
Abstract
Background
This study aimed to evaluate the effectiveness of unilateral external oblique intercostal nerve block (EOIB) in laparoscopic cholecystectomy surgery.
Material and Methods
After ethics committee approval, ASA I-II patients aged 18-70 who would undergo laparoscopic cholecystectomy surgery were included in the study. The patients were divided into two groups, external oblique intercostal nerve block (Group EOIB) and oblique subcostal transversus abdominis plane block (Group OSTAP). After surgery, EOIB or OSTAP block was administered with 20 mL of .25% bupivacaine then routine analgesia protocol was applied with iv paracetamol, and tramadol. Visual analog scale (VAS) scores and patient-controlled analgesia (PCA) consumption were monitored 24 hours after the operation. It was administered 25 mg pethidine as a rescue analgesic to patients with VAS ≥4.
Results
Thirty six patients for Group EOIB and thirty four patients for Group OSTAP were included in the study. Lower VAS scores were observed in all groups. When PCA consumption, side effects, rescue analgesia consumption, and patient satisfaction were evaluated, there was no statistically significant difference between the groups (P > .05).
Conclusion
It was observed that EOIB showed similar analgesic activity to the OSTAP block. EOIB may also be a part of postoperative multimodal analgesia by reducing postoperative opioid consumption in LC.
Introduction
Laparoscopic cholecystectomy (LC) surgery is a minimally invasive surgical procedure that causes less postoperative pain than conventional open surgeries. 1 In the literature, opioids and nonsteroidal anti-inflammatory drugs have effectively treated postoperative pain after LC surgery. In addition, there are many studies in which regional anesthesia techniques are used as a part of multimodal analgesia.2–4
Oblique subcostal transversus abdominis plane block (OSTAP), one of the regional anesthesia techniques, is used in middle and upper abdominal surgeries.5,6 OSTAP blocks the T6-9 intercostal nerves between the rectus abdominis and transversus abdominis muscle. Many studies have shown that OSTAP block reduces the postoperative analgesic and opioid requirement and improves the quality of postoperative pain control.2,3,7–9 Some studies have shown that it will be ineffective in abdominal organs and parietal peritoneal surgeries with the performance of OSTAP block targeting the analgesia of the upper abdominal wall.5,10
The innervation of the upper abdominal wall originates from the T6th and T10th intercostal nerves and requires effective blocking of these nerves to achieve analgesic and anesthetic efficacy. 11 Hesham Elsharkawy et al demonstrated the potential mechanism of the external oblique intercostal fascial plane block (EOIB) in a cadaver study in which both lateral and anterior branches of the intercostal nerves T7–T10 were stained. 12 Patients to whom this block was applied exhibited consistent dermatomal sensory blockade between T6-T10 in the anterior axillary line and T6-T9 in the midline. It has been shown that this block can be used in the clinical setting for upper abdominal wall analgesia.10,12
No study investigating the efficacy of EOIB and OSTAP block in LC surgeries has been identified in the current review of the relevant literature. In this study, our primary aim was to evaluate the effect of unilateral EOIB and OSTAP on postoperative pain scores in LC surgery. Our secondary aim was to evaluate analgesic consumption, side effects, and patient satisfaction.
Methods
This randomized and prospective study was conducted in our hospital’s general surgery clinic and operating room between 1st of the May and 31th of the December in 2022, after approval (2022/51) from the local ethics committee. Seventy six patients, ASA I-II, aged 18-70 years, who had undergone LC surgery were included in the study. Patients with known severe heart, kidney, liver, life-threatening hematological diseases, neurological disease, psychiatric disorder, drug allergy or history of allergy to amide-type local anesthetics, infection at the intervention site, bleeding diathesis, within 24 hours before the operation Patients with a history of narcotic drug use, chronic pain, narcotic substance or alcohol addiction and who refused to participate in the study were excluded from the study. The patients were randomized by the closed envelope method and divided into Group OSTAP (Bupivacaine .25% 20 mL) and Group EOIB (Bupivacaine .25% 20 mL).
Management of anesthesia, Surgery, and Interfascial Plane Blocks Administration
The patients were taken to the operating room. Electrocardiography (ECG), noninvasive arterial blood pressure (NIBP), and pulse oximeter oxygen saturation (SpO2) monitoring were performed. Anesthesia was induced with 2 mg iv midazolam, 2 mg/kg iv propofol, .6 mg kg−1 iv rocuronium, and 2 mcg kg−1 iv fentanyl. Anesthesia was maintained using sevoflurane at MAC 1 concentration with 50% O2-50% air and remifentanil .25-1 mcg/kg/min by evaluating the hemodynamic response.
