
Abstract
Background
The congruence or discordance between actual and perceived balance ability has been proposed to be linked to functional outcomes such as falls. However, gaps remain in our ability to quantify discordance, and its relationship to relevant outcomes.
Objective
To investigate a novel quantification of concordance/discordance between balance performance and perception and determine the relationship to falls among people with Parkinson’s disease (PwPD).
Methods
Data from 244 PwPD were aggregated from 5 previously conducted studies. Variables extracted included age, sex, Activities-Specific Balance Confidence scale (ABC; perceived balance), Timed Up and Go (TUG; balance performance), Movement Disorder Society Unified Parkinson Disease Rating Scale (MDS-UPDRS) part III scores, and retrospective falls (6- or 12-month). Data validation between studies was established. Discordance was quantified as the difference between an individual’s predicted ABC, based upon their TUG score, to their reported ABC.
Results
Two methods for calculating discordance were tested: simple linear regression and segmented regression. As there were no differences between the bootstrap distributions of both approaches (P = .520), simple linear regression was utilized for the subsequent logistic regression model. Discordance was the only statistically significant predictor of fall status (OR = 0.98, P = .003), after controlling for age, MDS-UPDRS part III, sex, and TUG. The inclusion of discordance in the logistic regression model boosted the predictive accuracy by 58%.
Conclusions
Discordance between actual and perceived balance was uniquely related to retrospective fall history among PwPD. Clinicians and researchers should consider discordance between actual and perceived balance as a potentially modifiable target to minimize falls.
Introduction
Actual and perceived balance may interact to facilitate one’s movement, activities, and participation.1 -4 Recent work suggests that the nature of this relationship may inform how people choose to engage with the tasks and environments they encounter.1 -3,5 -10 Theoretically, concordance of balance performance and perceived balance or confidence may facilitate an optimal trade-off between safety and engagement in physical activity and community participation.1,2,11 -13 This could be observed as a continuum where relatively high physical abilities corresponds to high levels of perceived balance or movement confidence, continuing to low physical ability and low perceived balance or movement confidence.2,13 While concordance is thought to be related to optimal outcomes at the level of the individual, discordance between actual and perceived balance may result in negative outcomes including activity limitation, participation restriction, and falls.2,3,5,12,14 -16 This discordance can be observed in at least 2 circumstances (1) having a high balance confidence with poor actual balance ability (“overconfident condition”), and (2) having low balance confidence despite good actual balance ability (“underconfident condition”). The manifestation of concordance or discordance is likely driven by meta-cognitive processes that occur as individuals weigh the perceived demands of the task relative to their perceptions of their own capability.
Previous work has identified these potential conditions of balance discordance, and proposed that they may be predictive of or relevant to functional outcomes such as falls.2,13 This may manifest as an underconfident pattern in which individuals modify their balance behaviors due to excessive anxiety, fear of falling, or perceived limitations of their balance. Conversely, individuals may demonstrate limited insight into their balance limitations and present with an overconfident pattern in which they fail to appropriately limit their balance behaviors. Both of these manifestations of discordance hold the potential to increase falls.2,13 However, previously proposed quantification techniques rely on categorization of individuals into bins (over, under, or appropriately confident).2,13 In reality, the degree of discordance is continuous, and quantifying this outcome as such improves the measurement precision of the construct and, subsequently, our ability to understand and evaluate its relevance and treatment approaches to address it. Further, whether discordance between actual and perceived balance is relevant for functional outcomes, such as falls is poorly understood.9,10,17 -24
Parkinson’s disease (PD) is a neurodegenerative disorder that results in balance impairments and reduced perceived balance confidence.9,10,17,25,26 Falls are a hallmark of PD and are accompanied by progressive reduction in physical activity and community participation as the disease advances.23,27,28 Due to these factors, PD is an optimal population in which to further investigate the concept of discordance. While current models provide information on the likelihood of a future falls among individuals with PD (eg, age and fall history),9,10,17 -24 there is less information regarding potentially modifiable physical, psychological, and cognitive characteristics (such as discordance) that relate to falls.27,29 Identifying modifiable characteristics related to falls and quality of life would provide a deeper understanding of possible contributing factors for falls and could inform treatment strategies targeting fall prevention in these groups.27,30
In sum, although the concept of discordance between actual and perceived balance has been described previously, gaps remain in (1) our ability to quantify discordance, and (2) its relationship to relevant outcomes such as falls. 2 Therefore, the purpose of this study was to propose a novel and continuous quantification of concordance and discordance between balance performance and perceived balance, and use this metric to characterize discordance in people with PD. Additionally, this study aimed to determine the relationship between discordance and falls in a fall-prone neurological population (PD). It was anticipated that degree of discordance would be related to a history of falls in individuals with PD.
Methods
Design
This study employed a coordinated analysis, which is a method of harmonizing raw data from individual studies into a single parent data which is then used to perform an integrative analysis to test a specific hypothesis.31,32 This is a semi-standardized approach, developed to facilitate efficient analysis across multiple data sets. The current study utilized data from 5 previously conducted studies across 4 institutions: Arizona State University (ASU) which conducted 2 of the included studies (ASU1 and ASU2), Saint Louis University (SLU), Oregon Health & Science University (OHSU), and The University of Nevada, Las Vegas (UNLV).33 -38 Among the 5 studies, data of 244 persons with PD were extracted and compiled to be used as the analytic sample in this secondary analysis. Inclusion criteria for this study were: (1) diagnosis of idiopathic PD and (2) having data for measures included in the primary analyses (Activities-Specific Balance Confidence scale [ABC], Timed Up and Go [TUG], age, sex, and Movement Disorder Society revised Unified Parkinson Disease Rating Scale [MDS-UPDRS] part III scores). Exclusion criteria were: (1) presence of other neurologic disease or injury (ie, cerebrovascular accident, multiple sclerosis, and Alzheimer’s disease), (2) recent (within the prior 6 months) major orthopedic injury or surgery (ie, total joint replacement), and (3) orthopedic conditions that affect the participants walking or balance.
