
Abstract
With cybersecurity guaranteed, a novel augmented-reality-driven medical simulation platform was designed for percutaneous renal access, which can overcome the limitations of conventional bench simulators and existing augmented reality models. This article presents a new framework design and establishes validations for the simulator for percutaneous nephrolithotomy (SimPCNL) assessment with the consideration of cybersecurity in the implementation. In particular, the new cybersecurity awareness design includes code security and hardware security. SimPCNL is mainly composed of a personal computer and two PHANTOM Omni (three-dimensional haptic device) with one stylus that mimics the percutaneous needle. A database storing clinical fluoroscopic images of percutaneous nephrolithotomy and a reproduced visual–haptic environment mimicking actual surgical performance consist of the training interface. In total, 54 professors comprising 36 medical students and 18 urologists were employed to evaluate the simulator we designed, which performed in the surgical department of Yunnan First People’s Hospital. Objective metrics and Global Rating Scale questionnaire are used to record the face and content validities, skills improvement validity, construct validity, and criterion validity. The median appraisal value of the face and content was 4 (1–5) by 18 urologists. Professors’ results demonstrated extremely better than medical students’ in total evaluation results. After a training group of medical students, SimPCNL showed a better result than the commercial training framework, especially for the quantitative feedbacks group. SimPCNL Global Rating Scale scores and objective assessment demonstrated a better result than PERC Mentor in percutaneous renal access surgical training. Training percutaneous renal access on SimPCNL is reliable and versatile through the face, content, improvement construct, and criterion validations. Furthermore, we also consider cybersecurity when implementing our novel platform.
Keywords
Introduction
Percutaneous nephrolithotomy (PCNL) is recognized as the highest stone-free rate (>90%) procedure among renal calculus therapies, especially for large-size stones (>2 cm), staghorn stone, as well as children and obesity patients. Nevertheless, the curve of surgical learning on this minimal invasive surgeries is precipitous, especially in the process of percutaneous renal access (PCA);1,2 on account of precise operation, various complications and adjacent viscera complicacy3,4 investigations indicated urologists need 45–60 cases to come up to the steady standard, beyond that, being proficient in this field requires more than 100 cases.2,5 Although the simulators are increasingly utilized to obtain, improve, and rehearse PCA technical abilities in the wet and dry laboratory, the adoption of skill learners and the dummy is restricted due to the difference of patients, inaccurate description of biological soft tissue, and physical abrasion for re-use.6–8 Compared to fluoroscopy-guided biologic and bench training models of PCA, augmented reality (AR) simulator provides a repeatable, no-radiation, easy recording, and intuitional training environment.9–11 In addition, applying cybersecurity techniques in surgical implementation can improve the privacy and security problems; Gao 12 studies the CPS (cyber-physical system) assaults in the surgical fields and presented encroachment location method based on the behavioral analysis that manifests a better capability. Machine learning–based methods are highly integrated into the surgical implementations; an architecture to solve sufferer’s private data leakage is presented based on the double-blinding technology. 13 To satisfy the diverse nature of the surgical data implantation, a novel Naive Bayes classifier is designing by T Li et al., 14 an architecture introduced to let the users forecast and supply the privacy-query with high-security consciousness. 15 To settle the data encryption and the computing costs in the process of data manipulation, Li 16 presented a multi-key, completely homomorphic encryption program to allow the data owners to coordinate with high accuracy. Li 17 presented a lightweight privacy-preserving data query framework based on the format-preserving encryption. The above-mentioned research works are concentrated on the surgical data based on origin learning, but there is no timely surgical clinic data. Robust network of data traffic classification in the medical field is also another essential issue required to be settled in the machine learning–based data processing; the robust statistical traffic classification (RTC) is the most prevalent classification way presented in 2015; 18 later, the cross-project transfer representation learning became prevalent, and its foundation is the machine learning principle, particularly based on the long short-term memory (LSTM). 19 In addition, the nearest neighbor (NN)-based means has a better classification capability in the surgical data implementation, for instance, the traffic classification correlation (TCC) 20 and the artificial neural network (ANN)-based schemes. 8
We designed a novel cybersecurity-based AR training model for fluoroscopy-guided PCA skills acquisition, which is demonstrated in Figure 1; detailed functions in comparison with PERC Mentor and the benchmark PCA trainer are shown in Table 1. To date, no simulators have employed quantitative analysis of operation techniques in PCA training, meanwhile we also integrated original dynamic fluoroscopy images, without complexity in AR PCA trainer for the first time. The aim of this study is to propose and evaluate a solution to achieve better training immersion by incorporating multiple higher-fidelity factors toward a trainee’s sensations (Vision, Touch, and Hearing) during virtual training sessions. Compared to the existing surgical simulation framework, the major contributions of this work are as follows:
A three-tier quantitative grades model is proposed and implemented toward trainee’s sensations (Vision, Touch, and Hearing) during virtual training sessions (Table 1);
For the haptic rendering, human-based percutaneous force data from real operation room have been recorded, which provide the 100% immersive haptic data source.
