
Abstract
Background. Postoperative monitoring of deep inferior epigastric perforator (DIEP) flaps for breast reconstruction using noninvasive tissue oximetry enables timely recognition of vascular compromise. This may limit ischemic tissue damage, minimizing postoperative morbidity and healthcare costs. The aim of this review was to provide an economic analysis of tissue oximetry for postoperative monitoring of DIEP flap breast reconstruction. Methods. A systematic literature search was conducted utilizing PubMed and Embase. Articles reporting costs related to tissue oximetry following DIEP flap breast reconstruction, costs directly related to DIEP flap surgical procedure, and costs associated with postoperative complications were included. Risk of bias was assessed using different tools depending on study type. Results. Six articles were included. Four studies provided an overview of total costs associated with DIEP flap breast reconstruction; two studies focused on whether tissue oximetry could facilitate a decrease in hospital costs. Average overall costs for DIEP flap procedure were estimated at $28 000, with additional costs up to $37 530 in case of total flap failure. Tissue oximetry to monitor DIEP flaps could potentially save up to $1667 per procedure. Moreover, it might eliminate the need for specialized postoperative care. Conclusion. Tissue oximetry following DIEP flap breast reconstruction can potentially facilitate a decrease in hospital costs since its readings enable physicians to intervene in an early stage of tissue malperfusion, contributing to minimizing complications. Tissue oximetry may eliminate the need for specialized postoperative care. However, based on the current literature, no firm conclusions can yet be drawn regarding cost-effectiveness of standard implementation.
Keywords
Introduction
The deep inferior epigastric artery perforator (DIEP) flap is one of the most frequently used methods for autologous breast reconstruction.1-3 Since the introduction of free flap reconstruction and advances in microsurgical techniques, flap viability has improved significantly, with reported success rates around 98%.4,5,7 Nevertheless, circulatory failure (5-25% of cases) appears as a relatively common complication, necessitating reexploration in 5-7.5% of the procedures and complete flap loss in 1.5-6% of cases.6-9 Salvage rates are inversely related to the time interval between the onset of critical tissue oxygenation and surgical intervention to restore local tissue perfusion.8,10 Hence, accurate and continuous monitoring of DIEP flaps is an absolute necessity for timely detection of potential flap failure, allowing surgical intervention in an early stage.11,12 In a study by Creech and Miller, the characteristics of the theoretically ideal monitoring technique were defined as harmless to the patient, rapidly responsive, accurate, reliable, easy to use, and cost effective.4,13 Despite the introduction of various new monitoring techniques, to date none of them fulfills all the above mentioned criteria.4,14 Clinical observation of flap color, temperature, and capillary refill remains the benchmark for assessing flap viability, despite its obvious shortcomings in terms of objectivity and continuity.14,15
Tissue oximetry proved to be a versatile clinical monitor with various applications,16,17 including DIEP flap monitoring. 18 Noninvasive tissue oximetry uses near-infrared spectroscopy (NIRS) to continuously assess regional tissue oxygen saturation (StO2) based on the modified Lambert-Beer law.9,15,19,20 Application of tissue oximetry in free flaps enables early recognition of vascular compromise before clinical symptoms of flap failure become apparent.4,19,21,22 This may limit the extent of ischemic tissue damage and its detrimental consequences, such as wound problems, including deep tissue infection, and fat necrosis.3,8 Tissue oximetry has proven to be reliable, sensitive, accurate, and user friendly.2,4,8 Several clinical studies indicated that tissue oximetry is a viable monitor for this relatively new application. Nevertheless, recent studies report that tissue oximetry could be relatively expensive to implement in clinical practice and it is used in less than 5% of DIEP flap procedures.4,14,23
The aim of this review was to provide an economic analysis of tissue oximetry for postoperative monitoring of DIEP flap breast reconstruction and whether inclusion in routine monitoring protocols could be justified.
Methods
This review was written according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement for reporting systematic reviews. 24
Search Strategy.
