
Abstract
There is accumulating evidence for collective approaches to leadership, where multiple individuals share leadership roles, but there remains a lack of theory-informed research on how collective leadership is fostered in practice. This study evaluated the impact of a collective leadership intervention, exploring what works for whom, how, and under what circumstances through a mixed-methods realist evaluation of four case studies. Eight context-mechanism-outcome configurations (theories) were extrapolated that elucidate the mechanisms triggered to drive outcomes in particular settings. This is the first study to apply a realist lens to understand collective leadership and articulate the generative mechanisms that enable/inhibit collective leadership in healthcare teams.
Introduction
In the context of escalating multimorbidity and the concomitant shift toward integrated care, healthcare delivery is becoming increasingly complex, requiring collaborative approaches to ensure optimal patient care. Such ways of working require healthcare to be delivered via multidisciplinary teams, where medical staff, nursing staff, health and social care professionals, and other professional groups are expected to coordinate and navigate systems within and across teams and organisations. Team training has consistently been found to improve team performance (Carpenter et al., 2017; Salas, Cooke, et al., 2008; Salas, DiazGranados, et al., 2008). Despite a strong body of evidence to support this, dedicated time to reflect on team operations is not common in healthcare (Miller et al., 2007) and may be perceived as taking time away from direct patient care. Teams that are reflexive tend to learn from previous mistakes, errors, and refine team processes, which in turn will improve the performance of the team (Nawaz et al., 2014; Schippers et al., 2013; Tucker et al., 2007). This is especially important for teams that are not performing optimally (Schippers et al., 2013). Protected time to reflect, agree priorities and plan is crucial for promoting multidisciplinary team working (Miller et al., 2007) and is associated with team innovation and adaptability (West, 2000).
Given teams are the mechanism through which care is delivered, this has led to calls for a shift away from traditional, hierarchical ‘command and control’ cultures of leadership in healthcare where one individual is responsible for leading the team towards achievement of goals. Leadership is increasingly advocated as a skillset that should not be limited to senior managers in formal roles. Several theoretical perspectives have been proposed to conceptualise leadership as a team property as an alternative to the person-centred trait and behavioural approach (Friedrich et al., 2014; Yammarino et al., 2012). Accumulating evidence from systematic reviews and meta-analyses indicates that collective and shared approaches to leadership in many settings can operate as a driver of team effectiveness and performance and create a more positive working environment for staff (Beirne, 2017; De Brún, O'Donovan, et al., 2019; Wang et al., 2014; West et al., 2014; Wu et al., 2020). Such approaches have been advocated for organisational change and improvement (Martin et al., 2009) given that a strong hierarchical healthcare culture can inhibit safety climate and speaking up behaviours (Crowe et al., 2017; Hartmann et al., 2009).
These non-hierarchical approaches conceptualise leadership as a collectivistic phenomenon that involves multiple individuals assuming and sharing of leadership roles over time in both formal and informal relationships (Yammarino et al., 2012). The ‘umbrella’ term of collectivistic leadership incorporates various theoretical perspectives such as team, shared, collective, distributed and network leadership. These all share the fundamental underlying tenet that leadership roles and responsibilities are adopted by multiple actors in teams, depending on the task at hand (D’Innocenzo et al., 2014; Friedrich et al., 2009). The importance of a strong internal team environment to promote collective leadership has been established (Carson et al., 2007; Wu et al., 2020). This environment is characterised by a shared purpose, social support, voice and team trust (Carson et al., 2007; Wu et al., 2020). Successful collective action is driven by relationships and transpires when vision and values are aligned (Rycroft-Malone et al., 2015). Collective identity is particularly relevant to the development and enactment of collectivistic leadership (Venus et al., 2012).
When collective leadership is practiced, teams experience less conflict, with higher levels of trust and cohesion (Bergman et al., 2012). Additionally, there is an association between shared leadership styles and helping behaviours (Ziegert, 2005). Collective leadership is inclusive in nature and by inviting feedback and input from all team members, leaders can help to diminish the deeply ingrained hierarchy that exists in healthcare settings. Inequities of status within teams hinder effective communication (Edmondson, 2003) and is associated with patient safety failings (Nembhard & Edmondson, 2006).
While there is strong evidence for the positive impact of such approaches to leadership on team effectiveness and performance in many sectors and contexts (D’Innocenzo et al., 2014; Wang et al., 2014), yet there is a dearth of research conducted in healthcare settings (De Brún, O'Donovan, et al., 2019; De Brún, Rogers, et al., 2019). This is notable given the high level of task and role interdependence in healthcare, indicating a context that is particularly suited to collective leadership (Wu et al., 2020). Though evidence in health settings is limited, a recent systematic review highlighted that most interventions aimed at introducing collective approaches to leadership demonstrated success, with benefits observed in staff engagement and satisfaction, team performance and quality and safety outcomes (De Brún, O'Donovan, et al., 2019; De Brún, Rogers, et al., 2019). Researchers have asserted the necessity to widen the scope of leadership training to all professions on teams as this represents the most effective leverage to improve care quality (Lega et al., 2017).
Progress in researching collective leadership has been hampered by a lack of knowledge about how to develop leaders as part of a collective (Yammarino et al., 2012). There has been a lack of theory-informed research on how collective leadership is cultivated in teams (Pearce, 2007) and the study of its implementation and impact in heterogeneous contexts has been advocated (Pearce & Sims, 2000). Also unexplored are the generative mechanisms underpinning interventions to promote collective leadership: how and why they may be effective, and the contexts which can inhibit or promote successful implementation (Eva et al., 2019). The aim of the current study was to systematically investigate key features of contexts, mechanisms and outcomes and their interactions by testing and refining a set of explanatory theories to interrogate how and why collective leadership interventions can lead to outcomes including improved safety culture, teamworking and quality of care.
Methods
Study Context
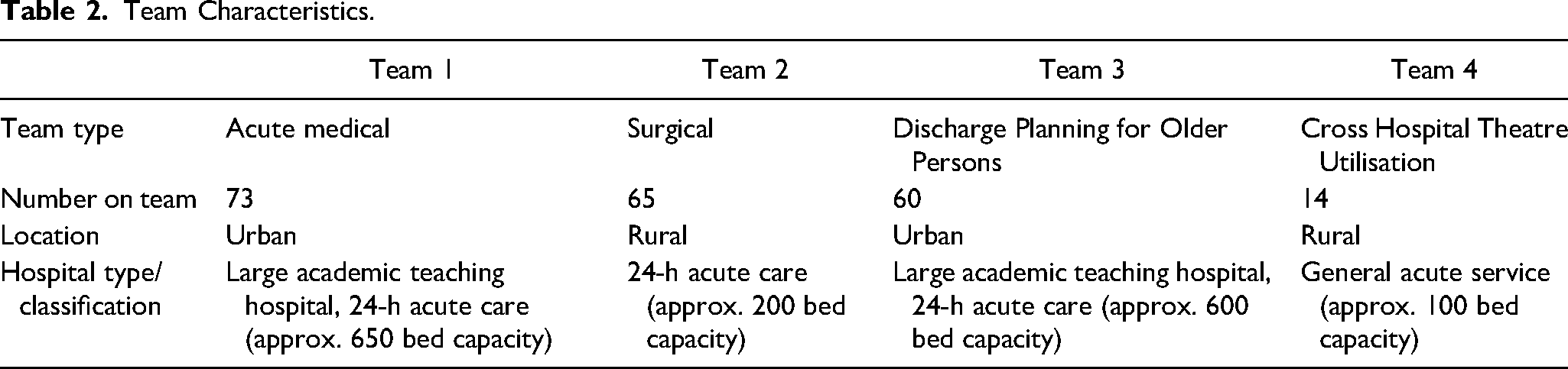
This research was conducted within one hospital group in Ireland. This group represents the largest and most complex of the groups, consisting of 11 hospitals in the hospital group, ranging from small speciality hospitals to large academic teaching hospitals. The teams that participated in this research represented four teams operating in four different hospitals within the group. The sample included a surgical team, an acute medical team, a hospital theatre utilisation team, and a discharge planning for older persons team (see Table 2 for further information on teams and context).
Study Design
A multiple case study design using realist evaluation (RE) was the approach adopted for this research. RE acknowledges the complexity of the healthcare setting and enables consideration of the significant role of context in implementation and evaluation (Braithwaite et al., 2018; Greenhalgh & Papoutsi, 2018; Pawson & Tilley, 1997). It is a theory-driven approach to evaluation grounded in scientific realism (Pawson & Tilley, 1997). It explores the inner mechanisms (M) or psychological drivers, that trigger outcomes (O) in certain contexts (C) (Dalkin et al., 2015; Pawson & Tilley, 1997). Of interest in RE are the relationships between specific contexts, mechanisms, and outcomes or ‘CMO’ configurations (i.e., C + M = O). These programme theories, or theories of change, are tested across multiple contexts (e.g., organisations, teams, etc.) to refine the programme theory in order to develop an in-depth understanding of why interventions work (or not).
