
Abstract
Background
Near-infrared fluorescence imaging (NIRFI) is an increasingly utilized imaging modality, however its use amongst general surgeons and its barriers to adoption have not yet been characterized.
Methods
This survey was sent to Canadian Association of General Surgeons and the Society of American Gastrointestinal and Endoscopic Surgeons members. Survey development occurred through consensus of NIRFI experienced surgeons.
Results
Survey completion rate for those opening the email was 16.0% (n = 263). Most respondents had used NIRFI (n = 161, 61.2%). Training, higher volumes, and bariatric, thoracic, or foregut subspecialty were associated with use (P < .001).
Common reasons for NIRFI included anastomotic assessment (n = 117, 72.7%), cholangiography (n = 106, 65.8%), macroscopic angiography (n = 66, 41.0%), and bowel viability assessment (n = 101, 62.7%). Technical knowledge, training and poor evidence were cited as common barriers to NIRFI adoption.
Conclusions
NIRFI use is common with high case volume, bariatric, foregut, and thoracic surgery practices associated with adoption. Barriers to use appear to be lack of awareness, low confidence in current evidence, and inadequate training. High quality randomized studies evaluating NIRFI are needed to improve confidence in current evidence; if deemed beneficial, training will be imperative for NIRFI adoption.
Introduction
Interest and studies evaluating the utility of intraoperative near-infrared fluorescence imaging (NIRFI) in general surgery disciplines has grown dramatically over the last decade.1,2 For general surgeons, indocyanine green (ICG) NIRFI has increasingly been utilized for a variety of roles including biliary mapping,3-7 evaluation of anastomotic perfusion,8-12 and identification of hepatic tumor margins,13,14 localization of metastatic disease13,15 and lymph nodes,13,16-20 characterization of vascular anatomy,21,22 and ureteric identification.13,23,24 Studies evaluating these techniques and their optimal implementation are ongoing. Despite the evolving interest in NIRFI, the use of ICG technology including its barriers to use, and procedural selection remain poorly characterized thereby potentially limiting its adoption.
Near-infrared fluorescence imaging involves injecting a fluorophore intravenously and illuminating it within the tissue of interest at its absorption wavelength. Novel techniques are also injecting the fluorophore in a submucosal or subserosal region. The intravenous fluorophore will then excite, and emits light at its fluorescent wavelength.2,25 ICG is the most commonly used fluorophore used; with light absorption at 700-800 nm and emittance in the 700-900 nm near infrared-1 (NIR-1) spectrum.25,26 The dye is highly plasma protein bound, therefore remains intravascular, has a half-life of 2-4 minutes, does not have significant uptake into peripheral tissues, and is rapidly excreted into the biliary system.2,25,27 Together, these features allow ICG to be safely injected intra-operatively to allow for a more precise delineation of patient and/or tumor anatomy.
The aim of this study was to develop and implement a survey to characterize current ICG utilization and barriers to use amongst general surgeons. Characterizing differences between adopters and non-adopters, techniques where NIRFI is most commonly used, and barriers to use remains essential to ongoing work evaluating this technology. Considering promising results from current NIRFI studies, this information will enable targeted actions aimed at increasing NIRFI accessibility and utilization.
Methods
This is a voluntary response, electronic survey designed following The American Association for Public Opinion Research (AAPOR) Survey Disclosure Guidelines. 28 The survey was conducted without a supporting sponsor and emailed to general surgeons and general surgery subspecialist members of the Canadian Association of General Surgeons (CAGS) and the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) (n = 3933). The survey sample was used as a surrogate for North American general surgeons. The study protocol was reviewed and approved by the University of Alberta Research Ethics Board (REB: Pro00105472).
