
Abstract
Keywords
Introduction
Learning difficulty is a condition that includes all those with problems learning basic academic skills, and socio-cultural factors have a primitive role to play in it. Existing literature explains the associated factors such as substance abuse by parent/s, adverse socio-cultural environment, a deficit in learning cognitive skills, sensory deprivation, and demotivation due to deprivation in socio-linguistic interaction that can strongly negatively influence cognitive and academic performance in school children.1,2 These vulnerable children are at higher risk for learning problems (Fletcher, 2009). 3 According to Ramadas and Vijayan, 4 the prevalence of learning difficulty in India is estimated to be 35% to 50%. Studies suggest that learning difficulties are amenable to specific educational interventions. Effective educational intervention improves basic academic skills such as reading and writing and enhances the individual's academic achievement. A student's ability to learn can be fostered when the learner has opportunities to practice the new skills and receive feedback from an “expert” (such as a teacher, therapist, or parent). 5 Feedback helps them apply the knowledge or skill in day-to-day situations with lesser assistance from others.3,5
Several neuropsychological studies revealed that with the child's maturity, the cognitive, emotional, and behavioral functions during the learning process increase the capability of executing complex tasks. 6 Therefore, the learning process requires the maturation and integration of several brain areas.1,2 Literature suggests the role of the basal ganglia, limbic system, and prefrontal cortex in the learning process and self-regulation.7–10 It helps them to encode, remember, and respond appropriately to essential features of the cognitively demanding task they face. 11
The most commonly reported pattern of EEG characterization among children with a learning difficulty is to have higher absolute and relative theta power values. Excess of slow activity is noted, mainly in the theta frequency range, and an alpha activity deficit compared to typical children. 12 Excess delta activity is observed when severe disability is observed. 13 Harmony et al 13 agree with the occurrence of delta and theta activity in anterior regions, who described the electroencephalographic characteristics of children who took a reading and writing test. In addition, higher theta values were suggestive of worst performance characterized by frontal delta activity, identified as a sign of brain dysfunction. Studies also indicated that as age progresses, Beta absolute power, although this decrement is not as notorious as in delta and theta absolute power. 14 The children with a learning disability had more delta and theta absolute powers in frontocentral derivations than the control group. The absolute and relative power in delta and theta bands decreases with age while alpha power increases. 15 An increase in delta and theta powers with a concomitant decrease in alpha power seemed to be related to an immature EEG pattern. 16 Maturation of activity in the beta band passes from the center to lateral and frontal regions. 17 Studies have suggested an increase in the absolute power in the delta and theta bands, 18 while alpha and beta activity was reduced 13 with poor spatial differentiation. Children with severe reading/writing disabilities had more delta activity in frontal-temporal regions. Those with less intense disabilities had more theta activity (absolute and relative) and less relative alpha activity. 13 Findings in a study suggested that the Mean Spectral Power of EEG frequencies was higher in children with learning problems than in the control group of children of the same age. 19
Early studies on EEG characterizations in children with learning problems reported that dyslexic children have more theta power than the alpha power band in the parito-occipital region. Furthermore, significant differences were predominantly observed in the alpha, and beta frequencies, whose power was lower in children with learning problems than in mentally healthy children of the same age. The power of the EEG beta components in the right frontal and temporal derivations was lower in children with learning problems. In contrast, the delta, theta, and alpha EEG components in the left frontal derivations were higher than in the control group of children. Overall analysis suggested that retardation of the functional maturation of the brain structures is responsible for the deficit of involuntary and voluntary attention and the disorder of a systemic organization of perception and analytical–synthetic brain activity compared to the average age characteristics. 20 Arns et al 21 reported increased slow activity (delta and theta) in the frontal and temporal regions in children with dyslexia who had problems in the memory recall test. The same dysfunction in the T3 was also reported by Simos et al. 22 Mann et al 23 showed that children with ADHD had higher absolute power band values in theta, especially in the frontal and central regions, while performing cognitive tasks. The beta activity decreases in posterior and temporal regions with tasks requiring sustained attention. Beta activity (15-30 Hz) has also been related to cognitive activity. Similar results were obtained by Chabot et al, 24 Clarke et al, 25 and Lazzaro et al. 26
However, several studies also indicate that early intervention can help manage EEG characterizations during resting and activity conditions. Neurofeedback training (NFT) is helpful in the improvement of cognitive deficits. Studies report that the normalization of coherence was explicit in the theta band at T3-T4, the delta band at Cz-Fz, and the beta band at Cz-Fz, Cz-Pz, and Cz-C4. These changes indicate the connectivity between frontal and posterior association and the association between sensory and motor areas, suggesting the improvements in attention and working memory of children with learning problems. 27 Othmer et al 28 reported the successful use of NFT for academic and cognitive improvements by decreasing theta and enhancing beta. In another study, Fernandez et al 29 also reported that EEG absolute power of delta, theta, alpha, and beta bands decreased after twenty-half-hour neurofeedback sessions on children with a learning disability. In a recent study, Kaushik and Jena 30 reported a significant improvement in absolute and relative power values of waveforms achieved post-PEABLS intervention. The study reported a significant increase in relative alpha, theta, and delta band power values in the FP1FP2 and T3T4 scalp regions under both eyes-closed and eyes-open conditions.
Furthermore, some studies have focused on neurofeedback, a non-invasive mechanism, to modulate human brain activity for treating hyperactivity, impulsivity, and maintaining self-regulation among students. This system is based on real-time integration of simultaneous rtfMRI and EEG data strings. There is the feasibility of simultaneous self-regulation of hemodynamic (rtfMRI) and the human brain's electrophysiological (EEG) activities. It is a novel cognitive neuroscience research paradigm and enhanced cognitive therapeutic approaches for major neuropsychiatric disorders and neurocognitive dysfunctions. 31
The present study assessed the differences in QEEG patterns under hyperventilation, reading, and writing conditions among children with learning problems. The study aimed to analyze the relative band power of EEG activity in children facing difficulties in learning before and after the introduction of The Program for Enhancing Academic and Behavioral Learning Skills (PEABLS) sessions. An accessible school-based cognitive-behavioral intervention, PEABLS, focuses on developing self-regulation skills and resiliency and improving students’ academic performance with learning difficulties.5,32 PEABLS was introduced to urban slum-based school children from grade 3 to grade 7 (age range 8-12 years) with learning difficulty for over 2 months (15 sessions, twice a week) to learn and practice cognitive-behavioral skills and academic concepts. EEG was applied before and after the intervention and was presented as a measure. EEG is an efficient means that helps to acquire brain signals corresponding to different states from the scalp surface. It is a notable tool for studying the neurocognitive processes underlying human behavior because of its very high time resolution and ability to capture cognitive processes in the time frame in which cognition occurs. 33 Although several pieces of research have been done to identify the common correlates of learning problems in school children, it is difficult to state the specific EEG characteristics of learning difficulty due to a lack of common consensus among the studies. EEG data can help clinical psychologists and neuropsychologists to establish an accurate diagnosis. In clinical practice, EEG has emerging potential for detecting cognitive dysfunction. It contributes to early identification to promote early intervention to facilitate student learning skills. This study reports the pre- and post-EEG relative band power of alpha, beta, theta, delta, and gamma activations at FP1FP2, T3T4, and O1O2 scalp locations—applicability. The primary research questions were: (1) Does the application of intervention on children with learning difficulty changes the band power values of QEEG?; (2) what are the patterns of EEG characterizations during hyperventilation, reading, and writing conditions, before and after intervention?