Measures
Data extracted included information regarding demographic characteristics (age, sex), PD severity (MDS-UPDRS part III, Hoehn and Yahr), falls experienced in the prior 6 months or year, physical function ability (TUG), and perceived physical function (ABC).
PD Severity
The MDS-UPDRS part III, Hoehn and Yahr, were used to characterized PD severity. The MDS-UPDRS part III is a motor examination that consists of 18 items with higher scores indicating more severe PD-related motor impairment. 39 The test-retest reliability of the MDS-UPDRS part III is high with an intra-class correlation coefficient (ICC) of .89. 40
Falls
Data on falls was obtained by asking participants to recall the number of falls they had experienced in the previous 6 months (OHSU and both ASU data sets) or year (UNLV and SLU data sets; see Supplemental Material 1). Falls were defined as any unintentional lowering to the ground. From the falls data a fall status variable was created with zero falls indicative of non-faller status and 1 or more falls indicative of faller status.
Balance Performance
The TUG is a test of balance and functional mobility and was used to quantify balance performance during the performance of basic physical functions. Individuals were asked to stand, walk, turn around and return to the chair where they began the test, with shorter times indicating better balance and functional mobility. The TUG is a commonly used clinical measure and has excellent reliability among individuals with PD (ICC = .85). 40 Among the 5 studies, this test was performed with some variability, notably 2 studies (SLU and UNLV) instructed participants to walk quickly where the other 3 studies (ASU1, ASU2, and OHSU) instructed participants to walk at a comfortable pace. Additionally, while 4 studies (ASU1, ASU2, SLU, and UNLV) utilized the standard walking distance of 3 m, 1 study (OHSU) utilized an extended distance of 7 m. To address these inconsistencies in administration of the TUG, data from each study were normalized to each sample’s relative mean and standard deviation prior, that is, each sample’s TUG were centered to their mean and divided by their standard deviation prior to being integrated with the data from the other studies. Additionally, given the variability in TUG procedures the data were reviewed to determine variations in the relationship between TUG and ABC, and ensure the data were consistent among each study for use in the coordinated analysis (see 2.3.1 and 3.2). Of note, the TUG was completed with participants ON PD medications in 4 studies, however, in 1 study (OHSU) participants completed the TUG in the OFF PD medication state, following a 12 hour or withdrawal of their PD medications.
Perceived Balance
The ABC is a 16-item self-report measure of confidence with balance and mobility and was used to describe individuals’ perceptions of their balance. Individuals are asked to rate each item from 0 (no confidence) to 100 (complete confidence). The ABC is commonly used clinically and it has excellent reliability among individuals with PD (ICC = .96). 41
Statistical Analysis
The 2 primary goals of this study were to (1) propose a novel and continuous quantification of actual and perceived balance discordance, and (2) determine whether discordance was related to falls. A 3-phase statistical approach was taken to achieve these aims, including (1) validating the use of data across studies, (2) estimating TUG discordance with linear and non-linear formulations, and (3) relating discordance to falls. A vignette including all the code that generated the results and visualizations presented in this paper is included in Supplemental Material 2.
Validation of Between Site TUG to ABC Relationship
The first step in this coordinated analysis, given that the TUG was administered in a variety of ways across sites (see Balance Performance Section for details), was to establish that the relationship between TUG and ABC between studies was consistent. To validly combine data across sites we must ensure that variation in TUG administration does not lead to variation in the general TUG to ABC relationship, that is, presence of a TUG administration to ABC interaction whereby the estimated slope between TUG and ABC changes as a function of the type of TUG administered. To establish that the TUG to ABC relationship was consistent between studies, multivariable linear regression was performed with raw ABC as the dependent variable, normalized TUG by Group interaction as the primary independent variable, and control variables of age, sex (male/female), and MDS-UPDRS part III score. To establish that there was no significant difference of the TUG to ABC relationship across studies, a pairwise comparison of the linear trends was performed using a Tukey method of P-value adjustment for multiple comparisons. If no statistically significant differences between the TUG to ABC relationship between any sites was observed, combination of normalized TUG across sites was unlikely to impact interpretability of results when combining TUG scores.
Coordinated Analysis to Estimate ABC to TUG Discordance with Linear and Non-Linear Formulations
Within this coordinated analysis, our estimation of individual discordance was quantified as the difference between an individual’s TUG-predicted ABC (ie, the ABC value predicted by the fitted TUG coefficient while controlling for age, sex, and MDS-UPDRS part III scores) to their actual ABC. For this measure of discordance, a positive value would suggest perceived confidence is greater than predicted confidence, based on TUG, (“over-confident”), and a negative value would suggest lower than predicted confidence (“under-confident”, see Figure 1 for a conceptual plot of the measure). However, it is unclear if the relationship between TUG and ABC is linear or non-linear (ie, if a constant change in TUG leads to a constant change in ABC). Understanding the linearity of this relationship would inform which type of model to calculate discordance would best relate to individual falls. Therefore, we chose a segmented regression model with optimal knot placement (ie, where the change in regression slope will occur dependent on the value of the primary independent variable (TUG), must first be determined). To determine optimal knot placement, we iteratively fit segmented regression models with incrementally different knot values across the total TUG range and recorded their AIC value to determine the knot of best fit. The identified optimal knot would then be carried forward to the model comparison stage.
