shoulder arthroplasty. Rate of benzodiazepine use slowly decreases beginning at age 70, and this may contribute to the difference in risk factors in the 2 groups. In contrast, patients aged 70 years and older showed a sharp increase in age-specific delirium risk, possibly due to higher baseline risks of polypharmacy and underlying impaired cognition. Therefore, while reducing benzodiazepine use in patients over 70 years of age is necessary and in line with American Geriatric Society guidelines, additional interventions are likely needed to reduce postoperative delirium [2,3,20].
Of note, perioperative opioid use on D0 or D1 (irrespective of dose) was not associated with increased risk of postoperative delirium. This finding supports prior research that found no association between use of any postoperative opioids and delirium [26]. Yet, it has been shown that, for example, people with dementia receive lower doses of opioids postoperatively, possibly due to the concern that this will increase their risk of postoperative delirium [1,26]. Judicious opioid use is important, as are concerns about postoperative pain management.
Our findings may inform surgical practice on the need for preoperative risk stratification and screening, specifically among certain patients. Such preoperative risk stratification and screening strategies have been shown to result in significant decreases in postoperative complications, including delirium, in a total knee arthroplasty study population [23]. Policy shifts may incentivize increased risk stratification in shoulder arthroplasty patients, including bundled payments and outpatient surgery [10,28]. In the former, screening and risk stratification would be beneficial in earlier recognition and subsequent intervention to minimize patient harm and health care expenditures; in the latter, screening strategies could aid in candidate selection for either inpatient or outpatient shoulder arthroplasty. Such policies further emphasize the continued need for research, including prospective clinical studies, in testing the utility of screening and risk stratification strategies in clinical practice.
In conclusion, our retrospective cohort study using a national database suggests that benzodiazepine use and increasing patient age are significantly associated with postoperative delirium in shoulder arthroplasty patients. Moreover, benzodiazepine use was common even in the oldest patients in our study. In addition, we found an inflection point at 70 years of age where age-specific delirium prevalence sharply increased. Our findings suggest that future studies are needed on the utility of preoperative risk screening and stratification in mitigating risk of postoperative delirium in shoulder arthroplasty patients.
Supplemental Material
sj-docx-1-hss-10.1177_15563316221134244 – Supplemental material for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study
Supplemental material, sj-docx-1-hss-10.1177_15563316221134244 for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study by Sara N. Kiani, Samuel Z. Maron, Manasa G. Rao, Nicole Zubizarreta, Madhu Mazumdar, Leesa M. Galatz, Jashvant Poeran and Paul J. Cagle in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-2-hss-10.1177_15563316221134244 – Supplemental material for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study
Supplemental material, sj-docx-2-hss-10.1177_15563316221134244 for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study by Sara N. Kiani, Samuel Z. Maron, Manasa G. Rao, Nicole Zubizarreta, Madhu Mazumdar, Leesa M. Galatz, Jashvant Poeran and Paul J. Cagle in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-3-hss-10.1177_15563316221134244 – Supplemental material for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study
Supplemental material, sj-docx-3-hss-10.1177_15563316221134244 for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study by Sara N. Kiani, Samuel Z. Maron, Manasa G. Rao, Nicole Zubizarreta, Madhu Mazumdar, Leesa M. Galatz, Jashvant Poeran and Paul J. Cagle in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-4-hss-10.1177_15563316221134244 – Supplemental material for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study
Supplemental material, sj-docx-4-hss-10.1177_15563316221134244 for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study by Sara N. Kiani, Samuel Z. Maron, Manasa G. Rao, Nicole Zubizarreta, Madhu Mazumdar, Leesa M. Galatz, Jashvant Poeran and Paul J. Cagle in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-5-hss-10.1177_15563316221134244 – Supplemental material for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study
Supplemental material, sj-docx-5-hss-10.1177_15563316221134244 for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study by Sara N. Kiani, Samuel Z. Maron, Manasa G. Rao, Nicole Zubizarreta, Madhu Mazumdar, Leesa M. Galatz, Jashvant Poeran and Paul J. Cagle in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-6-hss-10.1177_15563316221134244 – Supplemental material for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study
Supplemental material, sj-docx-6-hss-10.1177_15563316221134244 for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study by Sara N. Kiani, Samuel Z. Maron, Manasa G. Rao, Nicole Zubizarreta, Madhu Mazumdar, Leesa M. Galatz, Jashvant Poeran and Paul J. Cagle in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-7-hss-10.1177_15563316221134244 – Supplemental material for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study
Supplemental material, sj-docx-7-hss-10.1177_15563316221134244 for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study by Sara N. Kiani, Samuel Z. Maron, Manasa G. Rao, Nicole Zubizarreta, Madhu Mazumdar, Leesa M. Galatz, Jashvant Poeran and Paul J. Cagle in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-8-hss-10.1177_15563316221134244 – Supplemental material for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study
Supplemental material, sj-docx-8-hss-10.1177_15563316221134244 for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study by Sara N. Kiani, Samuel Z. Maron, Manasa G. Rao, Nicole Zubizarreta, Madhu Mazumdar, Leesa M. Galatz, Jashvant Poeran and Paul J. Cagle in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-9-hss-10.1177_15563316221134244 – Supplemental material for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study
Supplemental material, sj-docx-9-hss-10.1177_15563316221134244 for The Burden of Postoperative Delirium After Shoulder Arthroplasty and Modifiable Pharmacological Perioperative Risk Factors: A Retrospective Nationwide Cohort Study by Sara N. Kiani, Samuel Z. Maron, Manasa G. Rao, Nicole Zubizarreta, Madhu Mazumdar, Leesa M. Galatz, Jashvant Poeran and Paul J. Cagle in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Paul J. Cagle, MD, declares relationships with Stryker and Johnson & Johnson. The other authors declare no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived for all patients included in this study.
Level of Evidence
Level IV, retrospective prognostic study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
CME Credit
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.