For organisational research in complex adaptive systems such as healthcare, RE confers several advantages. It facilitates researchers to penetrate below the surface level inputs and outcomes and develop rich and nuanced insights into ‘what works for whom, in what context, to what extent, how and why’ (Pawson & Tilley, 1997). It enables researchers to offer practical and specific policy and practice recommendations from the findings as it seeks to maximise the external validity of case studies by looking for patterns or ‘demi-regularities’ across cases or implementation contexts. Repeated case studies across various settings allow for the critical role of context to be considered in the implementation and evaluation of healthcare interventions (Pawson & Tilley, 1997). This also enhances the transferability and generalisability of findings as well as providing insight into how programmes operate contingently within specific implementation contexts.
The programme theory tested in this study was developed through realist synthesis of the literature, qualitative interviews with key informants and expert panel discussions (De Brún & McAuliffe, 2020; De Brún, Rogers, et al., 2019). The CMOCs that constitute the initial programme theory (IPT) are detailed Appendix 1. This IPT was tested in this analysis to understand if theories were supported, could be refined, or even refuted. It also allowed for new theories to emerge. The IPT directed the data collection and analytical process adopted.
Intervention
The co-designed collective leadership intervention evaluated in this study is a complex intervention (Craig et al., 2013). The Co-Lead programme (De Brún et al., 2020) [the intervention] was co-designed by healthcare staff, patient representatives and researchers during six half-day workshops and one full-day workshop over a seven-month period (Ward et al., 2018). The co-design approach helped to ensure the intervention was grounded in the real-world needs and realities of healthcare teams and was feasible to implement given the time pressures already inherent in healthcare delivery. The exercises, activities, and inputs to the co-design process (including evidence syntheses, sharing healthcare staff experiences of leadership and teamworking and the patient perspective on teamworking and healthcare delivery) and the outputs of the process have been described in detail (De Brún et al., 2020; Ward et al., 2018). Each component has a clear and explicit focus on leading collectively and a key priority for the co-design team was to ensure intervention content selected and prioritised was consistent in aligning to the core tenets of collective leadership (Contractor et al., 2012; Friedrich et al., 2009; Mumford et al., 2012; West et al., 2014; Yammarino et al., 2012).
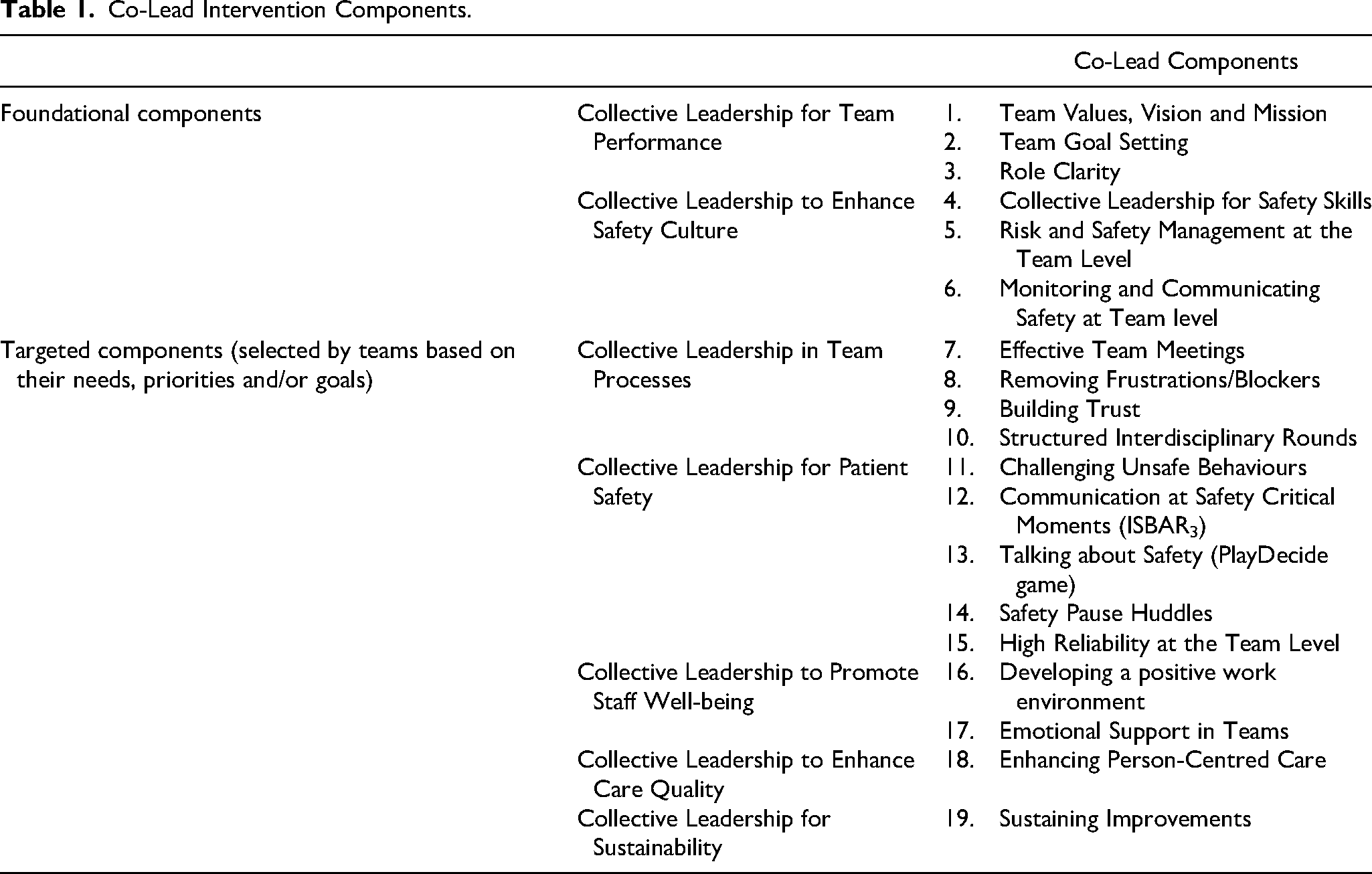
The intervention comprises a minimum of 8 components or team sessions delivered by team members to their own team: 6 one-hour ‘foundational’ components related to collective leadership for team performance and collective leadership for safety culture and at least 2 further intervention components selected (from an additional 13 components) by teams based on the team's specific needs, priorities and/or goals. From the total of 19 targeted interventions, the 6 foundational components are compulsory and a core first phase for all teams. Table 1 provides an overview of the intervention components. The materials are available open source at the project website [www.ucd.ie/collectiveleadership]. Each component of the self-development intervention takes an hour to complete, and the components are co-led on a rotating basis by two members team of the healthcare team, with the team meeting in their regular work environment. The components were designed so that minimal advance preparation is required of those co-facilitating the team sessions.
Co-Lead Intervention Components.
Data Collection
A mixed methods approach to evaluation was adopted and data collection began prior to implementation. Qualitative data was gathered initially with team members to gain insight into their teamworking and processes and for the purposes of feeding this information back to teams to assist them in selecting the optional interventions for their team. Field notes were taken during non-participant observation of the teams’ intervention sessions. Once each team had completed 8 intervention sessions, post-intervention evaluation began. The research team booked a room at each site for the purpose of conducting one-on-one interviews, guided by Manzano's theory-based approach to conducting realist interviews (Manzano, 2016). To ensure a wide range of perspectives, we interviewed staff of various disciplines and levels of experience within teams. A team of four qualitative researchers conducted data collection and met frequently in the initial stages to iteratively refine the interview guide and discuss findings as they emerged. Each participant was interviewed once and consistent with the theory-based realist interview approach, the IPT previously developed informed the interview guide (see Appendix 1). Ethical approval for this research was obtained from University College Dublin Ethics Committee (LS-16-20).
