
Abstract
Background/Need
Precision suturing in confined surgical fields poses ergonomic and visibility challenges, particularly in minimally invasive and reconstructive procedures. A novel Vertical Needle Holder (VNH) was designed to enhance control, angle precision, and accessibility in restricted spaces.
Methodology and Device Description
This proof-of-concept study evaluated the VNH’s ergonomic design and suturing performance compared with a standard Mayo-Hegar needle holder. Thirty surgeons and surgical trainees participated in simulated suturing tasks using both instruments. Surgeon-reported outcomes were assessed using standardized synthetic-tissue suturing tasks and a structured Likert-scale questionnaire focusing on perceived precision, ergonomics, and ease of use.
Preliminary Results
Surgeons reported improved perceived precision and maneuverability of the VNH in confined spaces compared with conventional needle holders. Participants reported reduced wrist strain and greater visibility. The majority of participants (87%) rated the VNH as ergonomically superior to conventional needle holder designs.
Current Status
These findings suggest that the VNH offers an innovative, practical enhancement to traditional surgical tools, potentially improving safety and efficiency in complex operative fields. Further clinical validation is underway to confirm translational applicability.
Keywords
Introduction
Accurate needle placement is essential for successful wound closure, anastomosis, and tissue reconstruction in both open and minimally invasive surgical procedures. In confined or deep operative fields, such as pelvic floor repair, vascular anastomosis, and base of tongue reconstruction, the precision of needle trajectory directly influences tissue healing, operative time, and complication rates. 1 Conventional needle holders are widely used in surgical practice, yet their design turn hand movements of surgeons into an elliptical needle path. This often results in an off-midline deviation between intended and actual suture points, which can be clinically significant in microsurgical or anatomically constrained settings. 2
The ergonomic demands of conventional designs further compound this limitation. Standard drivers require wrist pronation-supination to align the needle with the target plane, which can lead to increased hand fatigue and suboptimal control in restricted surgical spaces. 3 These challenges have spurred the development of advanced multi-degree-of-freedom (multi-DOF) needle drivers, particularly in laparoscopic surgery, where constrained instrument maneuverability has long been recognized as a limiting factor. 4 Prior studies of articulating and multi-DOF laparoscopic devices have demonstrated improved needle trajectory control and suturing efficiency compared with conventional laparoscopic needle holders.5,6
Despite these advances, most existing innovations are optimized for laparoscopic or robotic platforms and are not readily transferable to open surgery in anatomically restricted fields. Such systems often involve complex articulation mechanisms, higher costs, and learning curves that limit their routine use outside minimally invasive settings. Consequently, open surgical procedures performed in deep or narrow operative fields continue to rely predominantly on conventional straight needle holders, despite their known ergonomic and trajectory-related limitations.
The Vertical Needle Holder (VNH) was developed to address this unmet need in open and hybrid surgical environments. The device enables a mechanically guided vertical needle trajectory without requiring wrist twisting or complex articulation. The VNH automatically orients the needle tip towards an orthogonal entry point between two target locations by employing dual perpendicular pivot axes. This configuration is intended to maintain the surgeon’s wrist in a neutral position while improving steadiness, control, and precision during suturing in deep or confined operative fields.
The objective of this study was to describe the design and mechanical principles of the VNH, to evaluate its usability across multiple surgical specialties through a multicenter proof-of-concept survey, and to compare surgeon-reported performance outcomes with those of a conventional needle holder in a controlled synthetic-tissue suturing model.
Materials and Methods
Study Design and Overview
We evaluated a novel Vertical Needle Holder (VNH) through a two-phase assessment consisting of a multicenter proof-of-concept (PoC) survey and a supplementary synthetic-tissue evaluation. . The initial PoC survey was conducted among practicing surgeons following a standardized device demonstration, while the later synthetic-tissue evaluation served to update usability perceptions in a contemporary cohort using the same instrument design. The work was deemed minimal risk and exempt from formal institutional review board oversight because it involved no patients, patient data, or identifiable personal information. All procedures adhered to good research practice, with pre-specified outcomes and standardized demonstration protocols.