In both groups, surgeries were performed under laparoscopic technic. Carbon dioxide (CO2) pneumoperitoneum was administered gradually, ranging from 2 to 4 liters per minute, to mitigate adverse hemodynamic responses and minimize right shoulder discomfort. The pneumoperitoneum was maintained below a maximum threshold of 12 mmHg. The surgical approach involved three trocar incisions, resulting in a total of three ports: one umbilical port, one subxiphoid port, and a right subcostal ports. Only the fascia at the umbilical trocar sites was closed by the surgeon in the patients. Laparoscopic cholecystectomy (LC) was uniformly performed utilizing identical techniques by the same surgeon across all patients.
In the OSTAP block, 20 mL of bupivacaine .25% was applied to the fascia between the rectus abdominis and transversus abdominis muscles, accompanied by a linear ultrasound probe (Xperius®, BBraun Medical Ltd,). For EOIB, 20 mL of bupivacaine .25% was applied to the tissue plane between the external oblique and intercostal muscles and between the sixth and seventh ribs by placing the linear ultrasound probe on the sagittal plane between the midclavicular and anterior axillary lines at the level of the sixth rib. For this study, all blocks were performed in the supine position at the end of surgery and before patients woke up. Postoperatively, the muscle relaxant effect was antagonized with 2 mg kg−1 iv sugammadex. After all extubation criteria were met, the patients were extubated and taken from the operating room to the recovery room. (Figure 1) (A) The positioning of the patient and the ultrasound probe for the External Oblique Intercostal Plane Block procedure. (B) The ultrasonographic image illustrating the intervention.