Data Analysis
Consistent with the realist approach, a retroductive approach to data analysis was adopted (RAMESES II, 2018). Retroduction moves back and forth between inductive and deductive logic to interrogate both cases that are consistent and inconsistent with the IPT (presented in Appendix 1) to enable confirmation and/or refinement as analysis progresses (RAMESES II, 2018). Initially, notes were kept on potential contexts, mechanisms, and outcomes during the familiarisation stage of analysis. For the purposes of protecting the confidentiality and anonymity of participants and participant organisations, we have referenced each team as a numbered case study (Team 1–4; see Table 2). Consistent with case study methods and previous RE research (Rycroft-Malone et al., 2015; Yin, 2013), each case was analysed at the individual case-level and cross-case comparisons were then conducted to explore commonalities (i.e., demi-regularities) and differences between sites. The analysis process was managed by the primary researcher and with regular discussion with members of the wider team as analysis progressed.
Team Characteristics.
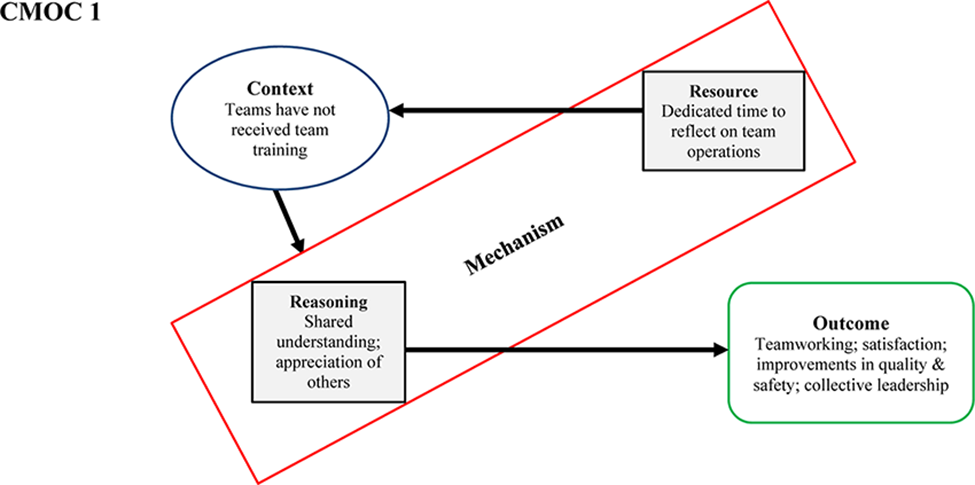
Supported by NVivo12 (QSR International Pty. Ltd., 2012), the coding process involved applying a deductive lens to code relevant information to existing CMOCs (Appendix 1) to help confirm, refine or refute existing hypotheses and applying an inductive lens to also enable new CMOCs to emerge within each implementation site. Memos were used to make sense of the data, document ideas and inferences and record the decision-making process where CMOCs were refined, amended or developed. Consistent with the theory-based interviewing approach adopted, the analysis began by interrogating the outcomes reported by interviewees, and then sought to understand the resources and mechanisms triggered (or not) in these contextual conditions that led to the stated outcomes. In line with Pawson's strategies in applying a realist lens (Pawson, 2006), juxtaposition (comparing and contrasting CMOCs across cases), reconciliation (exploring reasons for differing mechanism and outcomes) and consolidation strategies to identify patterns in the data were employed. A subset of data (approx. 20%) was independently coded using this approach. The findings were highly similar when patterns and conclusions were compared, conferring confidence and trustworthiness in the findings. CMO configurations are illustrated using the approach outlined by Dalkin et al. (2015) to promote operational and conceptual clarity. In this conceptualisation, a resource mechanism refers to the component of the intervention introduced into the context and the reasoning mechanisms relate to participant's implicit reactions and reasonings in response to the intervention resources in the context. RAMESES II best practice guidelines for the reporting of RE studies (Wong et al., 2016) were adhered to in reporting of results.
Results
Sample Characteristics
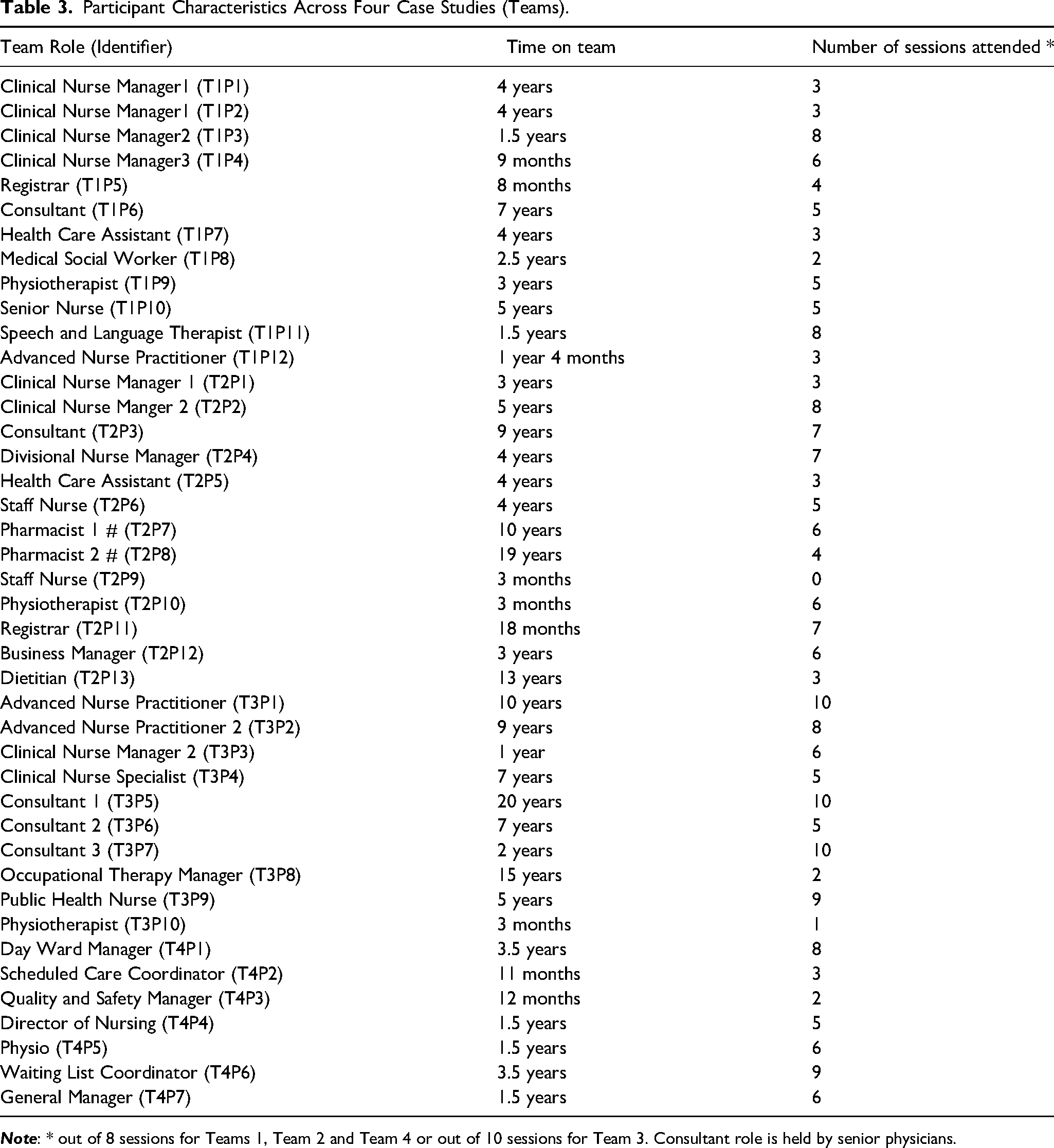
Across four cases, a total of 42 individuals took part in a realise interview to test the IPT and discuss their experience of the intervention. Sampling for interviews was broadly representative across each team, with 12 participants interviewed from Team 1, 13 from Team 2, 10 from Team 3 and 7 from Team 4. Further details about participants’ role on the team and the duration of team tenure are available in Table 3.
Participant Characteristics Across Four Case Studies (Teams).
The following sections report the results of testing an IPT that was developed to inform this research (De Brún & McAuliffe, 2020). This IPT (see Appendix 1) formed the basis for the RE and as such, guided the analysis.