Methods
Design
The present study utilized a pre-test and post-test quasi-experimental research design to check the difference in EEG characterizations before and after PEABLS intervention.
Program for Enhancing Academic and Behavioral Learning Skills (PEABLS): PEABLS is a self-designed cognitive-behavioral group intervention program for school students of 8 to 12 years of age (3rd-7th grade) who have difficulty in learning. The intervention aims to enhance self-regulation learning and resilience skills and assist students in applying those skills to meet established goals of improving their academic performance. The PEABLS intervention was carried out in 15 sessions; each session lasted 60-min and was delivered twice a week. It consists of 3 components: (1) self-regulation therapy, (2) resilience-building training, and (3) academic remediation. The first helps the student to identify their negative beliefs and allows them to develop cognitive flexibility when confronted with negative thoughts. In the second part of the program, students were taught to resolve interpersonal conflicts, assertive communication and deal effectively with conditions of aggressive spells, passivity and make effective decisions in various day-to-day situations. The third part of the program consists of an individualized educational program (IEP) to help them to cope with conceptual deficits. The first 2 components of the program were conducted at school premises during school hours. The third component of academic remediation involved the IEP, scheduled after school hours at a university lab near their residence. It focused on clearing conceptual deficits and enabling the students to cope with the school curriculum. As part of this program, students’ baseline performance was assessed, and teaching modules were designed to meet their specific needs. In their intervention causative model, Zimmerman and Martinez-Pons34,35 proposed that with the enhancement of self-regulated skills, learners become aware when they know facts and skills or when they do not know. Improvement in a fundamental aspect of learning (including self-regulation, behavior, emotions, and resilience) in children with learning difficulties helps them learn to pay attention, regulate their behavior, and control their impulses. Empowering executive functioning skills in students gives promising results in the domains of academic, social, and personal life, where they often require problem-solving and decision-making skills. 36 Recipients of PEABLS intervention exhibited improvements in cognitive skills like working memory, verbal and written expressions, self-regulation and resilience skills, and academic skills.30,32
Sampling
Fifty students from primary and elementary government-run schools participated in the study. Their age ranged from 8 years to 12 years (mean age = 10.38, SD = 1.39), and they studied in grades 3 to 7 (mean = 4.78, SD = 1.32). All participating children belonged to urban slums. The average family income of participants was ₹18 420 monthly. Their mean body mass index was 13.88 (SD = 2.01). They had shown low academic performance for 2 years before starting the study and behavioral issues at school. The mean pre-intervention academic aggregate score was 37.9%, and the mean post-intervention academic aggregate score was 47.78%, with 48% of students scoring in the 31% to 40% range and 34% of students scoring in the 51% to 61% range. Their vulnerability to dropping out of school due to frequent academic failures and behavioral problems highlighted their need for this intervention, especially since evidence indicates the problems in multiple domains further elevate that risk.37,38
Permission from concerned authorities was taken before approaching the Principal of the school. Class teachers of grades 3 to 8 were briefed about the project, and the list of students with learning problems was received. Parents of those students were oriented about the significance of intervention in the annual parent–teacher meeting. The authors considered the student's academic records for the last 2 years, the teacher's feedback, and the parent's report to identify the students with learning problems. Inclusion criteria for the study comprised the following: (1) age range from 8 to 12 years (3rd to 7th grade), (2) obtained IQ score ≥ 50 percentile on Raven's Color Progressive Matrices (RCPM), 39 (3) failed in class for 2 consecutive years, (4) low classroom participation and co-curricular activity, and (5) behavioral issues. The exclusion criteria comprised (1) obtained IQ score ≤ 50 percentile on Raven's Progressive Matrices, (2) sensory impairments, (3) any known case of developmental disorder, and (4) physical disability (as they may have associated co-morbidities). The parents of the students signed the written consent. The students’ assent was taken to confirm their study participation. After fulfilling the above criteria, 50 students with learning problems were identified. None of them withdrew from the study after the intervention started. The Indian Council for Social Science Research and the Department of Psychology, University of Delhi, approved the study, which followed the Ethical Principles for Medical Research Involving Human Subjects established by the Declaration of Helsinki. The process of student selection, assessment, and intervention was conducted under the supervision of a Clinical Psychologist. EEG was recorded at the Psychophysiology Lab, Department of Applied Psychology, University of Delhi.
Procedure
The baseline assessment of the student participants was only shared with teachers and respective parents to maintain confidentiality. The PEABLS intervention was planned for students with low academic performance and behavioral issues. The study was conducted in 3 phases. During phase I, IQ scores and scores for level of learning disability were obtained using RCPM and Diagnostic Test of Learning Disability (DTLD), 40 respectively, for screening all identified students. Those who obtained IQ ≥ 50th percentile in the RCPM and a score of ≥40% in the DTLD were further subjected to the Digit Span Test, forward and backward, a sub-test of Malin's Intelligence Test for Indian Children 41 to assess their working memory status. The Bender Gestalt Test (BGT) 42 to evaluate visual-motor functioning and EEGs was also recorded. For the baseline level of academic performance, the aggregate scores of each student received in their final term in the previous grade were noted. After the pre-assessment, phase II of the study proceeded, where all the students were introduced to PEABLS intervention that continued for 2 months (15 sessions, twice a week). Then immediately after the 2 months intervention, in phase III, they were re-assessed on the cognitive measures, and EEG patterns were recorded. Post-intervention academic performance of these students was based on aggregate scores received after mid-term exams of their current grade. The age and grades of the participants were approximately normally distributed, with skewness of −0.21 (SE = 0.34) and kurtosis of −1.17 (SE = 0.66) for the age variable and skewness of 0.15 (SE = 0.38) and kurtosis of −1.11 (SE = 0.66) for the grade variable.43,44
Measurements
The students were assessed twice, ie, before and after the intervention, with EEG recording and the cognitive measurements described below.
