
Abstract
The development and implementation of pandemic response protocols for museum workers and visitors evolved over many months following the recognition of the SARS-CoV-2 virus as a major public health threat and crisis trigger. Initial response to the crisis in many museums was cessation of all activity and interaction with the public and with coworkers. Museum functions were suspended. Museums closed their doors to visitors and staff. Access to exhibits and collections was disrupted. Ensuring the safety of objects on display was difficult. The air we breathed, the objects we touched, the spaces we were in were all suspect as potential transmitters of the virus. As research was conducted on virus transmission, research results were incorporated into the development of reopening protocols for museums and museum collections allied with a university museum consortium. Case studies of the compilation, distribution, implementation, and reflection of pandemic response protocols within consortium member museums provide insight into including these crisis protocols for emergency response and collections management policies going forward.
Keywords
Museums Respond to Crisis-Driven Closure
On March 19, 2020, eight days after the World Health Organization had declared COVID-19 a pandemic, the governor of Pennsylvania ordered a statewide closure of all “non-life sustaining” businesses, services, and other ventures (Commonwealth of Pennsylvania 2020). Within ten days, cultural institutions, including universities, across the state had closed. Consequently, university museums, galleries, libraries, and other entities with collections and exhibitions closed their doors to visitors, volunteers, and personnel. Access to campuses were restricted to designated essential workers (e.g., security personnel, live animal caretakers, critical facility maintenance). In-person classes were suspended. Work was to be carried out remotely. These measures were extreme but deemed necessary to keep everyone alive and, hopefully, healthy.
By the end of March 2020, mandates for mitigating the spread and potentially lethal effects of the SARS-CoV-2 virus (the cause of COVID-19) had been instituted by the state’s largest university. These mandates complied with state directives and Center for Disease Control (CDC) guidelines. Implementation of the mandates was disruptive to all university operations. SARS-CoV-2 virus was recognized as a major public health threat, but little was known about the ways the virus could spread or be transmitted. In an attempt to minimize the spread of the virus, the initial response to the threat was cessation of all interactions with everyone—friends, coworkers, family members, strangers. Students, faculty, and staff were sent home. The university’s museums functions (e.g., collections stewardship, education, and exhibition programming) were suspended. University buildings were locked. Access to university museum exhibit spaces was suddenly off-limits to museum staff as well as museum visitors. Safety of museum collection objects on display and in storage could not be monitored or assured. The air we breathed, the objects we touched, the spaces we were in were all seen as potential transmitters of the virus.
Ten years earlier, a voluntary network of fifty-three museum and archive professionals and informal education specialists representing twenty-one scientific, artistic, historical, or cultural research and teaching collections and galleries had formed a university museum consortium on the university’s largest campus. The museum consortium was concerned about the safety, security, and welfare of its members, as well as the safety, security, and welfare of collections on display, on loan, in storage, and elsewhere. Museum collections safety concerns were not considered in the mandates and protocols enacted by the university. Social distancing, mask wearing, deep cleaning, and sanitizing of people, places, and things were required across the university; however, for the museum consortium the concept of deep cleaning and sanitizing collection objects was alarming. As the American Association for State and Local History stated in an ethics position paper addressing museum closures, “regardless of what the law may require, history museums are obligated to protect the collections they hold in the public trust, regardless of what happens to the institutions” (AASLH Committee on Professional Standards and Ethics 2006). Not all consortium member museums were history museums, but most had collections held in the public trust. While no one was sure what would happen to the university or if the mandated closures would be prolonged or permanent, museum consortium members felt obligated to protect their collections.
Reopening Task Force
By May 2020, the museum consortium had a Reopening Task Force (a three person ad hoc committee) in place to help inform the membership about emerging research and protocols specific to museum facilities, materials, and objects. Although each member museum was governed by a different semi-autonomous organizational unit of the university (e.g., college, department, library, athletic corporation), the museum consortium had gained recognition by university leadership in 2015 as a professional, cross-disciplinary campus alliance committed to the promotion and preservation the university’s collections and museum facilities. This recognition allowed the museum consortium to take the lead in addressing safety concerns specific to university museum collections access and safety protocols.