Device Description
The Vertical Needle Holder (VNH) is a patented instrument (US Patent No. 8,535,348 B1, issued September 17, 2013 to Alshemari). It was developed to convert the surgeon’s linear hand motion into a guided vertical trajectory of the needle between two target points, thereby reducing reliance on wrist pronation or supination. The instrument incorporates two perpendicular pivot axes within its shaft that mechanically constrain the motion of the needle to a straight, orthogonal path during tissue penetration. The VNH is designed to maintain consistent midline alignment by guiding the needle along a linear push rather than the elliptical arc characteristics of conventional needle holders. The jaws are patterned with fine cross-hatching to improve purchase and minimize slippage, consistent with established needle-holder design principles, and a standard ratchet mechanism provides secure closure and a stable grip during tissue passage. Representative images of the instrument and its use are shown in Figure 1. Perspective view of vertical needle holder (US patent no. 8,535,348 B1)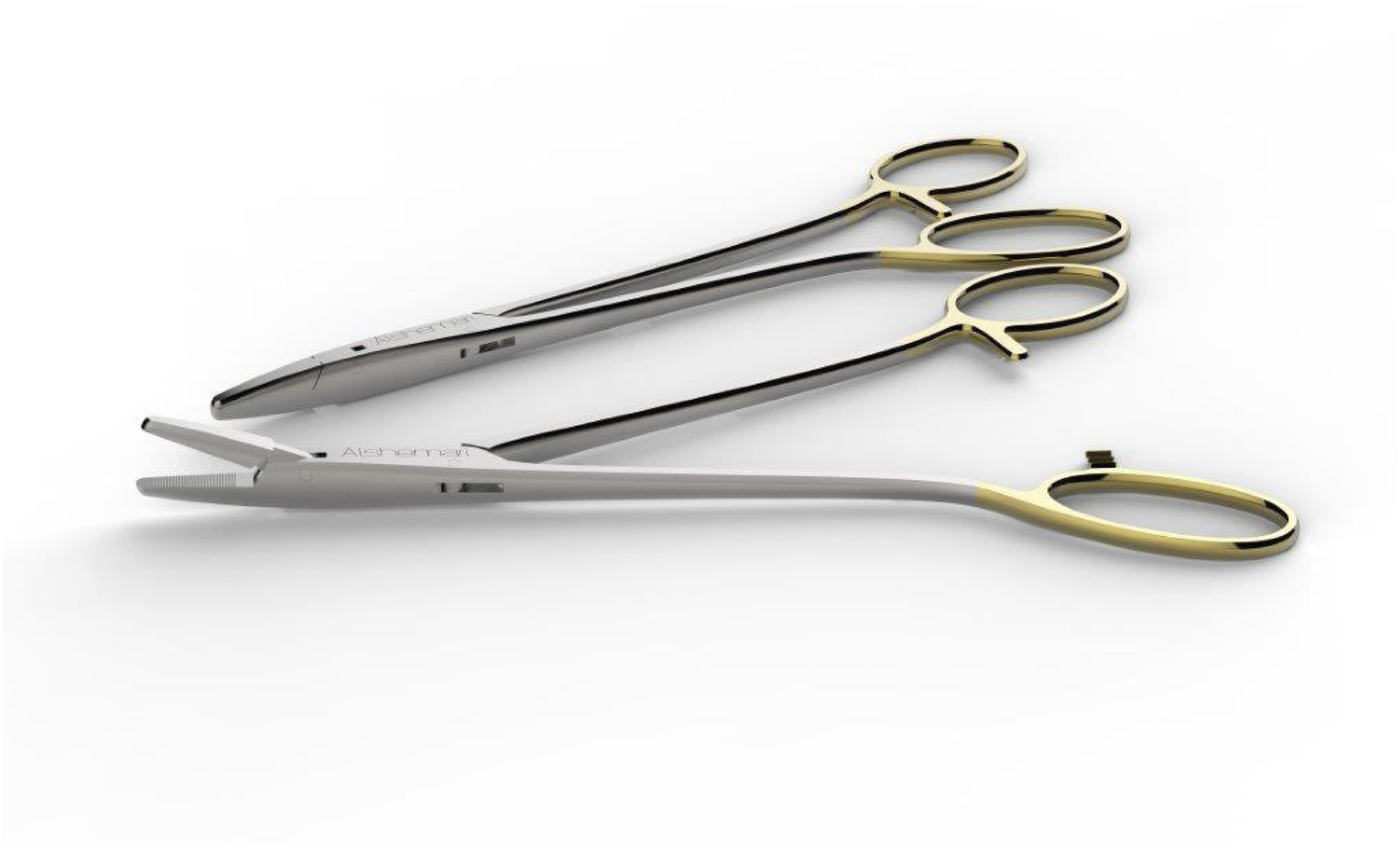
Multicenter Proof-of-Concept Survey (2016-2017)
Sites, Participants, and Procedures
From October 2016 to March 2017, surgeons representing 28 medical centers across the United States were recruited via departmental lists. Participants encompassed a range of subspecialties including general surgery, gynecology, otolaryngology, plastic surgery, urology, vascular surgery, and cardiothoracic surgery. Each session began with a standardized 10-12-minute demonstration of the Vertical Needle Holder (VNH), during which the device mechanism, grip, and straight-line needle-driving action were explained. Following this, participants were then invited to handle the instrument and perform two to three practice sutures on a synthetic pad. These introductory suturing attempts were not timed and were intended for familiarization rather than performance assessment. Immediately following the demonstration, participants completed a structured questionnaire comprising 5-point Likert-scale items and free-text responses. Survey domains included perceived precision in deep or narrow operative fields, ergonomics and comfort, ease of adoption and learning, and potential indications for clinical use.