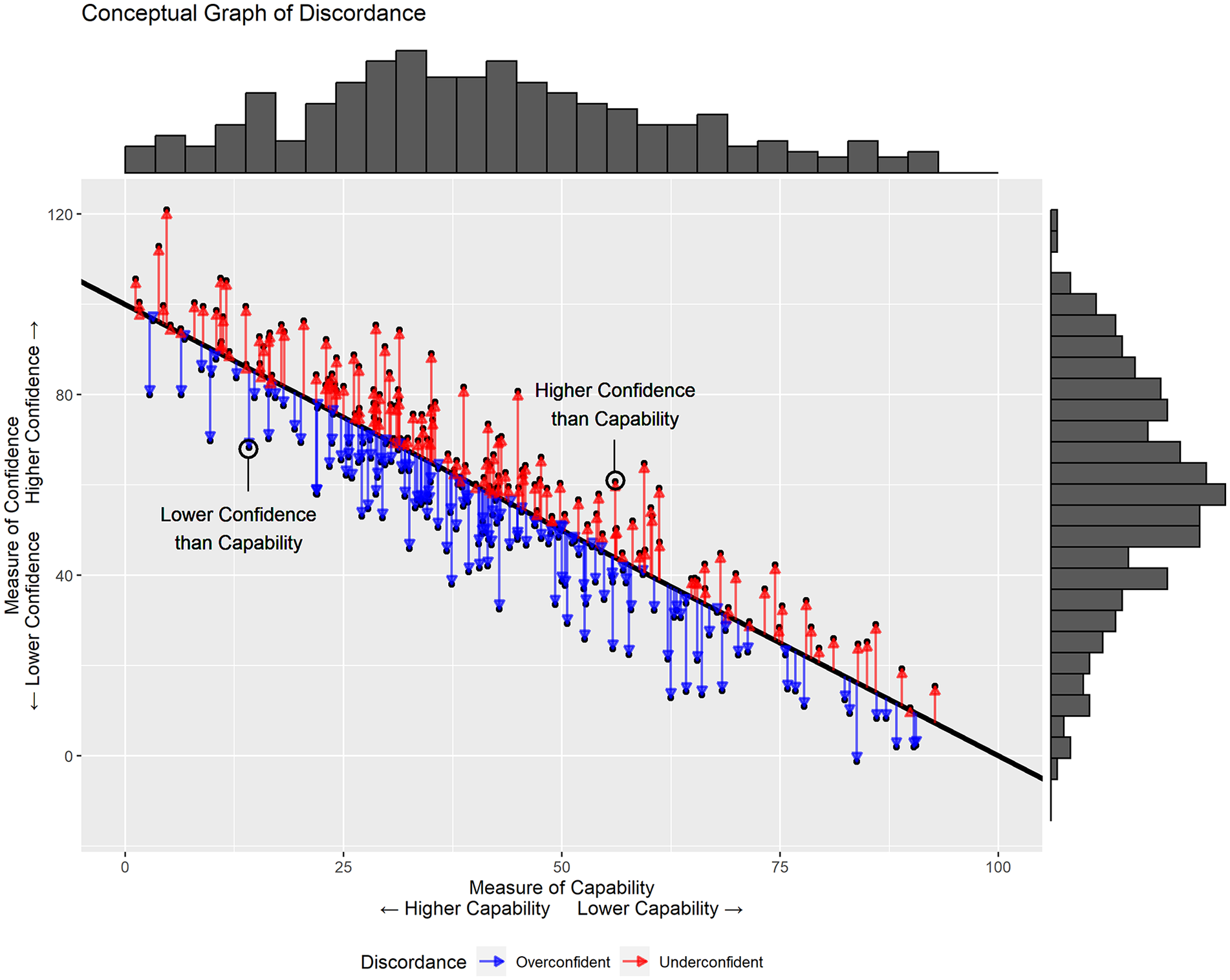
Conceptual graph representing the calculation of discordance between a measure of capability (x-axis) to a measure of confidence (y-axis). The black line represents the predicted value of confidence given a specific value of capability. Individual discordance would be calculated as the residual difference between the actual value of confidence versus the predicted value of confidence. The arrows that connect the black fitted line to the actual value of confidence represent the varying magnitude of discordance given this approach, that is longer arrows represent greater discordance than short arrows. Furthermore, arrows that are coded as red represent negative discordance (individuals with perceived confidence greater than their predicted confidence based on their balance performance) and blue arrows represent positive discordance (individuals with perceived confidence less than their predicted confidence based on their balance performance).
Model Selection to Identify Method of Discordance Calculation
To determine which approach (simple linear vs segmented regression) would provide the strongest association for individual falls, a bootstrapping approach for each model was performed. Specifically, the entire dataset was iteratively resampled 1000 times to generate random training and test sets to first generate the TUG-specific discordance metric using the training set (ie, either linear or segmented regression model with ABC score as the dependent variable, TUG as the primary dependent variable, and age, sex, and MDS-UPDRS part III score as control variables). Then, using the fitted model from the training set estimated TUG-specific discordance (predicted ABC – actual ABC) on the test set was calculated and then used as the primary independent variable in a logistic regression model with Falls (Faller vs non-Faller) as the dependent variable and age, sex, and MDS-UPDRS part III scores as control variables. For each bootstrap iteration, a predicted versus actual confusion matrix for falls was generated and the area under the curve for each model was stored for each model type (linear regression discordance AUC versus segmented regression discordance AUC). This bootstrapping approach allows for a distribution of fall predicted accuracy between discordance type to be compared using an independent t-test. Results of the t-test would allow us to infer which model for deriving discordance (linear vs segmented) had the better association with falls.
Analysis of Discordance to Falls in PD
If there was no significant difference between the discordance metrics, then the simple linear model of discordance would be used as the simpler of the 2 models. Once the discordance metric of best fit was determined, then logistic regression on the entire dataset would be used to examine the relationship between the validated measure of discordance to individual falls (Faller vs non-Faller) with discordance as the primary independent variable and control variables of age, sex, and MDS-UPDRS part III score.
Results
Participant Characteristics
A total of 244 people with PD were used in this analysis across 5 studies with a mean age of 69.5 ± 8.1 years, with 103 (42.2%) identifying as female. The average ABC score among all participants was 77.6 ± 19.0, with an average MDS-UPDRS part III score of 35.9 ± 14.3, and 97 (40%) identified as having a recent fall (Table 1). Between sites there were significant differences in ABC score (P < .001), distribution of sex (P < .001), MDS-UPDRS part III score (P < .001), and number of people with a recent fall (P = .04; Table 2). Between group differences in TUG by study could not be calculated given the difference in TUG method used by site. Overall, inclusion of each study demonstrates the variation in balance confidence, gender distribution, disease severity, and faller status across sites.
