
Abstract
Background
Surgery is a central component of healthcare but involves significant risks, with complications occurring in 16.4% patients, accounting for 7.7% of worldwide fatalities. “Surgery 4.0” or digitisation of surgery, has introduced extended reality (XR) technology, offering opportunities to enhance peri-operative care. This study explored the current uses of XR to improve outcomes for general surgery patients.
Method
A systematic search of MEDLINE, EMBASE, and Cochrane databases was performed in August 2024 to include studies using XR for pre-operative planning, navigation or patient experience for adult patients undergoing general surgery. Data on pre-operative planning, post-operative complications, patient experience, image segmentation and study reporting were presented using a narrative approach.
Results
The search returned 966 articles. 26 studies were included featuring 1142 patients. The most investigated procedure was liver resection (n = 11, 42%), with XR interventions showing significant reductions in length of stay, blood loss, operative time and complication rates. Improved outcomes were only seen for patients undergoing liver resection. For patient experience (n = 5, 19%), XR systems were shown to significantly improve anxiety, pain and mood scores. Most studies (n = 11, 73%%) utilised manual methods for image segmentation, costing up to €650 and taking 3-6 hours per model. Reporting of the XR technology, assessment and future development was variable.
Conclusion
The benefits of XR technology to improve patient outcomes in liver surgery are emerging but are yet to materialise in other general surgical procedures. Future research should focus on automatic image segmentation to improve workflow efficiency and innovation frameworks to generate robust evidence.
Keywords
Introduction
Around 310 million major surgical procedures are performed each year worldwide. 1 Despite advances in surgery and perioperative care, surgery still involves significant risks, accounting for 7.7% of all worldwide fatalities. 2 One or more surgical complications occur in 16.4% patients, with 9% being potentially life-threatening and requiring intervention. The risk of surgical complications increases with the complexity of the procedure. For complex surgery, such as pancreatic or liver resections, the risk of surgical complications has been reported as high as 48% and 60%, respectively.3,4 One way to reduce the rate of complications is to improve surgical planning. Implementation of new technologies, which enhance the review of individual patient anatomy, might improve surgical planning and improve patient outcomes. Surgical navigations systems, leveraging data from radiological imaging, could improve efficiency and safety in the operating theatre, reducing operative duration, complication rates and length of stay for patients. 5
“Surgery 4.0” is a concept that encompasses the digitisation of surgery, including the internet of things, artificial intelligence, surgical data science, and extended reality (XR). 6 XR is an umbrella term for all devices that alter the human-computer interaction. 7 This includes virtual reality (VR), where the user sees digitally rendered images without the physical world; augmented reality (AR), involving the physical world augmented by digital information, and mixed reality (MR), which uses a mixture of methods to blend the physical and digital world. Individual patient anatomy can now be displayed in XR using medical imaging segmentation, a process involving partitioning of images into distinct regions, enabling three dimensional reconstructions. 8 XR technology has been mainly used in general surgery for surgical training and education. 9 Clinical interventions using XR for patient care are emerging, but their efficacy is largely unknown. This systematic review aims to determine the current uses of XR to improve outcomes for patients undergoing general surgery.
Methods
Study Design and Definitions
The study protocol was developed in accordance with the PRISMA and AMSTAR 2 guidelines and was prospectively registered with PROSPERO (registration number CRD42024569448).10,11 XR interventions were defined as XR technology (VR, AR and MR) used as an intervention to influence patient outcomes in all pre-operative, intra-operative and post-operative aspects of care. The review focused on applications in general surgery, defined as gastrointestinal, endocrine, breast, trauma or organ transplantation procedures, in adult patients (aged 18 and over).
Selection Criteria
To enrich the data captured in this systematic review, all study types, excluding conference abstracts and case reports, were included. The studies included had to use XR as a patient intervention for perioperative care in adult patients undergoing a general surgical procedure. There were no time or language restrictions. Specific exclusion criteria included. Conference abstracts or case reports; Studies involving other modes of surgical visualisation technology rather than XR, such as robotic platforms or indocyanine green (ICG) fluorescence used without XR technology; Studies focusing on procedures not considered to be general surgery.
Systematic Literature Search
Embase (Ovid), MEDLINE (Ovid) and Cochrane Library databases were systematically searched in August 2024. All identified studies were reviewed against the inclusion and exclusion criteria to assess eligibility. Referenced studies within identified literature were accessed and considered for inclusion. Screening was performed by two independent investigators (MK and TW) and studies identified were analysed for relevance to the systematic review prior to full inspection. Any discrepancies between the independent investigators were addressed by a third senior investigator (DJ) until consensus was achieved. The search strategies used are displayed in full in Appendix S1.
Primary and Secondary Outcomes
The primary outcomes included post-operative complications (blood loss, resection margin status, operative time, complications, length of stay, mortality) to assess the impact of XR technology for pre-operative planning and surgical navigation. The secondary outcomes were collected to explore other XR interventions as part of the peri-operative pathway and the current reporting of XR technologies in the literature. Secondary outcomes were grouped into. Surgical planning and navigation uses (pre-operative review of anatomy, anatomical structure identification); Patient experience (pain levels, anxiety); Modality of primary source imaging; Mode of segmentation; Reporting of performance, safety and preparatory steps for definitive clinical trials.
Data Extraction
Two independent investigators (MK & TW) extracted data in duplicate using a standardised data collection form. The senior author (DJ) was consulted on any discrepancies. Data were extracted on patient characteristics (age, sex, type of surgery), intervention (type of XR, peri-operative stage), study characteristics (number of patients, study type, country of origin) and primary and secondary outcomes.