Quality Control and Bias Mitigation
Several measures were implemented to minimize bias and enhance data quality. All demonstrations followed a standardized script, and demonstrators were not involved in data collection or analysis. No explicit comparisons between the VNH and conventional needle holders were made during the demonstration sessions. Survey responses were collected anonymously, and participant specialties were coded to prevent identification of individual institutions.
Extended Synthetic-Tissue Evaluation (2023-2024)
Between January 2023 and March 2024, a supplementary evaluation was conducted using standardized synthetic tissue models to reassess surgeon perceptions of the VNH in a contemporary setting. Fifteen practicing surgeons from general surgery, gynecology, plastic surgery, and otolaryngology were invited to participate. Each surgeon performed interrupted sutures using both the VNH and a conventional needle holder. Participants completed the same structured questionnaire used in the 2016-2017 PoC survey, with items focusing on perceived precision, ergonomics, ease of use, and applicability in confined operative fields. This evaluation was intended to update usability perceptions rather than replicate the original multicenter PoC study or assess a modified instrument design.
Statistical Analysis
Survey data were analyzed descriptively. Categorical responses were summarized as frequencies and percentages. Likert-scale data were summarized using medians and interquartile ranges to reflect central tendency and variability. Comparative assessments between the VNH and conventional needle holder in the synthetic-tissue evaluation were examined using paired nonparametric tests, with a two-sided P-value < 0.05 considered statistically significant.