Almost all respondents reflected that their participation in Co-Lead was their first experience of any kind of team training. While some teams held regular meetings, these were typically patient-focused and only attended by a subset of team members and none had the opportunity to train together in their current team. “Just sitting in the room with everybody and getting that opportunity to speak to each other. You just don’t, you just don’t get it.” (T1P10)
Team members appreciated dedicated time to reflect on how they work, and this operated as a resource mechanism offered by the intervention. Protected time enabled the teams to “plan and focus” (T1P2) on key priorities for improvement. Among the mechanisms activated through having this dedicated time for team reflection was a sense of shared understanding and feeling valued and listened to. Team members reported developing a shared understanding of the challenges and goals of the team and a shared understanding of each other and the various roles on the team. The formation of this shared mental model gave “everybody a sense of common purpose and common direction” (T3P5). While the experience “created an understanding of roles” (T3P2) by “giving us a voice to kind of explain what we do” (T2P10), it also served to emphasise the person in the role: “we’re not just our professional silos, that we’re people with personalities behind it all” (T1P11). “What I have a much better feel for after [the intervention] was the clarity of the crucial importance of how the team works together, and the importance of everybody's individual contribution to it. I suppose that is a collective role clarity.” (T3P5)
“I think it was that sharing of experience which doesn’t really happen outside, hasn’t really happened outside Co-Lead to my experience, in the sense that it was really a unique cross-discipline meeting point… I suppose it was a hiatus of your day where you could think about other things, and think about – you know, exactly what we’re doing as opposed to just slavishly doing it.” (T1P6)
Participants mentioned that the team training together broadened their perspective and created a deeper understanding of other professions by learning from each other's experiences. They reported “seeing your colleagues in a different light” (T3P1) and an enhanced awareness of “their pressures” (T4P2): “you can see the struggles and the faces behind the job titles” (T3P9).
Feeling valued was another psychological mechanism reported across cases. People felt acknowledged and appreciated in their roles for the unique contribution they brought to the team. Having this dedicated team time for reflection was described as developing “rapport” (T2P6) and fostering “appreciation for a person's expertise and acknowledging that” (T3P3). This resulted in improved staff satisfaction, “helped team morale” (T3P5) and created a more positive working environment. “We all have a good communication and working morale between one another. I do think that makes a huge difference in how you feel when you're coming into work.” (T2P2)
Improved relationships and familiarity among team members was linked by interviewees to improved communication, enhanced patient safety and improved efficiency in service delivery. Participants felt the silo mentality that had existed was reduced, creating psychological safety and enabling people to speak up about concerns and approach others in a more informal manner. The safe space fostered meant people felt they could voice concerns and “put our hands up if things do go wrong.” (T1P1). “Well, you can see in the ward here, even the cooperation between the team itself. Now the nurses - maybe in the past they don't ask questions. Now they are talking to us, and they are. You can feel it in the ward.” (T2P3)
“It improves your quality and safety. It builds relationships. It improves communication. It gives clarity about people's roles and responsibilities. And clarity of the process. Identifies when things don’t go right, and why they haven’t gone right.” (T4P3)
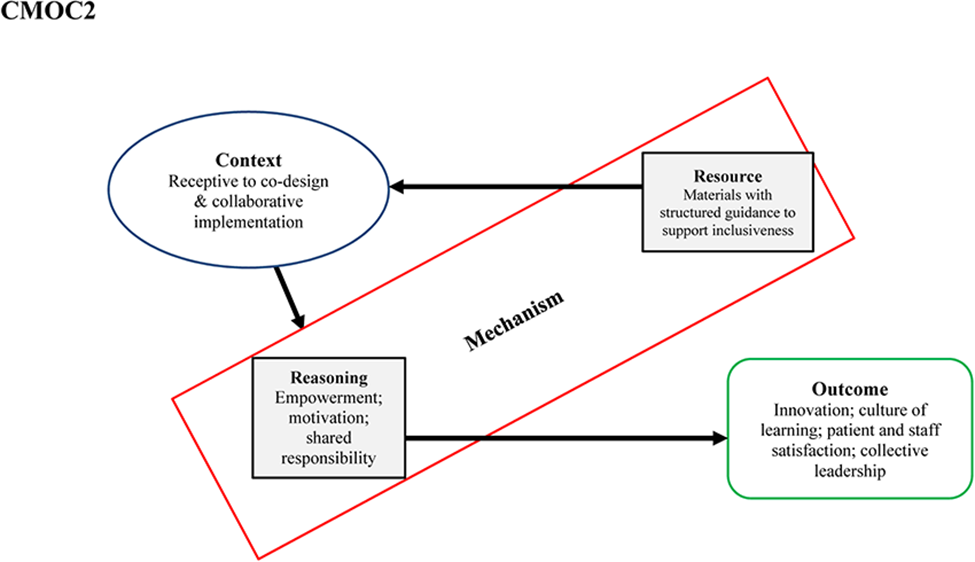
While the team training together on-site was a new experience, so too was the collaborative approach introduced by teams to improve team processes and outcomes. In contexts that were receptive and open to adopting a co-design approach, materials with guidance on how teams could promote inclusivity in co-design processes helped teams to adopt this way of working. Through this, team members felt listened to and reported that it “gave everyone a voice” (T2P10): “it's not often you get to do that kind of thing” (T2P7). Participants appreciated and enjoyed the opportunity to select what they felt was important to work towards, rather than only work towards targets and goals prescribed by the organisation. A collaborative exchange was described, where “we kind of amongst ourselves decided who would kind of look after different areas” (T1P3) and that actions taken were the result of a “shared decision” (T1P4). This served to remove “the cynicism people had about the progress of things [in the organisation]” (T3P5) as it was felt that “solutions come from the people doing the work” (T4P7). “It was more meaningful for the team that they were able to set their own goals” (T3P6)
However, in two cases, participants expressed concern that the process may not have included enough diverse perspectives and that “it would have been nice to get other perspectives like say HCAs [healthcare assistants], pantry staff, cleaners” (T1P11). Furthermore, although the decisions were shared, some reported that actions often fell to certain people on the team rather than actions being evenly shared, and this may have hampered progress.
The collective approach to improvement implemented was reported to activate mechanisms including empowerment, motivation and a sense of being valued and feeling part of the team. Team members felt “empowered by that kind of buy-in to make any procedural changes that we wanted to” (T1P6) and enjoyed the positivity of this way of working. “People really did enjoy the sessions and would come out, you know, a little bit rejuvenated and thinking “oh, there's so much we can do” and feeling very positive. I suppose that's what happens when you go in and talk positively with positive people. You come out and feel quite - sort of exercised to make things better.” (T1P6)
There was also evidence of the emergence of a shared sense of responsibility and “more ownership” (T3P7) for team operations, which in turn enhanced the sense of teamworking. It also served to provoke a more collective mindset and an awareness and appreciation of the benefits of collective leadership for enhancing patient care by putting “you out of your comfort zone and talking to people that you wouldn’t necessarily be talking to” (T3P3). “It just kind of helped to feel part of the team I think and to be driving something that wasn’t my own, it was on behalf of the team, makes you feel part of the team.” (T1P11)
“I suppose it's having that insight. Its nearly that, okay, well I know I’m not the only one that gets frustrated by this and okay, you know, what can we actually do? It's all well and good that we sit in here and moan about the cracks in the service, but actually, what can we do as a team to help with that?” (T3P1)
The senior manager on one team reported that the collaborative process enabled the creation of a “safe environment” (T4P7) to facilitate open and honest discussions in a constructive manner. This was perceived as instilling self-confidence and self-efficacy among team members who may not have had experience in offering or shaping solutions. In turn, the experience of a co-design approach was described by one senior leader as “a real emancipation” (T4P7), as he was no longer relied upon to find solutions to every challenge. “I always have anyway trusted them to come up with their own solutions, but they obviously haven’t trusted themselves or each other or probably didn’t feel that they had the authority to do it… It was a real emancipation for me to be able to listen and talk to people and ask questions. I learnt a huge amount, and without actually having to be the solution-giver.” (T4P7)