Data Synthesis
Included studies were tabulated and grouped according to type of general surgical procedure. Data relating to the outcomes of interest were recorded, but due to the heterogeneity amongst study types, meta-analysis of effect estimates were not performed. When applicable, treatment effects were displayed in odds ratios (ORs) or risk ratios (RRs) with 95% confidence intervals (CIs) for dichotomous data. Continuous data treatment effects were expressed as mean differences with 95% CIs. Alongside the traditional approach to reporting data, a structured narrative synthesis was conducted in line with the Guidance on the Conduct of Narrative Synthesis in Systematic Reviews from the Economic and Social Research Council. 12
Risk of Bias
Risk of bias assessment were conducted independently by MK and TW. Any disagreements were consulted with the senior author DJ. For studies which involved a comparison group, the Cochrane’s tool for assessing risk of bias was used. 13 Where applicable, the RoB-2 score was used for randomised controlled trials (RCT) and the ROBINS-I for non-randomised studies (NRS). The risk of bias was assessed as “low risk”, “high risk” or “unclear risk” for each study. The results were depicted graphically using a visualisation tool by McGuinness et al 14
Results
Included and Excluded Studies
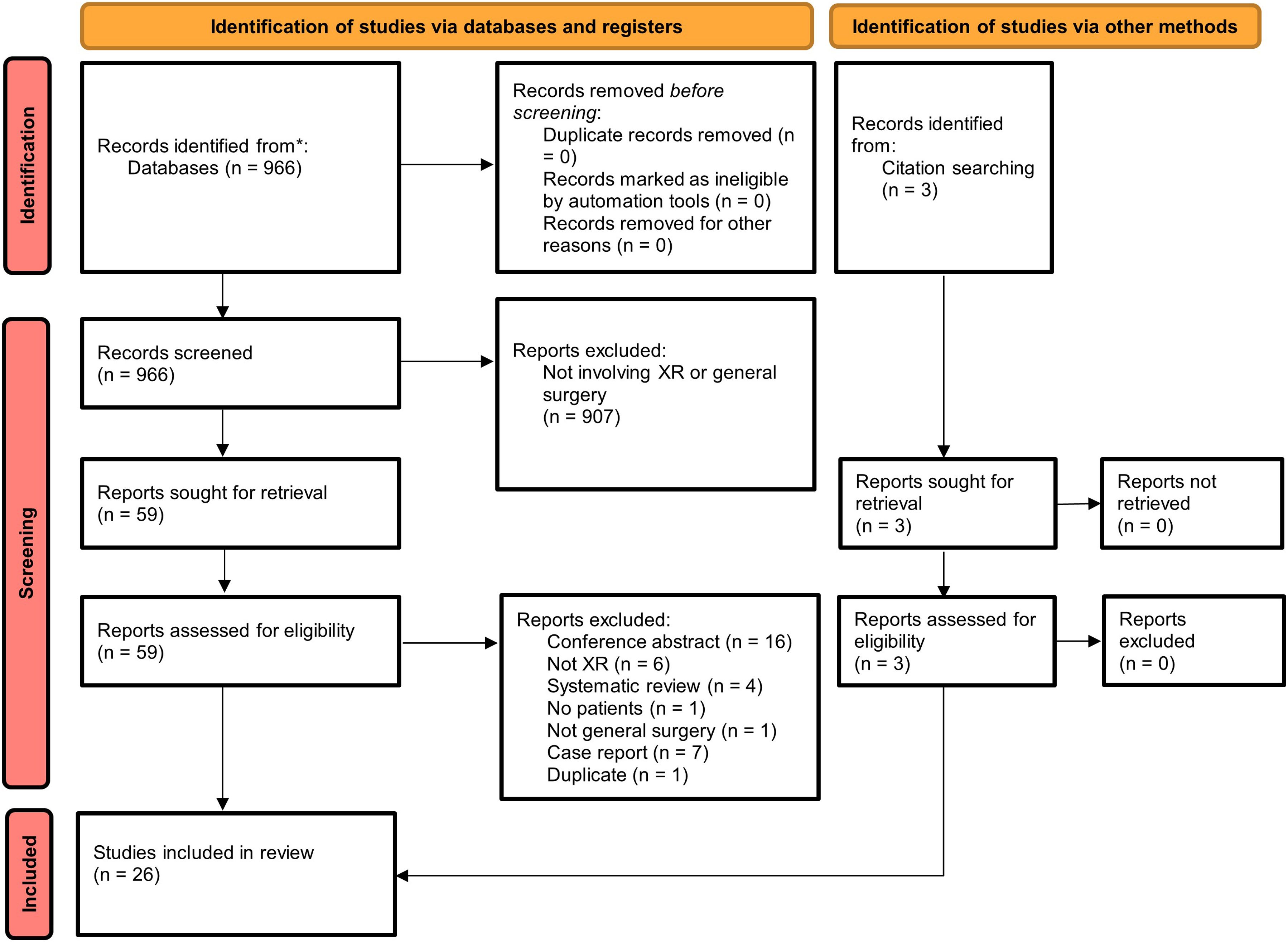
The search strategy returned 966 articles after removing duplicate studies. Following abstract screening, 907 articles were excluded. Full-text reviews excluded 36 studies and three studies meeting inclusion criteria were identified through reference searches. The 26 included studies subsequently underwent data extraction. The selection process together with reasons for exclusion are outlined in the PRISMA flowchart in Figure 1. PRISMA flow diagram for study selection. Adapted from
10
Study Characteristics
Study and Patient Characteristics
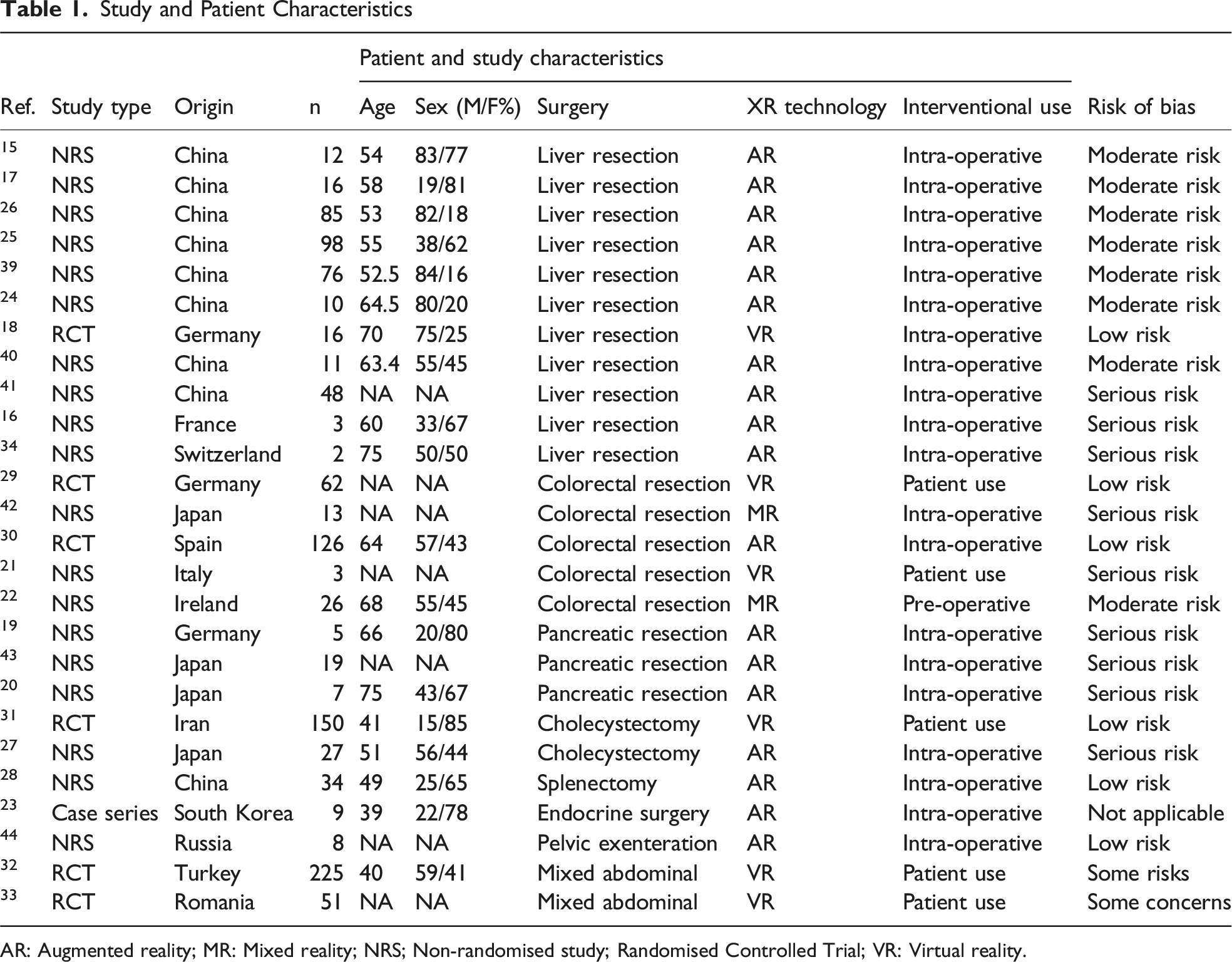
AR: Augmented reality; MR: Mixed reality; NRS; Non-randomised study; Randomised Controlled Trial; VR: Virtual reality.
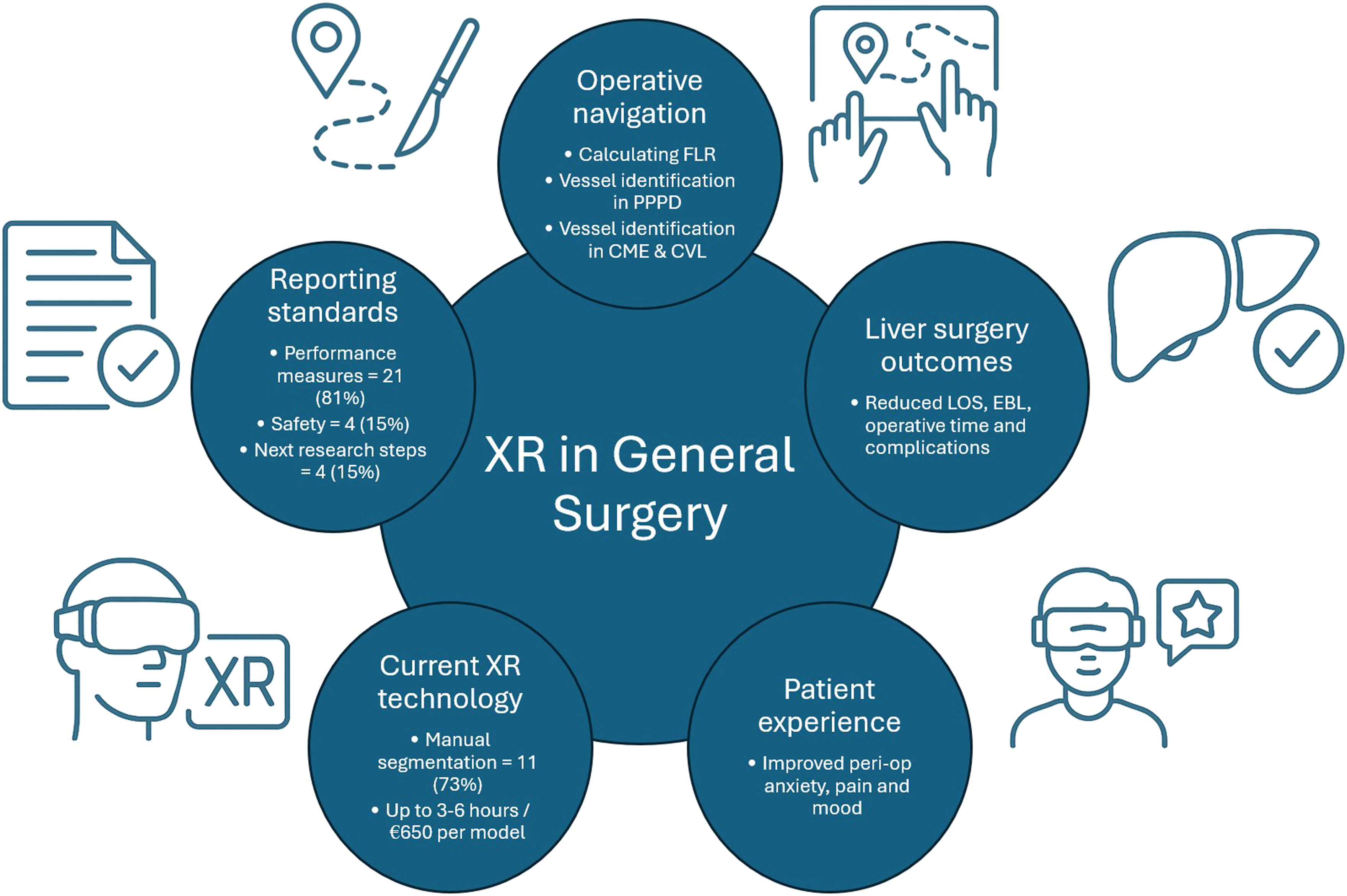