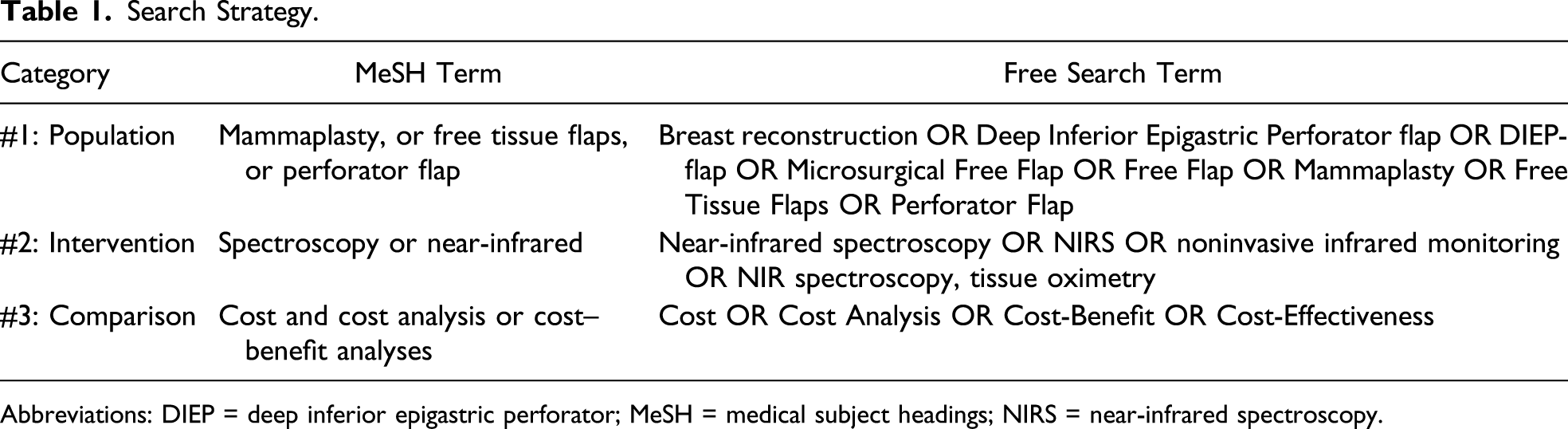
Abbreviations: DIEP = deep inferior epigastric perforator; MeSH = medical subject headings; NIRS = near-infrared spectroscopy.
For the Embase database, the following search strategy was used: (Deep Inferior Epigastric Perforator flap OR ''Mammaplasty'' [Mesh] OR ''Free Tissue Flaps'' [Mesh] OR ''Perforator Flap'' (Mesh] AND ''Near-Infrared'' [Mesh] Or Near-infrared spectroscopy OR NIRS OR non-invasive infrared monitoring OR tissue oximetry AND ''Cost analysis'' [Mesh] OR ''Cost-Benefit Analysis'' [Mesh] OR Cost-Effectiveness). The same search filters were used as in the PubMed search.
The literature search was performed by two researchers (AL/VR) independently. Following removal of duplicates, eligibility of the remaining articles was initially determined by screening the title. Subsequently, studies were screened based on the abstract. Remaining studies were screened by reading the full text; those that did not answer the research question concerning the cost-effectiveness of using NIRS following DIEP flap surgery were excluded. In case of disagreement between the aforementioned researchers, a third researcher (NV) was consulted.