Cognitive measurements
The Diagnostic Test of Learning Disability (DTLD) is a screening tool for measuring students’ visual and auditory perception and cognitive functioning. Raven's Colored Progressive Matrices (RCPM) is the standardized measurement used to assess students’ IQ levels. The Digit Span Test, forward and backward, a sub-test of Malin's Intelligence Test for Indian Children, was conducted to assess students’ working memory status. The Bender Gestalt Test was administered to assess students’ visual-motor functioning, developmental disorders, and neurological impairments.
Electrophysiological measures
QEEG of the participants was recorded twice at a gap of 2 months, at the psychophysiology lab of the Department of Applied Psychology, University of Delhi. The psychophysiology lab is well ventilated with a moderated-lighted, soundproof room. The subject was allowed to sit comfortably on a chair with an attached table for the subject to write and read. The subject was instructed to avoid unnecessary body movement except for writing and reading activities. EEG was acquired for one subject at a time during 3 conditions, ie, 120 s each during each condition during hyperventilation, writing, and reading tasks. During hyperventilation, the subject was asked to inhale and exhale rapidly for 2 min. For the writing task, subjects were asked to write a paragraph they had learned during IEP; for the reading task, subjects were asked to read a section from their respective school English textbook. The EEG recording was done in the afternoon after school hours. The subject was allowed to take proper rest after their lunch. EEG data were acquired using BIOPAC system MP36 (BIOPAC Systems, Inc.) from the 4 digital channels of the 10–20 system and analyzed with AcqKnowledge 4.1 software MP150, referenced to the linked earlobes (A1–A2). The reference of EEG bandwidth of waveforms was placed within the range of 0.5 to 70 Hz. The input impedance and output impedance of all electrodes were set at 2 MΩ and 50 Ω, respectively, with a gain of 50 000. EEG data were sampled at 2000 samples/second for every 0.5 ms. The raw EEG signals were processed with the help of AcqKnowledge software, and Delta (0.5-4 Hz), Theta (4-8 Hz), Alpha (8-13 Hz), Beta (13-30 Hz), and Gamma frequency (30-60 Hz); frequency band was then extracted from it. The average absolute and relative power of frequency bands for 50 participants was calculated in hyperventilation, writing, and reading conditions. EEG was recorded with 6 electrodes placed according to the international 10–20 system on the FP1FP2, T3T4, and O1O2 scalp locations. After raw EEG data were extracted from MP36 BIOPAC, the independent component analysis (ICA) was done using BIOPAC software. The artifacts were estimated using reference channels. Further, fast Fourier transformation (FFT) (epochs were set at 120 s), power spectrum density (PSD), absolute band power, and relative band power were calculated using MATLAB coding. The questions addressed in the study are as follows: (1) Determine the impact of the intervention on students’ EEG parameters; (2) Correlate EEG measures with cognitive measures utilized in this study.
Data Analysis
Data obtained was compared on cognitive and electrophysiological variables assessed at baseline and post-intervention. Recording of EEG was taken while hyperventilation, writing, and reading task conditions. The power values for absolute and relative EEG bands were calculated. The results of EEG variables of pre- and post-intervention in the absolute and relative band power values of delta, theta, alpha, beta, and gamma of the qEEG were compared using a t-test for paired samples. Correlation between qEEG parameters and cognitive data obtained from IQ scores on RCPM, BGT, and working memory status on digit span (forward and backward) was also studied using Pearson's correlation analysis. A paired t-test was performed to compare the pre- and post-assessment of absolute power (AP) and relative power (RP) of EEG waveforms.
Results
Table 1 depicts a paired sample t-test to compare EEG relative values (during hyperventilation condition) of alpha, beta, and theta on prefrontal and temporal locations for students with learning difficulty before and after the intervention. Mean scores differed significantly at FP1FP2 Alpha (t = 2.30, P = .05), Beta (t = 2.51, P = .01), and T3T4 Theta (t = 2.28, P = .05) (Fig. 1). During the writing condition, EEG relative band power values of alpha, beta, theta, and delta on FP1FP2; T3T4; and O1O2 locations (Table 2). There was a significant difference in the mean scores of FP1FP2 Alpha (t = 1.91, P = .05), T3T4 Alpha (t = 1.98, P = .05), and O1O2 Alpha (t = 1.94 P = .05). A significant difference was reported at FP1FP2 Beta (t = 4.03, P = .001), T3T4 Beta (t = 3.53, P = .01) and O1O2 Beta (t = 2.97, P = .05). There was a significant difference in the mean scores of FP1FP2 Theta and FP1FP2 Delta (t = 1.98, 2.08, respectively, P = .05) (Fig. 2). Table 3 (during reading condition) compares EEG relative values of alpha, beta, theta, and delta on FP1FP2, T3T4, and O1O2 locations for the groups of students with learning difficulty before and after the intervention. There was a significant difference in the mean scores of T3T4 Alpha (t = 4.42, P = .001), O1O2 Alpha (t = 1.99, P = .05), T3T4 Beta (t = 3.27, P = .01), FP1FP2 Theta (t = 2.40, P = .01), T3T4 Theta (t = 2.52, P = .01), and T3T4 Delta (t = 1.97, P = .05) (Fig. 3).
