
Abstract
Background: The United States accounts for the majority of prescription opioids consumed worldwide. Recent literature has focused on opioid prescribing patterns among orthopedic surgeons; however, public and patient expectations about postoperative opioid use remain understudied. Purpose: We sought to explore public perceptions of opioid use after elective orthopedic surgery. Methods: We posted a 32-question survey on Amazon Mechanical Turk (MTurk), an online platform with over 500,000 unique registered users that is a validated tool for collecting survey responses in medical research. The survey asked about attitudes regarding opioid use after elective orthopedic surgery and sociodemographic factors, as well as validated assessments of health literacy and patient engagement. Results: Of 727 respondents who completed surveys, nearly half (46%) said they would prefer nonopioid pain medication after elective orthopedic surgery, although 86% said they would expect to be prescribed opioids for 1 week to 1 month postoperatively. About half said they would expect to be prescribed extra opioid medication in case of unexpected pain following surgery, and 50% reported that they would save their pills to treat future pain. Approximately 63% said they would understand their surgeon’s opioid weaning, but over ⅓ said weaning would lead to decreased satisfaction with their surgeon. Roughly ⅔ reported that pain control after surgery would directly affect their opinion of the surgeon. Conclusions: Our survey found that some members of the general public reported expectations regarding postoperative opioid prescribing that could lead to decreased patient satisfaction. These findings suggest the need for further research on the value of preoperative patient education in pain management, on patient expectations of pain control after elective surgery, and on the use of opioids following orthopedic surgery.
Introduction
Over the past two decades, the opioid epidemic has been widely discussed in both the scientific literature and the news media [18]. The introduction of the pain as “the fifth vital sign” in 1995 led to pain relief becoming a proxy for inpatient patient satisfaction; this, ultimately, influenced hospital reimbursement rates [5]. This spurred an increased focus on pain control strategies both in hospital and outpatient settings as well as a subsequent rise in opioid consumption [54]. Today, the United States consumes the vast majority of the world’s opioids; its rate of consumption per day is nearly 40% higher than that of the world’s second highest consumers [21]. In 2009, orthopedic surgeons accounted for the third highest prescription rates of opioid analgesics among all physicians [39,50]. A 2020 review of opioid prescribing for Medicare beneficiaries indicated that orthopedic surgeons remained among the highest prescribers of opioids in surgical specialties [44]. As a result, orthopedic surgeons, anesthesiologists, and pain medicine specialists have scrutinized their role in this public health issue.
Substantial literature has focused on quantifying the scope of this problem [11,29,50], identifying risk factors for chronic opioid use [15,17] and decreasing opioid use via multimodal pain regimens [13,19,24]. While many of the latter studies include patient-reported outcomes such as postoperative pain and function scores, they do not explore patients’ expectations of pain management.
Numerous public opinion polls have been published regarding opioid misuse and addiction [10]. Up to 54% of people nationally know someone who has suffered from opioid addiction, and 20% to 25% of Americans report knowing someone who has died as a result of prescription opioid use [10]. However, it is also important to consider public expectations about opioid use for routine postoperative pain control. There may be a stark contrast between the public perception of these medications and expectations regarding their use in a routine clinical setting. While there is ample data on mostly negative public perceptions that surround opioid addiction and misuse, opioids remain a mainstay in postoperative pain management. So it is important to seek and understand attitudes toward postoperative pain management.
We decided to examine public perceptions of prescription opioid use after elective orthopedic surgery through a survey posted on the Amazon Mechanical Turk platform, which has gained popularity as a source of data acquisition in medical research, including orthopedic surgery [22,30,34,37,42]. We hypothesized that the majority of respondents would prefer not to use opioid pain medications following surgery but would still expect their surgeon to prescribe them. We also hypothesized that the majority of respondents would be amenable to efforts to wean them off opioids in the postoperative period.
Methods
We constructed a 32-question electronic survey to assess public perceptions of opioid use after elective orthopedic surgery using Qualtrics XM. The survey was posted on Amazon Mechanical Turk (MTurk), a web-based platform where individuals or businesses can crowdsource virtual tasks (such as survey participation) to registered users, who receive compensation for completion [30]. The MTurk platform consists of over 500,000 unique users worldwide, with many residing in the United States [40]. Upon survey completion, unique codes are generated to verify individual completion and ensure actual user responses. Data acquired with MTurk have been demonstrated to have high levels of internal consistency, strong test–retest reliability, metric equivalence/invariance across samples, and is generalizable to the overall US population [9]. MTurk has been proven to be an efficient, reliable, and cost-effective tool for collecting survey responses in medical research comparable to those collected through conventional means [30].