Graphical illustration of immersive reality technology applications and characteristics in general surgery
Quality Assessment
For studies involving a comparison between two groups (case series excluded), quality assessments were performed for 25 studies (19 NRS and 6 RCTs). Using ROBINS-I, the risk of bias in NRS was assessed as “low” in two studies (n = 2/19, 11%), “moderate” in eight studies (n = 8/19, 42%) and “high” in nine studies (n = 9/19, 47%). The reasons most likely to lead to an overall “high” rating included the presence of confounders or poorly defined interventions. For RCTs, the risk of bias according to ROB-2 was assessed as “low” in four studies (n = 4/6, 67%) and “some concerns” in two studies (n = 2/6, 33%). The results are shown graphically in Appendix S2 and S3.
Operative Planning and Navigation
XR Interventions for Pre-operative Planning and Surgical Navigation
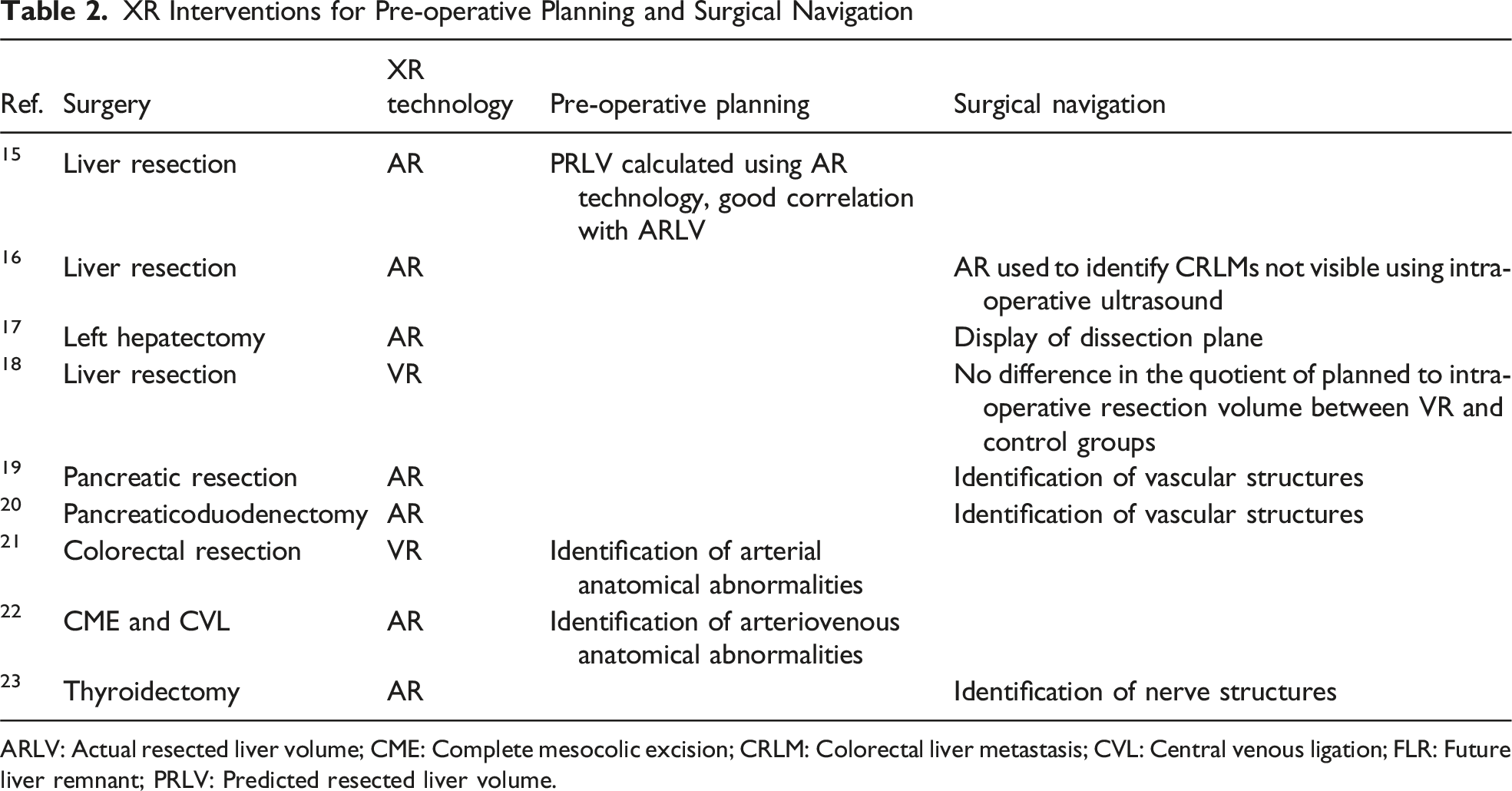
ARLV: Actual resected liver volume; CME: Complete mesocolic excision; CRLM: Colorectal liver metastasis; CVL: Central venous ligation; FLR: Future liver remnant; PRLV: Predicted resected liver volume.