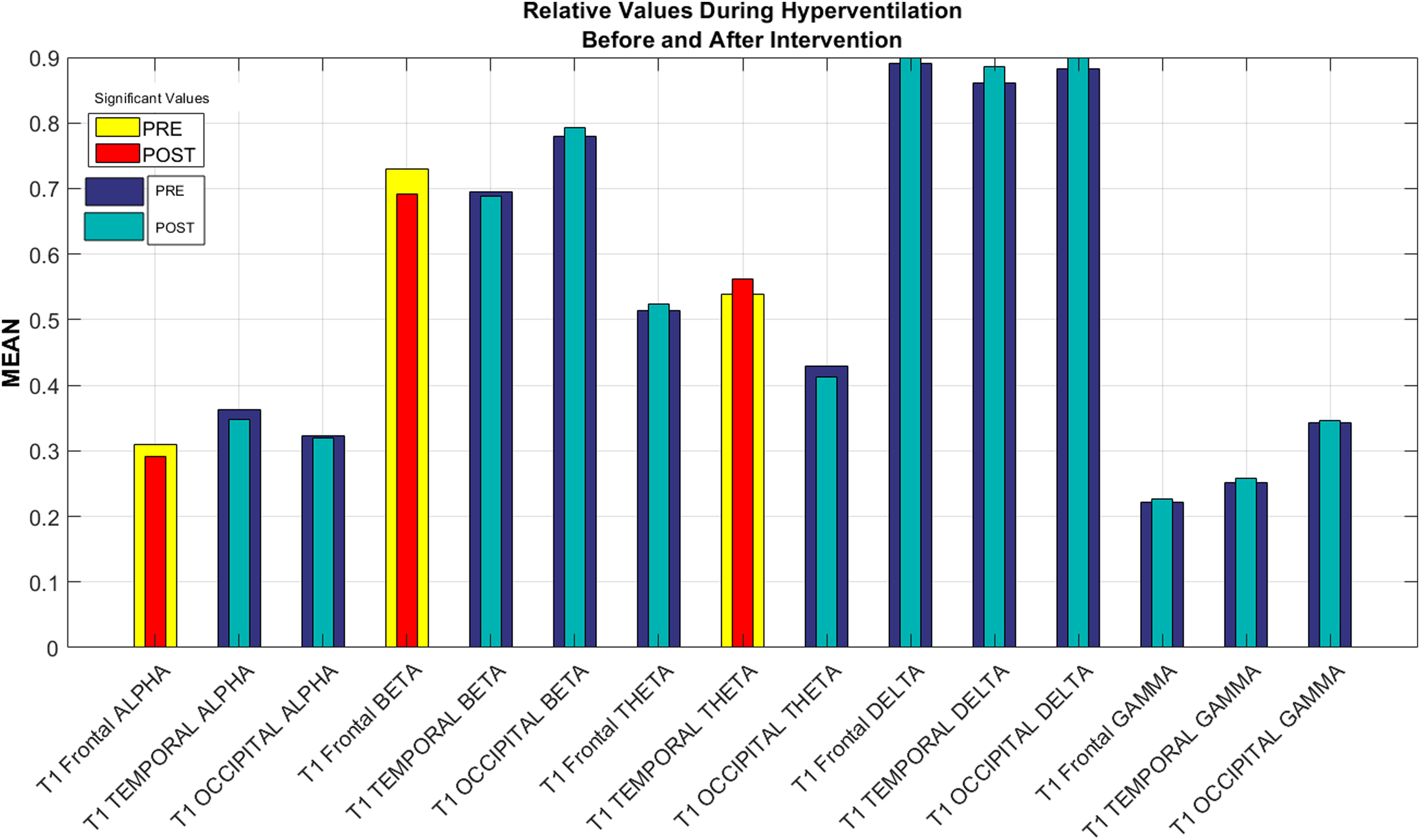
Electroencephalographic variables relative scores during hyperventilation condition, before and after intervention.
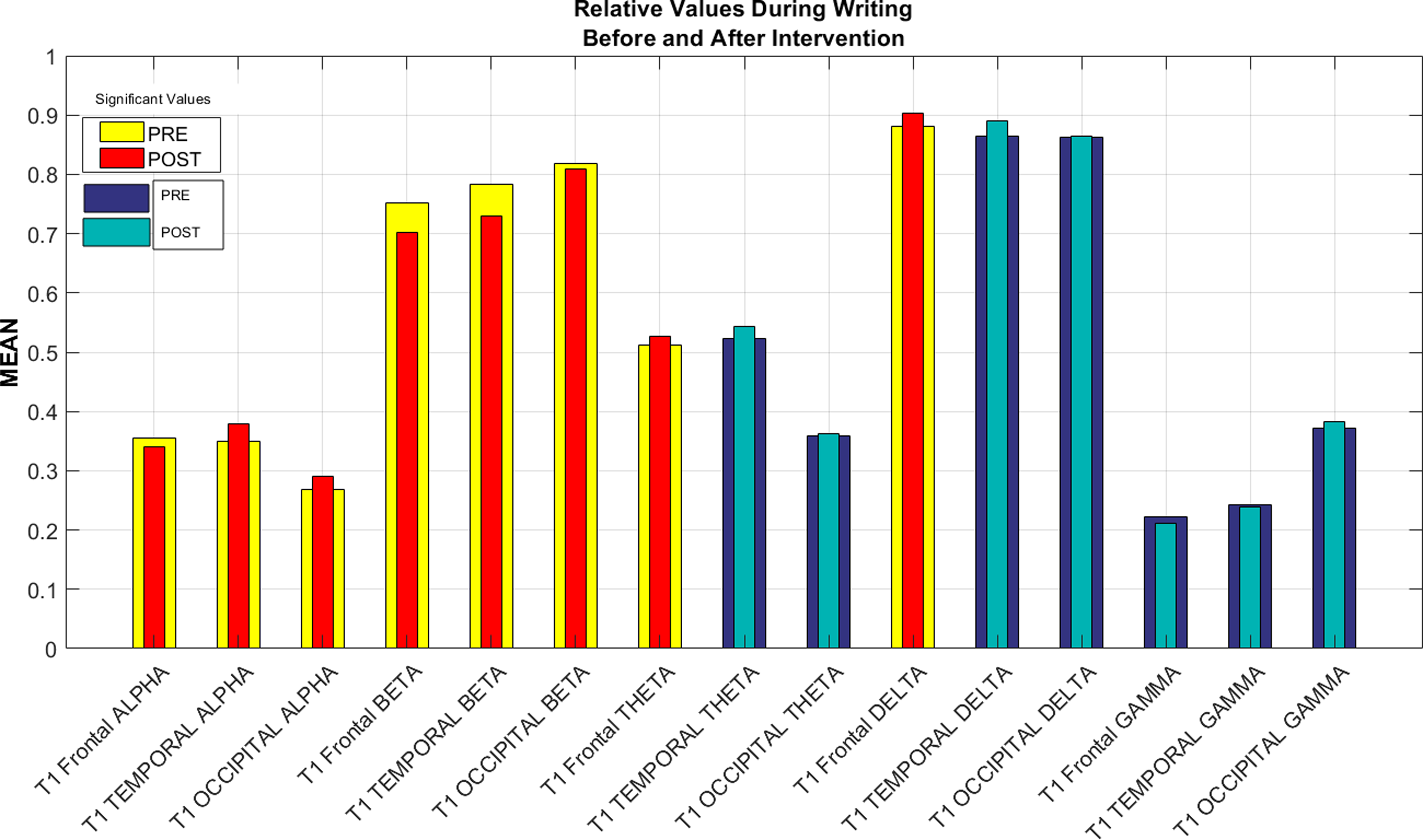
Electroencephalographic variables relative scores during writing condition, before and after intervention.