Survey development occurred through consensus of 3 surgeons experienced with NIRFI; the final survey is presented in Supplementary Material 1. The survey was developed to differentiate surgeons who utilize NIRFI (adopters) and those who do not (non-adopters) and to characterize NIRFI access, use, and barriers to use for specific general surgery procedures. The survey was distributed online through email marketing software (Mailchimp 29 ) in order to collect statistics on number of surgeons who opened emails, clicked on the survey link, and to identify surgeons who were sent a reminder email. Initial emails were sent on May 7th, 2021 with a subsequent reminder email sent May 25th, 2021. The online survey was available until July 1st, 2021. Survey responses were collected and managed using REDCap electronic data capture tools hosted at University of Alberta, a secure and encrypted platform that anonymized participant’s responses.30,31
Participants were identified through publicly available membership lists for the CAGS and SAGES. Identified surgeons with available emails were included in this study and data was collected regarding their city, state, country, and surgical subspecialty. The survey was constructed to identify surgeons who have used ICG (ICG-adopters), those who have not used ICG but have access (non-adopters with access), and non-users who do not have access to ICG technologies (non-adopters without access). Results from the survey including ICG use and barriers are presented as per these user categories.
Categorical data were expressed as absolute counts with percentages. No continuous data was presented. Normality testing was performed with the D’Agostino-Pearson normality test to determine the need for non-parametric testing, which was utilized for all subsequent analyses. Bivariate between group comparisons were carried out using the non-parametric Fisher’s exact test where appropriate. Where multiple between-group comparison was performed, data