In pancreatic surgery, XR technology has been used to identify key anatomical structures. Javaheri et al 19 used an AR system for pancreatic resection in five patients. Using AR intra-operative overlay, surgeons were able to identify all planned anatomical structures including the gastroduodenal artery, superior mesenteric artery, hepatic artery, splenic vein, inferior and superior mesenteric vein and portal vein. These structures were confirmed with intra-operative ultrasound. Onda et al 20 also found their AR system useful in seven patients undergoing pancreaticoduodenectomy. They were able to identify jejunal arteries and the inferior pancreaticoduodenal artery, which facilitated early intraoperative vascular ligation.
For colorectal procedures, Guerriero et al 21 used VR for pre-operative planning in three patients undergoing colorectal resections. The use of VR was crucial for one patient where an anatomical variant was detected with the left colic artery having an abnormally short origin from the inferior mesenteric artery, enabling the surgeon to anticipate the anomaly and execute safe surgery. Kearns et al 22 also tested their AR system for laparoscopic complete mesocolic excision and central venous ligation. Their 3-D models displayed in AR were able to detect 96% of arteriovenous variations in a cohort of 26 patients.
XR technologies have also been used for surgical planning and navigation in other general surgical procedures. An AR system was tested in the setting of robotic thyroidectomy to aid location of the recurrent laryngeal nerve. 23 In a pilot study involving six patients, all recurrent laryngeal nerves were successfully identified using an AR system with a 1.9 mm mean difference between the AR image and actual nerve position. To conclude, XR technologies have been used for pre-operative planning (such as calculating FLR) and intra-operative navigation, frequently to identify specific anatomical structures (vessels or nerves) or aid tumour identification. The current literature is limited to individual specific uses within small, early studies.
Intra-and Post-operative Outcomes
Intra- and Post-operative Outcomes From Comparison Studies
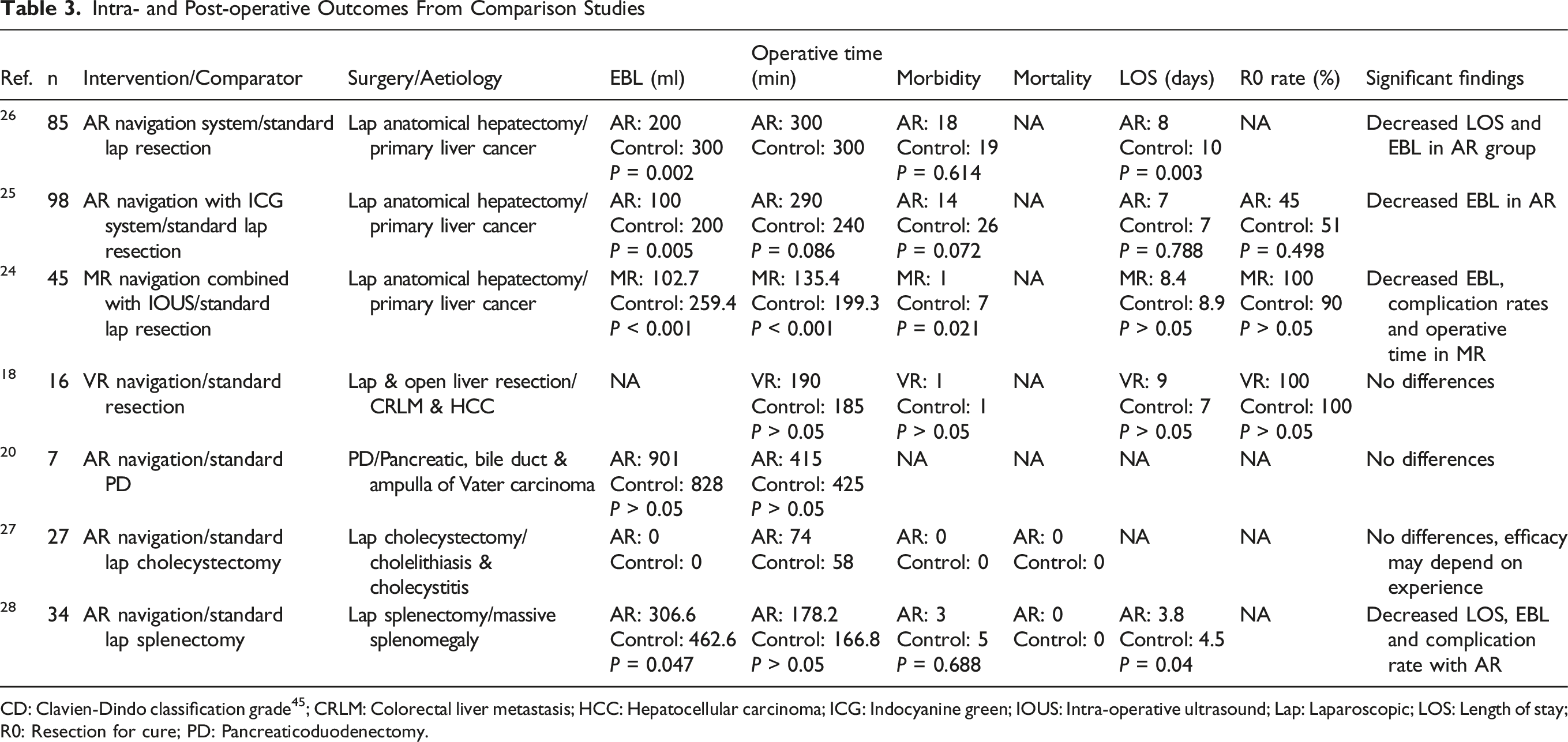
CD: Clavien-Dindo classification grade 45 ; CRLM: Colorectal liver metastasis; HCC: Hepatocellular carcinoma; ICG: Indocyanine green; IOUS: Intra-operative ultrasound; Lap: Laparoscopic; LOS: Length of stay; R0: Resection for cure; PD: Pancreaticoduodenectomy.