Ethical Considerations
This study involved no patient data or animal use. Both the proof-of-concept survey and synthetic-tissue evaluations were conducted in accordance with institutional research policies and ethical standards. All participating surgeons provided voluntary informed consent for anonymous participation and the use of their responses for research and publication purposes.
Results
Participant Characteristics
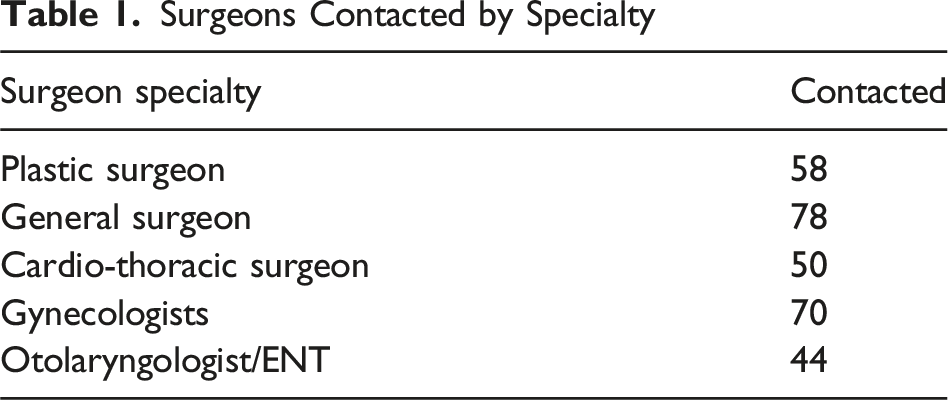
Surgeons Contacted by Specialty
Perceived Value and Adoption Potential
When asked whether the VNH would add value in routine surgical practice, 56% of participating surgeons responded affirmatively, indicating that they perceived benefit compared with conventional needle holders. These respondents frequently cited potential utility in procedures requiring precision in confined spaces, including vascular anastomoses, deep pelvic suturing, and oropharyngeal surgery. An additional 33% indicated that they would be able to judge device’s usefulness only after hands-on use during live operative procedures. This response reflects a pragmatic perspective in which conceptual appeal and bench-top demonstration were viewed as encouraging, but not sufficient for definitive clinical endorsement. A minority (11%) did not perceive additional benefit, suggesting that for some experienced users, conventional needle holders already meet their ergonomic and technical needs. This group tended to view the VNH as situational rather than universally necessary as shown in Figure 2. Perspective of surgeons on VNH significance in routine surgeries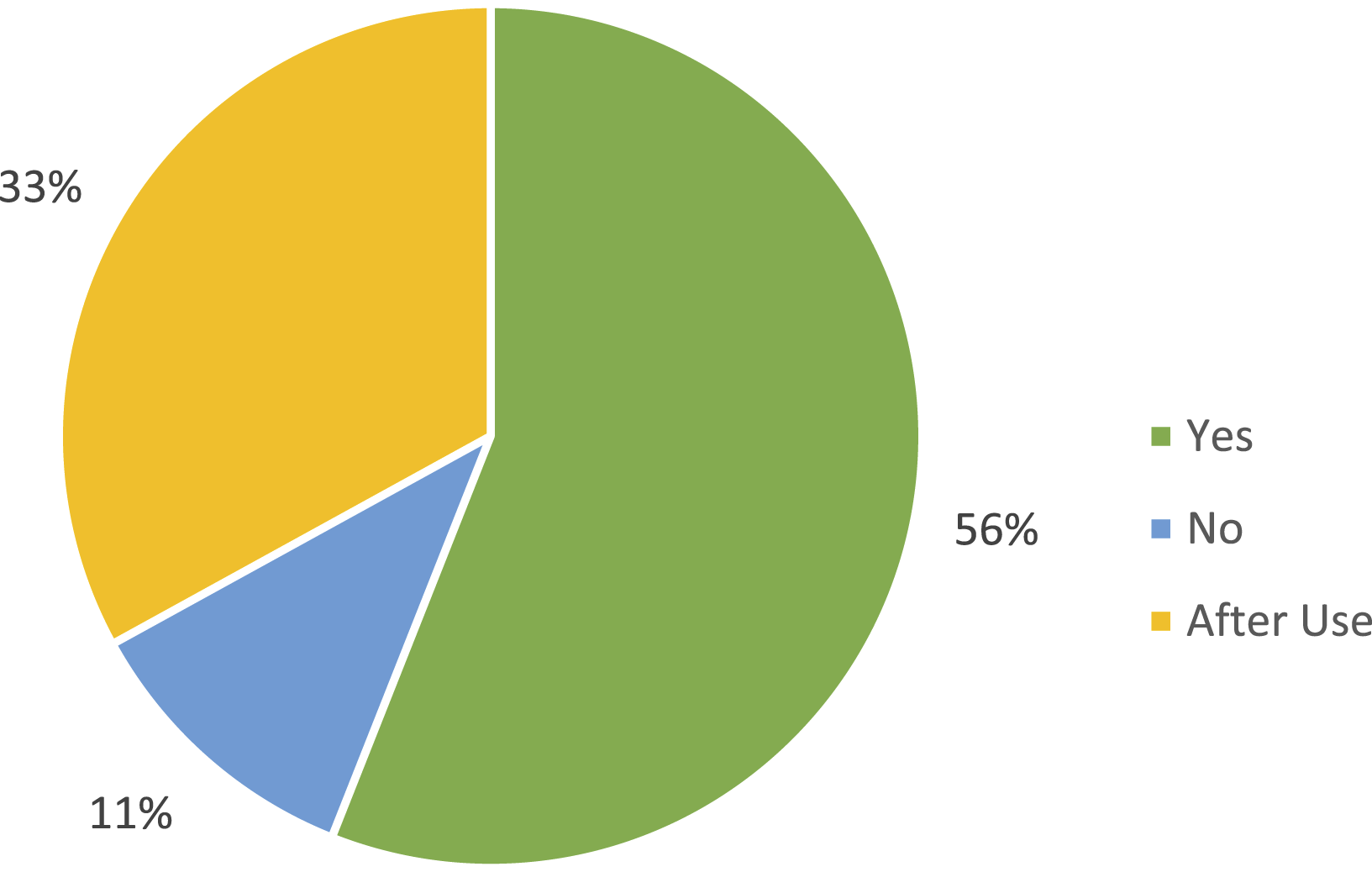