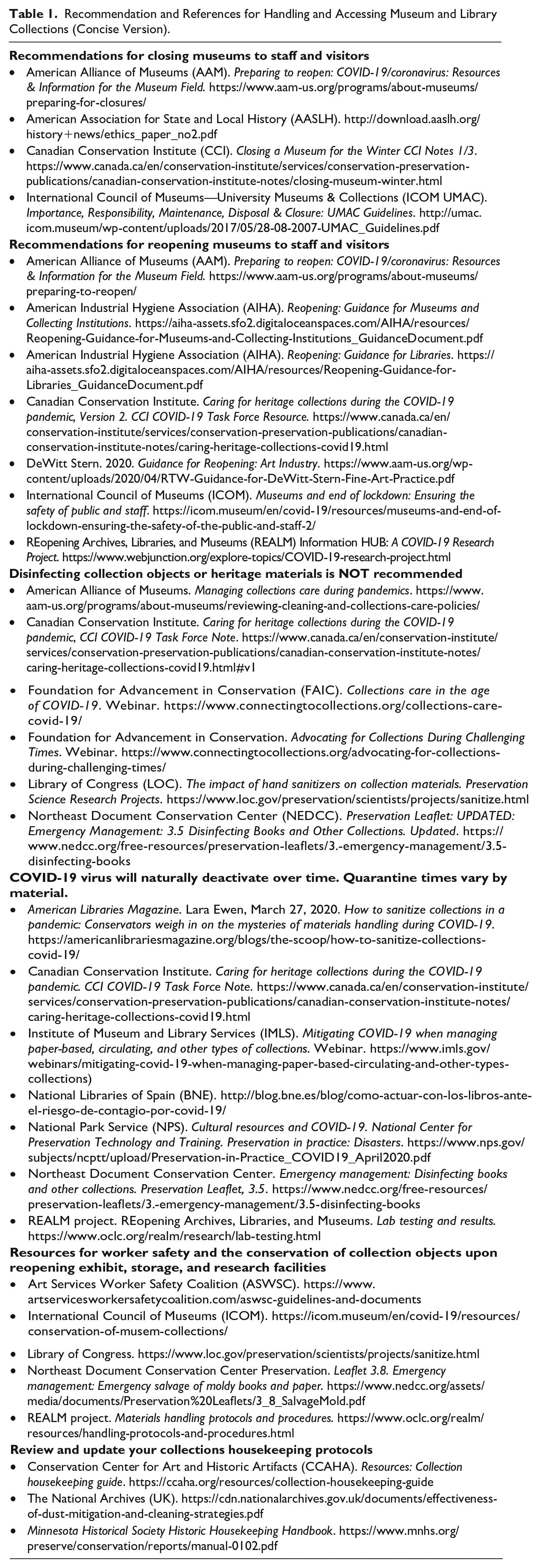
The Reopening Task Force began searching for and collecting research-based, reliable recommendations and references for handling and accessing museum and library collections as well as closing, opening, and reclosing museum facilities to staff and visitors. A growing body of recommendations and references were being developed by national and international organizations of museum, library, conservation, and risk management professionals. As information became more available online, the Task Force verified references and links before compiling and releasing them as a PDF through the museum consortium’s listserv. The first PDF document was posted on May 31, 2020. Each month the document, Recommendations and references for handling and accessing museum and library collections (Table 1: concise version of the document), was updated, amended, and distributed through the museum consortium listserv to the fifty-three individual members as well as by email to university and organizational unit risk managers. The first document was three pages long; by October 2020 the document had grown to seven single-spaced pages. Online resources listed in the document often linked to aggregations of more references and recommendations that were applicable to a wide range of museums and collections subject to sudden closure whether planned, unforeseen, unavoidable (e.g., unexpected loss of staff, natural disaster), or the then crisis of the rapid spread of the SARS-CoV-2 virus and resulting pandemic.
Recommendation and References for Handling and Accessing Museum and Library Collections (Concise Version).