Patient Experience
XR Interventions for Patient Experience and Recovery
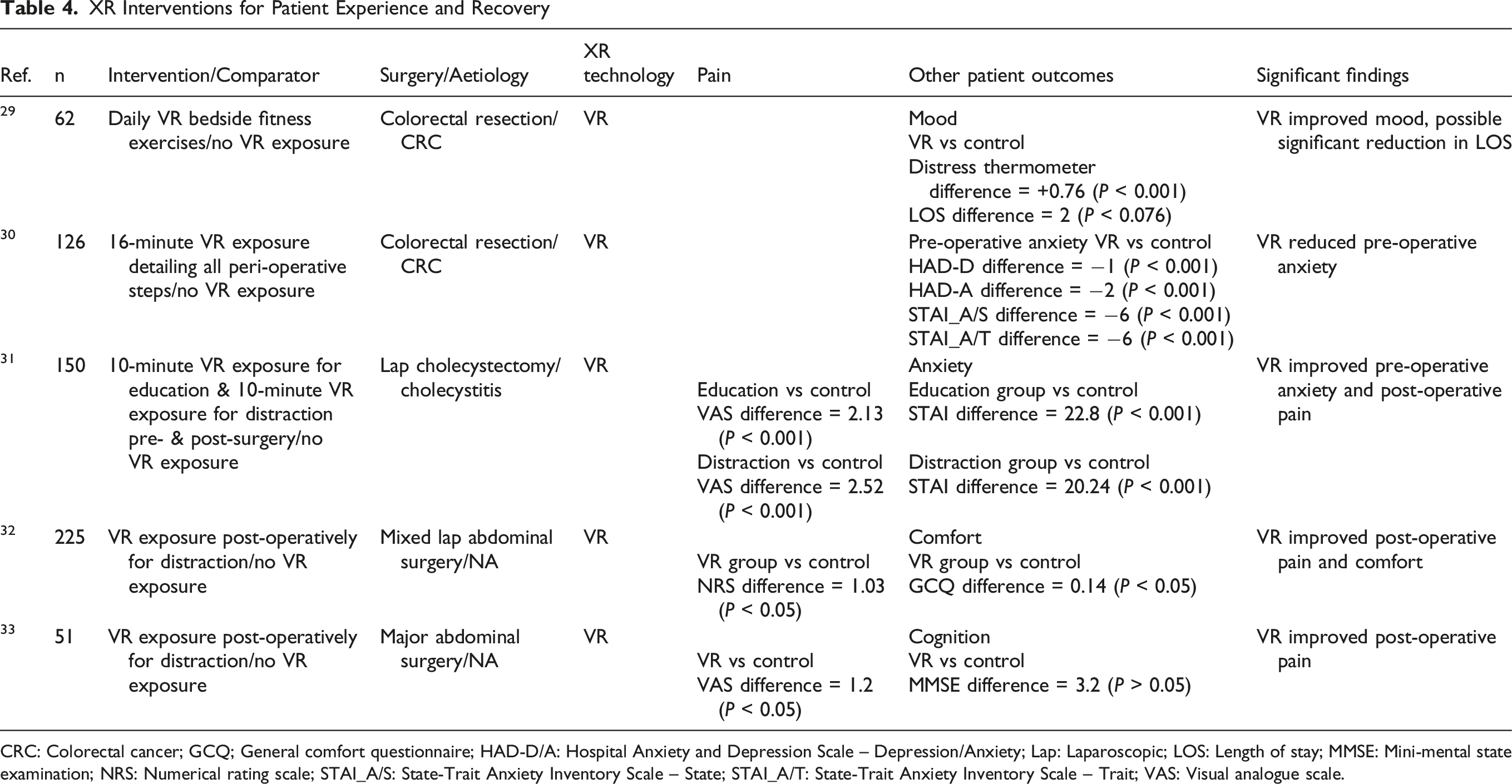
CRC: Colorectal cancer; GCQ; General comfort questionnaire; HAD-D/A: Hospital Anxiety and Depression Scale – Depression/Anxiety; Lap: Laparoscopic; LOS: Length of stay; MMSE: Mini-mental state examination; NRS: Numerical rating scale; STAI_A/S: State-Trait Anxiety Inventory Scale – State; STAI_A/T: State-Trait Anxiety Inventory Scale – Trait; VAS: Visual analogue scale.