From the included studies, the following information was retrieved: the surname of the first author, year of publication, country of origin, objectives, study design, study population, and documented costs.
Results
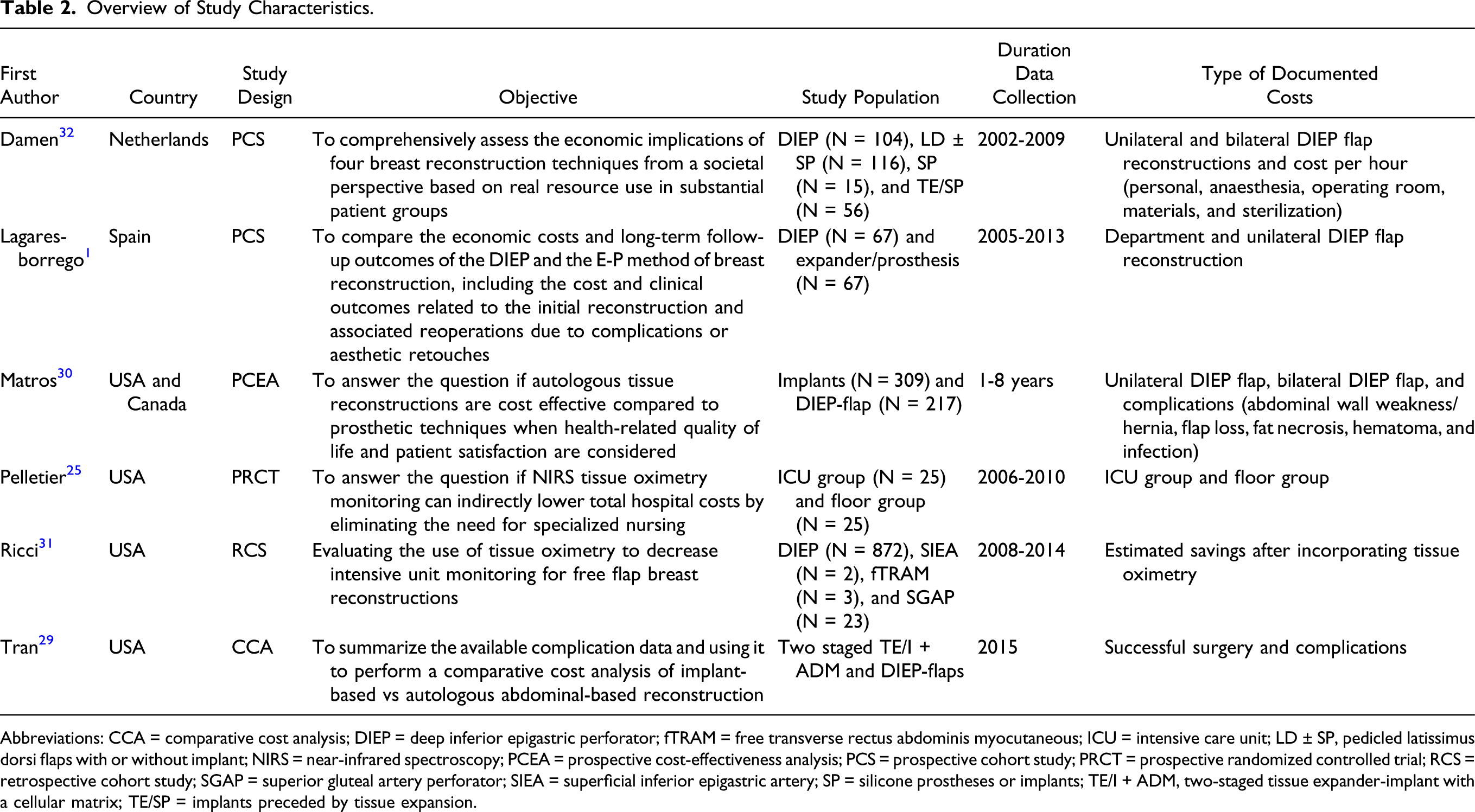
After conduction of the systematic literature search in the aforementioned databases, 6 of 160 articles were eligible for inclusion. See Figure 1 for the flow chart. Four studies (2 prospective cohort studies and 2 cost analysis studies) reported on costs related to the DIEP flap breast reconstruction. One study (a randomized controlled trial) reported costs related to noninvasive tissue oximetry following DIEP flap surgery. Another study evaluated the use of tissue oximetry to decrease intensive care unit (ICU) monitoring for free flap breast reconstruction. Table 2 shows the study characteristics. All studies were single center trials and were conducted in either