With respect to perceived accuracy and precision, 62% of participants reported that the VNH offered an advantage over conventional needle holders. Surgeons in this group highlighted the straighter needle trajectory and reduced off-midline deviation as perceived benefits, particularly when operating near delicate structures or within restricted anatomical spaces. Approximately 12-13% of respondents expressed uncertainty or skepticism, noting either satisfactory performance with existing instruments or the need for further evaluation under live operative conditions. As illustrated in Figure 3, these findings suggest a predominantly positive perception accompanied by appropriate professional caution. Perspective of surgeons regarding accuracy and precision of VNH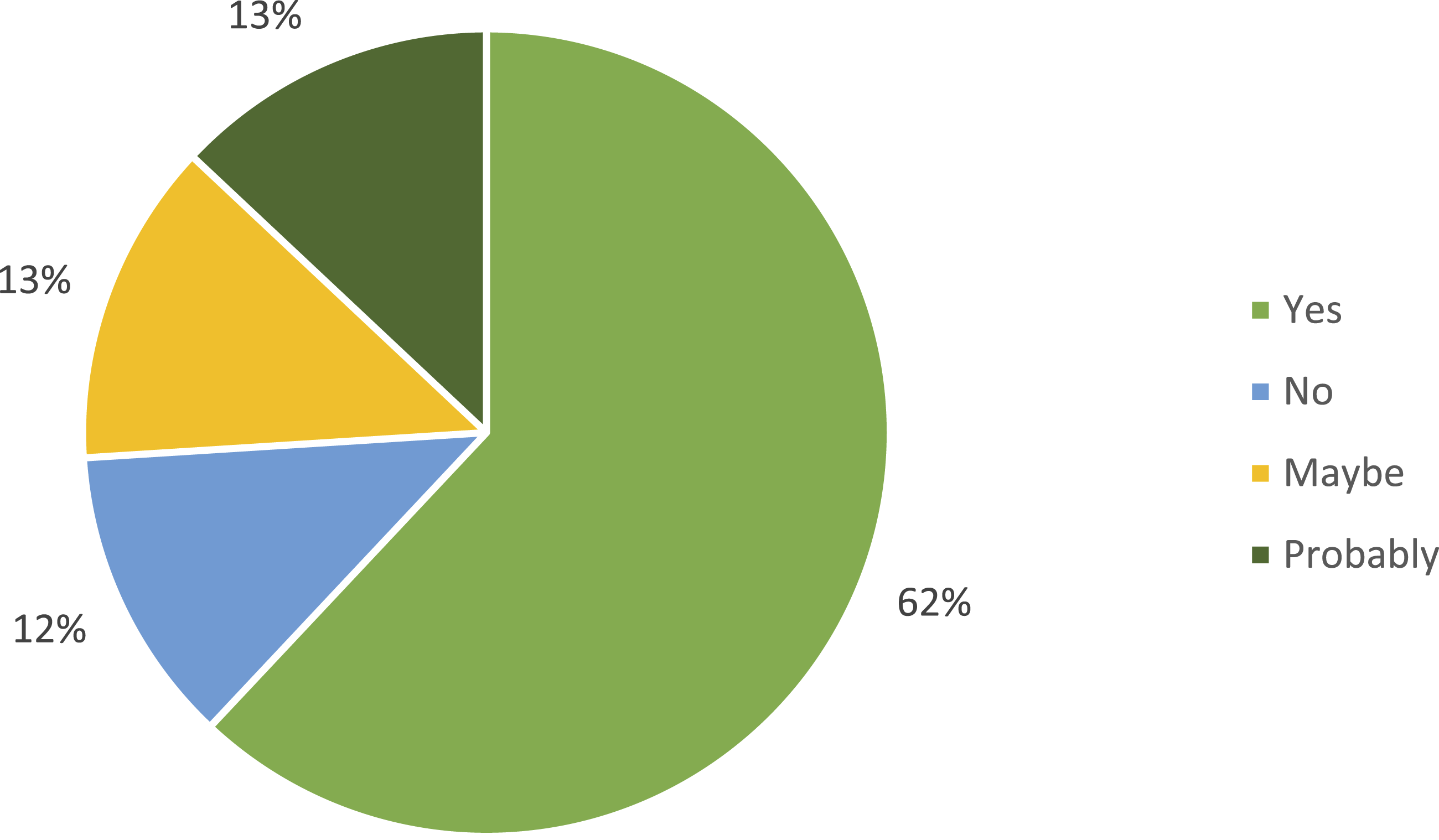
Regarding reach and access, 30% of surgeons identified superior access as a definite advantage of the VNH, particularly in deep or narrow operative fields such as the pelvis, retroperitoneum, or base of the tongue. An additional 30% regarded enhanced reach as a probable benefit as shown in Figure 4. Collectively, these responses indicate that more than half of participants perceived immediate potential value, while a substantial minority reserved judgment pending further clinical experience. Surgeons view on benefits of VNH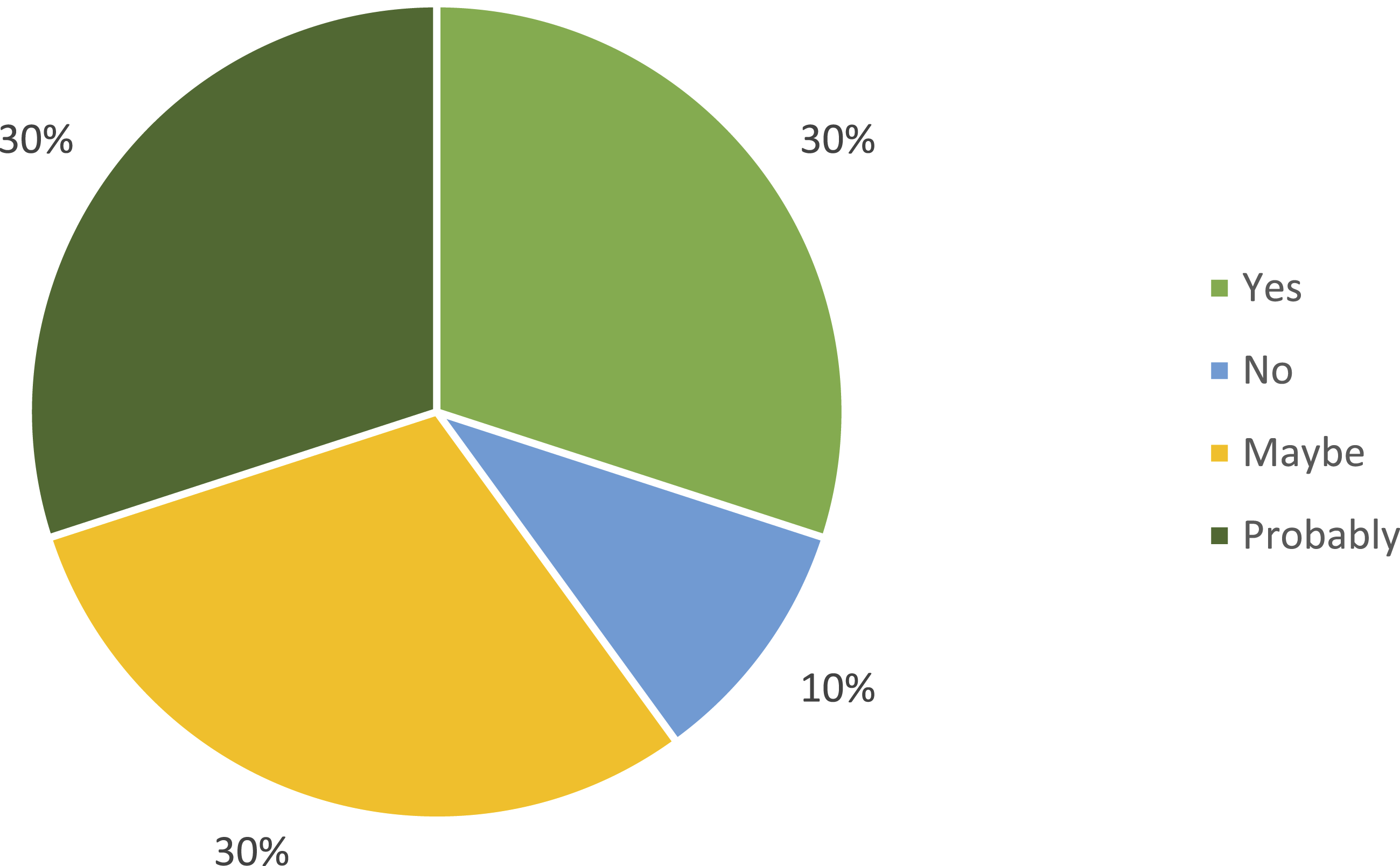
Reported Advantages
Across surgical specialties, several consistent themes emerged from surgeon-reported feedback. Participants noted that the VNH facilitated a straighter perceived needle trajectory and reduced reliance on wrist pronation or supination during suturing. Reported advantages included perceived improvements in precision within confined spaces, enhanced ergonomic comfort associated with a more neutral wrist posture, and an intuitive learning curve, particularly for junior trainees. These impressions were based on subjective assessment during demonstration and practice suturing and were not derived from objective biomechanical measurement. No mechanical failures, needle slippage, or loss of control were reported during the demonstration sessions.
Critical Feedback and Reservations
Despite generally favorable impressions, participants identified several limitations. The most common concern related to the learning curve, as some surgeons felt that adapting to a vertical needle-driving motion differed from long-standing suturing habits. Others questioned whether perceived ergonomic and precision advantages would translate into meaningful reductions in operative time during complex procedures. Several participants suggested that the VNH may be most useful as an adjunct or backup instrument for particularly difficult sutures rather than as a complete replacement for conventional holders. Many respondents emphasized the importance of controlled, side-by-side comparisons with standard instruments to better define the specific clinical scenarios in which the VNH offers a measurable advantage.
Qualitative Feedback
Open-ended survey responses reinforced these themes. Some surgeons described the VNH as “an interesting innovation that could be used in open or minimally invasive surgery” and highlighted its potential to “improve spatial access and visualization.” Others adopted a more cautious stance, noting that while the mechanism appeared intuitive, “practical advantages would only become clear during live surgical use.” Several respondents identified specialty-specific applications, including tonsillar pillar suturing, excision of anal lesions, and deep pelvic dissection, where a straight-line needle trajectory could be particularly advantageous.