The teams achieved many tangible outcomes aligned with their self-established goals as a result. Initiatives implemented included a patient information sheet to explain the purpose and functioning of the unit to patients, a poster of staff uniforms of all professionals on the team to enhance role clarity, a communication protocol to clearly introduce staff to patients, the implementation of a multidisciplinary team huddle (a team-based intervention to promote communication across professional silos) and a structured communication tool at handover, re-design shared spaces to improve staff experience, and modification of rounding processes to improve patient flow and on-time discharges. The huddle in particular was lauded at a significant outcome of the intervention, and one which has been mostly sustained and has improved coordination and communication in two teams. “The huddles came out of it as well, that's very positive, because I do think that has improved communication for me at ward level, so there was (sic) many very positive things from it.” (T2P2)
“The visible results? Well what's tangible is, well there's one or two initiatives that have already been put in place because people appreciated that you know that there was either risk or waste, unnecessary waste in some of the processes. So, they have actually proactively changed them, so that's very reassuring to me. It shows that they’re confident to make those decisions and so I’m very pleased with that.” (T4P7)
Staff reported a more positive work environment, enhanced team morale and greater levels of satisfaction as a result of this way of working. This collective approach was considered valuable to model as it was perceived as encouraging people to suggest things in future: “because they’ve seen people working collectively towards a common goal, they’re more willing to suggest other things that might come up” (T3P5). One interviewee stated the team had “developed a ward philosophy” (T2P6) and another commented that “people go away from their day thinking, yeah we did something good, you know, rather than going home stressed” (T1P4). “If you can sit down and solve problems together, it is amazing the work you can get done. But if you don't, you keep on working frustrated, when you could be working differently.” (T2P4)
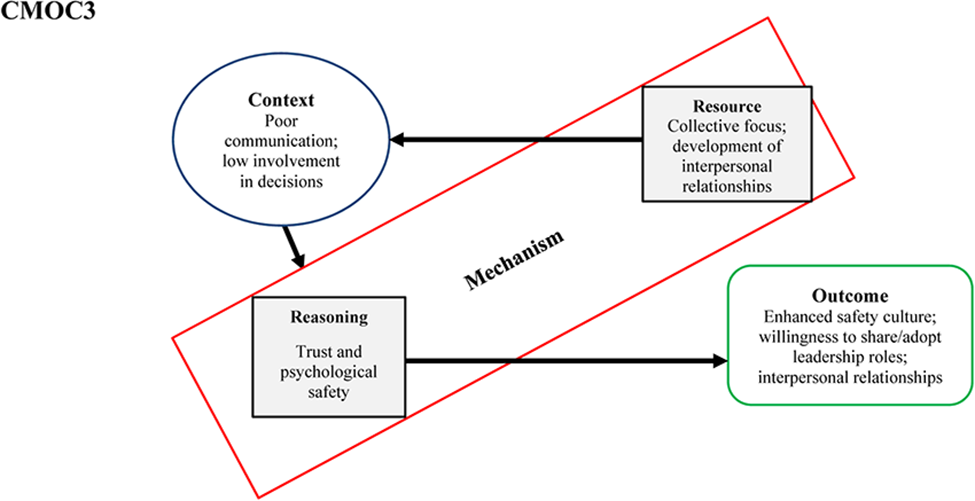
Prior to implementation of the Co-Lead intervention, poor communication and a lack of involvement in decision-making were evident in two teams (Teams 2 and 3). According to one interviewee: “it definitely needed to be highlighted, there was some communication issues” (T2P12). Another stated, “there are some communication cracks… the right information doesn’t go to the right people” (T3P1). Within one team, decision-making was described as “very top-down… driven by the surgeons” (T2P10) while on the other team, decision-making was “sometimes good when we collectively made a decision, but shockingly poor through conversations in a corridor” (T2P2) at other times. As a result of the collective focus of the intervention, there was consensus that barriers between professions on the team began to dissolve. Psychological safety was enhanced as people were more confident and “more willing to speak up” (T2P7) when they had any concerns or felt they had something to contribute to care decision-making. Additionally, team members described their senior colleagues as more open to their views. “It broke down the barrier or the wall… they are more able to voice their concerns or opinions. More confident and safer doing it.” (T2P1)
“You can, I suppose, ask them [senior colleagues] questions a little bit easier.” (T3P3)
Senior physicians also reported greater willingness to receive input and conveyed an enhanced sense of trust in colleagues. When they got to know colleagues better through the regular Co-Lead meetings, they were more confident relying on their judgement when communicating about patient care. “You're definitely listening more… The nurses are always the same. They know their patients, you know? You know how they run, you know. When you know the nurses, you know what's important and what's urgent and what's not.” (T2P11)
“[On hearing others’ voices] I think that it just increased my awareness of that and the importance and value of letting a voice be heard, and that no opinion, in the context of where we’re working, is an invalid opinion, because it's all about the patient.” (T3P5)
Among the outcomes reported were enhanced staff satisfaction, feeling valued as a member of the team, the perception of making a meaningful difference, and more inclusivity in decision-making and discussions regarding patient care. Participants described “a nicer environment to work in” (T2P1) and some felt some staff members who traditionally may not have spoken up for patients were more comfortable in doing so when necessary. “I can see it with staff nurses, I do feel they are more at ease… ultimately that's in the best interest of the patient, you know, for everyone to be able to say how they feel, or if they fear for person's safety or for a person's well-being.” (T2P2)
“If you feel you can input and influence things for the best, I think there's a huge amount of kind of satisfaction.” (T2P7)
With this more open and inclusive approach to patient care, participants felt that ultimately this had a meaningful impact on patient care and patient safety. One person commented that there was now “less likelihood of communication breakdowns” and “a more efficient service” (T2P4) as a result of the intervention, with another agreeing there was “less risk of something being missed” (T2P8). However, one cautioned that “sometimes it's still not what it should be, either” (T2P5) and there was still room for further improvement. “Definitely patient safety is a huge thing. I think we’ll flag up things quicker, we action them quicker, then obviously the patient stays safer and then hopefully discharges are better, length of stay is down.” (T2P10)
There was a strong sense that one of the four teams involved in the intervention operated in a context already characterised by open and inclusive communication and decision-making processes around patient care. In these cases, physicians were described as “open to input from others” (T1P1), in strong contrast with some previous experiences of working in healthcare teams. The same mechanisms were reportedly triggered in this context, and the main outcomes observed as a result of the intervention were increased team cohesion and improved interpersonal relationships. This enhanced familiarity meant team members were more comfortable approaching someone when they had that informal relationship to begin with. “It's very inclusive. I think probably it was to a degree before Co-Lead but I’d say you know relationships have improved with it you know even with the regular meetings. People are maybe more aware of each other, happier to talk to one another because you’ve met at sessions and you know you probably just have a better relationship, you might be more inclined to go up and talk to somebody on the ward about someone.” (T1P9)
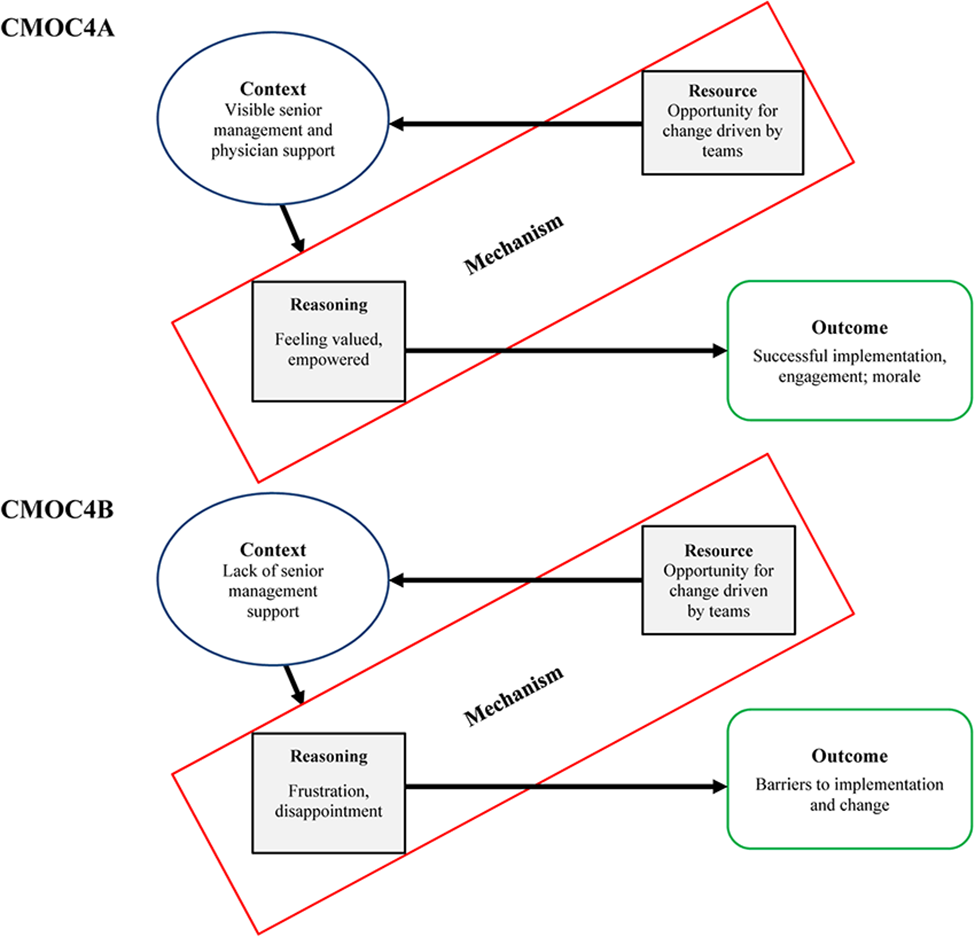
Across the four teams, there were mixed views on whether there was support for the intervention from senior management and these views often depended on the degree of involvement individuals had in supporting implementation. Those that were more involved in implementation were cognisant of management support, but this did not necessarily translate, or was not communicated to, other team members. Two teams (Teams 1 and 2) felt there was strong support and “good backing” (T1P10) for the implementation of the Co-Lead intervention from senior organisation management and from middle managers working more closely with the team. While some on these teams were not aware of any management presence or support or reported “not very much” support (T1P11), they knew that it was not being obstructed by management and felt it was not necessarily appropriate for management to be too closely involved in their team training. In one site, members of senior management did attend an initial launch session and a couple also attended one team intervention session. This was viewed positively by those who reported this visibility from management. Staff were surprised to see members of senior management attend a session, but it was perceived by senior team members as management being “involved and supportive” (T1P5). However, others felt anxious or more reticent to engage when there were members of senior management present at sessions. “[Support from management] was very good. They came to the launch, they paid for lunches for us, which is practically unheard of in the hospital these days, so I think they really did invest into it and support it.” (T1P6)
This middle management support in Team 2 was described as the key driving force for successful implementation and for promoting engagement. Middle management involvement and close existing links to the teams meant they could “pull people in and encourage people to attend” (T2P13).