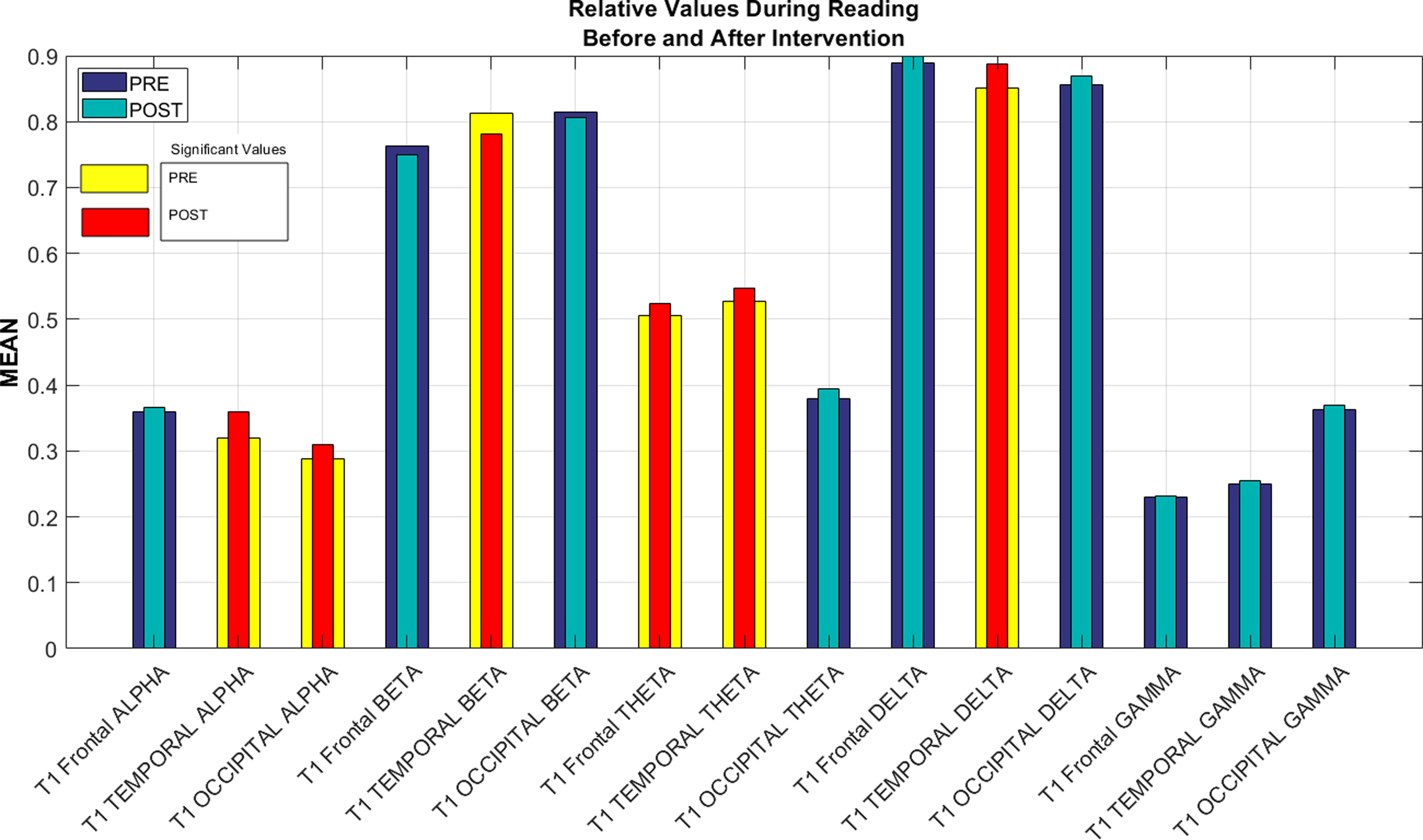
Electroencephalographic variables relative scores during the reading condition, before and after intervention.
Comparison of Electroencephalographic Variables Relative Band Power Values Before and After Intervention for the Groups of Students With Learning Difficulty and the Value for P in the Respective Comparisons During Hyperventilation Condition.
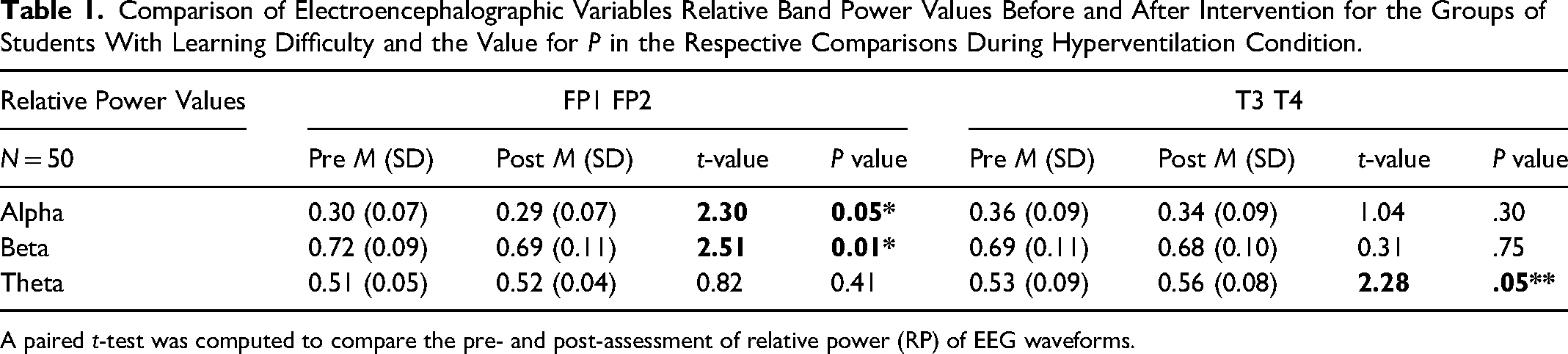
A paired t-test was computed to compare the pre- and post-assessment of relative power (RP) of EEG waveforms.
Comparison of Electroencephalographic Variables Relative Band Power Values Before and After Intervention for the Groups of Students With Learning Difficulty and the Value for P in the Respective Comparisons During Writing Condition.