The use of alcohols, chemical agents, and UV light exposure became recommended methods of sanitization, sterilization, decontamination, and disinfection for spaces and surfaces leading museum and library conservation organizations to voice opposition to applying any of these methods to collection objects and associated materials (e.g., paper documentation, supports, storage furniture). Many of the generally recommended methods were known to cause irreparable harm to collection objects and heritage materials (e.g., Karsten et al. 2020). REALM (REopening Archives, Libraries, and Museums), a project conducted jointly by OCLC (a nonprofit global library organization formerly known as the Online Computer Library Center), the Institute of Museum and Library Services (IMLS), and Battelle, a private nonprofit applied science and technology development company, reviewed published research, selected and vetted evidence-based resources, and conducted laboratory testing of:
SARS-CoV-2 virus transmission;
virus viability on surfaces;
the effectiveness of various disinfection and cleaning methods used to mitigate the spread of the virus; and
how (or if) collection objects and materials could be handled to minimize exposure to the virus by museum and library staff and visitors.
As the months passed and more research results were published it became evident that the SARS-CoV-2 virus on surfaces would deactivate over time (Biryokov et al. 2020; Kampf, Todt, and Steinmann 2020; Ratnesar-Shumate et al. 2020). Collection materials that may have been contaminated could be quarantined until the virus was no longer viable (Striegel 2020). Although definitive studies for all collection material types were not carried out, general guidelines for museum and library collection materials were developed (OCLC 2020). Recommendations for updating housekeeping protocols to take into consideration potential virus loads on surfaces and contamination through contact and proximity were made available (e.g., Miller 2020). Resources for worker safety and the conservation of collection objects upon reopening exhibit, storage, and research facilities were published and made available online (see Table 1 for examples).
As the first year of the pandemic drew to a close, mandated masking, social distancing, and working remotely remained enforced. The second year began with the availability of vaccines. Statewide mandates were relaxed but periodically reinstated regionally as outbreaks of virus infections rose and fell. Social distancing, frequent handwashing, meeting with colleagues, friends, and family online rather than in person had become standard. The museum consortium’s Reopening Task Force’s efforts had been instrumental in facilitating university recognition of some museum consortium members as essential workers with specialized skills and knowledge required to maintain the health, safety, and security of the university’s museum collections.
Case Studies: Museums’ Responses and Outcomes to the Crisis
Throughout mandated closures, the museum consortium held regular online meetings in an effort to decrease museum worker isolation and answer questions. Comparing the implementation of pandemic response protocols across consortium member museums provided insight into the efficacy of including these protocols in the museums’ policies and procedures going forward. During online meetings, consortium members reflected on the university’s and museum’s operational adjustments that they had made. Because of the efforts of the Reopening Task Force, collections health and security had not been compromised. All 21 of the consortium member museums eventually reopened; however, it became obvious that the closure affected each member museum in different ways. Unfortunately, not all of the museums recovered fully. Each member museum is governed by a different semi-autonomous organizational unit. Each museums’ mission, facilities, collections, staffing levels, budgets, and operational structures are different. These differences played a significant role in member museum reopening strategies. Despite the museum consortium’s efforts, several of the fifty-three consortium members were adversely affected by the pandemic. Case studies of member museums’ responses and outcomes, including the four highlighted in this article, aided in the development of a museum consortium strategic plan to address planning for the next crisis.
Case 1: Prioritizing Collection Access and Safety
The museum with the largest collection (>1,300,000 natural history specimens) and smallest exhibit space (450 ft2) had a staff comprised of one full-time collections manager/curator and a faculty member with one quarter-time museum director responsibilities. Traditionally, the collection was heavily used by students, faculty, and other researchers, and the exhibition space was open to the public and hosted several school field trips each year. During the mandated closure, while working from home, museum personnel increased the museum’s online exhibits and educational offerings. Access to the collection was restricted to one designated essential worker, in this case the collections manager. To enter campus and get to the collection, the collections manager was required to contact university security and make an appointment with an officer who would unlock doors and escort the essential worker in and out of the building. The essential worker and security officer were required to be masked, maintain social distance, and have proof of a negative COVID test for each access event. This protocol was required of all university personnel designated as essential workers who needed to be on campus. When students and researchers were allowed to return to work in the collection, masks, social distancing, and negative COVID tests were required if more than one person was in the building. With research and collections preservation being primary tenets of this museum’s mission, opening the collections for research use was given precedence over reopening the exhibit space. The exhibit space remained closed for more than two years.