In the other two teams, some staff (senior clinicians and nursing staff) within teams were not supportive of the intervention due to workload and time pressures. In one case, senior nursing staff were described as “obstructive” (T3P7) and there was “lip service” (T3P7) paid rather than actual engagement. In one team, membership included representation from people in senior management roles across two hospital sites. Initially, this was described as supportive, but over time attendance and involvement from senior management decreased noticeably, leading others to doubt the importance and relevance of the intervention. “I think it created a negative impact. People, you know, you did say ‘why are we here?’, ‘what's the purpose?’ So when you have senior management, the question is do you need senior management on a team to progress things? But in our case, I think we do, because we need the decisions being made, we need the support from management to help us move on… so the management is important in this structure” (T4P1)
Those that perceived support from management reported feeling valued as a result of having the opportunity to take part in Co-Lead. Visible support and ‘buy-in’ from middle management were cited as helping to implement the intervention. People felt management were approachable when they were on the ward and it was reported that they checked in with team members regularly to get update on how staff felt the intervention sessions were progressing. This presence was described as helpful and important to the successful implementation of the intervention. The majority viewed support from management as empowering staff to engage with the initiative and was “certainly was a positive thing for morale” (T1P6). “I think it's always a positive impact if senior management are encouraging you to go along to things. You feel more involved overall in the running of a ward… It's more empowering, I guess, to know that you’re, will be listened to, and you’re a part of something.” (T1P1)
For those teams that did not experience the same level of management support and engagement, team members felt that it was more challenging to progress their planned initiatives or make final decisions without such support. “In order to embrace the recommendations that Co-Lead has. I mean it really needs to be led from management otherwise it's very hard to stop, to start, for it to get the support in the department if you don’t have the support of management to drive the change.” (T3P6)
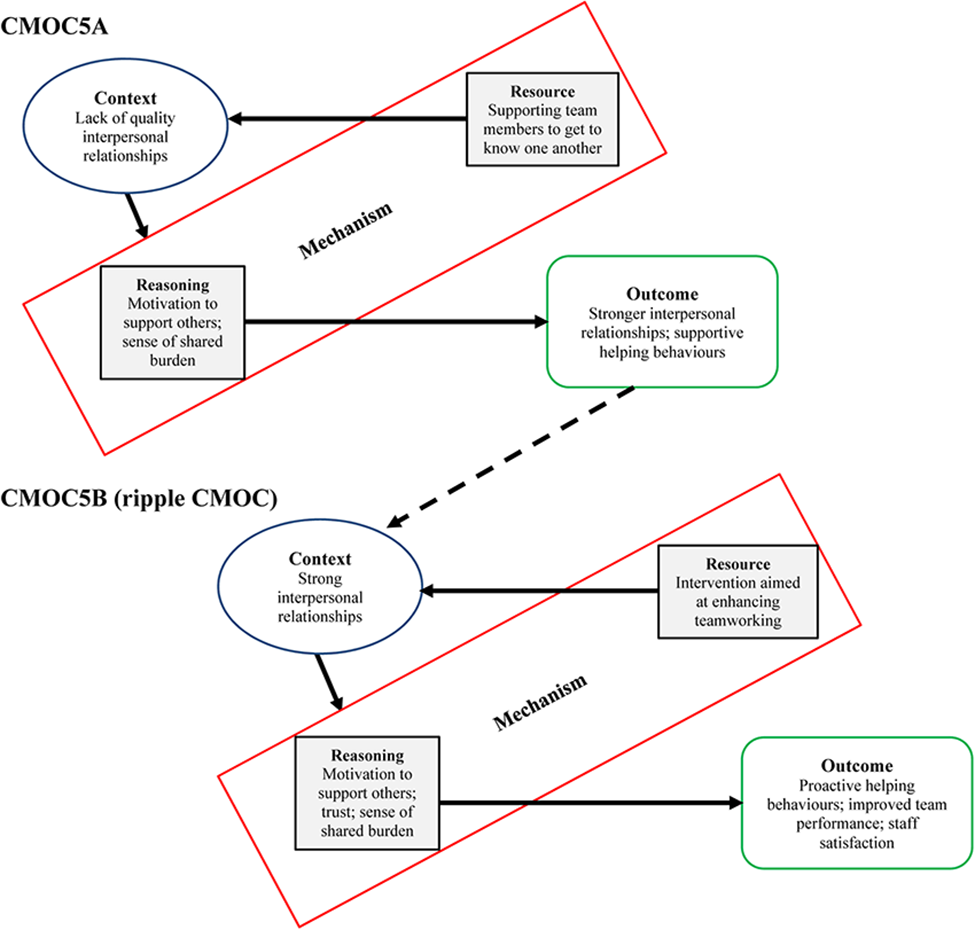
Interpersonal relationships were described as at the early stage across sites in Team 4 and as distant in Team 2. While some in Team 2 felt relationships were mostly cordial, others mentioned the frustrations with the perceived lack of respect felt when people did not try to get to know one another. “Well you saw that at one of the interventions with the, I think the one with the junior doctors attendance and that, so there's frustrations there with some relationships and that but you know it highlighted it, I suppose Co-Lead has highlighted it but you can see the gaps.” (T2P12)
The intervention provided a platform for team members to build relationships and get to know one another. Among the key mechanisms reported by interviewees was a sense of shared burden and a motivation to support and help colleagues on the team in a process of give and take: “If you have the time and spent the time, it's also that you get something back from them” (T2P11). Respondents believed the intervention improved the relationships among team members (“the Co-Lead piece definitely has strengthened those” (T4P4)). People felt that because they had fostered positive interpersonal relationships, “then you want to support them [colleagues] in what they’re doing” (T2P4). Consistent with the shift towards a more collective and team mindset, it was reported that people are more willing to go beyond their own role to “support each other and work for each other” (T3P9). This resulted in people engaging in role blurring behaviours and “helping each other out more as a group” (T2P6). As a result, “staff morale is much better, and people engage better with each other” (T2P10). “It leads to sea change. Say, with staff, and you’re really short staffed one day and you ask for help, that at least you get that help, you’re not left on your own.” (T2P9)
A ripple effect was observed in that when contexts were characterised by stronger interpersonal relationships, the effects of the intervention were strengthened. There was a majority view amongst participants that there was a positive working environment and good working relationships between team members on two teams prior to the team's participation in Co-Lead (particularly strong in Team 1 and evident in Team 3). Some felt there was “a good baseline relationship” (T1P12), team dynamics were “very positive” (T1P6) and that there was “good general collegiality” (T3P2). One person specifically cited such a context as one amenable to an intervention such as Co-Lead, as it aligns to the philosophy of how the team already operates. Another felt that the strong internal team environment made it easier to implement something like Co-Lead, as people could feel more at ease with listening, sharing their opinion and getting involved. “I think they're pretty good. Yeah. Yeah. I actually think it's a lovely area to work in, like, I've worked in other places where maybe there isn't as nice of a team atmosphere, I think here it's very open and everybody gets on quite well, and we are quite willing to ask each other for help and everything, so that's – so that's nice. And then, I don't know, I think Co-Lead probably links into all of that, in the mentality on the ward.” (T1P5)
In open and inclusive contexts, the resource mechanisms of deploying an intervention aimed at enhancing teamworking meant that team members built “familiarity, friendship” (T1P7) and people felt others were more approachable and were more comfortable approaching them for advice of help when needed. This was described by on individuals as a shift to “more of a team mentality” (T1P5) and using the expertise on the team when you knew colleagues better. “I suppose the better you know people the more you are inclined to help as well like say on the ward, if you’re very familiar with some of the nurses and you know they ask you to help with something or to, you kind of, you want to keep your relationships good with them and I suppose if you maybe don’t know people as well you might be less inclined to step outside what you’d usually do.” (T1P9)
Among the most commonly cited outcomes observed as a result of this motivation to support others was improved patient care and patient experience, a more efficient service, reduced staff stress due to a more positive working environment, improved morale and camaraderie. “It makes the patient care more seamless and more co-ordinated and then with that then we’d probably drive, increase, the patient care is better quality and possibly safer then because everyone knows what everyone is doing so it's more co-ordinated plan.” (T3P6)
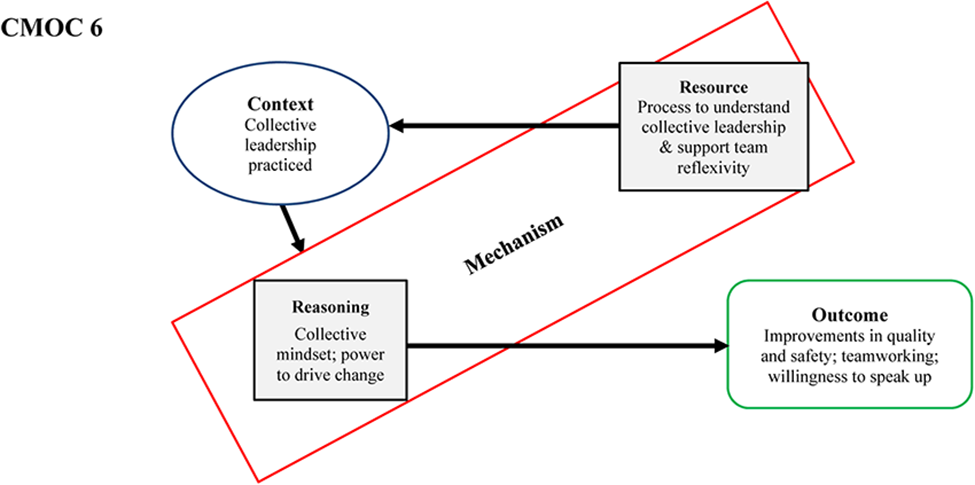