was analysed using the Kruskal–Wallis test. ICG-adopters and non-adopters, with and without ICG access, were defined a priori with the survey developed to identify these surgeons. Statistical significance was set at an alpha of .05. Statistical analysis was performed using STATA 17 (StataCorp, College Station, TX, USA).
Results
Survey Engagement
The initial survey was emailed to 3933 surgeons, of which 1641 (41.7%) opened the email. After the initial distribution, 251 (6.4%) surgeons opened the survey and 180 (4.6%) fully completed all questions. Following a reminder email, the total number of surgeons who opened the survey increased to 387 (9.8%), with 275 (7.0%) completing the survey. Survey response rate for those that opened the email was 16.8% and there were 51 (1.3%) asked to be unsubscribed from further emails. Of survey respondents, 12 (4.4%) did not adequately complete the survey and were excluded from analysis, leaving 263 (95.6%) surgeons who consented and adequately completed the survey (16.0% of those that opened the email, Figure 1). Breakdown of surgeons included in survey defining those who were emailed, opened the email, opened the survey, and that adequately completed the survey (ie survey respondents). *Survey respondents includes those who completed the survey adequately. An additional 12 surgeons did not adequately complete the survey and were excluded from analysis.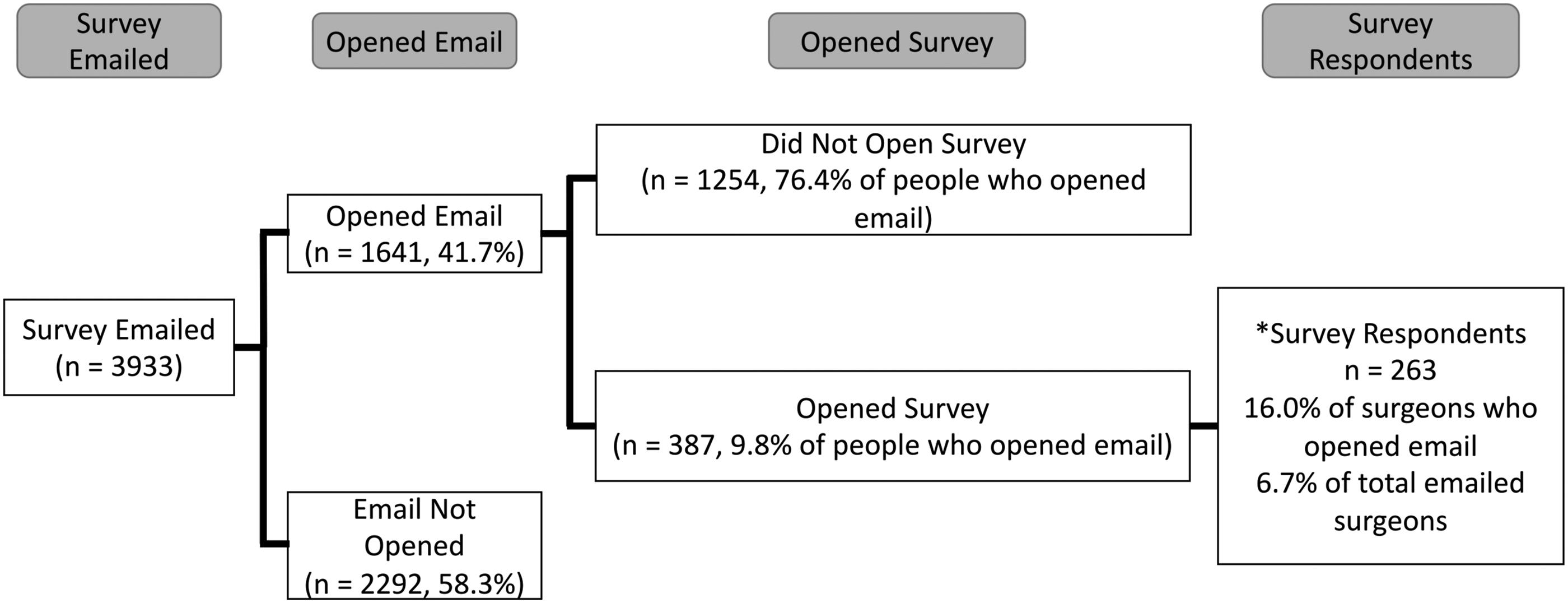
Respondent Demographics
Surgeon Demographics and Relationship to Intraoperative Near-Infrared Fluorescence Imaging Use.
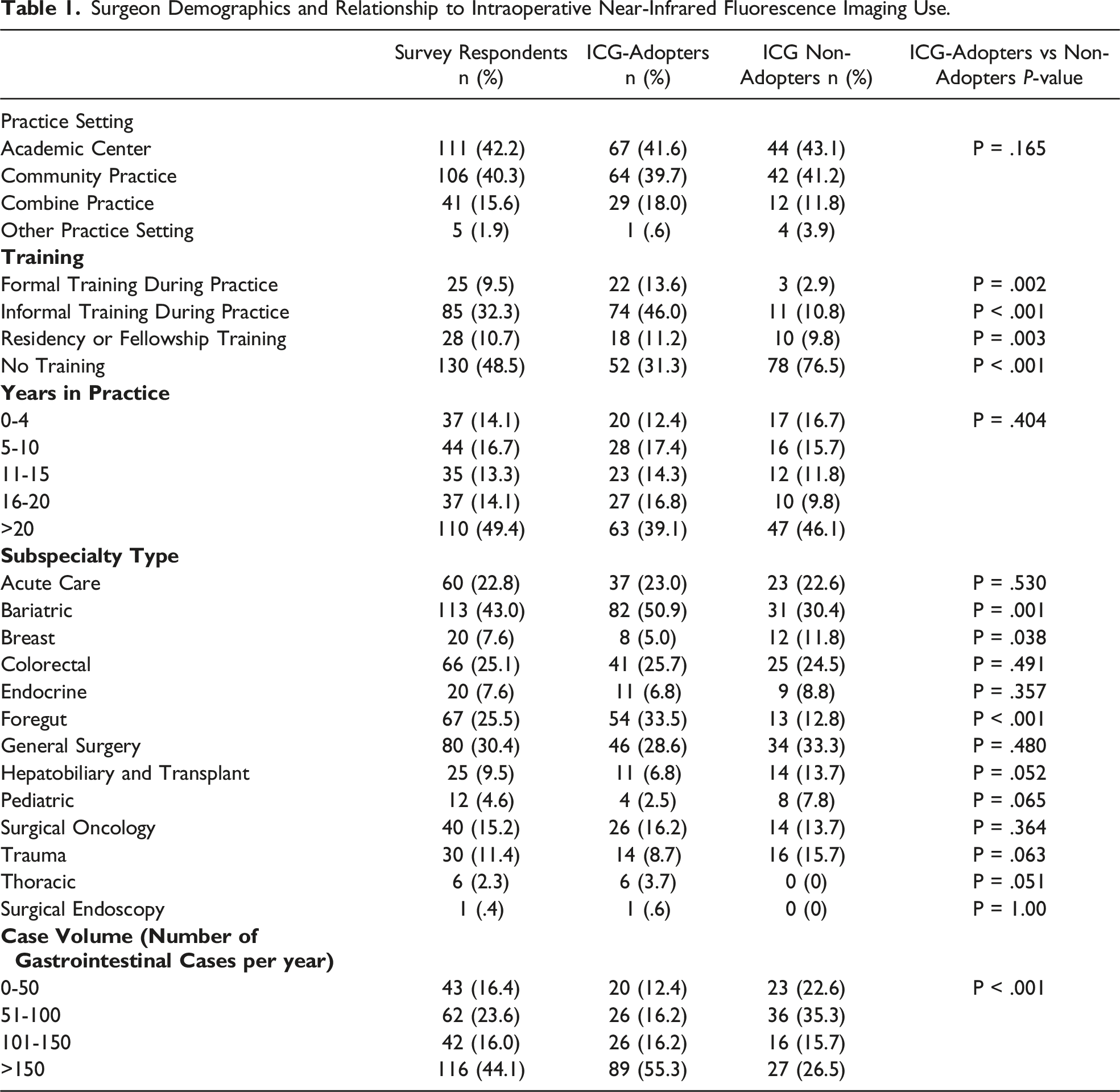
Of respondents who completed the survey, 130 (49.4%) had never received formal training associated with ICG or NIRFI. The remaining 133 surgeons had previous training, with 25 (9.5%) receiving formal training during their surgical practice, 85 (32.3%) having informal training during their surgical practice, and 28 (10.7%) receiving training during their fellowship or residency programs.