We recruited participants from all MTurk users residing in the United States. This included adults 18 years of age or older with a valid social security number, as these are the requirements for MTurk membership. Each respondent was awarded $0.10 for completing the survey. Incomplete surveys and survey respondents with a duplicate Internet Protocol (IP) address were excluded. This survey did not use protected health information and therefore did not require Institutional Review Board (IRB) review.
Demographic characteristics were gathered, including age, sex, native language, race, location (United States region), marital status, education level, employment in healthcare, annual income, primary health insurance, and overall perceived health status. We evaluated health literacy using the single health literacy screening question [53] and patient engagement using the single health confidence question [51].
Statistical Analysis
Regression analysis was performed to evaluate respondent characteristics associated with expectations of no pain after surgery and resistance to weaning efforts by their surgeon. First, univariate analysis was performed using logistic regression, and any covariate that had an association (p < .2) was then included in multivariable logistic regression analyses. This was used to identify characteristics significantly associated with the beliefs they should have no pain postoperatively and that they would be resistant to weaning efforts. This model adjusted for age, sex, geographical region, education, income, insurance type, level of health literacy, health efficacy, smoking status, history of illicit drug use, and history of taking prescription opioids. These results are presented as adjusted odds ratios (ORs) with 95% confidence intervals (CIs). Statistical significance was defined as P < .05. All statistical analysis was performed on SPSS Statistics Software.
Results
In total, 727 participants completed surveys that were included in the analysis. Complete demographic data of the sample population including US Census data for comparison is shown in Table 1. Nearly all participants were age 60 years or younger. Our sample included more smokers than is representative of the US population (30% vs 14%). In addition, 42% reported history of illicit drug use, which is similar to the 39.1% of adults aged 18–25 alone who have reported use of any illicit drug [41]. The sociodemographic status of our sample was representative of that of the US population, though our sample was marginally wealthier [47]. While ¼ of our respondents reported limited health literacy, overall, they achieved more advanced degrees than the US population [46]. In addition, ¼ of our respondents also described themselves as healthcare workers, whereas only 14% of the US population reports the same [45]. More respondents had public health insurance plans (ie Medicare, Medicaid, Veterans Affairs) than the US population [47].
Survey participant characteristics (n = 727).
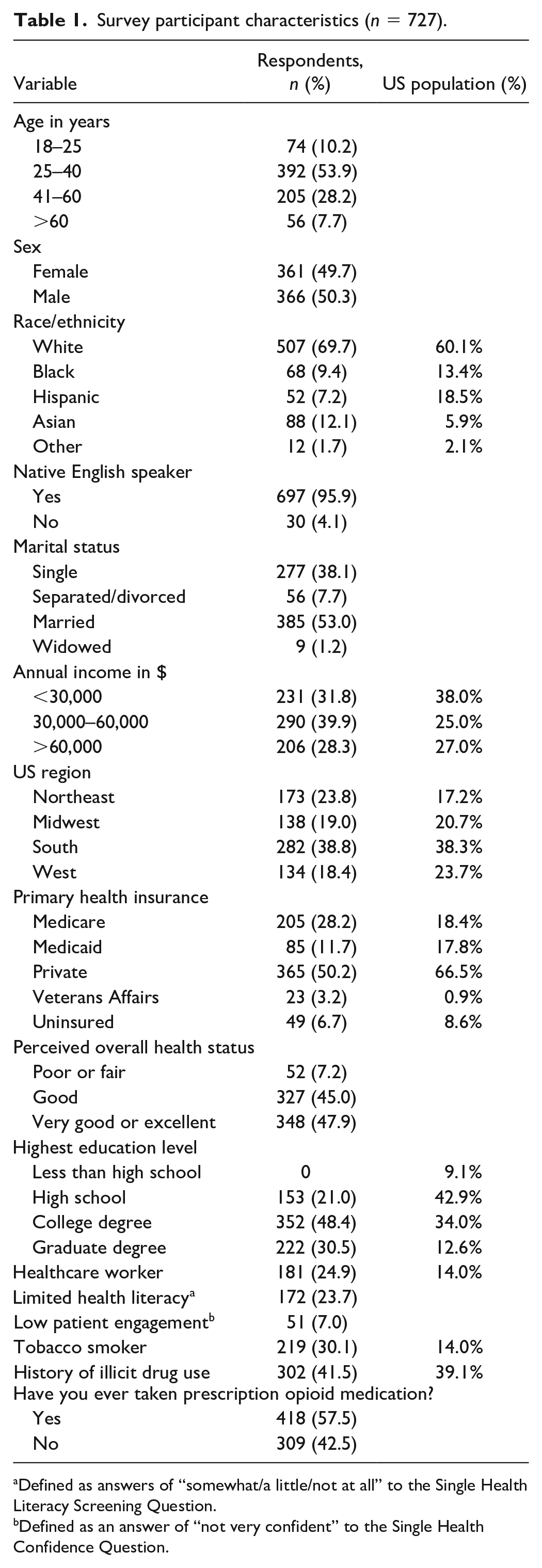
Defined as answers of “somewhat/a little/not at all” to the Single Health Literacy Screening Question.