Periodic extension idea is employed into the force data fitting, which demonstrated a high fitting rate.

Comparison of interface and operation between augmented reality trainers and real surgery: (a) real PCNL surgical interface and the fluoroscopic image; 21 (b) hands operation in Real PCNL; (c) simulation interface of PERC Mentor; 22 (d) trainees operation on PERC Mentor; 23 (e) simulation interface of SimPCNL; and (f) trainees operation on SimPCNL.
Function comparison between PERC and SimPCNL.

It is innovative to integrate intraoperative multi-sensation data directly into haptic-enabled virtual reality (VR) medical training simulation, which could complement the training immersion and minimize the gap between virtual and reality.
Material and methods
Cybersecurity simulator design
From the urology as well as engineering aspects, our most important contribution is proposed a comprehensive framework of AR-based PCA simulator. SimPCNL is mainly composed of a personal computer (PC) and two PHANTOM Omni with a stylus, where one mimics the percutaneous needle and another imitates the palpate hand as in Figure 1(f);24,25 three-dimensional (3D) urinary system requires relevant renal meshes obtained by anonymous C-arm fluoroscopic images during actual PCNL procedures with the Philips BV Pulsera 12″, which were collected from the radiology department of hospital. We integrated the movements of virtual C-arm control corresponding with fluoroscopic navigation image on the navigate window and overlaid the drop shadow of the puncture needle on the navigation window to simulate the PCA puncture steps. To improve the immersion of the operation environment, we presented a method to combine multi-tunnel higher immersive elements with a doctor’s sensations during actual surgery to complete total immersion. Relevant high-fidelity elements contain haptic factors such as accurate biomechanical models based on experimental data collection (biomechanical experiments) and a connector designed by AutoCAD that combined with 18G puncture needle linked to desktop haptic devices, as shown in Figure 2 (first row); visual factors such as the medical images of patient personalization were segmented and reconstructed for the extremely immersive stereo virtual surgical scene addressed by Microsoft HoloLens, as shown in Figure 2 (second row); audition factors such as the sound of supervisory systems (heart supervision, anesthesia, and breathing equipment) under different surgical conditions and surgical environments include the detailed anatomic structures which cannot be represented by CT images are also recorded and reconstructed in SimPCNL, which are shown in Figure 2 (see Video, Supplemental Digital Content 1).

The implementation of SimPCNL framework with intraoperative data, which contains the multichannel data with cybersecurity content in surgery room; force information is recorded by security-enabled 6-DOF ATI sensor which punctures a porcine kidney bought from butcher and reproduced in the simulator by dual haptic devices (first line), the force transfer path is protected by the security protocol; visual rendering pipe is done by the CT image of Yunnan First People’s Hospital in China with cyberspace security transmission. PCM-D100 (SONY), the high-resolution audio recorder, is used to copy surgical machine’s normal working audio regard as the background vocality in the training scheme in the third line, and the last virtual surgery training environment rendering and model lighting are also addressed in the fourth line.
Unity 3D is a Game Engine which has integrated basic visual and audio rendering functions for the haptic rendering; a cross-platform plugin has been written to callback the force model rendering. The following is the detailed processing of each pipeline rendering: for the visual rendering pipeline, the CT images have been reconstructed to the .FBX mesh files, then the bidirectional reflectance distribution functions (BRDF), a physics-based rendering (PBR) algorithm, has been employed to post-processing rendering by the .shader language. Except for the rigid rendering part, a physics-based deformation rendering module by the Bullet plugin and the mass–spring algorithm have been also added. The force rendering is through a callback function from the HD library, and the force rendering function has been called in the Unity; because of the difference between visual (60 Hz) and haptic (1000 Hz) refreshment rate, synchronization needs to be achieved between visual and haptic rendering by the “Update” function of Unity. Finally, the physics engine needed to be invoked to integrate the visual, video, and force rendering in the training scene; to meet the real-time interactive surgical simulation, the collider box has been added in the Unity engine based on collider detection on both surgical tool and the virtual organ. Once the collision detection detected, visual, haptic, and audio embedded model will be rendering corresponding effects in real time.