XR Technology Reporting
XR Technology Reporting
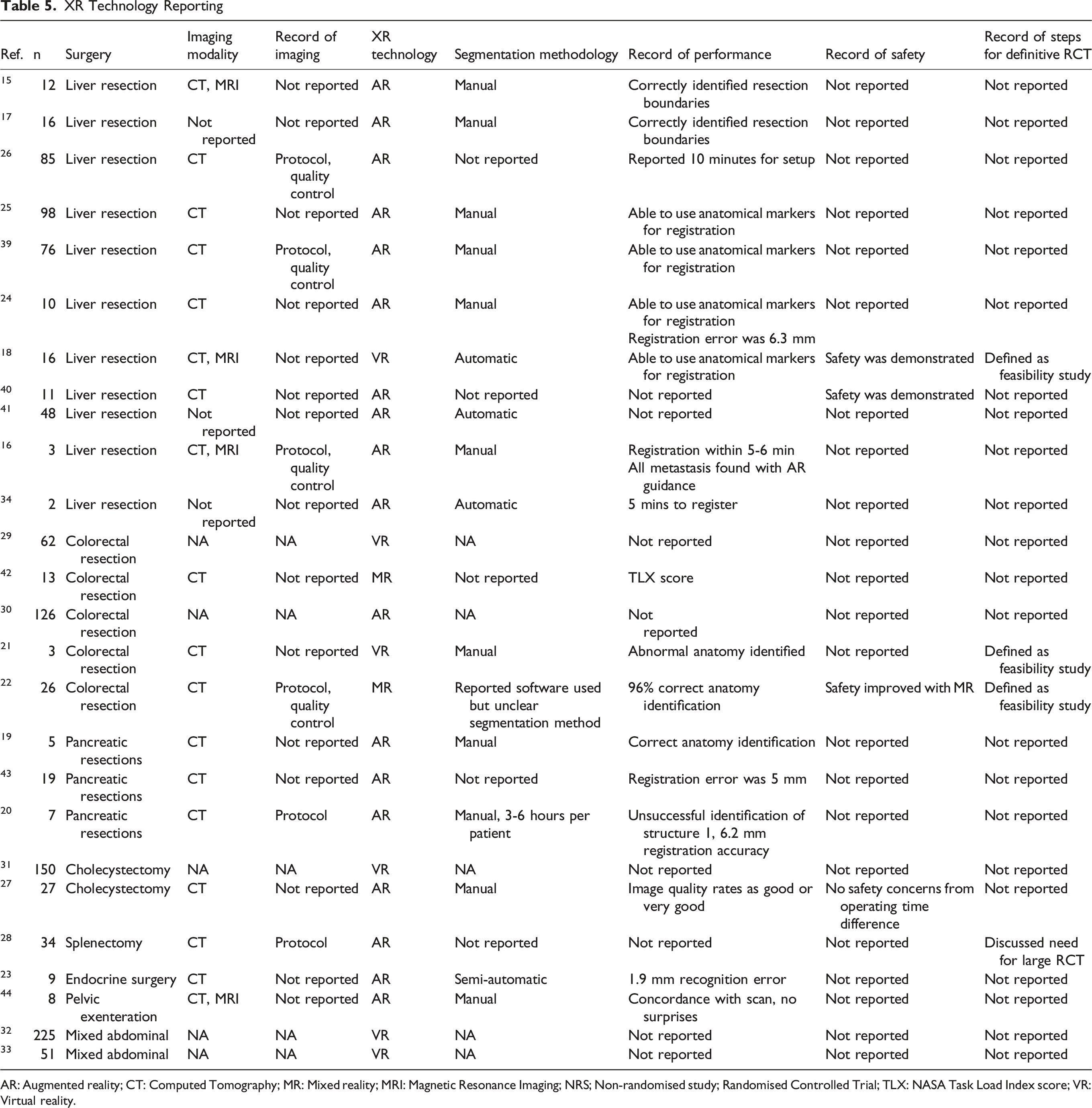
AR: Augmented reality; CT: Computed Tomography; MR: Mixed reality; MRI: Magnetic Resonance Imaging; NRS; Non-randomised study; Randomised Controlled Trial; TLX: NASA Task Load Index score; VR: Virtual reality.
Discussion
XR systems have been found to be useful in surgical planning and navigation, particularly in identifying vascular structures and tumours in hepato-pancreato-biliary (HPB) and colorectal resections. The benefits for patient outcomes have been reported in liver surgery for primary and metastatic tumours, with reduced LOS, EBL, operative time and complication rates. These results are from small, unpowered studies; however, they provide a signal of potential benefit. Improved outcomes are yet to be defined for other general surgical procedures. For patient education and recovery, XR systems have been shown to produce significant improvements in pre-operative and post-operative anxiety, pain and mood. There are currently no studies which focus on the use of XR for patient consent or for MDT purposes within general surgery. Current XR technologies rely on primarily manual methods for imaging segmentation, which were inefficient, taking 3-6 hours per model in one study, and costly, at 650 euros per model extraction and processing. The quality of current literature is variable, with over 75% of studies at moderate or high risk of bias, and infrequent reporting of imaging source and quality, intervention safety and next steps for definitive trials and technology development. To our knowledge, this is the first systematic review to report on XR interventions in general surgery.
VR technology was first described in a science-fiction story in 1935 and has evolved considerably. 7 Current MR systems enable display of digital and real-world content through a merged reality. This facilitates their use in healthcare environments, such as the operating theatre, where space and sterility are frequent barriers for technology implementation. Despite the technological evolution, clinical uses with an evidenced benefit for patient outcomes are limited. The most recent scoping review of XR research found that much of the XR literature (40%) is aimed at surgical education rather than clinical interventions. 35 When examining studies aimed at clinical uses, literature reviews in other surgical specialities also agree that current evidence for the benefit on patient outcomes is limited. 36 The versatility of XR technology has the potential to enhance all aspects of peri-operative care, but the opportunities are yet to be developed and investigated in high-quality studies.