Contemporary Synthetic-Tissue Findings (2023-2024)
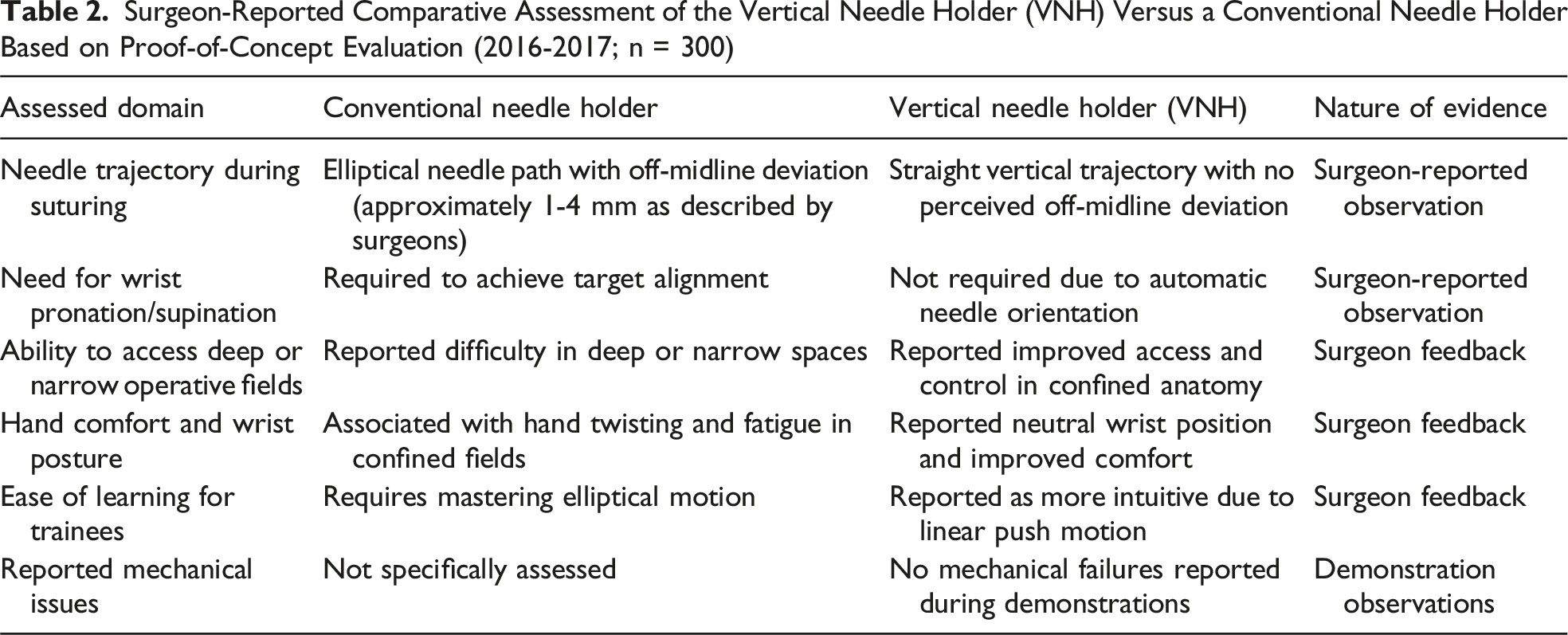
Surgeon-Reported Comparative Assessment of the Vertical Needle Holder (VNH) Versus a Conventional Needle Holder Based on Proof-of-Concept Evaluation (2016-2017; n = 300)
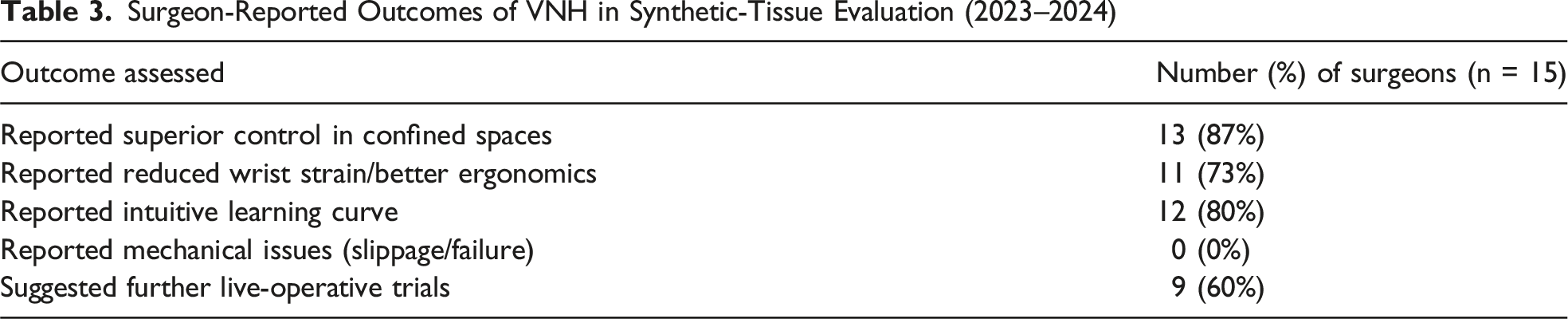
Surgeon-Reported Outcomes of VNH in Synthetic-Tissue Evaluation (2023–2024)
Discussion
Key Findings and Clinical Implications
The Vertical Needle Holder (VNH) demonstrated several perceived advantages compared with conventional needle holders. Surgeons from multiple specialties consistently reported improved precision, greater ergonomic comfort, and enhanced ease of use in confined surgical spaces. These findings are based on surgeon-reported assessments obtained during standardized demonstrations and synthetic-tissue suturing tasks. Participants perceived a straighter needle trajectory, improved control during perpendicular needle entry, and reduced reliance on wrist pronation or supination when using the VNH. Reported comfort and steadiness were also higher compared with conventional instruments.