Training environment
Using the fluoroscopy monitor, diamond-tripped puncture needles medial to posterior axillary line first penetrate the patient torso and pierce into renal capsule, traverse the renal cortex and pyramid, respectively, then get to the objective calyx as shown in Figure 3; every practice can be conducted with or without ministration.26,27 Both visible feedback (3D visualization and assistance) and numeral information of feedback are supplied. Ministration contains a 3D denotation of the renal anatomy structure in real time. Above-mentioned practices are used to assist learners to build a 3D mental denotation of the renal structure based on two-dimensional (2D) images and to enhance their hand–eye conformity. Every practice can be conducted separately or can be incorporated into a fulfilling learning path. Surgery time and fluoroscopy time can be used whether to select to conceal or show for time consumption; the depth and velocity bars indicated in the left bottom of the interface are dynamically connected with the distance between the needle tip and objective calyces and the insertion velocity, respectively.28,29 The angles of c-arm motion in two coordinate planes are manifested in the right bottom of the training interface. During the surgery, learners are directed to use their left-hand to palpate the ribs and common targeted position, then use the right hands to puncture into the virtual patients by the fluoroscopy navigation image, while left-handed trainees do conversely. Visual rendering is responsible for visual clues setting up according to an anonymous CT data set provided by the Yunnan First People’s Hospital, Kunming, China. The data set has a dimension of 512 × 512 × 3172 and 0.51×0.51× 0.50 mm accuracy. The CT data set (DICOM format) was first imported for region of interest (ROI) extraction using segmentation functions such as threshold and region growing. Based on the original CT data, the segmentation of the soft tissue is conducted using a threshold and region growing combined method, and for the soft tissue in each image, semi-automatic region growing method is adopted, and if it is over-segmented or under-segmented, manual modification is also used. Afterward, three urologists were invited from Yunnan First People’s Hospital to validate auto-segmentation result and perform manual correction where necessary. After that, the marching cube algorithm has been employed to reconstruct the dataset into 3D mesh model, with redundant mesh cleaning and Laplacian smoothing as intermediate steps; after that, 3D surface models can be output with the .FBX file. Finally, the mesh files have been imported into the Unity engine, and shader language is used to render the graphic effectiveness.

Demonstration of detailed surgical manipulation of SimPCNL; experienced urologists draw an empirical model of renal artery/vein based on the patient-specific CT image; after that, reconstructed this semi-artificial model in ZBrush (mesh model) and put the collision detection trigger on the surface of the vessel to assess the vascular injury.
Feedback interface
To provide the trainees detailed feedback of the surgical performance and reliable validations, there are three parts, consisting the interface, objective performance feedback, and a subjective scoring questionnaire as well as a video replay window. Objective performance feedback includes operation time (min), fluoroscopy time (min), numbers of needle punctures, infundibular injury, PCS perforations, rib injury, blood vessel injury, and successful attempts to the target calyx recorded during the operation, except for that, Global Rating Scale (GRS) scores also integrated into. The subjective scoring questionnaire includes details of the face and content investigation of SimPCNL, such as simulation of ease, graphics, training tool, and assessment tool; in addition, overall appraisal is also appended in. Each signal clause in the subjective scoring questionnaire has assessed the satisfaction by 5-point Likert-type scale. Moreover, the surgical simulation training all can be recorded in the video replay window, which facilitated the trainees to investigate and improve the PCA surgical skills in an intuitionistic aspect, which are demonstrated in Figure 4.

The feedback interface design of SimPCNL, objective, and task score windows are utilized to assess the trainees’ surgical performance, and the video replay window is for the trainee to watch the manipulation details during the training.