Defined as an answer of “not very confident” to the Single Health Confidence Question.
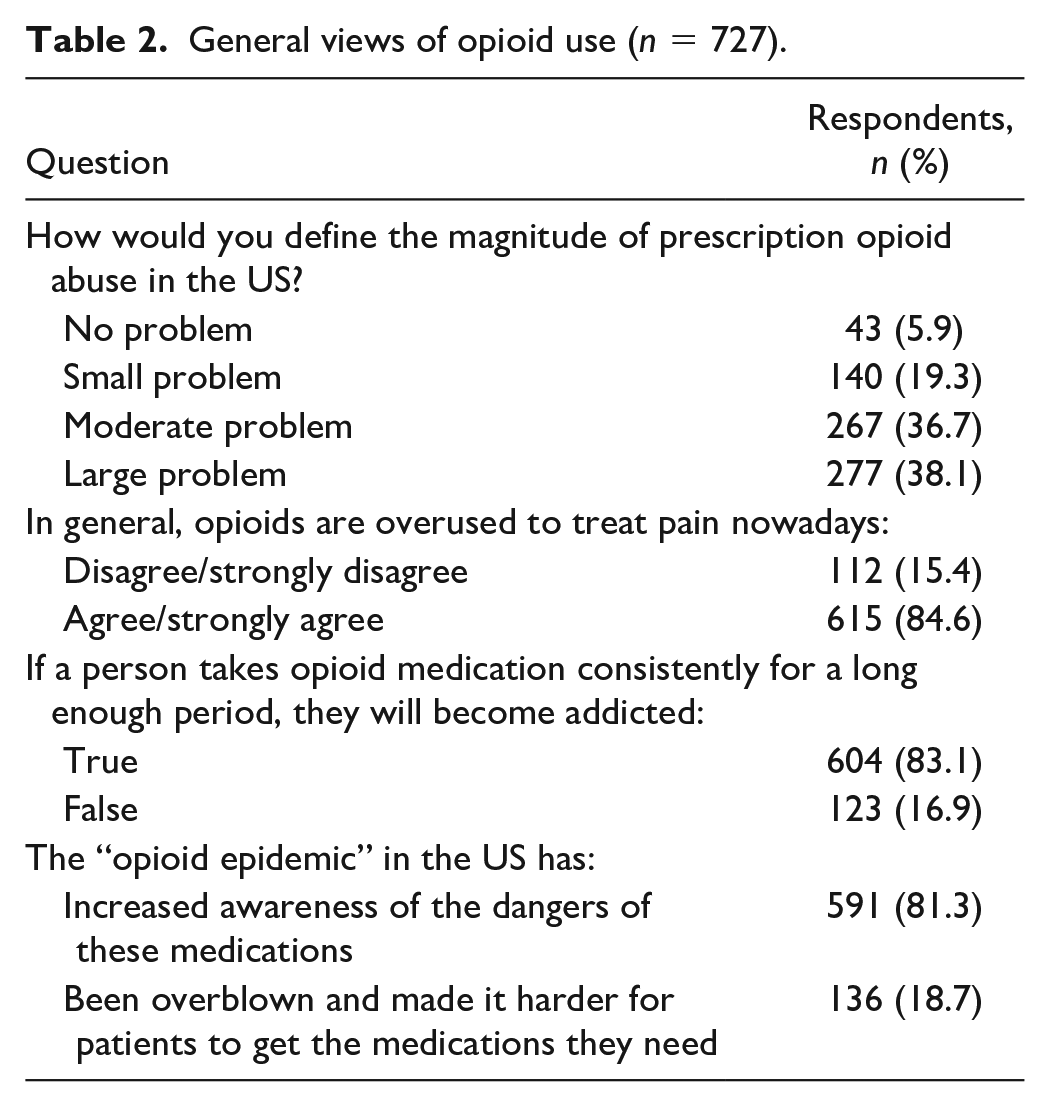
Nearly, 75% of participants defined the magnitude of prescription opioid misuse in the United States as a moderate or large problem (Table 2). Over 80% of respondents said they believe opioids are overused to treat pain.