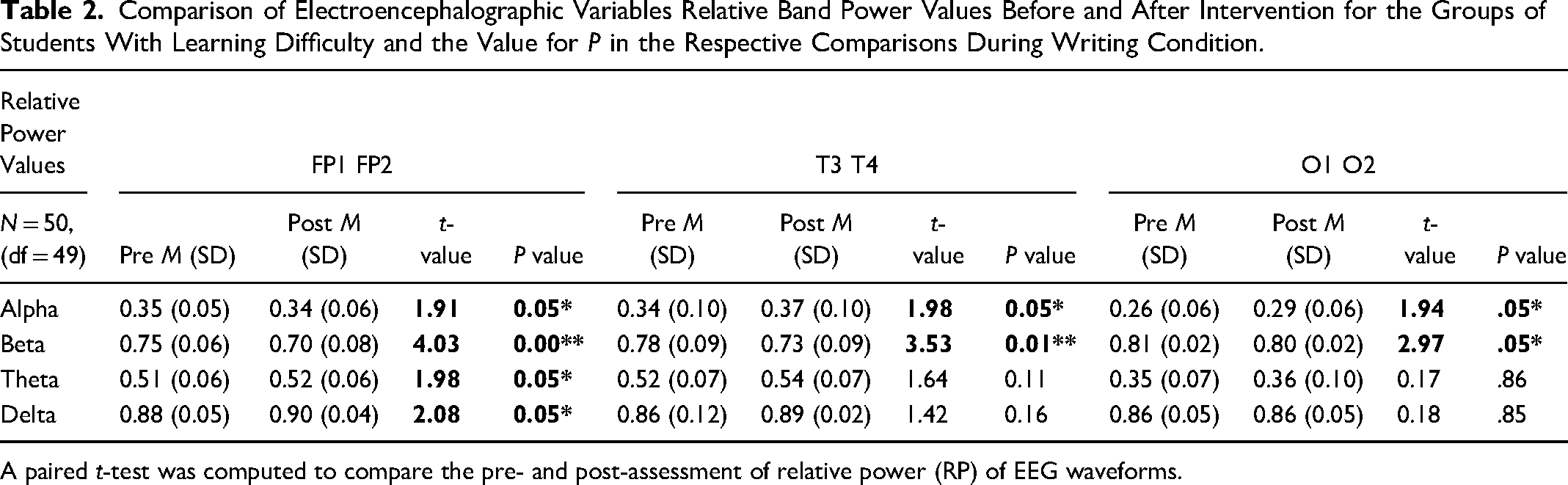
A paired t-test was computed to compare the pre- and post-assessment of relative power (RP) of EEG waveforms.
Comparison of Electroencephalographic Variables Relative Band Power Values Before and After Intervention for the Groups of Students With Learning Difficulty and the Value for P in the Respective Comparisons During the Reading Condition.
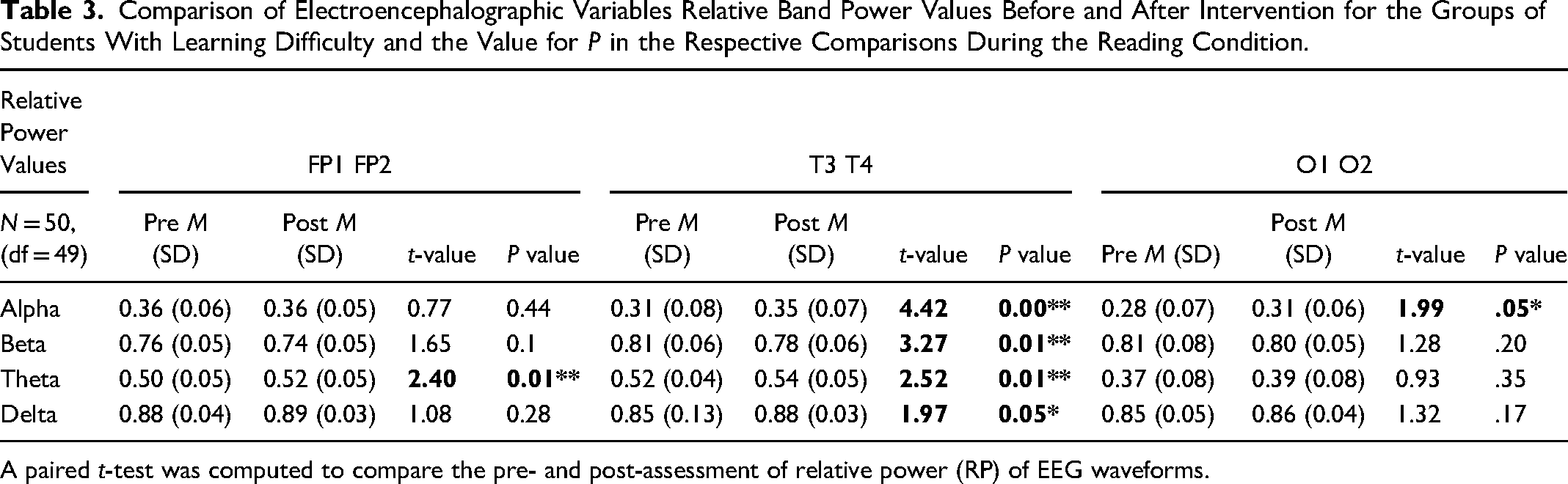
A paired t-test was computed to compare the pre- and post-assessment of relative power (RP) of EEG waveforms.
Table 4 depicts a paired sample t-test to compare EEG absolute values of alpha, beta, theta, delta, and gamma on prefrontal, temporal and occipital locations for students with learning difficulty before and after intervention during the hyperventilation condition. A significant difference in the mean score of T3T4 Beta (t = 1.93, P = .05). During the writing condition (Table 5), a significant difference was noticed in the absolute value of FP1FP2 Alpha (t = 1.95, P = .05), T3T4 Beta (t = 3.95, P = .01), FP1FP2 Theta (t = 3.49, P = .01), O1O2 Theta (t = 2.16, P = .05), O1O2 Delta (t = 1.99, P = .05), and T3 T4 Gamma (t = 2.51, P = .05). Table 6 states that the mean score had significant differences at the absolute value of FP1FP2 Beta (t = 1.96, P = .05), T3T4 Beta (t = 4.44, P = .01), T3T4 Delta (t = 1.94, P = .05), and T3 T4 Gamma (t = 2.61, P = .01).
Comparison of Electroencephalographic Variables Absolute Band Power Values Before and After Intervention for the Groups of Students with Learning Difficulty and the Value for P in the Respective Comparisons During Hyperventilation Condition.

A paired t-test was computed to compare the pre and post-assessment of absolute power (AP) of EEG waveforms.
Comparison of Electroencephalographic Variables Absolute Band Power Values Before and After Intervention for the Groups of Students with Learning Difficulty and the Value for P in the Respective Comparisons During Writing Condition.