Evaluation
In total, 36 newbies and 18 professional urologists are employed to evaluate the augmented actual training framework. Before the beginning of the training period, a detailed introduction of framework implementation is offered to the experts and newbies groups. Specialized-built GRS questionnaire is presented for the subjective estimation.30,31 The time gap between the training period is 1 day. Subjects got back 48 h after the second training to undertake another estimated the posttest examination as same as the steps in Noureldin and Andonian 1 and Allen et al. 32 After the experiments, the whole 54 learners’ manifestations were collected by the actual questionnaires to assess our system with details of urological skills advance. The evaluation system procedures are demonstrated in Figure 5. In the posttest training session, subjects were separated into three groups, group 1 (12 novices) as the control group with all novices receiving no training of SimPCNL; group 2 (12 novices) underwent SimPCNL training mentioned above; and group 3 (12 novices) underwent not only the SimPCNL training but also the quantitative feedbacks (compared with experts group results), which include the needle trajectory, puncture force, and needle velocity as well as puncture penetration recording. After the aforementioned experiments, whole 54 learners’ manifestations were collected by the actual questionnaires to assess the SimPCNL with details of urological skills advance and be compared with the PERC Mentor’s data in criterion validations. Figure 5 shows the detailed evaluation flowchart.
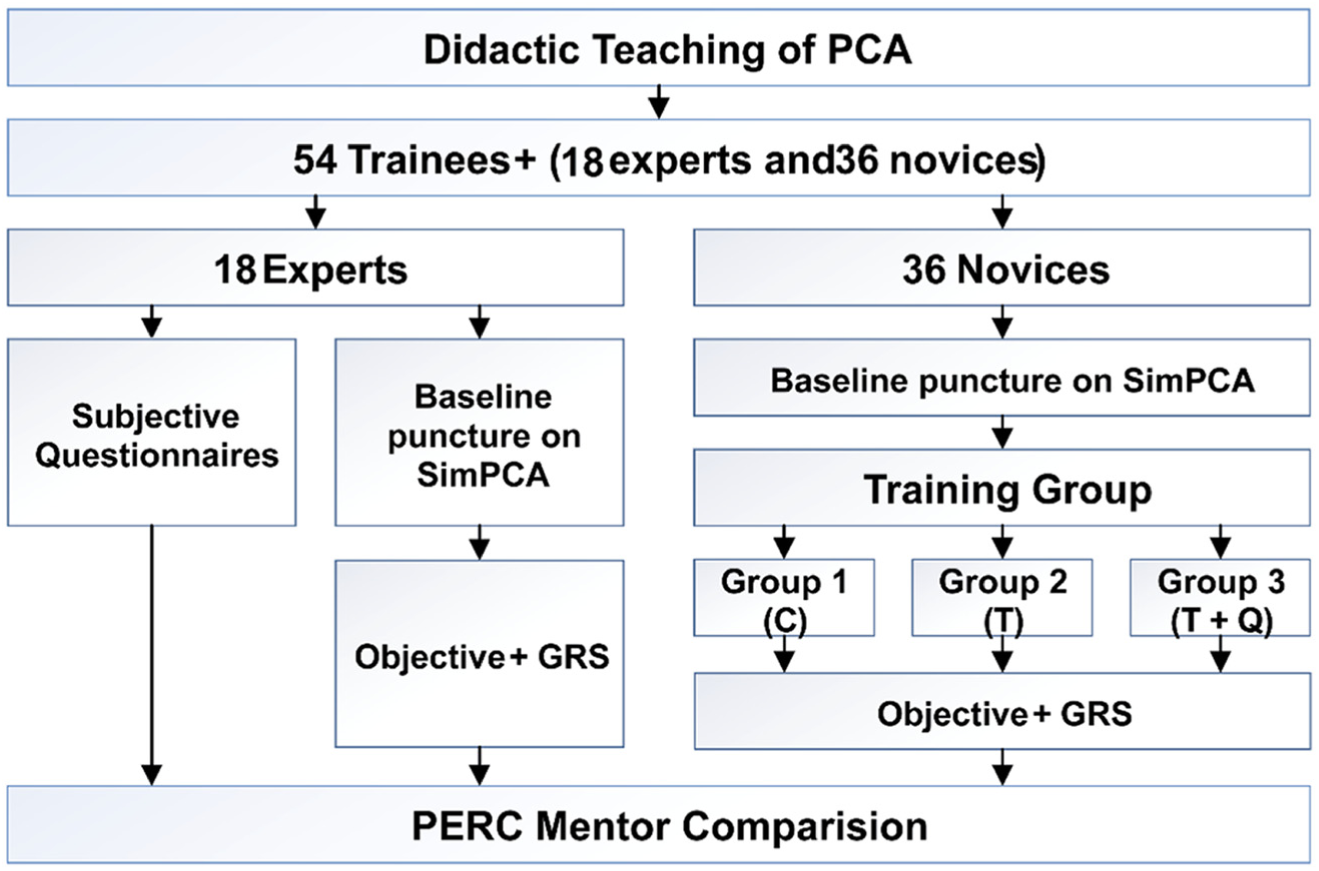
Evaluation flowchart of SimPCNL.