Europe or the United States. Flowchart of the used search strategy. Overview of Study Characteristics. Abbreviations: CCA = comparative cost analysis; DIEP = deep inferior epigastric perforator; fTRAM = free transverse rectus abdominis myocutaneous; ICU = intensive care unit; LD ± SP, pedicled latissimus dorsi flaps with or without implant; NIRS = near-infrared spectroscopy; PCEA = prospective cost-effectiveness analysis; PCS = prospective cohort study; PRCT = prospective randomized controlled trial; RCS = retrospective cohort study; SGAP = superior gluteal artery perforator; SIEA = superficial inferior epigastric artery; SP = silicone prostheses or implants; TE/I + ADM, two-staged tissue expander-implant with a cellular matrix; TE/SP = implants preceded by tissue expansion.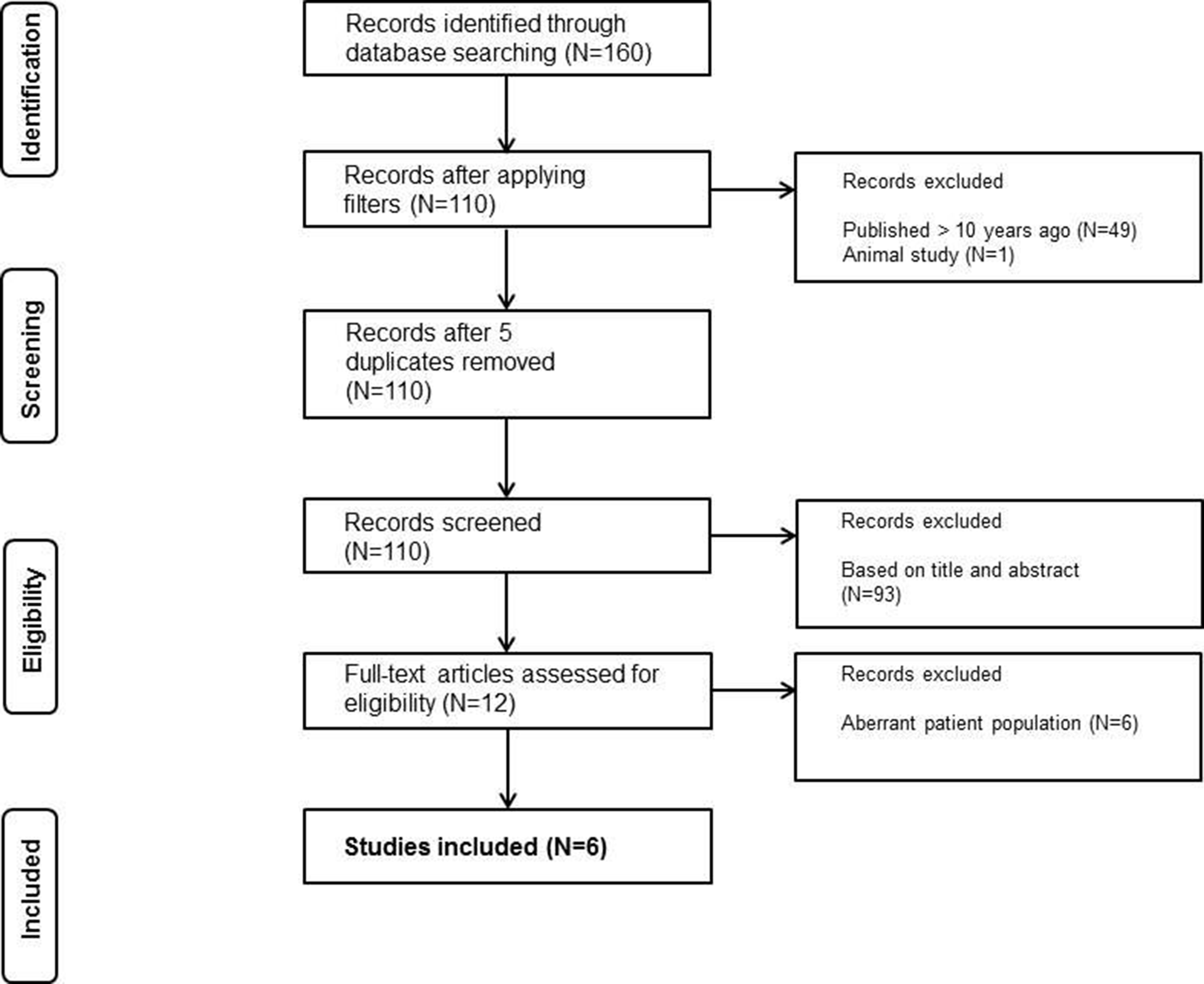
Risk of Bias Within Studies
Cochrane Risk of Bias Tool for Randomized Controlled Trials.
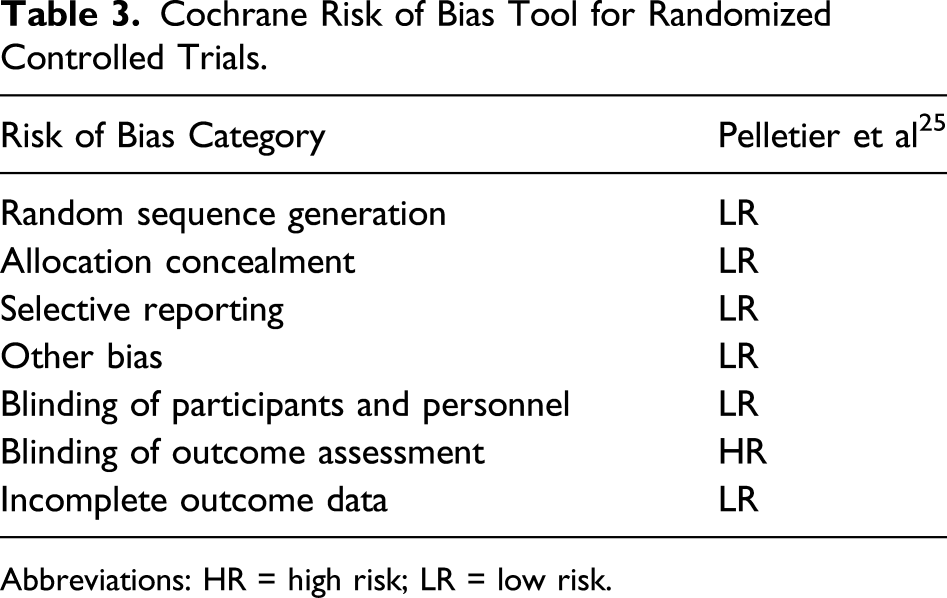
Abbreviations: HR = high risk; LR = low risk.
Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies.