Descriptive Characteristics for the Combined Sample.
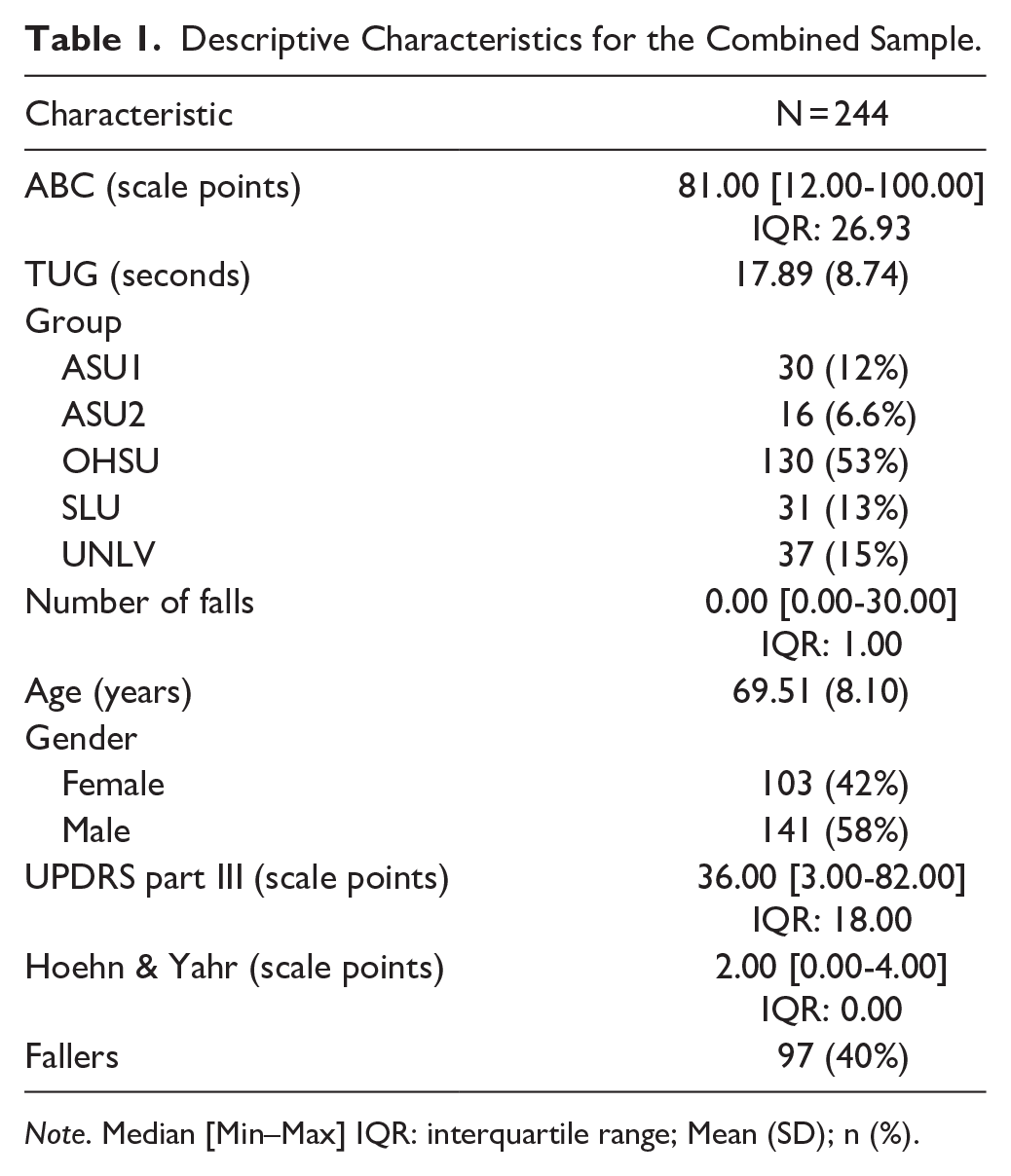
Note. Median [Min–Max] IQR: interquartile range; Mean (SD); n (%).
Descriptive Characteristics by Data Set.
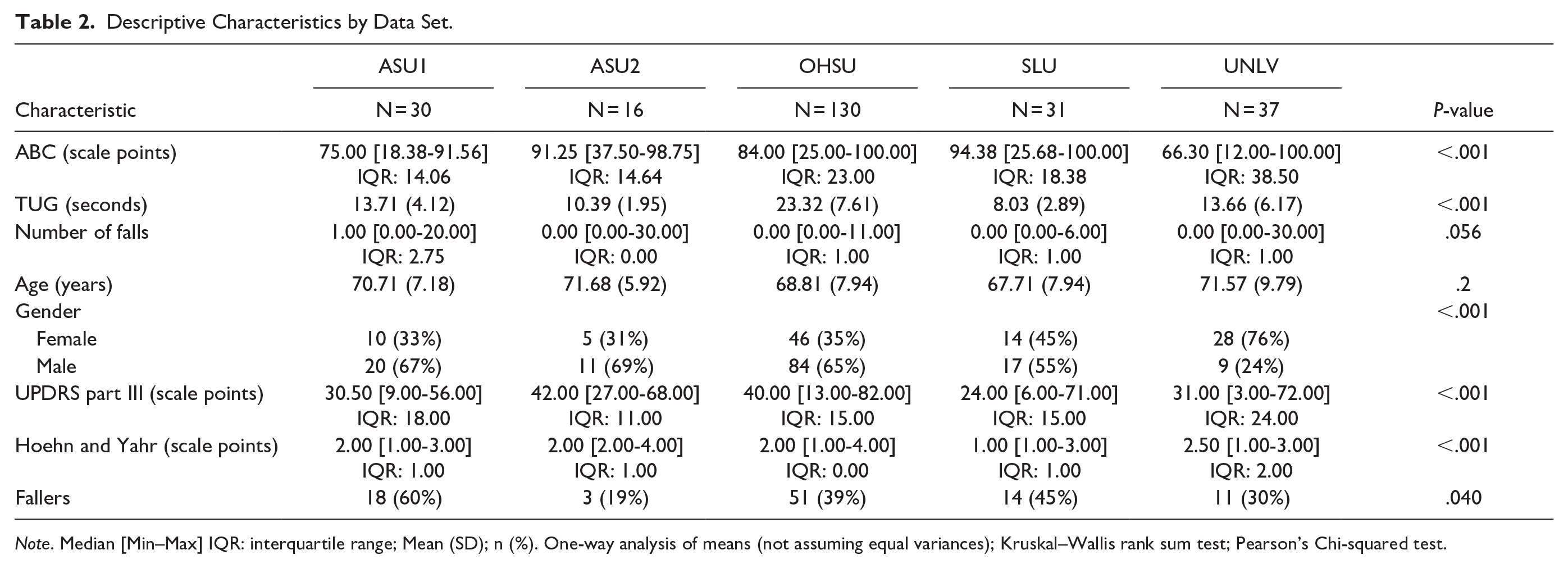
Note. Median [Min–Max] IQR: interquartile range; Mean (SD); n (%). One-way analysis of means (not assuming equal variances); Kruskal–Wallis rank sum test; Pearson’s Chi-squared test.