Characterizing ICG Utilization
Rate of ICG adoption by type of center, training, stage of practice, and subspecialty is described in Table 1. Over half of all respondents (n = 161, 61.2%) had used ICG during their surgical practice. Of ICG-adopters, use was often described as routine (n = 61, 37.9%) or selective (n = 70, 43.5%), and less likely to be described as rarely used (n = 30, 18.6%).
Comparing ICG-adopters and non-adopters, we see that community, academic, and mixed practice surgeons appear to use ICG with similar frequency (P = .165, Table 1). Surgeons with ICG training made up 70.8% (n = 114) of ICG-adopters, while those without training accounted for 76.5% (n = 78) of ICG non-adopters, which was a statistically significant difference (P < .001). Bariatric and foregut surgeons adopted ICG at a significantly higher rate than others (P = .001 and P < .001 respectively), with a trend towards increased use by thoracic surgeons (P = .051). Finally, a higher case volume also appears to be associated with increased ICG use (P < .001), while stage of practice doesn’t appear to have an effect (P = .404). Alternatively, hepatobiliary and transplant surgeons (6.8% of ICG-adopters and 13.7% of non-adopters, P = .052), and pediatric surgeons (2.5% of ICG-adopters and 7.8% of non-adopters, P = .065) trended towards disproportionately low ICG-adoption.
Of ICG-adopters, the most common reason for use was for evaluation of anastomoses, with 117 (72.7%) of adopters having used it for that indication. Similarly, 106 (65.8%) of ICG-adopters reported utilizing ICG during laparoscopic cholecystectomy. ICG-adopters have also frequently used ICG for a macroscopic angiogram (66, 41.0%), or to assess bowel viability during ischemic presentations (101, 62.7%). Fewer ICG-adopters have used it to assess for peritoneal metastases (7, 4.3%), for sentinel lymph node biopsy (19, 11.8%), to identify ureters (45, 28%), or to delineate tumor margins (22, 13.7%).