Case 2: Prioritizing Exhibit Access and Safety
Another member museum, located in a dedicated museum building in the heart of campus, prioritized reopening their 13,000 ft2 of exhibit space. While closure mandates were in effect, the museum’s designated essential worker (the registrar) followed campus security protocols to periodically enter the building to assess conditions and security of collections on exhibit and in storage. With twenty-one paid staff, a collection of about 9,500 objects, and a mission prioritizing exhibitions and cross-disciplinary programs, the museum concentrated on strategies for reopening exhibitions and programs to the public as soon as closure mandates were lifted. Museum administrators, working from home, used Reopening Task Force collated research and information sources to develop a comprehensive opening plan. Preparations for reopening included securing a contract with a timed ticketing service, and designing and producing signage reinforcing expectations for visitor social distancing, mask wearing, traffic flow, hand sanitizing, no touching of objects, and gallery capacities. Plexiglass (acrylic) barriers were designed and purchased for objects on display as well as for front desk workers interacting with visitors. Attempts to make the front desk barriers more playful by adding empty picture frames and “framing” front desk workers were abandoned soon after the museum reopened. Assessment of visitor reactions to the museum’s reopening efforts disclosed that the picture frames created too much of a visual barrier and a deterrent to visitor interactions with front desk personnel. During a museum consortium virtual meeting, the museum presented their reopening process as a model for other museum consortium members. The cost of reopening preparation efforts was $30,000, an amount well above other member museums’ operating budgets.
Case 3: Extended Loss of Access to Exhibits and Collections
A museum located within a multi-purpose facility on the edge of campus had a 10,000 ft2 exhibit space, about 4,500 objects in its collection, three full-time staff, one part-time paid staff, and a docent corps of thirty to lead tours of the exhibition gallery and other areas of the facility. At the time of the mandated campus closure, the museum’s director was chair of the museum consortium and instrumental in establishing the Reopening Task Force as well as integrating recommended handling and access procedures into the museum’s collections management policy. Nonetheless, unlike other member museums, the organizational unit overseeing this museum chose to furlough all unit employees (including those in the museum) for several months. The museum director’s discretionary account that had been created for emergency spending was frozen by the organizational unit. No one was designated as an essential worker. Museum workers lost access to the museum space, collections, campus, and income. The docent corps, a group predominated by retirees deemed highly susceptible to the SARS-CoV-2 virus, was dissolved. The entire facility was closed except for one section that was set up as a COVID testing site by the university. When the museum did reopen, most docents did not return resulting in reduced revenue for the museum—fewer docents meant fewer opportunities to offer revenue-generating facility tours. A furloughed full-time staff member had secured a position elsewhere leaving a vacant position at the museum that was not filled. The access protocols that had been incorporated into the collections management policy were eventually used to guide the museum’s exhibit gallery reopening but they did not address worker morale issues.
Case 4: Delayed Access to Exhibition Space
The member museum with an on-campus exhibit gallery in a multi-use building, off-campus collections storage, approximately 21,000 collection objects, three full-time staff, and one volunteer was scheduled for a complete exhibition gallery renovation when the closure mandates were enacted. The closure delayed the start of the renovation project. The role of designated essential worker was assigned to the managing director but access to the gallery to remove objects and exhibit furniture in preparation for renovation was not granted until several months after the initial mandated closure went into effect. Access to the off-campus collections facility was not as restrictive as on-campus security measures. The managing director was allowed to grant permission to other museum staff to work with the collections in storage to finish a grant-funded collections stewardship project. University social distancing and masking protocols as well as object handling protocols derived from the Task Force-compiled resources guided worker personal safety measures and collection object handling. Without an exhibit gallery, museum staff working from home increased the museum’s social media presence with highlights of collection objects and past exhibits. When museum personnel were able to enter the exhibit gallery, the safety and handling protocols that proved effective in the off-campus facility were implemented while removing objects and casework from the exhibit gallery. When renovations did begin, face-to-face meetings with architects in the gallery space were fraught—the architects and renovation crews, as outside contractors, were not required to follow university masking and distancing protocols or personal safety protocols employed by the museum. There were numerous work stoppages when renovation crew members tested positive for COVID. There were also work stoppages when supply chain problems resulted in delayed shipments of materials and supplies. When the gallery renovation was complete, installation of exhibit furniture and objects was delayed by backlogged university moving crew schedules. The exhibition gallery remained closed for more than two years. The stress and anxiety levels experienced by everyone forced into isolation during mandated closures were exacerbated in a staff member by the additional strains of the renovation project and an extended medical leave. The staff member resigned. Due to budget constraints within the organizational unit, the resulting open position was not filled.