Most respondents in two teams (Teams 1 and 2) stated they believed collective leadership, characterised by “shared responsibility and accountability” (T1P10), was being practiced within the team. As described by one interviewee, “there's no kind of hierarchy or anything like that” (T1P3) and there is “collective leadership, and collective management as well, as in that everyone is involved, it's not just a consultant making the decision” (T2P2). Some felt that aspects of collective leadership were already in place in Team 1 prior to the intervention, and the intervention served to bolster and make this explicit. Only a minority were uncertain about whether the team were practising collective leadership or not. There were mixed views in Team 3 and Team 4, with some recognising that the intervention had “changed the dynamic” (T3P7) and there is “collective leadership in the management of the patient” (T3P6), yet the practice “fluctuates” (T3P2) was “still disjointed” (T4P1), and while some were practising it “in their own way” (T4P1), there was a sense that the teams “could probably do better” (T3P7). Some felt however, that in order for collective leadership to be implemented, “a person to drive it” (T4P4) was still needed to ensure team members come together and monitor progress and performance. The challenge of culture change was acknowledged across cases. “It's really hard to change culture in something that's been embedded in people for so long” (T3P10).
Those that perceived collective leadership in practice described a more team-based approach to care, fostered through enhanced interpersonal relationships, and typified by regular communication and consultation between team members. There was evidence of a shift to a more collective mindset with the recognition that “it has to be a team effort” (T2P4) and “it's not a them and us” (T3P7). “Realising you know we’re not just you know us and them, you know it's this silo working, we need to work together to and you know we can work together you know, we can all you know, nobody has to be the boss. You know we can all work together, we can all make decisions together, we can all help the patient you know, [have a] better journey by working together.” (T1P4)
“I think Co-Lead is very positive and I think it's very progressive from a leadership perspective and I think the hierarchical days aren’t going to work any longer and from a patient safety and quality of care, I think all systems really will have to be ran on that collective, flat kind of structure.” (T4P5)
Staff reported feeling more “respected” and “valuable” (T1P7) through leading collectively. Asked how it feels to work collectively, one individual responded, “you never feel like you’re working on your own at any stage. It's positive for the patients, positive for the staff” (T1P2). This team-based approach to was described as “easier on everyone” (T2P5) when the team was working as a team rather than as a collection of individuals. This fostered an “improved working environment. Improved atmosphere” (T2P6). “People feel better because it's a win. It's a win, they feel more satisfied, they feel like they’re doing something as opposed to conveyer belt care”. (T3P2)
Among the key outcomes observed from the practice of collective leadership included a “more holistic approach to patient care” (T2P6) which resulted in safer and “more streamlined and more co-ordinated care” (T3P6), and improved patient flow. Respondents strongly believed that working as a team using the principals of collective leadership benefited the patient and their safety due to the inclusive nature of care and decision-making, but also the environment of psychological safety that it promotes. “Patient discharges, patient safety is huge. I suppose just knowing that you can approach like the CNM or the business manager or directorate nurse manager or whoever. Knowing that you can approach the surgeons if you need to or their teams. I suppose not having that kind of fear of approaching them and I suppose feeling a bit more confident that our professional opinion is taken on board. I think that's it.” (T2P10)
“We have a lot of junior staff now on the ward, so they’ve even kind of said that compared to some other places they have worked, they can see, like, we’re all kind of on the same level, like, and they’re not afraid to come to you with anything, where sometimes you would have found people would have been afraid to kind of speak up.” (T1P3)
Collective leadership was also perceived as enabling meaningful collective impact and change and giving people the sense of power to drive positive change. “When there's collective leadership, there's the power to make changes. There's less resistance. There's more, kind of atmosphere for change, kind of. And that people from – whether they’re – no matter what kind of role they’re in or where they’re placed on their team, that their opinions are listened to and that they feel that there's the power to change things.” (T3P9)
“You know, striving to sort out any issues or problems collectively that we – we work together, you know, that it's not just the management's problem, it's everybody's problem in the team. And get the solutions among – within ourselves. And I think that's the way it works really well.” (T4P1)
While some individuals believed there was “still quite a bit of cynicism about something like collective leadership”, there was a sense among others that outcomes observed may have been a mix between this and other initiatives in the system working synergistically. “I think it's a mix. I don’t know if it is directly Co-Lead… I wouldn’t say that it's one or the other, I think it's a combination” (T1P11)
Discussion
This study tested and refined an IPT to explore the context-mechanism-outcome configurations to evaluate the impact of a collective leadership team training intervention. Specifically, this paper outlines a series of patterns observed across implementation contexts to elucidate what works for whom, in what context, how and why to understand how the intervention operated to produce patient, staff and organisation level outcomes.
For most participants, this intervention was the first experience of any kind of team training. Participation in team sessions fostered a shared mental model of the team, its goals, and challenges, and created a shared understanding among team members related to personalities and roles. Shared mental models enable teams to form accurate explanations and expectations to effectively coordinate and adapt their behaviours to the task at hand (Cannon–Bowers & Salas, 2001). This was developed through the resource mechanisms of introducing a process to support team reflexivity. Reflective practice has been described as a mechanism to promote collective competence (Schön, 2017) yet, most focus tends to be on individual reflection rather than team-level reflection (Schmutz & Eppich, 2017). Protected time to reflect, agree priorities and plan is crucial for promoting multidisciplinary team working (Miller et al., 2007) and collective leadership (Mumford et al., 2012). Overwhelmingly participants reported this helped to enable a shared mental model about the team's purpose, role and the roles of those on the team, which promoted role clarity. When there is role clarity in teams, team members can develop transactive memory systems, that is, a means through which members collectively encode, store and retrieve information and expertise (Wegner, 1987). This was perceived as leading to enhanced teamworking, job satisfaction, improved communication, and coordination, which was associated with improvements in quality and safety of care. Taken together, the findings make a powerful argument for the importance of team reflection and collective reflexivity to support the practice of collective leadership.