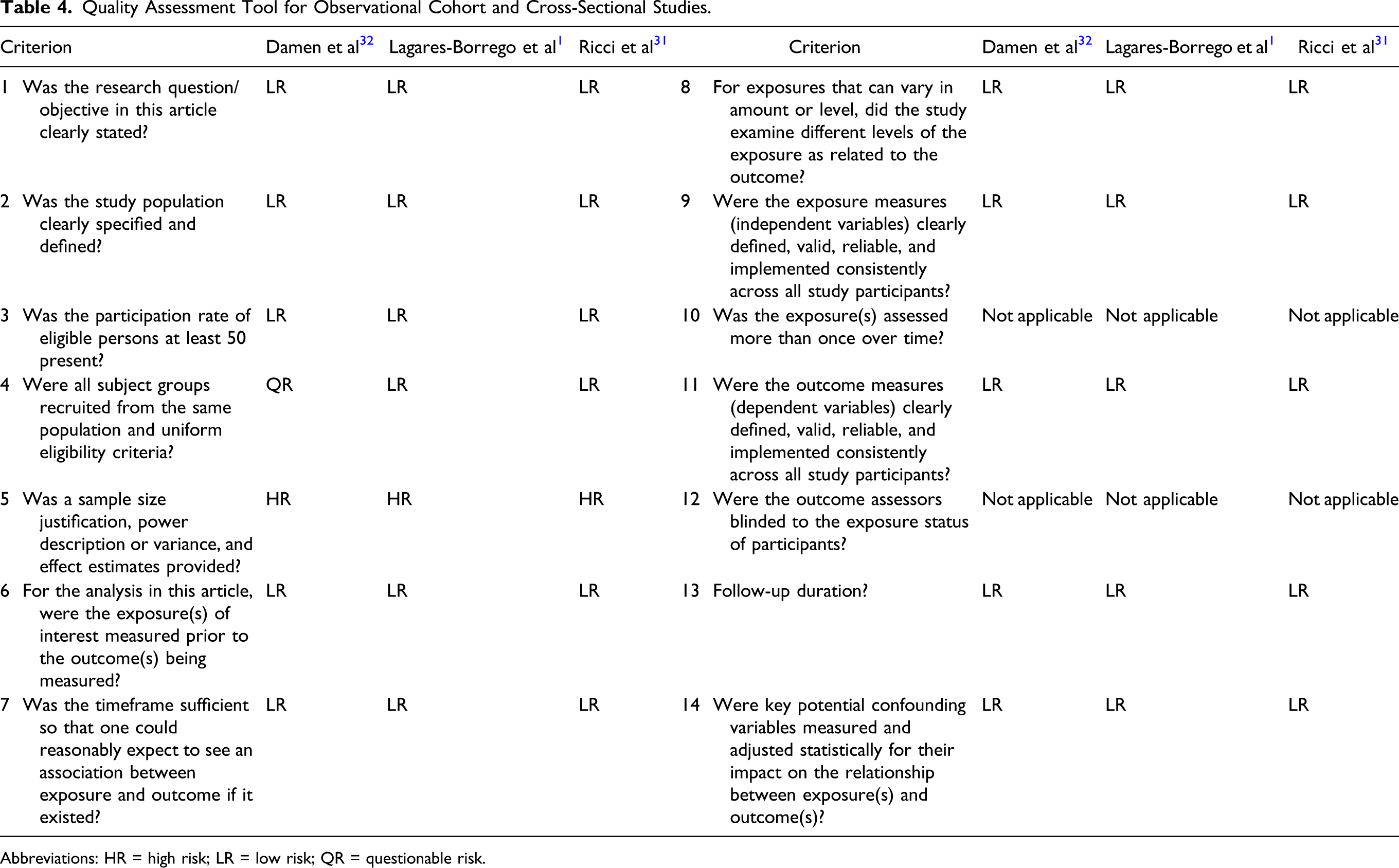
Abbreviations: HR = high risk; LR = low risk; QR = questionable risk.
Assessment of Bias Following the Short Checklist of Drummond et al.
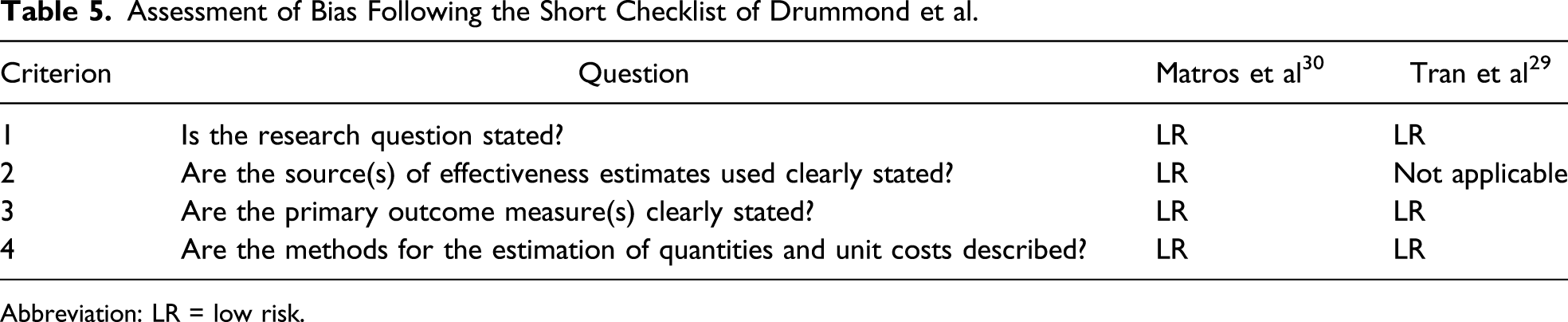
Abbreviation: LR = low risk.