Validation of Between Study TUG to ABC Relationship
Results that compared significant deviation in the TUG to ABC relationship by group were non-significant (adjusted P > .05 for all group-by-TUG pairwise comparisons, Figure 2) which suggests that, when normalized, there is no difference in the relationship between the different type of TUG variation to individual ABC score when controlling for individual age, sex, and MDS-UPDRS part III score.
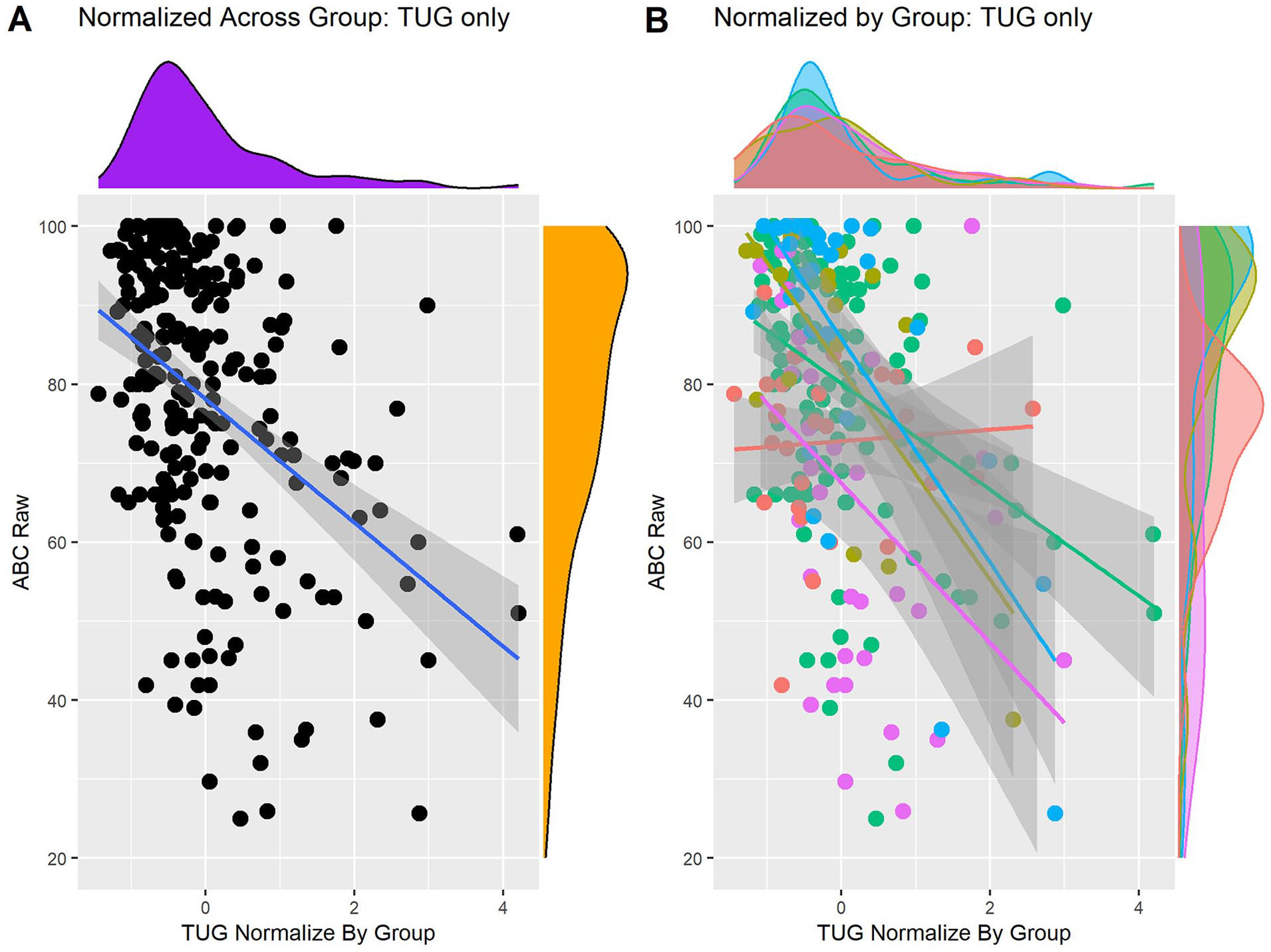
A comparison of the distribution and relationship between TUG when normalized to the individual site mean both when (A) combined and (B) stratified by group. A represents the combined relationship between normalized TUG to the raw ABC scores with the distribution of each measure on the x and y axes, respectively. B represents the individual site relationships between normalized TUG and raw ABC scores with the individual distributions for each sites TUG and ABC scores on the x and y axes respectively.