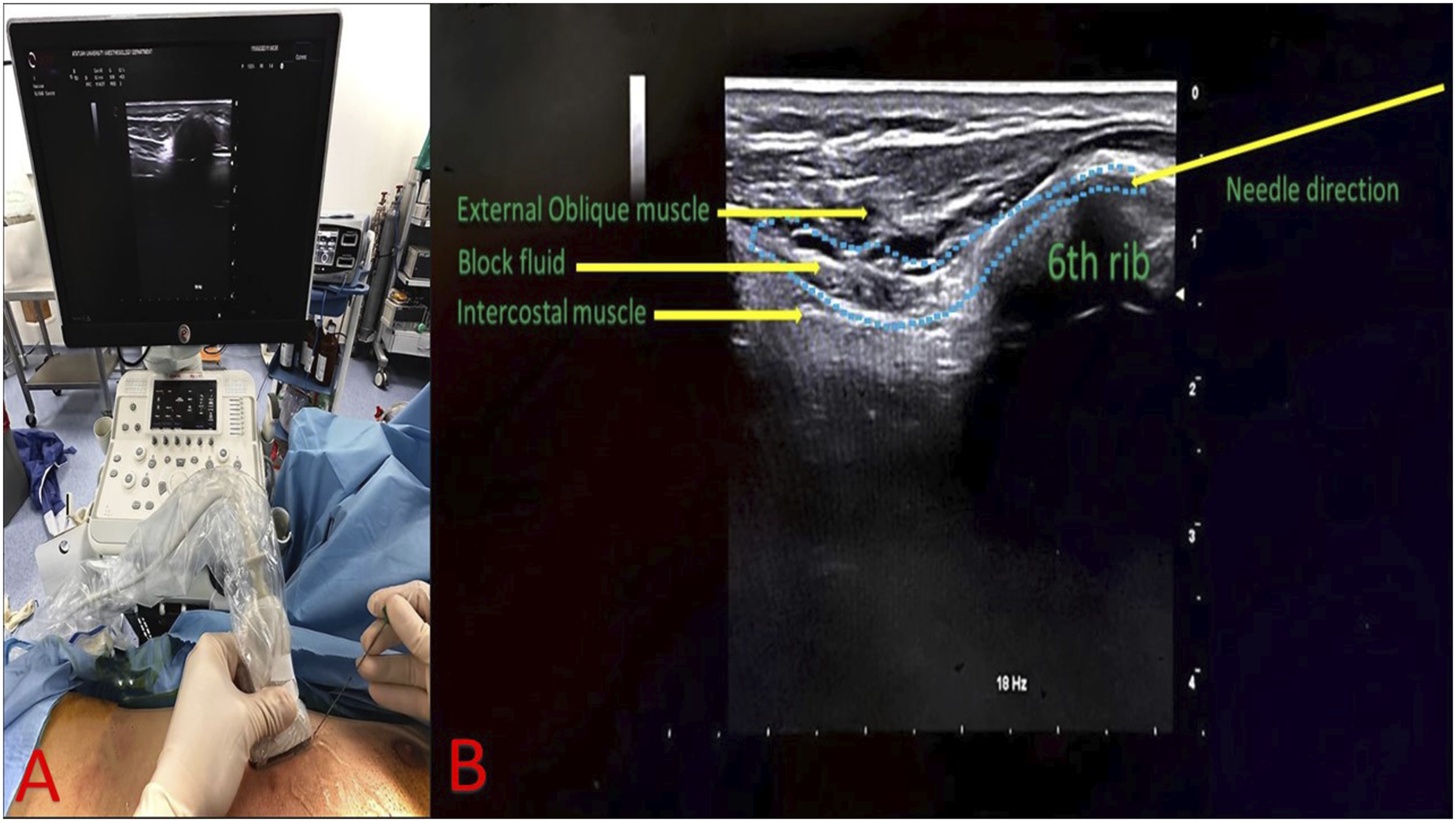
Postoperative Analgesic Management
Perioperatively, 1 g paracetamol iv and 100 mg tramadol iv in 100 mL saline was administered to each patient as part of their routine pain management regimen for 20 minutes. As postoperative analgesics, 1 g paracetamol iv every 8 hours and tramadol (without basal infusion, 15 mg iv bolus, 15 min locking) with a patient-controlled analgesia (PCA) device were administered. Patients with VAS ≥4 were given 25 mg pethidine iv as a rescue analgesic.
As a primary outcomes of the study postoperative pain was assessed at 1st, 2nd, 4th, 6th, 8th, 12th, 18th, and 24th hours using VAS scores (VAS 0 = no pain; VAS 10 = worst possible pain). As a secondary outcome of the study postoperative tramadol consumption was recorded as 0-4, 4-8, 8-16, 16-24 hours time intervals, and 24-hour total values. Time to first analgesic requirement (minutes)” was defined as the time elapsed between administration of the block and VAS pain score ≥4. Opioid-related postoperative nausea and vomiting have been noted. Patient satisfaction was classified as excellent/good/moderate/poor.
Statistical Analysis