Randomized Controlled Trial
For assessing quality of the randomized controlled trial of Pelletier et al, 25 the Cochrane risk of bias tool was used, which consists of seven categories, as shown in Table 3. The study scored a “high risk of bias” on the criterion “blinding of outcome assessment” because the principal investigator was informed about the choice of department for postoperative stay of the patients.
Prospective Cohort Studies
The quality assessment tool for observational cohort and cross-sectional studies from the National Heart, Lung, and Blood Institute was used to assess the quality of the included cohort studies (Table 4). The study of Damen et al 32 scored a questionable risk of bias on criterion four (uniform eligibility criteria of subject groups) because one of the surgical reconstructive techniques included in the study was sparsely performed in the chosen time frame (2002-2006). To provide a representative study sample, they extended the inclusion period for this single technique with three years. Furthermore, both prospective cohort studies1,32 did not provide any justification for their sample size, nor include a statistical power calculation. Therefore, both studies were rated as “high risk of bias” on this specific criterion.
Retrospective Observational Cohort Study
The quality assessment tool for observational cohort and cross-sectional studies from the National Heart, Lung, and Blood Institute was used to assess the quality of the retrospective observational cohort study of Ricci et al 31 (Table 4). The study scored a high risk of bias on criterion 5 (sample size). Due to the type of study, no sample size justification or statistical power calculation was provided.
Cost Analysis Studies
To assess the quality of the cost analysis studies, the short checklist by Drummond et al was used (Table 5). The study of Tran et al 29 as well as the study of Matros et al had an overall score of “low risk of bias.” 30
Economic Analysis of Tissue Oximetry
Overview DIEP Flap Surgery Related Cost.

Abbreviation: DIEP = deep inferior epigastric perforator.
Euro converted into dollars by means of currency rate on May 01, 2020 (€1 = $1.10).
Overview of Specific Departmental Costs per Hour.

Euro converted into dollars by means of currency rate on May 01, 2020 (€1 = $1.10).
Overview of Additional Costs (US Dollar) Related to DIEP Flap Failure.
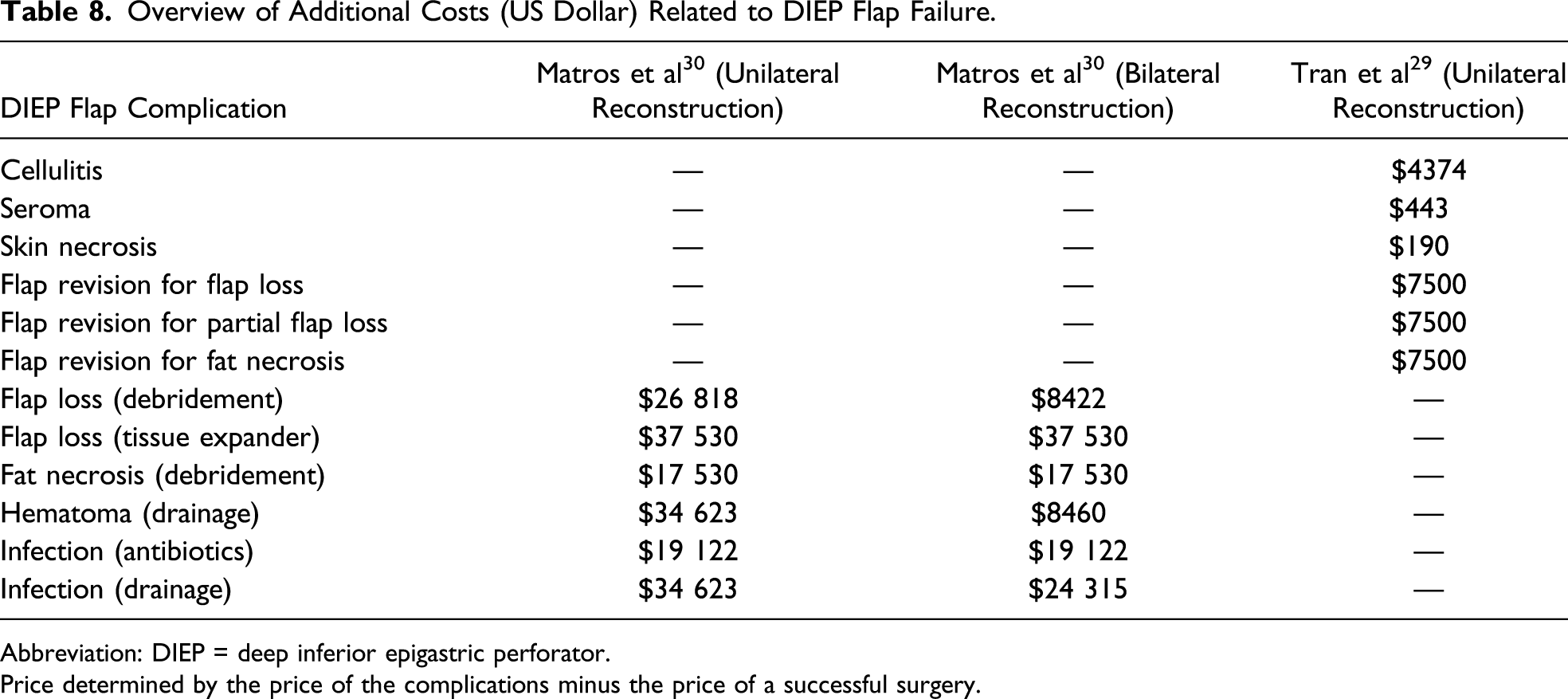
Abbreviation: DIEP = deep inferior epigastric perforator.
Price determined by the price of the complications minus the price of a successful surgery.
The implementation of noninvasive tissue oximetry for completion of standard monitoring routine entails additional costs. For example, as described by Smit et al, 4 costs for a tissue oximetry device account $16 500, with $150 for one disposable sensor. Nevertheless, according to Pelletier et al, estimated savings of $1337.00 per procedure could be obtained when NIRS would be implanted as the standard monitoring tool. 25 In the study of Ricci et al, they incorporated tissue oximetry into standard postoperative monitoring protocol since June 2008. They concluded that the use of tissue oximetry in the postoperative phase reduced the amount of time spent in the intensive care. Patients with continuous oxygen sensor monitoring could be transferred to the ward after 15 hours instead of 24 hours. This resulted in a significant decrease of $1667 in costs per DIEP flap reconstruction. 31