The strengths of this systematic review include defined inclusion criteria for XR use in general surgery. The results provide a granular description of XR utilisation as well as the benefits for patient outcomes, with significant results for patients undergoing liver surgery. The review also provides a detailed analysis of study reporting, which is variable within this emerging technological field. The quality assessments performed enable a comprehensive review of the current evidence, which is shown to be of limited quality at present. In addition, the review provides an assessment of XR technology, such as imaging source, segmentation methods, along with current limitations and the research required for wider adoption. The limitations of this study are also acknowledged. The heterogeneity of studies prohibited quantitative synthesis by meta-analysis, however, the narrative synthesis provides a meaningful analysis of research across general surgery and the XR field. The low quality of evidence found precludes recommendations for clinical practice at the current stage, but it does highlight the need for robust, high-quality research to assess the evolving XR technology.
The areas for further research in surgical XR have been highlighted. The main factor limiting widespread adoption is manual segmentation. Having experienced clinicians performing image analysis for three to six hours per patient is not feasible in a large healthcare system, such as the National Health Service (NHS). External services providing such analysis are costly, and therefore unlikely to be cost-effective. Artificial intelligence (AI) offers a possible solution for automated segmentation, enabling surgeons to view patient anatomy, operative plans, and intra-operative navigation on demand, and unlocking the potential of XR for widespread use.37 Another challenge to address will include fusion of multiple imaging modalities, as in this review 19% of studies were noted to include more than one type of imaging in their XR models. Automatic segmentation will have to account for variables, such as patient movement and timing of scans, in the image co-registration, but if solved XR models will harness the benefits of different imaging modalities. For example, CT and MRI scans can miss lesions close to the liver surface, whereas ultrasound is able to locate these, but lacks the definition to find deep small lesions in the liver parenchyma, showing that a fusion of the modalities could enhance MDT review, surgical planning and operative navigation. Another barrier to adoption involves the diversity of current XR systems. Nearly all studies involved locally developed early-stage XR systems aimed for one specific surgical application. A generic XR platform that can display multiple organ systems would be beneficial, but would require further innovation. The platforms must be versatile to cater for all surgical approaches. The included studies frequently involve an additional screen or headset to display 3D reconstructions next to laparoscopic stack systems. 22 To reduce the task load associated with new surgical tools, XR technologies must provide a seamless experience integrated within existing surgical equipment, such as laparoscopic stack systems or robotic platforms. Headsets will need to remain an option for open surgery, providing a similar experience to integrated laparoscopic or robotic solutions. In this systematic review, only four studies reported further plans for clinical trials. Ideally, XR systems should be subjected to the same prospective evaluation frameworks as other surgical technologies with minimum standards for reporting, which should include primary imaging source and quality, methods for segmentation, along with safety, efficacy, and utility. 38 XR technology has the potential to improve all aspects of peri-operative care and further studies are required to investigate its utility across the whole surgical care pathway, including multi-disciplinary decision-making and post-operative follow-up. There is scope for more research in other surgical specialties, rather than the current focus on HPB surgery. XR could also explore challenges within surgical subspecialties, such as anastomotic leak or advanced/recurrent cancer.
Conclusion
The use of XR technology has been reported for pre-operative planning, patient education, intra-operative navigation and patient rehabilitation in the field of general surgery. A signal towards improved outcomes has been shown for patients undergoing liver resections, including reduced LOS, EBL, operative time and complication rates. Similar patient benefits are yet to be documented for other general surgical procedures. The findings are limited by the quality of evidence and varied reporting standards of primary imaging source, methods of segmentation and safety. Areas for further research include AI-powered automatic image segmentation, fusion of multiple imaging modalities, interdisciplinary XR platforms, and the use of XR systems across surgical care pathways.
Supplemental Material
Supplemental material - General Surgery 4.0 – A Systematic Review of Extended Reality Interventions in General Surgery
Supplemental material for General Surgery 4.0 – A Systematic Review of Extended Reality Interventions in General Surgery by Mikolaj R Kowal, Tom Williams, Alexios Dosis, Samir Pathak, Shahid Farid, Deborah D Stocken, Peter Lodge, Sharib Ali, Damian Tolan and David G Jayne in Surgical Innovation
Footnotes
Author Contributions
Conceptualization, MRK, SF, SP, DDS, PL, DT, SA, DGJ; resources, MRK, TW, AD; writing—original draft preparation, MRK; writing—review and editing, MRK, TW, AD, SF, SP, DDS, PL, DT, SA, DGJ; visualization, MRK; supervision, DT, SA, DGJ. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MRK receives funding from the European Union, under Grant Agreement No 101137233. Co-funded by the European Union. Views and opinions expressed are, however, those of the authors only and do not necessarily reflect those of the European Union or the European Health and Digital Executive Agency (HADEA). Neither the European Union nor the granting authority can be held responsible for them. AD receives funding from Leeds Hospital Charities (A2002555) and Bowel Research UK Ref: BRUK_SG_24012. DGJ and DDS receive funding support from the National Institute of Health and Care Research (NIHR213331; NIHR205280; NIHR302439). The project is supported in part by the National Institute for Health and Care Research (NIHR) Leeds Biomedical Research Centre (BRC) (NIHR213331). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author PL has previously acted as a paid consultant for HoloCare Limited but declares no non-financial competing interests. All other authors declare no financial or non-financial competing interests.
Supplemental Material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.