Data from a preliminary study taking into account the total tramadol consumption parameter [Group OSTAP (n:6): 99.38 ± 45.21, Group EOIB (n:6): 74.2 ± 35.32] was used to calculate a minimum sample size of 33 participants per group (type 1 error = .05, type 2 error = .20, and power = .80). The final decision was taken to include 36 patients per group, taking into account possible losses to follow-up.
This study analyzed the data using the SPSS 25 (Armonk, NY: IBM Corp.) program. Median (Q1-Q3-IQR) were used for descriptive statistics. Kolmogorov Smirnov test was used to evaluate the distribution of the data. The student-t test was used to evaluate parametric data, and the Mann-Whitney U test was used to evaluate nonparametric data. Chi-square (Pearson, Yates, Fisher’s Exact, and Likelihood ratio) tests were used to analyze categorical data. The significance level for all tests was determined as P < .05.
Results
Seventy six patients were included in this study. One patient was excluded from the study because of didn’t meet the inclusion criteria and one patient didn’t want to be included in the study. Seventy four patients were randomized for study. One patient in Group EOIB was excluded because of a change in operating procedures to open surgery, one patient in Group OSTAP for reoperation, and 2 patients for conversion to open surgery. Therefore, 36 patients in Group EOIB and 34 patients in Group OSTAP were included in the study. (Figure 2) CONSORT flow diagram.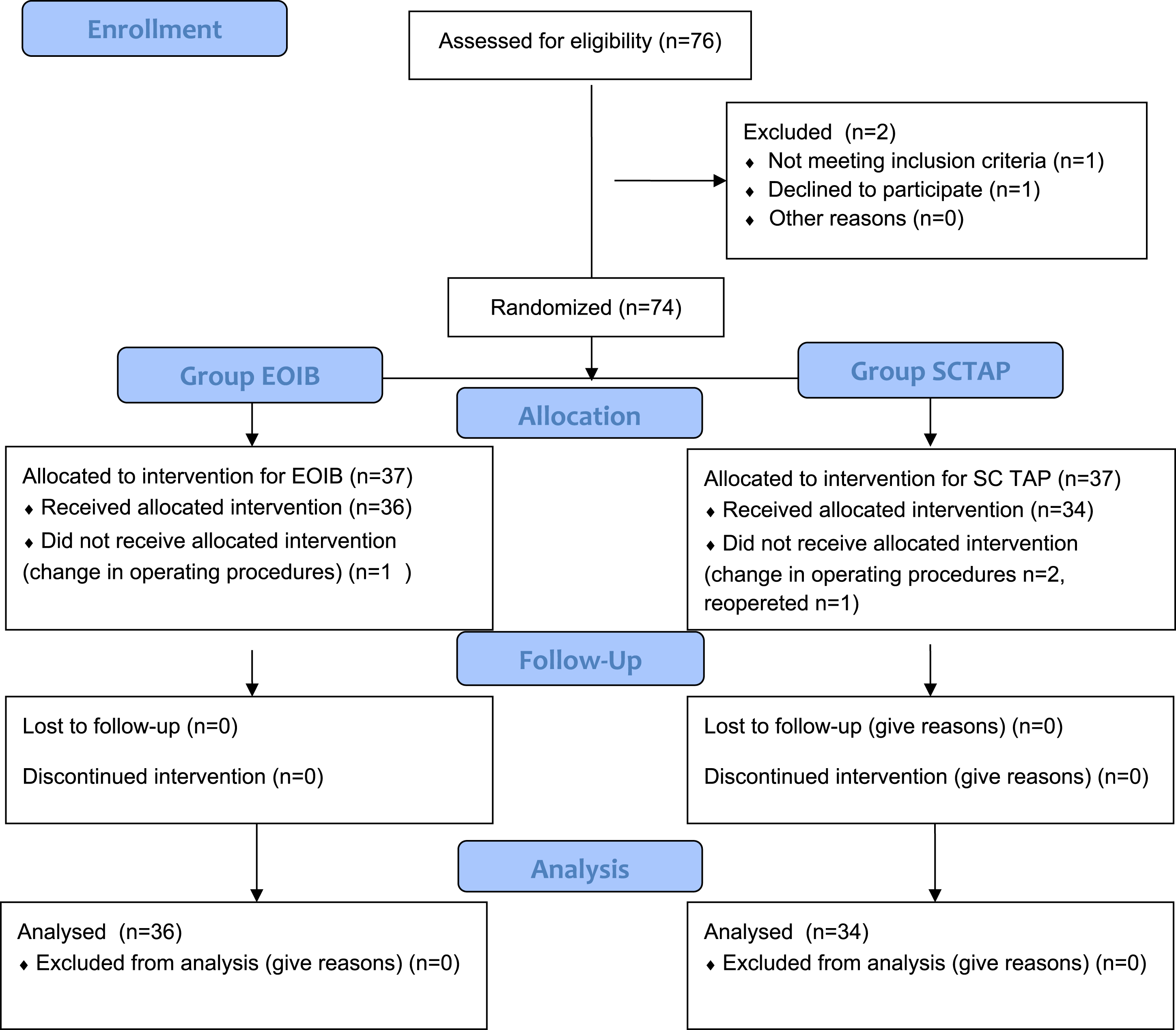
Comparisons of the Demographic Variables Between Groups.
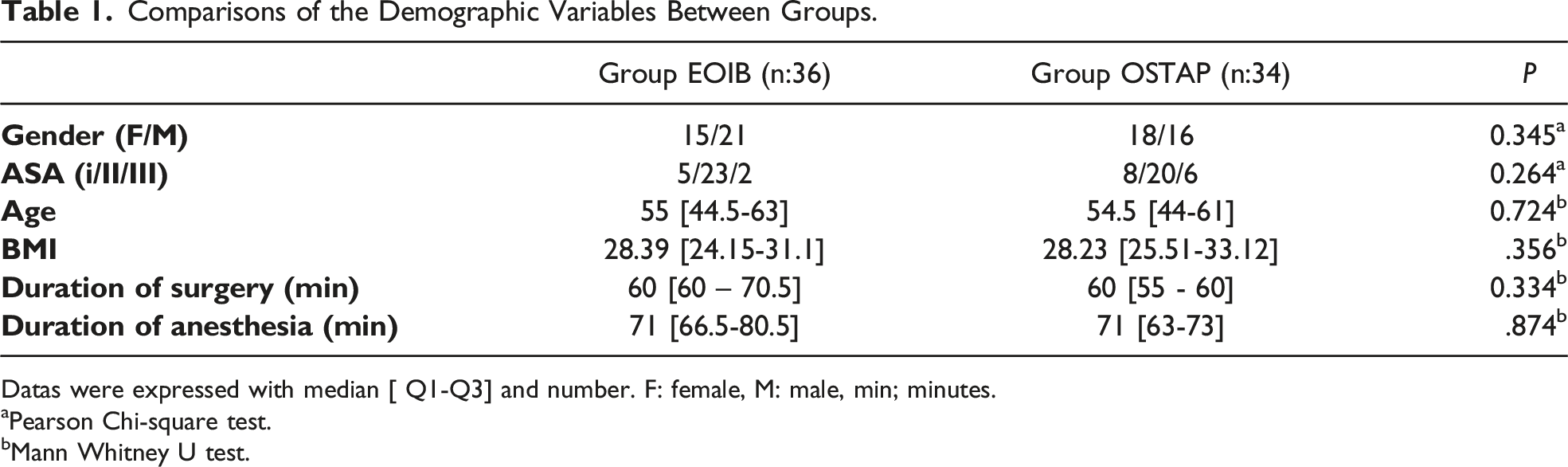
Datas were expressed with median [ Q1-Q3] and number. F: female, M: male, min; minutes.