Selection of Discordance Measure
The optimal knot for our segmented regression approach based on knot placement that yielded the lowest AIC was 1.469 (Supplemental Figure 1, segmented model fit to complete dataset can be seen in Figure 3B). The segmented regression analysis then used in the bootstrapping approach used this knot. Comparison between bootstrap distributions (simple linear vs segmented regression) of AUC values revealed no significant difference (P = .52, mean linear = 0.692 ± = 0.035, mean segmented = 0.691 ± −0.035, Supplemental Figure 2). Therefore, the value of discordance derived from the simple linear regression model was used (simple linear regression model fit to complete dataset can be seen in Figure 3A).
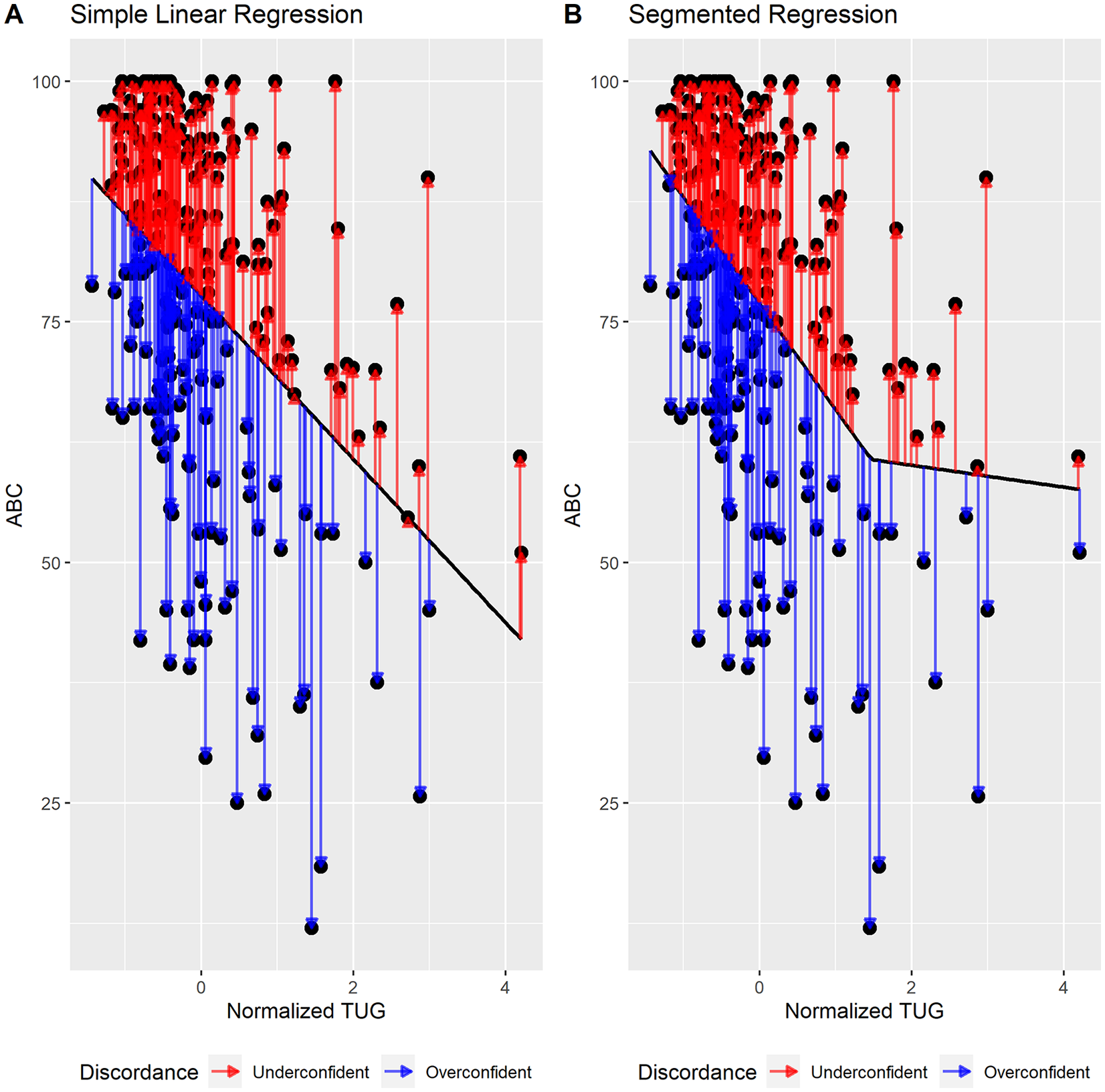
Visual representation of the calculated discordance between the different regression methods. (A) Simple Linear Regression. (B) Segmented Regression with an optimal knot at 1.47. Arrows that are coded blue represent positive discordance values that equate to individuals with less perceived confidence than their model predicted confidence. Arrows that are coded red represent negative discordance values that equate to individuals with greater perceived confidence than their model predicted confidence.
Relationship to Discordance to Faller Status
Results of the logistic regression model with faller status as the dependent variable (Faller vs non-Faller) demonstrated that discordance was the only statistically significant measure (OR = 0.98, 95% confidence interval [CI] [0.96, 0.99], P = .003, Figure 4). This result indicates that a 1 unit increase in discordance (less confidence per ability) is associated with a 2% increase in probability of being classified as a faller. Neither TUG (OR = 1.34, 95% CI [0.98, 1.86], P = .07), Age (OR = 1.01, 95% CI [0.98, 1.05], P = .52), MDS-UPDRS part III score (OR = 1.01, 95% CI [0.99, 1.3], P = .25), or sex (ORmale = 1.22, 95% CI [0.70, 2.16], P = .48) were associated with faller status. The overall model AUC was .68, with a sensitivity (prediction of faller) of 35%, a specificity (identification of non-faller) of 82%, and an overall accuracy of 63%. Within the context that the no-information criterion is 40% (ie, the predictive accuracy of a naïve classifier (Faller ~ 1)) the inclusion of discordance in the logistic regression model boosted the predictive accuracy by 58% (63/40).