Discussion
This review focused on providing an economic analysis of tissue oximetry for postoperative monitoring of DIEP flap breast reconstruction and whether inclusion in routine monitoring protocols could already be justified based on the current literature.
Since the introduction of autologous breast reconstruction, success rates have improved.4,6 Nevertheless, circulatory failure for which reexploration is needed occurs in approximately 5-7.5% of the procedures, resulting in a total flap loss of 1.5-6%.6-9 Costs for DIEP flap surgery are estimated to amount $28 000, with a widespread variation between countries.1,25,30 Additional costs accompanying flap failure can extend to $37 530. 29 In order to limit or prevent these complications, timely detection of vascular compromise is most essential.
Several studies described the added value of tissue oximetry in postoperative flap monitoring.9,25 A timely detection of possible flap failure and intervention when applying tissue oximetry in the postoperative setting can prevent a subset of complications, resulting in an increase in flap salvage rate from 91-99%. 15 In order to benefit from the advantages of continuous monitoring using tissue oximetry, inclusion of the measurement method in the standard monitoring protocols is required. According to Smit et al, costs for a tissue oximetry device account $16 500, with $150 for one disposable sensor. 4 Important to note is that when using continuous monitoring, patients may safely be transferred to the ward instead of the ICU in the early postoperative period. 25 This, in turn, may lead to an estimated saving up to $1667 per unilateral DIEP flap reconstruction. 31
When interpreting the results of this review, some limitations need to be taken into account. None of the included articles reported on all types of costs associated with DIEP flap surgery. Given the fact that the included studies were performed in different countries (e.g., Europe and United States) with different healthcare systems, a widespread variation in costs for the surgical procedure can be expected. Therefore, interpretation of the total costs of a DIEP flap procedure was challenging.
The literature objectively describing the benefits vs all costs accompanying application of tissue oximetry in DIEP flap surgery remains scarce. As a result, a true cost-effectiveness analysis could not yet be performed. Further studies are necessary to provide a more specific overview in clinical benefits and costs associated with noninvasive monitoring through tissue oximetry.
In conclusion, tissue oximetry for postoperative monitoring of DIEP flap breast reconstruction can aid in preventing a subset of complications, it can limit the extent of ischemic tissue damage, and can possibly reduce the need for specialized nursing care. This noninvasive tissue monitoring technique can therefore result in a decrease of total costs. However, based on the results of the currently available literature, no firm conclusions can be drawn regarding cost-effectiveness and subsequent endorsement of implementation in standard postoperative protocols.