aPearson Chi-square test.
bMann Whitney U test.
Comparisons of the Tramadol Comsumption Between Groups.
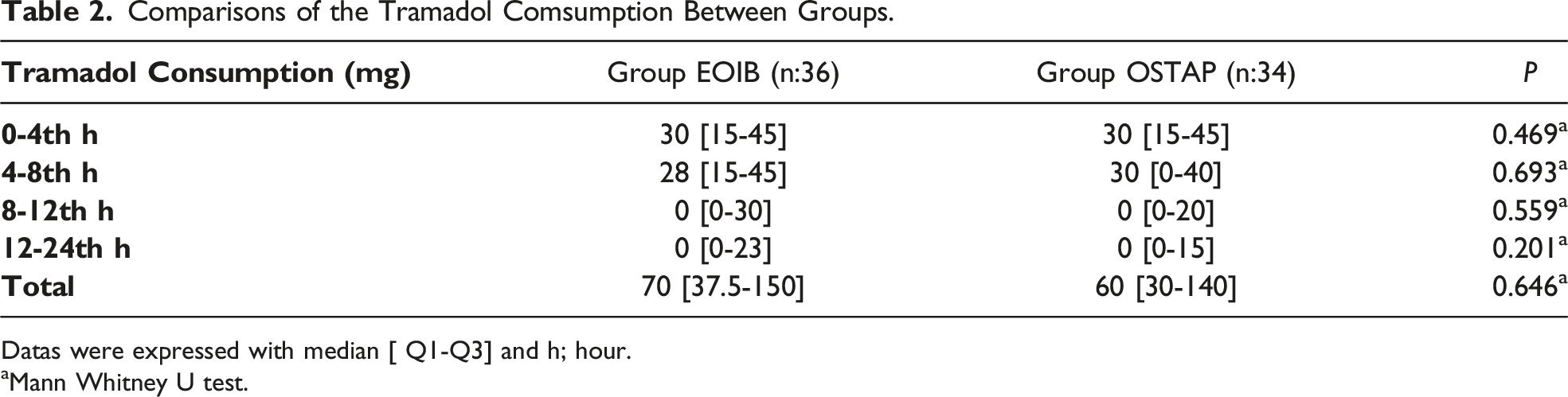
Datas were expressed with median [ Q1-Q3] and h; hour.
aMann Whitney U test.
Comparisons of the VAS Scores Between Groups.
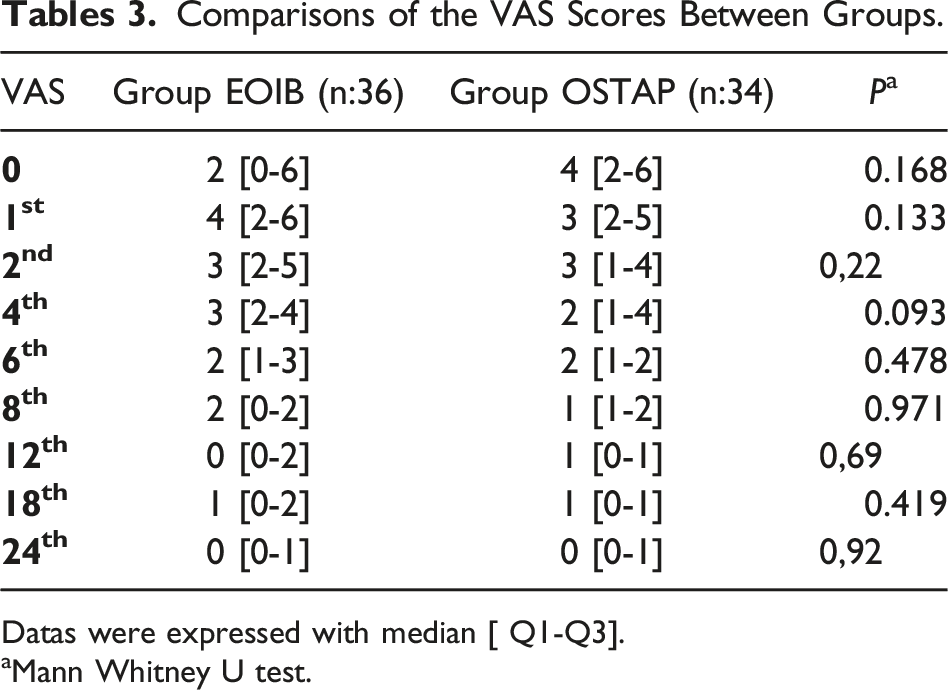
Datas were expressed with median [ Q1-Q3].