Results
Face and content validation
Each expert contributor can attempt to puncture on the model and easily puncture the renal stone in the calyx. The investigation manifested that 14 contributors (77.8%) would select the SimPCNL to cultivate newbies and would select the SimPCNL to show the bull’s eye skills. 16 surgeons (88.9%) deemed the kidney model as a precise anatomic expression with only 2 participants (11.1%) who did not agree with this statement. 12 contributors (66.7%) deemed that the described graphics simulation is as real as the real surgical scene. The other six were neutral about this statement. 10 (55.5%) participants thought the system has a high-performance haptic feedback, and 4 (22.2%) were neutral. 16 attendants (88.9%) deemed the X-ray-simulated guiding image as a precise expression of a real fluoroscopic image and everyone (100%) considered that avoiding radiation was essential for training.
Construct validation
Construct validity is essential to the surgical-simulation-perceived validity of the system evaluation; the bigger the score difference between the novice and expert’s groups, the better of the training system design. During our construct validation, 36 novices demonstrated a higher score in the GRS and objective assessment than the 18 experts (identify anatomy: 2.8 ± 0.1 vs 3.2 ± 0.2; design needle penetrate: 2.2 ± 0.2 vs 3.1 ± 0.2; instrument use: 2.1 ± 0.1 vs 3.1 ± 0.1; capability to conduct tasks: 2.3 ± 0.1 vs 3.4 ± 0.2; overall performance: 2.5 ± 0.1 vs 3.6 ± 0.2; surgery time (min): 6.8 ± 0.4 vs 8.9 ± 0.5; fluoroscopy time (min): 6.2 ± 0.3 vs 8.6 ± 0.3; infundibular injury: 0.4 ± 0.08 vs 1.2 ± 0.1). Number of needle punctures manifest a high p-value that is 0.002, PCS perforations p-value is 0.024, and rib injury p-value is 0.02, which means the SimPCNL system demonstrated a high performance of simulation
Improvement validation
Compared to the control group’s performance, two posttest groups show significant improvements in the PCA skills (identify anatomy: 3.43–4.26–4.31; plan needle puncture: 2.91–4.13–4.61; instrument use: 3.2–4.16–4.65; ability to perform tasks: 2.72–4.3–4.55; overall performance: 3.53–4.21–4.57; operation time (min):7.6–4.58–3.43; fluoroscopy time (min): 7.12–3.7–2.18; number of needle punctures: 3.65–1.84–1.44; infundibular injury: 1.47–0.27–0.08; PCS perforations: 2.11–0.64–0.48; rib injury: 2.48–1.01–1.04; blood vessel injury:3.19–2.01–1.23).
Criterion validation
Criterion validity is the extent to which a measure is related to an outcome; in this article, we chose the PERC Mentor as the benchmark to assess our system. Based on the previous validation of PERC Mentor in Table 3, we integrated Knudsen’s improvements validation, Mishra’s face and content validation, and Noureldin’s constructive validation as the benchmark to verify the criterion validation of SimPCNL, and the detailed results comparison is displayed in Figures 7 and 8. In improvement comparison, SimPCNL demonstrates a similar training effect as PERC Mentor, especially for the post-training group, the SimPCNL simulator demonstrated a higher score.
Discussion
There are many training models for PCNL practicing to facilitate surgical skills and acquire experience now; wet laboratory models, 33 bench models,34,35 and VR simulators 36 cannot displace each other by their own advantages and disadvantages. Compared to AR simulator, the significant advantages of other kinds of models are lively tactile sensation and original X-ray image from C-arm, which are mimicked in AR simulator.37–39 To address the first issue, we employed the quantitative analysis of operation techniques during the PCA training procedures, which means “how much of the puncture force,”“how fast of the needle velocity,”“how deep of the needle penetration,” and “how is the needle trajectory” can all be recorded and compared with the experts; afterward, these targeted collecting data of surgical exercise can narrow the gap in the sense of lively touch. Mean fluoroscopy imaging exposure time of PCA operation is 8 min and mean radiation quantity entrance skin is 110 mGy; 40 more amount of radiation may be exposing of the novice training during the C-arm facilitated models. We saved the primitive clinical fluoroscopic images of C-arm controlling during PCA operation, and these are combined with the virtual C-arm used in the virtual scene to conquer the drawback of irradiation exposing as well as unreal mimic images of C-arm training for the first time. There have been several publications about the evaluation of PERC Mentor (Table 2).