General views of opioid use (n = 727).
A small portion (13%) of respondents said they would expect to have no pain after surgery, while the majority (87%) would expect some degree of pain after surgery, even with pain medication (Table 3). Multivariable regression analysis identified tobacco use (OR 1.91; 95% CI 1.17–3.13; P = .010) and Northeast region (OR 1.80; 95% CI 1.09–2.96; P = .021) as significantly associated with the expectation that patients should have no pain after surgery. However, people with private insurance (OR 0.483; 95% CI 0.30–0.78, P = .003), low health efficacy (OR 0.546, 95% CI 0.35–0.86, P = .009) and those with history of prescription opioid use (OR 0.45, 95% CI 0.28–0.73, P < .001) were significantly associated with expectations that they will have some pain after surgery.
Postoperative expectations related to pain control (n = 727).
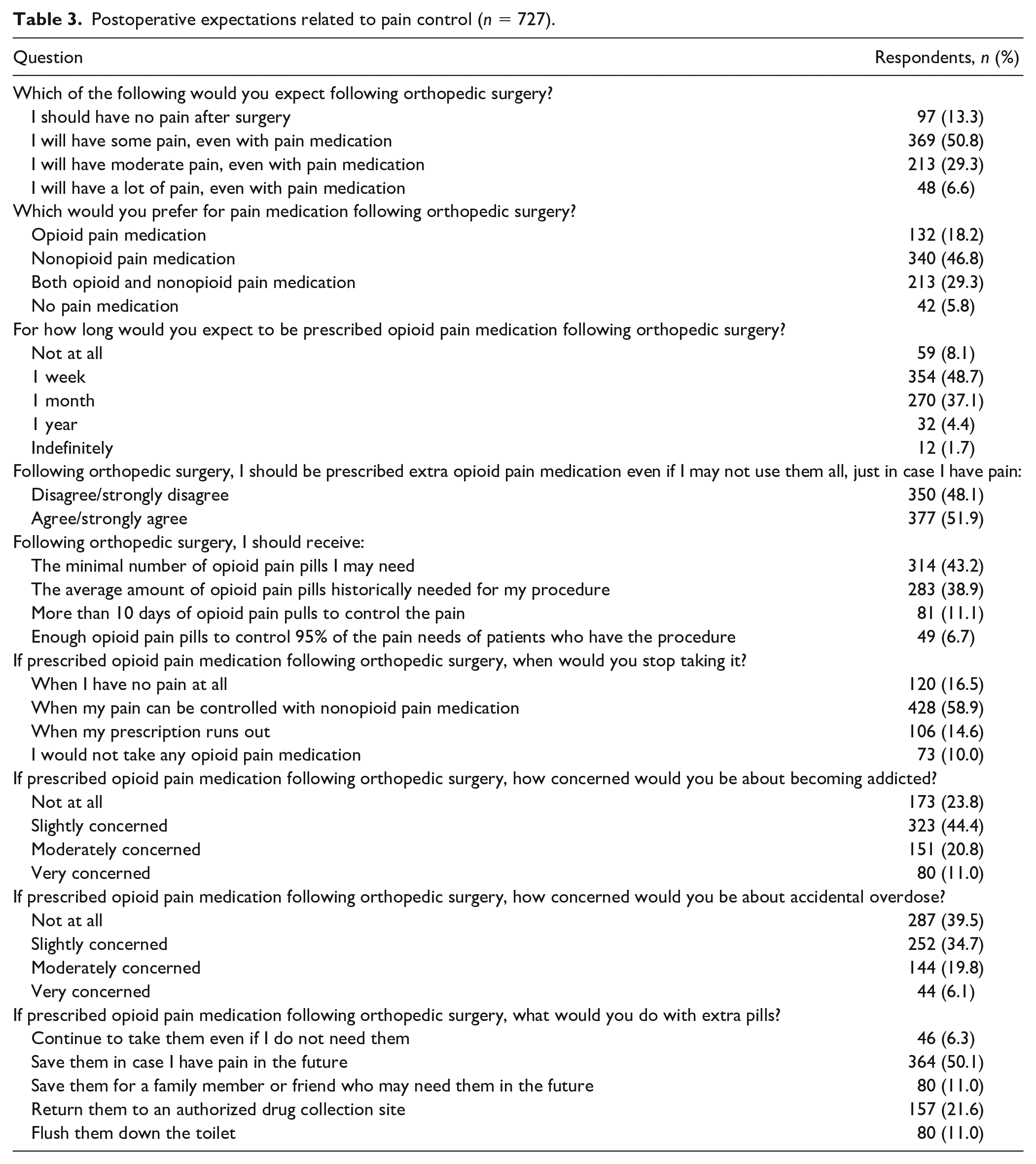
Nearly half (46%) of respondents said they would prefer nonopioid pain medication after elective orthopedic surgery and 29% would prefer both opioid and nonopioid pain medication. However, 86% said they would expect to be prescribed opioids for 1 week to 1 month postoperatively. About half (52%) believe they should be prescribed extra opioid pain medication in case they have unexpected pain following surgery, and 50% would save their extra pills to treat potential pain in the future. A majority of participants (59%) said they would stop taking opioid pain medication when their pain could be controlled with nonopioid pain medication; however, 15% would continue taking opioid pain medication until their prescription ran out.