Barriers to ICG Utilization
ICG-Adopters
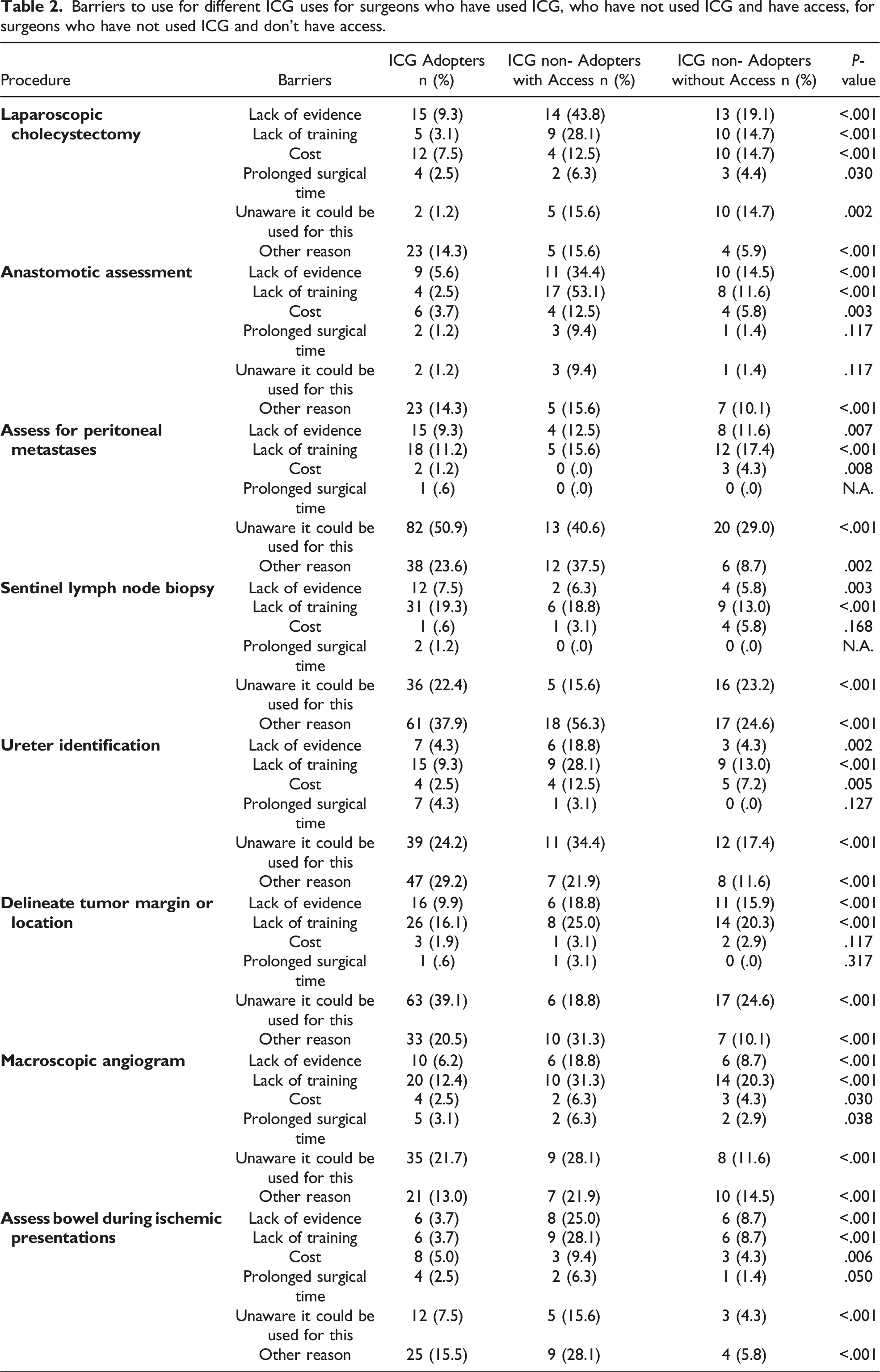
Barriers to use for different ICG uses for surgeons who have used ICG, who have not used ICG and have access, for surgeons who have not used ICG and don’t have access.