The clinical implications of these perceived advantages are potentially meaningful. Even small deviations in needle placement may be critical in microsurgical and anatomically constrained contexts where proximity to delicate structures such as vessels and nerves leaves little margin for error.7,8 Surgeons also reported improved control during tissue penetration, which may have implications for tissue handling in vascular and reconstructive procedures where excessive manipulation can compromise outcomes. 9 From an ergonomic perspective, musculoskeletal strain and repetitive wrist motion are well-recognized contributors to surgeon fatigue and occupational injury, and instruments that promote a neutral wrist posture may help mitigate this burden. 10 However, these ergonomic implications remain inferential and warrant objective validation.
Comparison with Existing Innovations
Previous approaches to improving suturing in confined spaces have included articulating laparoscopic needle drivers and robotic platforms. 11 While these systems provide enhanced dexterity and trajectory control, they are often associated with higher costs, increased technical complexity, and steeper learning curves, which may limit accessibility and widespread adoption, particularly outside minimally invasive settings. 12 The VNH offers a more straightforward alternative that preserves the tactile familiarity of conventional open surgical instruments while mechanically guiding needle along a straight trajectory. This balance between innovation and familiarity may facilitate adoption, as substantial deviations from established psychomotor patterns can hinder acceptance among practicing surgeons. 13
Strengths of the Study
A major strength of this evaluation is the inclusion of surgeon-reported outcomes from a large, multispecialty cohort. Participation from general surgery, gynecology, plastic surgery, otolaryngology, vascular surgery, and cardiothoracic surgery supports the broad potential applicability of the VNH across diverse procedural contexts. The supplementary synthetic-tissue evaluation further strengthens the study by demonstrating consistency of surgeon perceptions across two separate timeframes using the same instrument design.
Limitations and Critical Appraisal
Several limitations should be acknowledged. First, surgeon feedback was collected immediately following demonstrations and practice suturing, introducing the possibility of a novelty effect that may have influenced positive perceptions. Second, the learning curve associated with the VNH was not formally quantified. Although many participants described the device as intuitive, repeated-measures studies would be required to determine how rapidly proficiency is achieved and sustained. Third, outcomes related to precision, ergonomics, tissue handling, and task completion time were based on subjective assessment rather than direct biomechanical or motion-based measurements. Wrist angles, muscle activity, tissue displacement forces, and needle trajectory were not objectively quantified and therefore should be interpreted as perceived rather than measured advantages.
Future Directions
Findings from 2023-2024 synthetic-tissue evaluation reinforce and extend the original 2016-2017 proof-of-concept survey, suggesting consistent surgeon-reported usability and perceived ergonomic benefits across two distinct time periods. Nevertheless, the original proof-of-concept data are now nearly a decade old, and updated clinical validation in live operative environments remains essential. Future studies should incorporate objective performance metrics, including motion tracking, force measurement, and ergonomic assessment tools such as electromyography, to substantiate perceived advantages. Longitudinal studies across varying levels of surgical experience would also help define learning curves and adoption patterns. Finally, cost-effectiveness analysis will be important to clarify the value proposition of the VNH relative to conventional instruments and advanced robotic systems.
Conclusion
The Vertical Needle Holder represents a pragmatic innovation in suturing instrumentation aimed at addressing challenges encountered in confined surgical fields. Surgeon-reported findings suggest that the VNH may improve perceived needle control, ergonomic comfort, and ease of suturing while preserving the familiar mechanics of conventional needle holders. As a proof-of-concept evaluation, these findings highlight the potential utility of the device but do not establish definitive performance superiority. The ultimate role of the VNH in surgical practice will depend on future clinical studies incorporating objective ergonomic, biomechanical, and outcome-based validation.
Supplemental Material
Footnotes
Acknowledgments
The authors acknowledge that all participants were informed of the research purpose and voluntarily provided consent to participate. Their contributions provided critical insights into the usability and potential clinical applications of the instrument.
Ethical Considerations
Ethical approval was not required for this study because it involved demonstrations of a surgical instrument with volunteer surgeons and did not include patients, patient data, or human tissue. The study complied with institutional and international research ethics standards.
Consent to Participate
All participating surgeons provided informed consent prior to the instrument demonstration and survey.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received initial financial support from the Sabah Al-Ahmad Center for Giftedness and Creativity at the beginning of the project. No additional funding was obtained for the extended evaluation phase. The work was otherwise conducted without specific grant support from any public, commercial, or not-for-profit funding agency.
Declaration of Conflicting Interests
The authors declare the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Hasan Alshemari holds U.S. Patent No. 8,535,348 B1 for the Vertical Needle Holder (VNH) discussed in this study. The patent holder authorized the reporting of this study. All other authors declare no competing interests.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.