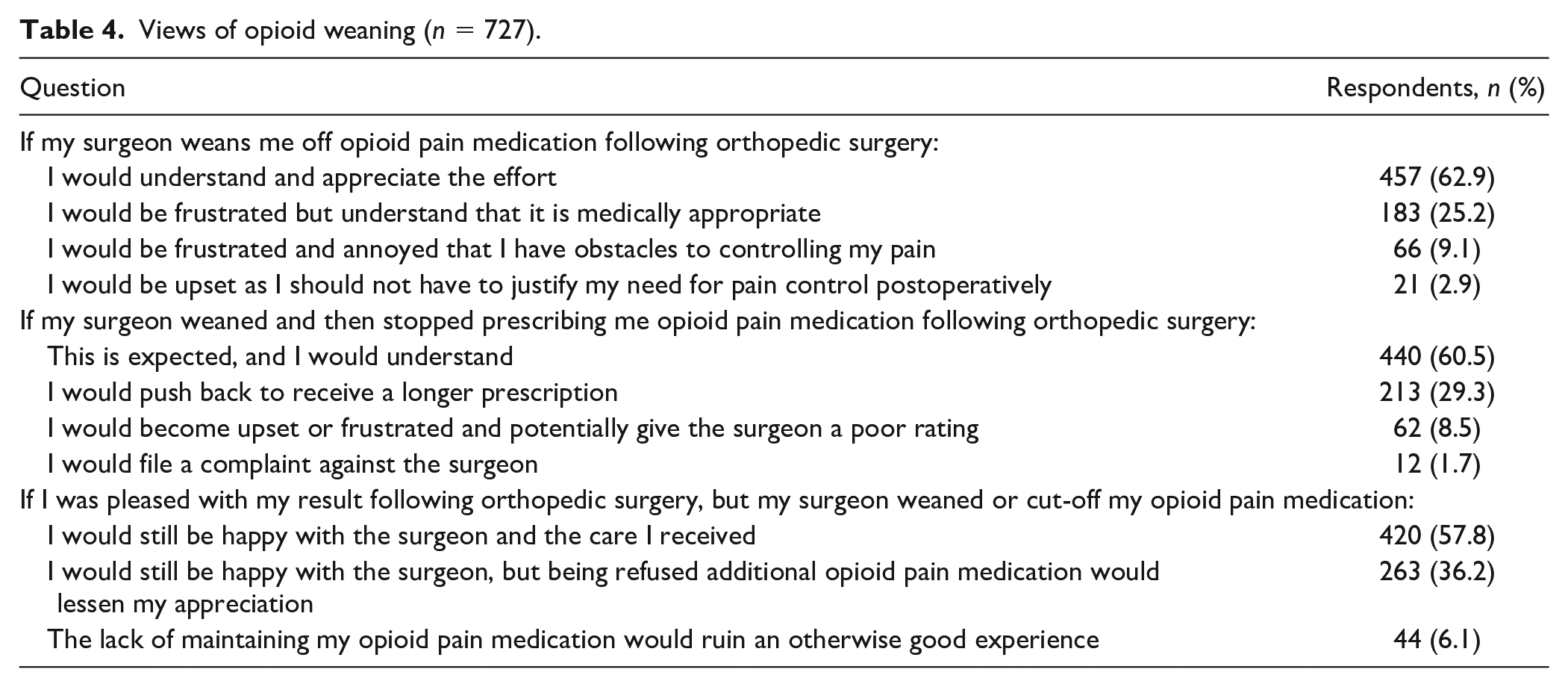
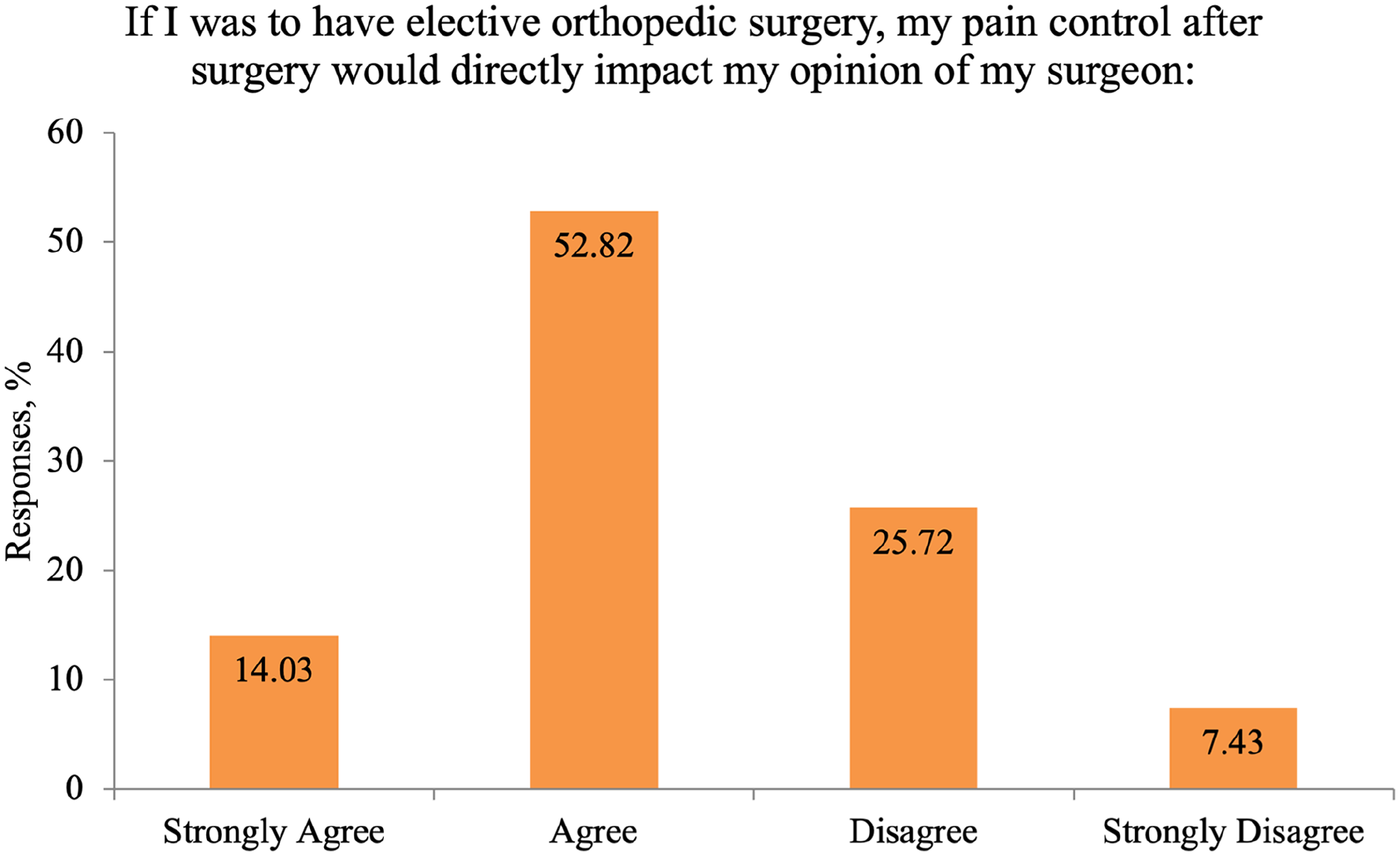
Most respondents (63%) said they would be understanding of opioid weaning attempts by their surgeon in the postoperative period; however, over a third (37%) said they would have reduced satisfaction with their surgeon as a result (Table 4). When asked about opioid weaning following orthopedic surgery, 60% of participants reported that it is expected. However, nearly 30% reported they would push to receive a longer prescription and 8.5% would potentially give their surgeon a poor rating (Table 4: Question #2). Roughly ⅔ (67%) of respondents believed that pain control after elective orthopedic surgery would directly affect their opinion of their surgeon (Fig. 1). Multivariable regression analysis identified respondents with limited health literacy (OR 2.73; 95% CI 1.69–4.40; P < .001) and current tobacco use (OR 1.80; 95% CI 1.11–2.91; P = .017) as significantly associated with feeling upset or frustrated with their surgeon, whereas privately insured people (OR 0.59; 95% CI 0.36–0.978, P = .041) were more likely to say they would be satisfied with their surgeon’s efforts.