Non-Adopters With Access
For surgeons who had not used ICG (n = 101), only 31 (30.7%) worked at centers with access to near-infrared imaging technology. For these non-adopters with access to ICG technology, inadequate training and belief that there is inadequate evidence to support its use (ie low confidence in current evidence) were the primary barriers cited for lack of use during laparoscopic cholecystectomy or evaluating of anastomotic perfusion. These reasons were also frequently cited, along with lack of awareness about ICG use, for non-use during other techniques. Notably, surgeons with access that do not use ICG cited lack of training and lack of confidence in current evidence much more frequently for all procedures than surgeons who used ICG.
Non-Adopters Without Access
For surgeons who had not used ICG and worked at centers without access (n = 68, 67.3% of non-adopters), over half stated they would use near-infrared imaging for laparoscopic cholecystectomy (35, 51.5%), anastomotic perfusion (43, 62.3%), ureteric identification (39, 56.5%), and to assess bowel viability during ischemic presentations (52, 75.4%) if they had access to the technology. Similarly, over one-third would use ICG for the other techniques discussed in this survey if they had technological access. For non-adopters without current access who would not use NIRFI if given access, similar reasons were cited as barriers for all techniques as adopters, and as non-adopters.
Discussion
Our work presents the largest survey characterizing NIRFI and barriers to its use within general surgery disciplines. Over half of all respondents reported ICG use, with adoption highest amongst those with increased case volume, as well as those practicing bariatric, foregut, and thoracic subspecialties. The most common uses for ICG was evaluation of anastomoses and biliary anatomy, followed by use during ischemic presentations and in macroscopic angiograms. Primary barriers to ICG use was lack of confidence in current evidence, while education and awareness were cited as barriers for procedures where NIRFI was used less commonly. Considering the high rates of NIRFI use, future high-quality prospective randomized studies evaluating the utility of ICG for these procedures is of utmost importance to improve surgeon confidence in the current evidence. If NIRFI efficacy is demonstrated, increased training and knowledge dissemination will be required to reduce barriers to access.
Surgeons more likely to report using NIRFI appear to be those with prior ICG training, practicing bariatric, foregut, and thoracic surgery. It is not surprising that increased training is associated with NIRFI adoption as reasons for early technological uptake amongst surgeons frequently include ability to practice, test the technology, and use it in a trial period.32,33 Uptake by colorectal surgeons in our study is consistent with rates recently reported by Italian surgeons. 34 In contrast rates for ICG use amongst bariatric, foregut, and thoracic surgeons has not previously been reported, yet the increased use amongst those specialties is not surprising given the evolving literature in the respective disciplines. More frequent use amongst foregut, thoracic, and bariatric surgeons is in keeping with ease of NIRFI integration into their surgical techniques due to a high volume of laparoscopic procedures enabling routine access to NIRFI equipment. 35
Additionally, increased frequency of high risk anastomoses in bariatric, foregut, and thoracic surgery, combined with growing evidence for beneficial effects from ICG on anastomotic assessment is likely related to use in these groups 8 It is also not surprising that increasing operative volume is associated with ICG use; procedure experience has previously been associated with early technology uptake.32,33 On the other hand, it is surprising that ICG uptake appears to be similar for community and academic surgeons, since surgical technology is typically adopted at high volume centers initially when start-up cost is high and only becomes economically feasible with significant patient volume.36-38 However, much of this data arises from implementation of robotic surgery, which has a much higher up-front cost than NIRFI. Indeed, equal uptake by community surgeons may support cost-efficacy noted by experts in recently published consensus documents. 1 Alternatively, NIRFI uptake in community-based surgery may be due to a few influential early-adopters at these sites having a large influence on a smaller surgical department.