Validation comparison between former studies with this research.

GRS: Global Rating Scale; E: expert; N: novice.
Specialist for the aforementioned improvements, SimPCNL has also shown many more advantages such as portable, low-cost, and reusable without limited wastage, which are compared with PERC Mentor in Table 1. This research detailed the verifications of the simulation and demonstrated the capability of SimPCNL simulation as a stable surgical trainer for PCA surgical technique acquisition in clinical training. Face and content of SimPCNL simulator are shown in Table 2, we also employed the subjective questionnaires based on the literature, 41 and specialists who have participated in this assessment have clinical surgical experience of PCNL more than 50 times. Comparison result of both PERC Mentor and SimPCNL demonstrates the total useful evaluation as 4 in a scale of 1–5 (1 is poor and 5 is excellent).
Simulation complexity and graphics on visualization were shown a superior mark on SimPCNL, and this can be interpreted by the fact that the actual fluoroscopy images are unified in SimPCNL surgery face which provides a precise visual representation for a specialist. However, the training instruments and evaluation instruments displayed a great capability on PERC Mentor, and results can arouse by the needle simulation in the current version which utilized the actual surgical tools combined with a low-fidelity stylus of haptic device of simulation, which could be confusing for the specialists; furthermore, the missing of foot pedal fluoroscopy controls may also decrease the immersion of the environment. Compared with PERC Mentor, whole specialists had the agreement of SimPCNL as being a stable and brilliant training instrument for urology learners of the face and content performances.
In addition to the subjective verification on face and content, more target assessments also need the construct validity, which is shown in Table 3. To our knowledge, this study is the first to verify an AR PCA simulator by utilizing original fluoroscopy imaging and force recording, which provided a high-fidelity simulation of PCA construct validity. The comparison result between the GRS and the PERC Mentor is shown in Figure 6. In both PCA cases, specialists had markedly shorter removal times than newbies. In addition, SimPCNL simulator indicated a better score in the identify anatomy and the overall performance; furthermore, PERC Mentor shows a better gap between specialists and newbies in most of the GRS scores. Objective assessment results showed that the surgery and fluoroscopy time demonstrated significantly better performance than the PERC Mentor, and this may be due to the time taken for the control of C-arm in our emulation. The rib injury amount in SimPCNL is lower than the PERC Mentor, the reason should be because of the guiding hand which can detect the rib before surgery. Blood vessel injury is better and without statistically significant in SimPCNL, which is due to the reconstruction demo from the CT image which contains several blood capillary; however, lots of such vessel injuries may be ignored in the process of PCNL.
Results of face and content validities.


Construct validation between PERC and SimPCNL. The horizontal axis demonstrated the numbers, and we normalized these items in one figure to present the validation results in an intuitive way.
After the SimPCNL training, there is an obvious improvement in the novice group, which is shown in Figure 6; novice group shows a high improvement in decreasing the whole surgical time and fluoroscopy time, reducing collecting system and perforations attempting puncture amount. In the pretest and posttest GRS scores comparison, to our surprise, novice group performed better in SimPCNL training than the experts. This could be explained that the repetition of the same work increasing test–retest reliable mistake. Compared with the control group (G1), group with the quantitative feedbacks training shows the highest scores in both GRS and the objective measurement, which verified our hypothesis that the quantitative analysis of surgical skills in PCA training procedures can lower the learning curve of the PCA skills acquisition. Detailed comparison among three groups of improvement evaluations on SimPCNL is shown in Figure 7 (GRS score) and Figure 8 (objective metrics).

Improvements validation after training between PERC and SimPCNL; the horizontal axis demonstrated the numbers; we normalized these items in one figure to present the validation results in an intuitive way.

Improvements validation after training between novices and experts; the horizontal axis demonstrated the numbers; we normalized these items in one figure to present the validation results in an intuitive way.