aMann Whitney U test.
Comparisons of the Patient Satisfaction, Rescue Analgesic and Side Effects Parameters Between Groups.
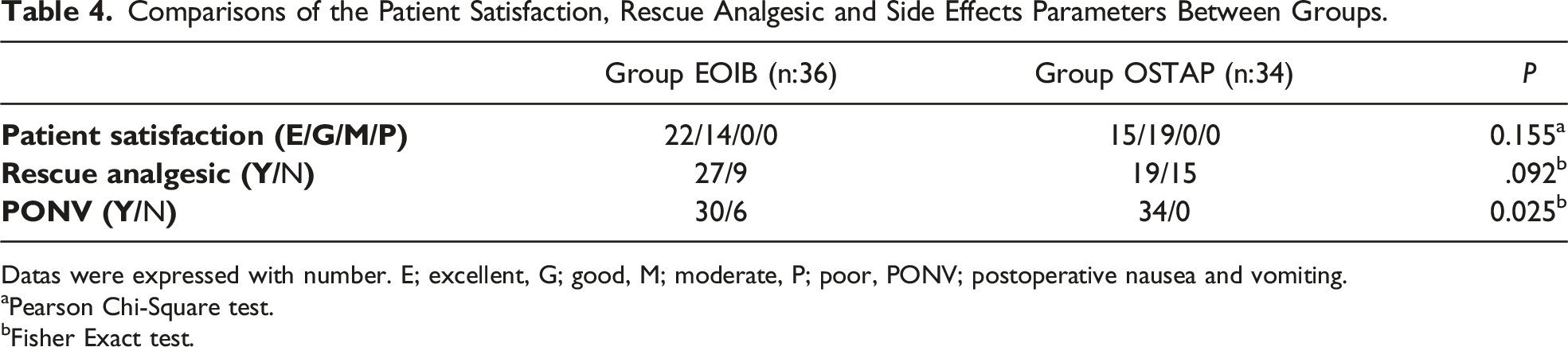
Datas were expressed with number. E; excellent, G; good, M; moderate, P; poor, PONV; postoperative nausea and vomiting.
aPearson Chi-Square test.
bFisher Exact test.
Although postoperative nausea and vomiting (PONV) was seen in 6 patients in the EOIB group, it was not seen in the OSTAP group (P < .05). There was no statistically significant difference between the groups in the evaluation of patient satisfaction between the two groups (P > .05) (Table 4). No further complications or exclusion criteria were identified among the patients.