Footnotes
Author Contributions
Study concept and design: Anouk A. M. A. Lindelauf, Nousjka P. A. Vranken, Vivian G. H. Rutjens, Rutger M. Schols, John H. Heijmans, Patrick W. Weerwind, and René R. W. J. van der Hulst
Acquisition of data: Anouk A. M. A. Lindelauf, Nousjka P. A. Vranken, and Vivian G. H. Rutjens
Analysis and interpretation: Anouk A. M. A. Lindelauf, Nousjka P. A. Vranken, and Vivian G. H. Rutjens
Study supervision: Rutger M. Schols, John H. Heijmans, Patrick W. Weerwind, and René R. W. J. van der Hulst
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Appendix A: Search Strategies for PubMed
Category
Query
#1: Population
"Mammaplasty"[Mesh] OR "Free Tissue Flaps"[Mesh] OR "Perforator Flap"[Mesh] OR ("mammaplasty"[MeSH Terms] OR "mammaplasty"[All Fields] OR ("breast"[All Fields] AND "reconstruction"[All Fields]) OR "breast reconstruction"[All Fields]) OR (Deep[All Fields] AND Inferior[All Fields] AND Epigastric[All Fields] AND ("perforator flap"[MeSH Terms] OR ("perforator"[All Fields] AND "flap"[All Fields]) OR "perforator flap"[All Fields])) OR DIEP-flap[All Fields] OR (("free tissue flaps"[MeSH Terms] OR ("free"[All Fields] AND "tissue"[All Fields] AND "flaps"[All Fields]) OR "free tissue flaps"[All Fields] OR ("flap"[All Fields] AND "free"[All Fields]) OR "flap free"[All Fields]) AND ("tissues"[MeSH Terms] OR "tissues"[All Fields] OR "tissue"[All Fields])) OR (("surgical flaps"[MeSH Terms] OR ("surgical"[All Fields] AND "flaps"[All Fields]) OR "surgical flaps"[All Fields] OR "flap"[All Fields]) AND Microsurgical[All Fields] AND Free[All Fields]) OR ("free tissue flaps"[MeSH Terms] OR ("free"[All Fields] AND "tissue"[All Fields] AND "flaps"[All Fields]) OR "free tissue flaps"[All Fields] OR ("free"[All Fields] AND "flap"[All Fields]) OR "free flap"[All Fields])
#2: Intervention
"Spectroscopy, Near-Infrared"[Mesh] OR ("spectroscopy, near-infrared"[MeSH Terms] OR ("spectroscopy"[All Fields] AND "near-infrared"[All Fields]) OR "near-infrared spectroscopy"[All Fields] OR ("near"[All Fields] AND "infrared"[All Fields] AND "spectroscopy"[All Fields]) OR "near infrared spectroscopy"[All Fields]) OR near-infrared[All Fields] OR NIRS[All Fields] OR (noninvasive[All Fields] AND infrared[All Fields] AND monitoring[All Fields]) OR ("spectroscopy, near-infrared"[MeSH Terms] OR ("spectroscopy"[All Fields] AND "near-infrared"[All Fields]) OR "near-infrared spectroscopy"[All Fields] OR ("nir"[All Fields] AND "spectroscopy"[All Fields]) OR "nir spectroscopy"[All Fields])
#3: Comparators
"Costs and Cost Analysis"[Mesh] OR "Cost-Benefit Analysis"[Mesh] OR ("economics"[Subheading] OR "economics"[All Fields] OR "cost"[All Fields] OR "costs and cost analysis"[MeSH Terms] OR ("costs"[All Fields] AND "cost"[All Fields] AND "analysis"[All Fields]) OR "costs and cost analysis"[All Fields]) OR ("costs and cost analysis"[MeSH Terms] OR ("costs"[All Fields] AND "cost"[All Fields] AND "analysis"[All Fields]) OR "costs and cost analysis"[All Fields] OR ("cost"[All Fields] AND "analysis"[All Fields]) OR "cost analysis"[All Fields]) OR ("cost-benefit analysis"[MeSH Terms] OR ("cost-benefit"[All Fields] AND "analysis"[All Fields]) OR "cost-benefit analysis"[All Fields] OR ("cost"[All Fields] AND "benefit"[All Fields]) OR "cost benefit"[All Fields]) OR ("cost-benefit analysis"[MeSH Terms] OR ("cost-benefit"[All Fields] AND "analysis"[All Fields]) OR "cost-benefit analysis"[All Fields] OR ("cost"[All Fields] AND "effectiveness"[All Fields]) OR "cost-effectiveness"[All Fields])
#1, #2, and #3: PIC
#1 AND #2 AND #3