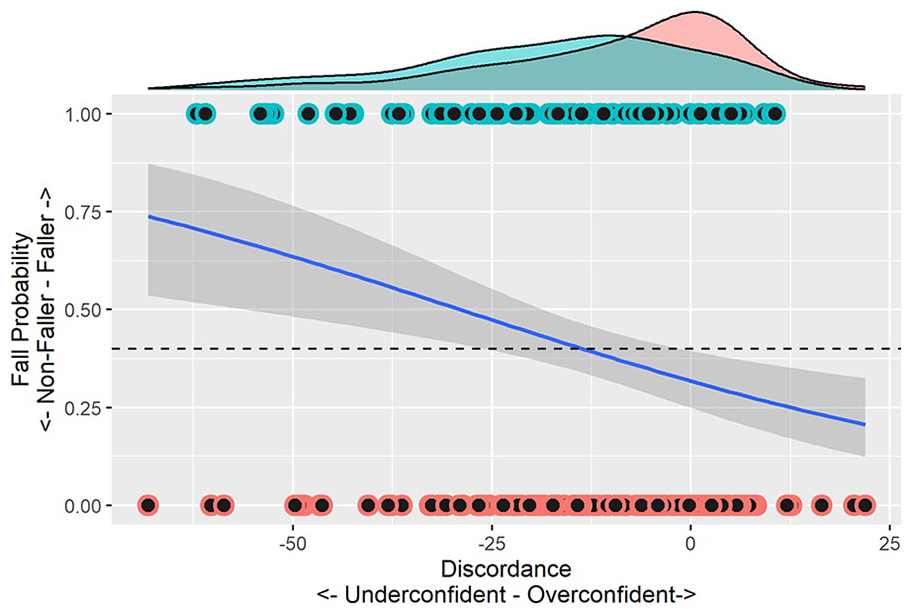
The binomial relationship between probability of being a faller or a non-faller to magnitude of simple linear regression derived discordance. Density plots on the superior x-axis visualize the distribution of the fall types given the value of discordance with greater confidence (higher perceived balance confidence compared to predicted balance confidence) associated with a greater probability of being a non-faller. The horizontal dashed line represents the no-information criterion which is equal to 40% given that only 97 out of 244 participants in the study were classified as Fallers.
Discussion
It is well established that deficits in actual and perceived balance relate to negative outcomes such as falls.17,42 -44 Results of the current project extend this work, showing that the accuracy of individual’s perceived balance (ie, discordance between actual and perceived ability) also relates to fall risk. Specifically, using a novel, continuous quantification of discordance between actual and perceived balance ability, we show that under-confidence is related to retrospective falls, even after accounting for balance performance alone. Although additional work will be necessary to understand the directionality of this relationship, this work highlights an important and under-studied aspect of falls and fall prevention.
Previous work has introduced the idea of discordance between actual and perceived balance, and its potential importance.2,13 However, while this work provided important theoretical groundwork, methods proposed to quantify discordance in a sensitive and quantitative way were limited. Landers and Nilsson 2 and Delbaere et al 13 both suggested categorization of individuals as inappropriate or maladaptive (discordantly over or under confident) or appropriately adaptive (concordant). However, this approach loses the continuous nature of the relationship between perceived and actual ability and is not sensitive to subtle changes in concordance. Therefore, a goal of the current analysis was to propose a quantitative approach to characterize this construct. To achieve this, we first needed to establish a line of best fit relating perceived with actual balance, or a concordance line. Theoretically, an individual at any point on this line would have an appropriate weight between perceived and actual balance and, thus, would be concordant. The results of this study indicate that a simple linear relationship best fit the data, rather than alternative non-linear approaches. Discordance was then operationalized as the vertical distance from the concordance line or the difference in ABC from predicted ABC based on the concordance line. This relies on the assumption that there is a relatively similar number and degree of individuals that manifest as under- and over-confident and that the individuals closest to the fitted line exhibit a concordant relationship. It is possible that in certain populations, including PD, other factors (eg, disease severity, psychological contributors, impaired cognition) or measurement tool limitations (eg, floor and ceiling effects) may shift the mean away from “true” concordance. However, this study successfully developed a quantitative method for describing discordance and showed that discordance as uniquely related to falls, providing initial evidence for the construct validity of this measurement approach.
The second goal of this study was to investigate the relationship of discordance to a functionally relevant outcome such as falls. We observed that discordance uniquely and more strongly related to fall status (faller vs non-faller) than other included factors, including MDS-UPDRS, ABC, TUG, age, or sex. Additionally, inclusion of discordance substantially improved the predictive accuracy of the model to correctly classify participants according to fall status. This illustrates the potential of quantifying and considering the interplay between perceived and actual balance abilities. This study found that as discordance increased (less confidence per ability) the odds of being classified as a faller also increased. In other words, participants who were under confident were more likely to be classified as fallers. This finding is somewhat surprising, given previous notions that over confident individuals may be a greatest risk for falls given their lack of activity curtailment to match their diminished balance abilities or their lack of insight to their balance deficits. 2 However, this finding is consistent with those of Delbaere et al 13 who found that among older adults with similarly elevated physiologic fall risk, those with lower perceived fall risk were less likely to experience a fall. While the factors that contribute to and help provide meaning to this finding will require further investigation, it is possible that this finding may be related to altered attentional strategies for balance control. One possible explanation of this finding is that under confident individuals may excessively attend to their movement particularly in balance challenged situations which may interrupt automatic processes which are potentially more efficient and effective at maintaining balance control and safety in these situations. Notably, prior work has found an increased propensity for conscious control of movement production as PD progresses. 45 Follow-up work will need to determine whether discordance is related to outcomes such as mis-prioritization of attentional resources or cognitive dysfunction and robust longitudinal studies are needed to understand the relationship between balance, balance confidence, falls, physical activity restriction, and the development of discordance. It is possible that changes in constructs such as balance confidence, self-efficacy, and fear of falling may exert an important and distinct influence on discordance and subsequently on mitigating fall risk. Additionally, future studies should consider the progression and development of discordance, notably the sequence of worsening of balance and balance confidence, relative to falls and PD progression.