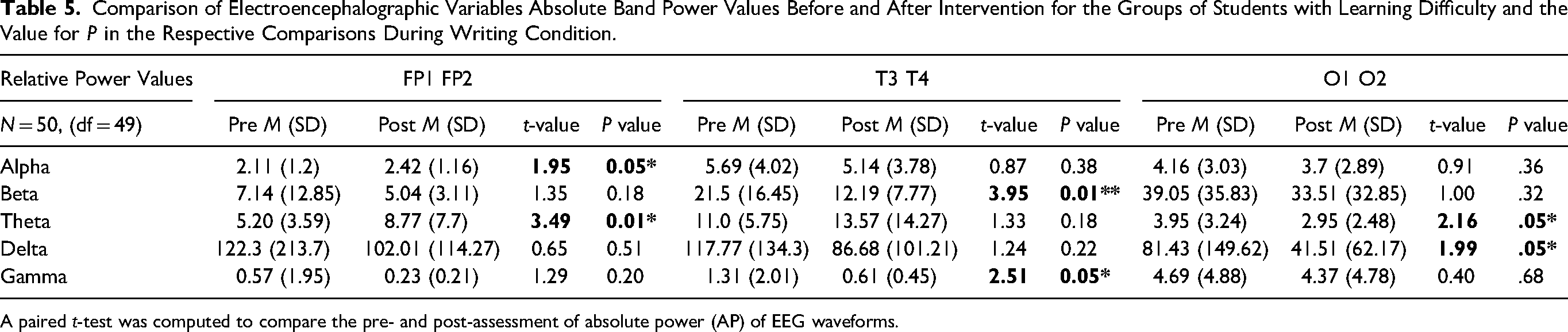
A paired t-test was computed to compare the pre- and post-assessment of absolute power (AP) of EEG waveforms.
Comparison of Electroencephalographic Variables Absolute Band Power Values Before and After Intervention for the Groups of Students with Learning Difficulty and the Value for P in the Respective Comparisons During Reading Condition.

A paired t-test was computed to compare the pre- and post-assessment of absolute power (AP) of EEG waveforms.
Pearson's correlation coefficient was calculated between relative EEG band power values on scalp locations (FP1FP2; T3T4; and O1O2) and IQ, working memory, and BGT. Table 7 depicts the correlation between post-intervention cognitive variables and EEG relative band power acquired during 3 conditions: hyperventilation, writing, and reading. The table suggests that during hyperventilation conditions, there is a positive correlation between O1O2 alpha band power values and academic scores (r = 0.3, P ≤ 0.05) and IQ scores (r = 0.29, P ≤ .05). FP1FP2 Beta (r = −0.32, P ≤ .05) and T3T4 Delta (r = −0.26, P ≤ .05) had a significant negative association with working memory. During the writing condition, the academic score was related to O1O2 alpha (r = 0.29, P ≤ .05) and T3T4 delta (r = 0.28, P ≤ .05); and negatively related to O1O2 gamma (r = −0.26, P ≤ 0.05). IQ was positively associated with O1O2 alpha (r = 0.28, P ≤ .05) and negatively associated with O1O2 gamma (r = 0.27, P ≤ .05). Working memory was positively associated with T3T4 alpha (r = 0.31, P ≤ 0.05), O1O2 alpha (r = 0.32, P ≤ .05), and T3T4 delta (r = 0.31, P ≤ 0.05), while negatively associated with T3T4 theta (r = −0.38, P ≤ .05) and O1O2 gamma (r = −0.38, P ≤ .05). DTLD scores were also related to O1O2 alpha (r = 0.46, P ≤ .01), O1O2 beta (r = −0.25, P ≤ .05), T3T4 delta (r = 0.32, P ≤ .05), and O1O2 delta (r = 0.26, P ≤ .05). BGT scores were positively associated with the T3T4 delta (r = 0.31, P ≤ .05) and O1O2 gamma (r = 0.29, P ≤ 0.05). The academic score was positively related to O1O2 alpha (r = 0.42, P ≤ .01) during the reading condition and negatively linked to the T3T4 delta (r = −0.25, P ≤ .05). IQ score was negatively associated with the FP1FP2 beta (r = −0.27, P ≤ .05) T3T4 delta (r = −0.35, P ≤ .05). Working memory was positively linked with O1O2 alpha (r = 0.36, P ≤ .01) while negatively related to O1O2 beta (r = −0.29, P ≤ 0.05) and T3T4 delta (r = 0.45, P ≤ .01). DTLD score was associated with O1O2 alpha (r = 0.56, P ≤ .01), O1O2 beta (r = −0.36, P ≤ .01), T3T4 delta (r = 0.45, P ≤ .01), and T3T4 gamma (r = 0.31, P ≤ .05). At the same time, the BGT score was associated with O1O2 alpha (r = −0.4, P ≤ .01), T3T4 beta (r = −0.28, P ≤ .05), and T3T4 delta (r = 0.25, P ≤ .05).
Correlation of EEG Relative Power Data of Conditions—Hyperventilation, Writing, and Reading and Cognitive Variables.