Interestingly, the most frequently cited barriers to ICG appear similar for adopters, non-adopters with access, and non-adopters without access. For the most common procedures with ICG use (cholecystectomy and anastomotic evaluation), a lack of confidence in current evidence appeared to be the primary barrier, while awareness and training appear less important. Lack of confidence in current evidence was cited very frequently by non-adopters compared to adopters. This is interesting since significant prospective and meta-analysis data suggests that ICG cholangiography has similar efficacy to intraoperative cholangiogram during laparoscopic cholecystectomy.3,4,7,39,40 Evidence and consensus guidelines also exists demonstrating the utility of ICG cholangiography, its benefit to help delineate anatomical variants, and for educational purposes.6,7,40,41 Uncertainty regarding evidence for ICG cholangiography may also reflect a need for studies evaluating its use in acute cholecystitis, as most current evidence evaluates elective cholecystectomy.5,7,40 Similarly, meta-analyses and prospective data has demonstrated benefits for anastomotic assessment in colorectal and other high risk anastomoses. 8 However, these studies frequently state that ICG techniques remain heterogeneous and the optimal technique should be delineated. This uncertainty regarding optimal technique for NIRFI during cholecystectomy or anastomotic assessment may lead to critical evaluation of evidence for these techniques. For other procedures, barriers included lack of evidence, education, and awareness. This suggests that additional work is required in promoting less well-known indications of NIRFI.
Overcoming these barriers may be accomplished by continuing to highlight NIRFI benefits and indications, both locally and internationally. This may be achieved at key conferences or academic events, which are often attended by general surgeons across North America. Additionally, webinars or training on ICG/NIRFI use, potentially during conferences, may be beneficial. Fortunately, the International Society for Fluorescence Guided Surgery (ISFGS) has recently been launched with education and webinars planned that are likely to provide further education access for surgeons. Programs such as this appear to be particularly beneficial since many surgeons without current access appear to be interested in utilizing NIRFI.
The most significant limitations of this study are response bias and sampling bias due to the low response rate of our survey; surgeons with more interest in NIRFI are more likely to complete this entirely voluntary survey. This likely biases our study towards higher reported rates of NIRFI use in this survey sample. Due to the low survey response rate, outcomes of this study may also be biased in directions that we cannot predict. Considering the growing use of NIRFI, future studies during in person conferences or with respondent benefits may be valuable to achieve a better response rate. However, our response rate should also be evaluated considering that surveys of surgeons typically only achieve a 50% response rate. 42 In terms of sampling bias, only members of CAGS and SAGES with publicly available emails were included; these may not represent the opinions of most surgeons with SAGES surgeons more likely to work laparoscopically and have NIRFI access. Although nearly 300 surgeons across various practice types, career stages, and general surgery subspecialties participated, the low response rate in this survey leaves significant uncertainty and results should be evaluated with caution; many other perspectives may exist regarding ICG use and its barriers. Despite these limitations, we had a substantial number of responses, which included an array or adopters, non-adopters, and surgeons without access, which should improve generalizability of these results.
Despite these limitations, this study demonstrates that a large proportion of general surgeons currently use ICG, with its use to evaluate anastomoses, biliary anatomy, and bowel viability being the most common uses. Considering such high rates of ICG use for these techniques, prospective, randomized trials to provide further confidence in current findings is required. If benefits continue to be supported, increased training opportunities and information dissemination is required to eliminate barriers to use for many surgeons.
Conclusions
NIRFI use is common amongst general surgeons, with high operative case volume, and bariatric, foregut, and thoracic surgery subspecialty practices are associated with adoption. Cholangiography and anastomotic assessment appear to be the most common uses, while commonly cited barriers appear to be lack of confidence in current evidence, lack of awareness, and lack of education. Prospective randomized are required to further improve confidence in current evidence; if benefits continue to be shown, technical information and training will be imperative to improve ICG access.
Supplemental Material
Supplemental Material - Characterization of Near-Infrared Imaging and Indocyanine-Green Use Amongst General Surgeons: A Survey of 263 General Surgeons
Supplemental Material for Characterization of Near-Infrared Imaging and Indocyanine-Green Use Amongst General Surgeons: A Survey of 263 General Surgeons by Kevin Verhoeff, Valentin Mocanu, Breanna Fang, Jerry Dang, Warren Sun, Noah J. Switzer, Daniel W. Birch and Shahzeer Karmali in Surgical Innovation
Footnotes
Author Contributions
KV conducted the survey and created the manuscript draft, BF collected data and assisted with analysis, VM and JD conducted analysis and performed manuscript editing. NS, DB, and SK directed the project, provided guidance throughout, and assisted with manuscript editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.