When the rescue analgesic requirement was evaluated, it was observed that more patients in the OSTAP group (n:19) compared to the EOIB group (n:24) needed analgesics at the end of the first 2 hours. During the time period after the 2nd hour, more patients in the EOIB group compared to the OSTAP group required analgesic medication. (End of the 24 hour Group EOIB n:27 - Group OSTAP n:19). (Figure 3) Kaplan-Meier curve and table showing patients’ first analgesic requirement according to time intervals.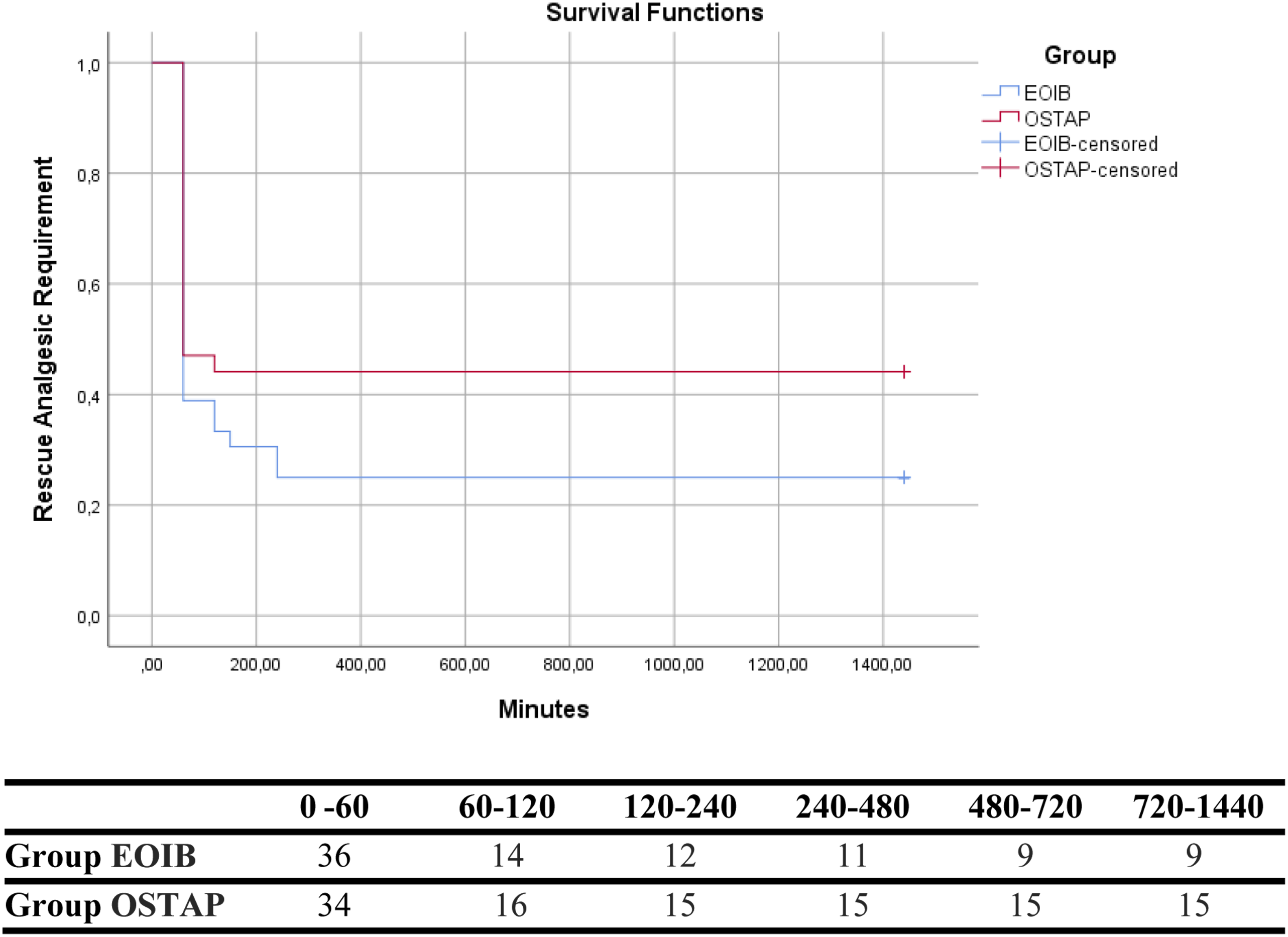
Discussion
As a result of the study, EOIB group has no superiority over OSTAP group in terms of pain scores and has the same analgesic efficacy. At the same time, no difference was observed between VAS scores, opioid consumption, time to first analgesia, rates of rescue analgesia use, and patient satisfaction rates in both groups.
Understanding the trigger and source of postoperative pain in LC surgery is essential. In addition to the somatic pain caused by the surgical incision, patients also suffer from visceral pain. Trocar access incisions, gallbladder resection, and peritoneal distension cause somatic pain. Meanwhile, sources of visceral pain are diaphragm irritation due to high intra-abdominal pressure and distension of CO2 insufflation.13,14 Despite the reduction in surgical times and the fact that laparoscopic procedures are performed under lower insufflation pressures, postoperative pain still needs to be effectively treated in LC surgery.
Ting Li et al. reported that upper abdominal surgeries were more painful and required more opioids postoperatively than lower abdominal surgeries. 15 Therefore, postoperative pain management is more critical in upper abdominal surgeries. At this point, fascial plane blocks can be a savior. Despite multiple facial plane blocks, only OSTAP, EOIB, and their modifications target the upper abdominal wall.