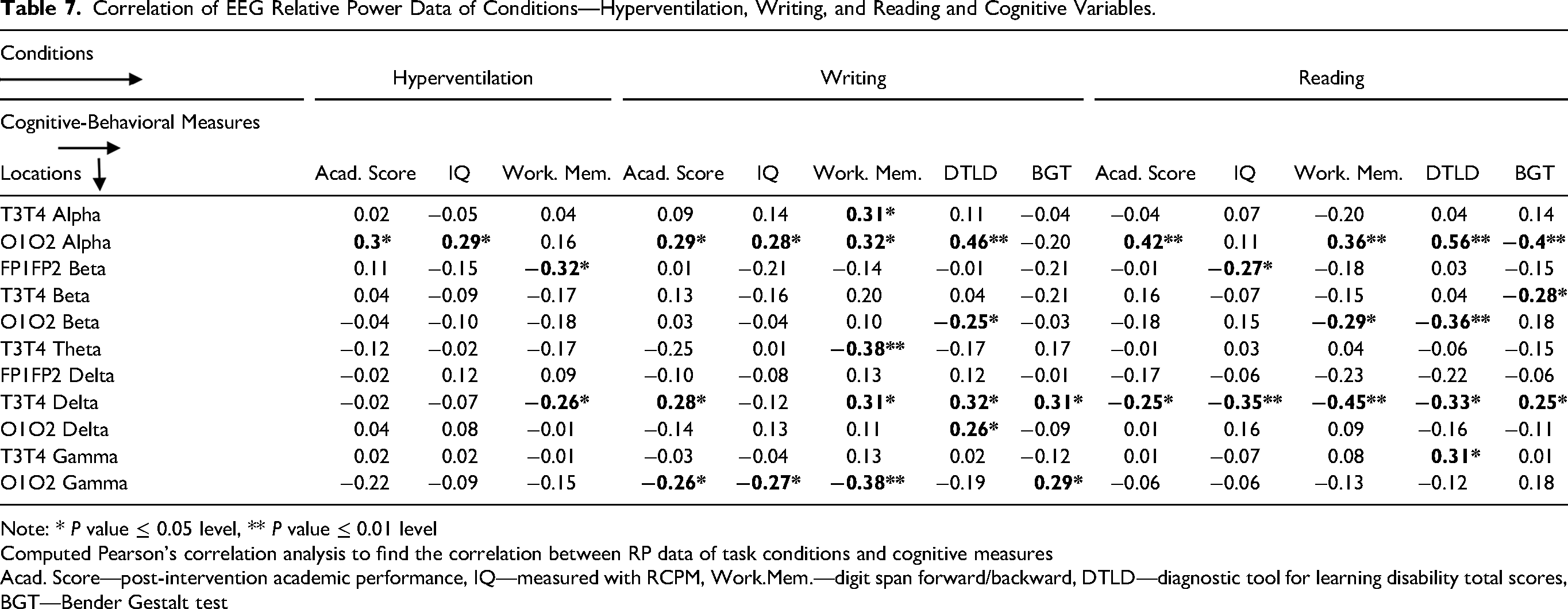



Note: * P value ≤ 0.05 level, ** P value ≤ 0.01 level
Computed Pearson's correlation analysis to find the correlation between RP data of task conditions and cognitive measures
Acad. Score—post-intervention academic performance, IQ—measured with RCPM, Work.Mem.—digit span forward/backward, DTLD—diagnostic tool for learning disability total scores, BGT—Bender Gestalt test
Discussion
The present study aimed to evaluate pre and post-PEABLS intervention qEEG activity under hyperventilation, writing, and reading conditions, among students with learning problems. PEABLS, a cognitive-behavioral intervention, has significantly improved academic, cognitive, and behavioral measurements.5,30,32 Some significant findings included increased relative alpha power values at the FP1FP2, T3T4, and O1O2 scalp locations during writing and reading conditions. The results showed overall post-intervention changes in relative and absolute power values. Related studies have emphasized that during the process of brain maturation up to the adult stage, there is a progressive decrease in delta, theta, and alpha activities. The findings show that the immaturity of brain development corresponds to the high powers of the delta, theta, and alpha bands in children with learning problems. As Harmony et al 13 reported in the evolutive study, EEG abnormalities tend to disappear with maturation. Children with learning problems have higher absolute and relative delta and theta power values compared to same-age children. This has been interpreted as a lag in brain maturation.15,45,46 Klimesch 47 explained this pattern of deficiencies these children exhibit because frontotemporal regions are directly related to language processing and general attention processes, memory, and executive processes. Brain maturity signifies the presence of posterior alpha with adequate reactivity.
Lubar et al 48 suggested that higher theta and lower alpha activity were observed among children having problems in learning and difficulty in the attention process. John and associates 49 also observed a high level of delta theta and lower R alpha power values, indicative of EEG activity slowing among children with learning problems and deviant development.50,51 Harmony et al 13 further reported that high delta and theta values and lower alpha power were related to compromised educational performance. In contrast, the high alpha level and lower theta indicate moderate learning difficulty. It was further added that higher theta and lower alpha, and high delta reflect cerebral dysfunction. Another study stated that students with learning problems noticed the excessively slower activity of theta power 52 and an alpha activity deficit 53 compared to typical children.
Similarly, in a study, authors mentioned that EEG studies on children with LD-NOS compared to normal children have demonstrated higher theta and lower alpha and beta activity during resting conditions.12,54 Studies have suggested an increase in the absolute power in the delta and theta bands, 17 while alpha and beta activity was reduced 55 with poor spatial differentiation. Children with severe reading/writing disabilities had more delta activity in frontal-temporal regions. Those with less intense disabilities had more theta activity (absolute and relative) and less relative alpha activity. 56
Pearson's correlation coefficient between relative EEG band power values on scalp locations (FP1FP2; T3T4; and O1O2) and cognitive measures suggested a significant correlation during hyperventilation, writing, and reading conditions. The correlations between the EEG variables at the various electrodes and IQ were broad in their extension and sometimes in frequency bands could, in part, be because the tests measured heterogeneous abilities.57,58 Clarke et al, 59 in their study, suggested that children with learning problems have more significant anomalies such as high alpha, excess delta, and during hyperventilation conditions, higher EEG activities. Lower theta and higher alpha and beta are noticed during early childhood while studying developing children. 60 Fonseca et al 12 reported a high positive correlation in children with learning disabilities between the relative power alpha 2 and the verbal, performance, and total IQ values. Such correlation can be explained by the fact that the alpha 2 power is associated with greater maturity of the brain's electrical activity, as already shown in healthy children.13,61,62
Limitations
The best effort was made to control the variables under study, but not all. Due to a paucity of time and resources, the baseline and post-intervention assessments with EEG were not done for the control group. Therefore, the comparison of the experimental group and the control group was not possible. Moreover, students’ age groups of 8 to 12 years varied (corresponding to the education levels of 3rd to 7th grade) could have caused heterogeneity. Varying stages of brain development during this phase may modulate the learning process. The maturation effect may also significantly affect the results. It can be suggested that future researchers maintain sample homogeneity to prevent errors in results.
Conclusion
The present study sheds light on several concerns related to biological brain aspects involved in children with learning problems, with particular reference to brain immaturity as one of the possible factors in the genesis of such conditions among children.
Footnotes
Declarations
I hereby declare that the work described in the manuscript has not been published before, and it is not under consideration for publication anywhere else. I also declare that the publisher will not be held legally responsible should there be any claims for compensation. I further declare the following details:
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, and authorship of this article: This work was supported by the Indian Council of Social Science Research (grant number 3-80/17-18/PDF/GEN)
Ethics Approval
The study was approved by the responsible authorities of Department of Psychology, University of Delhi, where the study was carried out and Indian Council of Social Science Research (ICSSR file no. 3-80/17-18/PDF/GEN), from where fellowship was approved.
Consent to Participate
Written consent forms were signed by the parents of the student participants, and ascent was given by the student to participate in the study.
Consent for Publication
The publication of the manuscript has been approved by all co-authors and provides consent for publication of the manuscript entitled “QEEG Characterizations during Hyperventilation, Writing and Reading Conditions: A Pre–Post Cognitive-Behavioral Intervention Study on Students with Learning Difficulty.”.
Availability of Data and Material
Data is secured with the corresponding author; it will be made available whenever reviewers will require for verification.
Code Availability
Not Applicable