Criterion validation includes “correlation of results of the tool with the established tool” and the predictive validity.42,43 To our knowledge, this study is the first to validate an AR PCA simulator by utilizing original fluoroscopy imaging and quantitative analysis of operation techniques, and we summarized all the validation studies of the existing benchmark PERC Mentor and compared SimPCNL with it in face, content, construct validation, and skill improvements through the subjective and objective assessments. SimPCNL GRS scores and objective evaluation showed at least a same high-level performance as PERC Mentor in PCA surgical training in Figures 8 and 9, even better in several aspects such as face and contents validation on graphic and simulation of ease, number of punctures, and rib injury, especially the group of quantitative feedbacks training.

Comparison of objective performance improvements validation after training with SimPCNL: G1 is the control group, G2 is trained after SimPCNL, and G3 are trained after quantitative feedbacks.
Each exercise can be performed independently or can be combined into a complete learning pathway. Operation time and fluoroscopy time can be chosen to hide or display for time consumption; the depth and velocity bars demonstrated in the left bottom of the interface are dynamically linked with the distance between the needle tip and targeted calyces and the puncture speed, respectively. C-arm movement angles in two coordinate planes are shown in the right bottom of the training interface. During the operation, trainees (right-hander) are guided by their left-hand palpation to locate the ribs and general targeted area and utilized right hands to puncture into the virtual patients with the navigation of fluoroscopy image, and left-handed trainees are on the contrary.
With best performances in both expert and novice groups, the cybersecurity-combined haptic-enabled AR navigation should be the most effective and reliable navigation framework. Although the haptic clues are more helpful for the experts and the AR visual clues demonstrated better performance in the novices, the combination also shows an outstanding score in the general performance. However, medical residents mentioned that haptic-enabled AR navigation may be not the critical guide cues during the real surgery; since they relied only on natural visual navigations, the advantages of AR–haptic surgical navigation sometimes cannot be displayed in several surgical tasks. Apart from that, some of the surgeons noted that the force feedback was suboptimal. Machine learning–based cybersecurity algorithms are highly, practically integrated into the medical applications; this framework is proposed based on the double-blinding technique to avoid patients’ private information leakage; in addition, the force estimator used for graphical display provides spurious force signals during motion. And, we believe the combination among the AR, haptic, and machine learning methods in our framework and these remarkable results held especially real for experience for the new generation of Da Vinci surgeons. The limitations and problems of the SimPCNL simulator, which are missing the foot pedal fluoroscopy controls and guide-wire simulation which utilized to perform puncture incorporated with precise visuals are supplied by the computer system. The comparison data of PERC Mentor are not from one experiment because we cannot find a study that includes all these validities of PERC Mentor. Evaluation of learning curve improvement and predictive validation of SimPCNL will be further studies for the training of PCA.
Conclusion
Face, content, construct, and criterion verification of our developed SimPCNL for transcutaneous renal access training shows its stability and availability in operative skills obtaining. Compared with the bench simulators and existing the cybersecurity combined AR models, SimPCNL provides novel training concepts: quantitative analysis of operation techniques during the training procedure for precise muscle memory acquisition; meanwhile without bulky C-arm machine and radiation exposure, it integrated the original X-ray images with a portable and low-cost hardware which demonstrated a high degree of performance in objective and subjective assessments. Evaluation of learning curve improvement and predictive validation of SimPCNL will be further studies for the training of PCA.
Supplemental Material
Supplemental_material – Supplemental material for Augmented-reality-driven medical simulation platform for percutaneous nephrolithotomy with cybersecurity awareness
Supplemental material, Supplemental_material for Augmented-reality-driven medical simulation platform for percutaneous nephrolithotomy with cybersecurity awareness by Yonghang Tai, Lei Wei, Hailing Zhou, Jun Peng, Qiong Li, Feiyan Li, Jun Zhang and Junsheng Shi in International Journal of Distributed Sensor Networks
Footnotes
Acknowledgements
The authors thank Professor Minghui Xiao, Dr Min Zou, Dr Jie Shen, and Mr Ran Cao of Yunnan First People’s Hospital for the helpful surgical suggestions.
Handling Editor: Weizhi Meng
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Natural Science Foundation of China (61650401) and the National Science Foundation of Yunnan Province, China (ZD2014004) of Yunnan Key Laboratory of Opto-electronic Information Technology, Kunming, China.
Supplementary material
The supplementary video is demonstrated the peg transfer experimental procedures on the SimPCNL virtual reality trainer.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.