Upon evaluating the literature, there is one study examining the effectiveness of the EOIB block in laparoscopic cholecystectomy surgeries. This study demonstrates that the use of the EOIB block is associated with lower opioid consumption compared to multimodal analgesia without EOIB. 16 No study in the literature compares EOIB and OSTAP block in LC surgery. Many clinicians currently use OSTAP as an effective regional anesthesia technique in middle and upper abdominal surgeries. Many studies have shown that OSTAP improves the quality of analgesia and reduces the need for analgesia in LC surgery.2,3 However, a recently published study reported that OSTAP caused a 90% blockage in the mid-abdominal region and 26% of the lateral abdominal surface area, resulting in sensory blockage between the Th7 and Th12 dermatomes. 17 In light of this finding and considering the anatomy of the surgical field, OSTAP may be insufficient in some patients undergoing LC surgery. Many studies report on the bilateral use of OSTAP or its combination with other blocks. 18 However, in a cadaver study, they showed that dye spreading extends to the midaxillary line in a cadaver applied EOIB. Despite all this data, there was no significant difference in VAS scores between the groups in our study. 12 This result shows us that there may be different efficacy in different studies and that the lateral abdominal surface area may be affected by OSTAP block.
Some studies have reported that the lateral cutaneous branches of the intercostal nerves that contribute to the innervation of the upper abdominal wall cannot be reliably blocked by TAP block approaches, including OSTAP block, and that even variants of OSTAP block cannot provide a consistent block of this region.19–21 Namely, injection in the lateral side of the linea semilunaris creates a block centered around T10–T11, and even if it is close to the xiphoid process in the medial of the linea semilunaris, only 50-70% of the procedures spread to T6–T7. 21–24 In both cases, the lateral cutaneous branches are not adequately blocked, limiting the use of the OSTAP block for several abdominal surgical procedures such as nephrectomy, cholecystectomy, or hepatic or gastric surgery. 21 In this study, unilateral OSTAP and EOIB showed similar analgesic efficacy in LC surgery that did not require extensive surgical intervention.
Elsharkawy et al demonstrated the potential mechanism of this technique, with a cadaveric study reporting consistent staining of both the lateral and anterior branches of the intercostal nerves T7-T10. 11 In this retrospective case series, bilateral single-injection EOIB blocks were applied to sixteen patients, and continuous bilateral catheters were used on six patients. Bilateral dermatomal coverage has been shown to extend from the posterior axillary line laterally to the midline medially within 30 minutes of block performance in all patients. The median bilateral sensory dermatomal level obtained was determined as T6-T10 in the anterior axillary and posterior axillary lines and T6-T9 in the midline. This combination case series and a cadaveric study of EOIB noted the continuity between the thoracic and abdominal wall fascial planes, demonstrating the excellent use of this technique to target upper abdominal wall analgesia, an area not adequately covered by the previously described fascial plane. The fact that the EOIB used in the current case series reduces opioid consumption to almost zero may indicate that it will soon be very close to being the first choice as an opioid protective block. 25 In this study, we think that EOIB can be an alternative to OSTAP, which is as analgesic as OSTAP in LC and is challenging to administer in obese patients.
In a study by Shahid et al. comparing the effects of paracetamol and tramadol on postoperative pain, it was seen that tramadol significantly increased the incidence of PONV. 26 Similarly, although there was no significant difference between the two groups in this study, PONC developed in six patients in the EOIB group with a higher tramadol requirement. None of the OSTAP groups had PONV.
There are some limitations in this study. Initially, the extent of routine dermatomal blockade could not be evaluated since all blocks were performed after induction of anesthesia. Secondly, during the evaluation of the VAS score, which measures the patients’ pain level, different factors depending on the investigator and the patient, may have affected the assessment. Thirdly, the block is not performed bilaterally, and with a volume of more than 20 mL, the effectiveness of the procedures may differ. Lastly, the non-inclusion of the Qqr15 scale might be construed as a limitation
In conclusion, EOIB and OSTAP blocks showed similar analgesic and patient satisfaction scores in LC surgery patients. Considering its ease of administration, favorable safety profile, and capacity to mitigate postoperative opioid consumption, EOIB may be regarded as a constituent of multimodal analgesic strategies subsequent to LC. Randomized controlled studies are needed to compare the effectiveness of these blocks for other types of surgery.
Footnotes
Author contributions
MSC, and HS designed the study. MSC, HSB and OK contributed by patients selection and clinical evaluation. ECC and MSC wrote the manuscript. SH and SU helped in performing intraop anesthetic infiltration. ECC, MSC and HS revised the manuscript and statistics.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.