Views of opioid weaning (n = 727).
Responses by percentage.
Discussion
In order to combat the opioid epidemic, clinicians must understand patients’ views about opioid medication and postoperative pain control. For our survey, we used an online crowdsourcing platform, Amazon MTurk, to explore public perceptions of opioids, their use for postoperative pain control, and expectations surrounding surgeon behaviors and prescribing practices. A majority of our survey respondents reported that they believe prescription opioids are overused to treat pain and opioid use and misuse is a serious problem. However, most respondents also reported that they would expect to be prescribed opioids for 1 week to 1 month after elective orthopedic surgery. More than half of respondents would also expect to be prescribed extra medication in case of unexpected future pain. Furthermore, most participants reported that pain control following elective orthopedic surgery would directly affect their opinion of their surgeon. Our findings suggest that there are several key areas clinicians might address during preoperative counseling, including patient expectations surrounding pain, pain management strategies, pill management, and postoperative opioid weaning.
There are limitations that should be considered when interpreting the results of this survey. Our respondents were largely under the age of 60 years old, and therefore our findings are not generalizable to older adults, a population with high prevalence of elective orthopedic surgery. Also, our respondents included more people who were current tobacco smokers (30%) than the general population (14%) [8]. However, the number of people reporting history of illicit drug use (42%) was similar to the rest of the US population (39%) [41]. In addition, our survey was prone to sampling error, as the respondents were more likely than the US population to be White or Asian, have more advanced educational degrees, and have public health insurance. Our respondents also reported few or no preexisting symptoms, as they were not patients indicated for orthopedic surgery and could not therefore be proxies for patients. Still, we believe that our survey respondents are an acceptable proxy for the general public for several reasons. Prior researchers have surveyed members of the public in order to understand patient perceptions regarding elective surgery [12,22], and the Amazon MTurk platform has been reported to produce data with closer generalizability to the US population than data obtained through traditional survey methods [6,30].
Prior research has found that postoperative pain is a primary concern for up to 80% of patients before surgery [14] and that 55% to 76% of patients expect no pain after knee surgery [26, 27 ]. In our survey, just 13% of respondents expected no pain after surgery. Preoperative patient expectations have been studied in total hip and knee arthroplasty, shoulder surgery, and spine surgery, all of which showed higher expectations of pain control than our survey found [43]. We hypothesize that in our survey the rate is lower because our questions focused on the immediate postoperative period. We think that this addresses a gap in the literature, as most surveys have focused on longer-term patient expectations. Despite the fact that a lower percentage of our respondents expected no pain postoperatively than prior studies showed, 13% is still a high percentage since rarely are patients completely pain-free in the immediate postoperative period. Our multivariate regression analysis revealed that respondents who were current smokers and those from the Northeastern United States were more likely to say that they would expect no postsurgical pain. Historically, patients have been shown to be poor predictors of postoperative pain, with 43% underestimating it [25]. Surgeons should consider investigating patient pain expectations during counseling preoperatively, when concerns can be addressed.
Although significant efforts have been made to reduce opioid consumption after orthopedic surgery, opioid medications continue to be an important component of postoperative pain control [16]. Efforts to reduce opioid prescribing and use include mandating the use of prescription drug monitoring programs, identifying and educating high-risk patients, increasing the use of regional anesthesia, and encouraging the use of alternative analgesics such as acetaminophen and nonsteroidal anti-inflammatory drugs [3,16,35]. In our survey, 76% of respondents said they would prefer either nonopioid medication or a combination of nonopioid and opioid medication for postoperative pain management. This suggests that many people are open to multimodal pain management therapies including opioid-sparing approaches. In contrast to this, 86% of our respondents said that they would expect to be prescribed opioids for 1 week and up to 1 month after surgery. This discrepancy highlights the importance of communication between patients and surgeons to set expectations regarding opioid medication prescriptions and use after surgery. For example, Sun et al found that a single prescription of low-dose opioids was sufficient for patients undergoing total joint arthroplasty who received preoperative counseling on postoperative pain expectations and management [42].