In contexts receptive to collaborative and co-design approaches to improvement, teams’ self-delivery of structured materials to foster collective leadership behaviours was strongly linked to enhanced empowerment, motivation due to a shared responsibility for team performance. Empowerment can be an effective mechanism for sharing leadership roles (Mathieu et al., 2006). Team empowerment is the collective experience of increased levels of task motivation as a result of members’ assessment of their team's tasks as providing them with high levels of meaningfulness, autonomy and impact (Kirkman & Rosen, 1999). More empowered teams tend to be more proactive (Erkutlu, 2012) and demonstrate higher levels of job satisfaction and team and organisational commitment (Kirkman & Rosen, 1999). In this study, the increased sense of ownership for team operations led to adoption of a collective leadership approach towards improvement. This was described as an ‘emancipation’ by appointed leaders, demonstrating that team members were more willing to offer solutions and adopt leadership roles and responsibilities. Consequently, teams collaboratively and successfully implemented quality and safety initiatives (e.g., safety huddles).
However, the current findings uncovered differential levels of senior managerial support on outcomes: one context characterised by strong management support for the intervention and the other which reported an absence of management support when needed to promote implementation. In the latter situation, participants reported feeling disheartened and frustrated by a lack of support. This had implications for the team's ability to drive change and negatively impacted team morale. Conversely, in contexts with visible management and senior physician support for implementation, participants felt empowered and valued, in turn promoting engagement with the intervention, conferring credibility and a sense of importance to the initiative. Previous work on factors influencing team intervention effectiveness in healthcare found that leadership support and physician engagement were crucial enabling conditions for success (Cunningham et al., 2018). This, again, likely speaks to the deeply ingrained hierarchy in healthcare and the need for leaders to explicitly give teams autonomy to collectively shape solutions. Friedrich et al.'s (2009) integrative collective leadership theory maintains the importance of the focal leader in sharing leadership with others and in creating the conditions in which individuals can emerge as informal leaders. Inclusive behaviours enacted by formal leaders are crucial to support and encourage the adoption of collective leadership. This includes leaders engaging in give and take, actively listening, allowing others to develop solutions and explicitly recognising expertise and acknowledging expertise of others. Coordinated efforts between the formal and emergent leaders produce the best team performance outcomes (Mehra et al., 2006), underlining the importance of appointed leaders in establishing collaboration norms (Kramer & Crespy, 2011). To promote successful implementation and sustainability, collective leadership requires ongoing, open exchange among and between formal leaders and team members (Mumford et al., 2012). Thus, the power dynamics typical in such contexts require working around and within the existing hierarchies to help to diminish their potency and to promote collective leadership.
The contexts studied varied in terms of their levels of inclusiveness and openness in decision-making prior to the intervention. For two teams, it was apparent there were poor communication practices and a lack of multidisciplinary involvement in decision-making. Research suggests this context may be more common in healthcare settings, as healthcare organisations tend to be deeply hierarchical in nature. A top-down culture of medicine, characterised by intimidation and humiliation as akin to rites of passage, and where junior staff are expected not to question senior staff has been documented in the national context of this research (Crowe et al., 2017). This lack of psychological safety has significant implications for patient care, as communication gaps and lack of coordination are common barriers to effective teamwork (Nawaz et al., 2014). The intervention's collective leadership focus supported the teams to identify expertise and skill sets available within the team. In turn, this shared understanding and acknowledgement of the role of fellow team members helped to dissolve the silos between professions and created an environment more conducive to team members feeling psychologically safe. This fostered interpersonal trust, team members felt better equipped to share leadership roles, felt more at ease in contributing their views, and senior leaders were described as more inclusive and receptive.
Whilst previous research has found only moderate correlation between shared leadership and helping behaviours (Ziegert, 2005), the current study revealed a strong link between the development of interpersonal relationships, collective leadership and engagement in proactive helping behaviours. . A ripple CMOC was evident in that when contexts become characterised by stronger interpersonal relationships, this also results in enhanced levels of trust, a greater willingness to speak up and a willingness to ask for help when needed. Improved team cohesion and interpersonal relationships were also reported. It is notable that broadly similar impacts of the intervention were observed in two very different contexts. Dalkin et al. (2015) contend that the activation of relevant mechanisms operate on a continuum, where “intensity varies in line with an ever evolving context”. This may suggest that the difference was more marked in the context without those strong relationships in place but on that continuum, improvements were also still noted in those with stronger relationships among team members.
The final CMOC related to contexts where collective leadership is practiced and is inextricably linked to all other CMOCs identified. It is most appropriate to be considered a ripple CMOC generated through the action and interaction of others. The intervention served to foster a more positive work environment for teams and through this, team members developed a collective-focused mindset, recognising the need for, and value of, other disciplines to provide optimal care and to improve team performance and enhance safety and care quality. This resonates with previous research identifying the importance of a positive internal team environment (Wu et al., 2020) and work on outcomes of shared and collective leadership in teams (De Brún, O'Donovan, et al., 2019; Wu et al., 2020).
To our knowledge, this is the first study to apply a realist lens to understand the impact of collective leadership and explore how and why it operates to drive outcomes. We have tested and refine the IPT (Appendix 1) and amended existing theories through an in-depth analysis of four case studies. In RE, theory building is on-going process, with new evidence enabling the continual refinement of understanding what works for whom, how, why and in what circumstances. However, it is important to acknowledge some limitations of the research. Firstly, not all team members were involved as participants in training sessions. There were a number of reasons for this. First, it is logistically impossible for an entire team to remove themselves from patient care, as care delivery cannot be paused. Some felt the sessions were not relevant to their roles while others may not have been invited or aware sessions were taking place. Those typically considered as support staff (e.g., healthcare assistant, admin, ward clerks) were underrepresented during team training sessions. Healthcare assistants on two teams did not perceive the collective leadership intervention as relevant to them. This may reflect their relative position in the traditional team hierarchy or lack of historical engagement in informing team processes.
An unavoidable challenge to research of this nature and a threat to sustainability of collective leadership in teams is the transient nature of many of the team members, given the rotation of junior doctors and trainees through the health system. Edmondson and colleagues have noted the critical importance of team member selection in supporting implementation in healthcare contexts (Edmondson et al., 2001; Nawaz et al., 2014). Collective leadership may be more likely to develop in teams or organisations characterised by high levels of team stability (Pearce & Sims, 2000) and this reality may be a threat to the sustainability of the practice of collective leadership. Future research should follow teams over a longer period to explore the impact of turnover and instability in team membership.
Given these issues, researchers have advocated the study of shared leadership in heterogenous situational contexts (Pearce & Sims, 2000). Hawe et al. argue that one of the most important dimensions of complexity is the context into which an intervention is introduced (Hawe et al., 2009). The RE approach adopted is therefore highly appropriate in opening the ‘black box’ between intervention inputs and outputs, to explore the how and why an intervention may be successful or not. A review of the evidence on leadership research in healthcare concluded that contextual, organisational and team-based elements have a meaningful impact on leadership in practice (Lega et al., 2017). Previous leadership research has similarly concluded that a lack of consideration of context can minimise intervention effectiveness (Kwamie et al., 2014). Context and leadership are necessarily intertwined and mutually influential. As highlighted previously (De Brún & McAuliffe, 2020), while the description of CMO configurations is simplified for the purposes of pattern identification, the reality is far more complex, with CMOCs mutually influential and interdependent within implementation contexts.
Collective leadership is more important for work that is highly interdependent in nature (Wu et al., 2020). Furthermore, as task complexity increases, the opportunities for shared leadership are also likely to increase (Pearce & Sims, 2000). Given the necessity of interdisciplinary collaboration in healthcare settings to deliver high quality, safe care, we contend that healthcare is a prime setting for further exploration and testing of collective leadership, given the accumulating evidence for its positive impact on patients, staff members, teams and organisational outcomes, evidenced both in this study and in a previous systematic review of the healthcare literature (De Brún, O'Donovan, et al., 2019). However, the shift to collective leadership is challenging and it may not necessarily be possible or appropriate to implement in certain situations or contexts (Mumford et al., 2012). Research on shared leadership in healthcare teams found that participating teams still believed that every team needs a leader (Miller et al., 2007). While it is unlikely that collective leadership will completely replace the need for vertical leadership (Pearce & Sims, 2000), organisations can work to foster the conditions to enable collective leadership and enable designated leaders to practice a more collective style of leadership. This study contributes to the growing evidence base for collective leadership in healthcare by illuminating the contextual conditions which are amenable to the emergence of collective leadership and documenting the mechanisms that generate observed outcome.
Footnotes
Acknowledgements
The authors would like to thank Ms Lisa Rogers for feedback on an earlier draft of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work is funded by the Health Research Board, Health Service Executive, (grant number RL-2015-1588).
Author Biographies
Professor