Conclusion
During any crisis, ensuring human health and safety must take precedence. During a crisis that results in the closure of museum facilities and exhibit spaces, ensuring the safety and accessibility of exhibits and collection objects on display or in storage must be advocated for by museum personnel. In general, the museum consortium’s Reopening Task Force efforts to guarantee the safety and integrity of member museums’ collections and spaces during the COVID pandemic crisis were successful. The Task Force’s efforts raised university risk management officials’ awareness of the unique requirements for maintaining, caring for, and securing museum collections. As a result, several organizational units assigned museum consortium members to unit-specific Integrated Safety Plan groups. Additionally, museum consortium members recognized the value in developing collections care policies and procedures that, if implemented, could be instrumental in mounting effective and substantive responses to future closures due to pandemic responses, extended staff absences, natural disasters, or other planned or unplanned closures. Based on the Task Force’s work, the museum consortium strongly encouraged the incorporation of pandemic response protocols into member museums’ risk assessments, emergency response plans, safety training, collections management policies, visitor engagement protocols, and other policies and procedures.
During museum consortium meetings and listserv exchanges, museum consortium members expressed the importance of being proactive and prepared to maintain collections access and safety, ensure museum personnel safety and well-being, and to mitigate another suite of panic responses that could be triggered by rapid and prolonged closures of their museums. Not all consortium member museums had emergency management plans or collections management policies prior to the crisis. Those that did acknowledged the need to modify their crisis response plans and policies to reflect the efficacy of protocols developed and followed during the most recent real-life crisis before memories faded. Museum consortium members’ reflections of university and museum operational adjustments made during mandated closures formed the basis of a museum consortium strategic plan for preparing for the next crisis. The plan includes:
cross-training staff in collection critical tasks such as monitoring, housing, and handling collection objects;
implementing improvements in housings and storage methods to protect objects when unattended for extended periods of time;
stocking supplies and personal protective equipment that will not degrade over time for use when handling objects (e.g., cotton masks and cotton gloves have a much longer shelf life than products containing plastics, such as nitrile gloves or elastic straps);
considering remote monitoring options including water sensors, temperature and RH monitors, and Wi-Fi enabled data loggers;
developing measures for protecting staff, volunteers, and visitors from each other as well as unseen hazards (social distancing protocols, hazard barriers and warning signs, communication plans and other networking protocols)
having plans in place for flexible working conditions and scheduling; and
keeping a comprehensive suite of recommendations and resources that can be referred to even if connectivity is compromised. This entails not relying on electronic sources and websites being maintained or available forever. Hard copies should be downloaded and printed of articles, guides, and other publications. “Paper documentation has a one-time carbon cost (its manufacture), very low maintenance cost, and we know that information recorded with good quality paper and ink will last at least 500 years (probably much longer)” (Simmons 2024).
Several resources included in the museum consortium’s Reopening Task Force’s Recommendation and references for handling and accessing museum and library collections continue to be relevant. Since 2021, new and updated resources have become available for closing museums (Bautista 2021), health crises management by museums (Jardine and Musun-Miller 2022), returning to work in museums (AIHA 2022), and housekeeping for museums (CCAHA 2022). Incorporating established research results and practices into emergency preparedness plans, collections management policies, and training now may moderate panic reactions and uncertainty during the next crisis—whenever and whatever that may be.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.