The number of opioid pills prescribed compared to the number consumed has been studied, with findings showing that opioids are routinely prescribed and filled in excess of actual patient needs [1,4,23,36,53]. Over half of our survey respondents (52%) said they would expect to be prescribed extra opioid medication in case they have unexpected pain following surgery. The number of opioids prescribed postoperatively varies widely for the most common elective orthopedic surgeries. Sabatino et al found that the range of opioid pills prescribed including refills was 30–560 (mean 113.6) for patients undergoing total hip arthroplasty, 10–480 (mean 176.4) for total knee arthroplasty, 0–220 (mean 24.3) for endoscopic carpal tunnel release, 30–435 for arthroscopic rotator cuff repair, and 14–364 (mean 98.2) for lumbar decompression [36]. Longer durations of initial prescriptions have been shown to increase the risk of long-term opioid use, and extra pills are at risk for diversion for inappropriate use [31,32,33]. In our survey, approximately 1 in 7 respondents said they would discontinue taking their pain medication when the prescription ran out, rather than when their pain could be controlled with nonopioid medications. Our survey also found that 50% of respondents said that they would save extra pills to treat future pain, and 11% would save them to give to someone else. These findings suggest the need for diligent opioid prescribing and disposal practices. It also emphasizes the need for further research to more accurately tailor prescribing practices for specific orthopedic procedures. Patients undergoing orthopedic surgery should be informed that leftover opioid tablets can be disposed of at their local police station or a medication disposal site listed on the US Drug Enforcement Agency website [49]. Patients should also be asked about opioid use at every follow-up visit.
In our survey, 60% of respondents reported that they would expect and understand when their surgeon began weaning and eventually stopping their opioid use. Surprisingly, the other 40% of respondents did not select this option. Of these participants, 74% responded that they would push back and request a longer prescription and 21% responded that they would be upset and give their surgeon a poor rating. The remaining 4.2% in this group said they would file a complaint against their surgeon. Based on how the question (Table 4: question #2) was phrased we assumed that the action of weaning and stopping was the reason for this response and not merely suggesting weaning.
Multivariate regression analysis revealed that smokers and those with low health literacy were more likely to feel upset or frustrated with their surgeon. This is an essential point as it illuminates an unaddressed gap in patient education and preoperative counseling. Furthermore, our analysis of those respondents informs providers about a group that may be specifically targeted for future preoperative education. The American Academy of Orthopaedic Surgeons recently published an advisory on opioid stewardship aimed at decreasing opioid use while still managing pain, which may be difficult to achieve if patients are not amenable to decreasing their opioid usage over time in the postoperative period [2]. Opioid education and weaning expectations should be addressed preoperatively; this has been done with reported success in a controlled setting [3,33,52]. In a prospective randomized controlled trial by Ilyas et al, patients who had preoperative opioid education consumed half the number of pills as patients who did not receive opioid education prior to elective outpatient orthopedic surgeries [20].
Over ⅔ of respondents to our survey reported that pain control after elective orthopedic surgery would directly affect their opinion of their surgeon. This finding is critical, given that 25% of hospital and physician reimbursement from the Centers for Medicare and Medicaid Services (CMS) is directly tied to patient satisfaction [7]. The Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey is a well-known tool used by CMS to assess patient satisfaction. Poor pain control has been linked to lower HCAHPS scores and longer than expected length of hospital stay [28,38]. This poses a potential conundrum for surgeons. We found that a majority of the respondents to our survey would expect to be prescribed opioids after surgery, even though they also reported a preference for nonopioid pain control. A majority of our survey respondents also reported that they would experience decreased satisfaction if their physician attempted to wean their opioid use postoperatively. Interestingly, among respondents, tobacco smokers were more likely to report both expectations of no pain after surgery and frustration with opioid weaning attempts after surgery. These responses suggest a need for further study into the value of preoperative education and communication between surgeons and patients, as well as the value of targeting patients who smoke cigarette for such interventions.
In conclusion, this study used online crowdsourcing to conduct a survey of public expectations surrounding postoperative pain control and opioid use. Patients’ expectations and surgeons’ opioid prescribing practices could lead to potential conflict and decreased satisfaction. Orthopedic surgeons, midlevel prescribers, and ancillary staff may benefit from initiatives to better manage patient expectations surrounding postoperative pain control, medication management, and opioid weaning prior to surgery. We hope our survey findings may provide a window into public perceptions of opioid use as a basis for future research into how orthopedic surgeons can talk with patients about their expectations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was not required for participation in this survey.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
CME Credit
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.