This study utilized a coordinated data analysis approach in which data across 5 studies and 4 sites were combined to accomplish the aims of this project. Meta-analytic approaches of this sort align with contemporary open science approaches and the efficient use of scientific resources. In the context of this project, coordinated data analysis allowed for the combination of data to increase the breadth/range of the data; this was advantageous as understanding the value of discordance is best accomplished by having a variety of data points in both the under and overconfident regions. Additionally, this study combined sets of diverse data which utilized a variety of administrations of the TUG. Despite these differences in approach, the analytic method revealed that the relationships were consistent among the data sets and this allowed for inferences to be generalized across the variations in the mobility-related postural control task of the TUG. Additionally, as the results of this study were consistent, despite data stemming from multiple sites and methods of TUG administration, this underscores the robustness of the findings related to the aims of this study.
Discordance as a measure that relates both perceived and actual balance abilities, may have clinical utility for fall reduction. Current approaches, utilizing physical or behavioral change interventions to improve physical or perceived balance and mobility outcomes, only partially mitigate falls and increase physical activity.7,46,47 Therefore, discordance may be an additional intervention target to both optimize physical activity and reduce falls, by addressing both the perceptual and actual balance and their alignment.2,13 Optimization of intervention for these purposes would require a multifaceted approach that includes physical and behavioral change methods, and potentially others, to be used together in a coordinated fashion.7,47 -49 Assuming this to be the case, optimal outcomes are likely to be achieved more efficiently and more frequently when applying this theoretical approach to the clinical management of disorders that impact physical abilities, including but not limited to PD.
This study has several limitations which should be considered when interpreting its findings. First, as noted, this study utilized retrospective data from 5 prior studies, across 4 sites. Although the coordinated data analytic approach employed in this study provided a robust method to, at least partially, address the heterogeneity across these studies, it should be considered in the interpretation of results. Additionally, across these data sets, differing TUG procedures were utilized. Despite analyzing the congruence of relationships between TUG and ABC across all data sets, it is possible that differing TUG protocols may have subtly affected the relationships with ABC, which would consequently affect the calculation of discordance. However, analytic approaches were undertaken to confirm that the discordant relationships were not significantly different across studies. Further, while not ideal for internal validity, the variety of TUG procedures does allow for more generalizable interpretation of findings. The use of ABC as the variable of perceived balance is prone to a ceiling effect which may make estimation of concordance among those with a maximum measurement of balance confidence limiting (ie, a perceived balance measure without a ceiling effect would enable better estimation of discordance among individuals with high balance confidence). Previous research has shown that measures that are not prone to either ceiling or floor effects provide the most robust relationships.50,51 The use of the TUG as a measure of balance performance is also a limitation as it is a measure of both balance and functional mobility, and may have a different relationship to balance confidence than a measure that is confined exclusively to the domain of balance, such as the MiniBESTest. Future research should investigate if the discordance relationship is improved by inclusion of more aligned performance and perceived ability measurement tools (ie, MiniBESTest and ABC). Although the line of best fit for quantifying discordance was determined to be derived from simple linear regression, it should not be assumed this is true across all cases and will generalize to a more impaired population. Due to measurable skew in both the ABC and TUG measures, representing a sample with generally higher balance confidence and faster TUG times on average, among a sample that is more impaired a non-linear line may serve as a more sensitive measure of discordance. Future research should aim to reproduce the findings presented here among a sample that is more normally distributed across the measures of perceived and actual balance. TUG testing was completed in different PD medication states between studies. Given that no differences in the relationship between TUG and ABC were observed between studies, that the TUG data was normalized, and that the anticipated effect of lack of PD medications would be a universal slowing of gait, we do not anticipate that this had an influence on the findings of the current study. However, it is difficult to determine to effect of medication on discordance with confidence due to the differences in medication status and TUG administrations between studies. Additionally, the reporting period for retrospective falls varied between studies from 6 months to 1 year. Considering the varying falls reporting period and PD severities between studies it is possible that the results of this study could be affected by different degrees of PD progression. Additionally, it is possible that the retrospective nature and differences in reporting period could have influenced the findings regarding the relationship between discordance and falls, however, falls data was used in the analyses as dichotomous variable (faller vs non-faller) which may limit this influence. Further, as falls were obtained via retrospective report this data is prone to recall bias. Future studies should employ prospective approaches for capturing falls-related data. Additionally, future studies should investigate factors that influence the development and manifestation of discordance, such as cognition, mood, and gait and balance limitations.
Conclusion
This study utilized a coordinated analysis approach to develop a novel method for the quantification of agreement between actual and perceived balance referring to this on a spectrum from concordant to discordant. Discordance was subsequently found to be uniquely related to falls among individuals with PD. Clinicians and researchers should consider discordance between actual and perceived balance in conditions that impact physical abilities, such as, but not limited to PD as a potentially modifiable target to minimize falls and fall risk while optimizing physical engagement.
Supplemental Material
sj-pdf-1-nnr-10.1177_15459683241300456 – Supplemental material for Discordance Between Balance Ability and Perception Is Associated With Falls in Parkinson’s Disease: A Coordinated Analysis
Supplemental material, sj-pdf-1-nnr-10.1177_15459683241300456 for Discordance Between Balance Ability and Perception Is Associated With Falls in Parkinson’s Disease: A Coordinated Analysis by Jason K. Longhurst, Andrew Hooyman, Merrill R. Landers, Martina Mancini, Erika Franzén, Breiffni Leavy, Hanna Johansson and Daniel Peterson in Neurorehabilitation and Neural Repair
Supplemental Material
sj-pdf-2-nnr-10.1177_15459683241300456 – Supplemental material for Discordance Between Balance Ability and Perception Is Associated With Falls in Parkinson’s Disease: A Coordinated Analysis
Supplemental material, sj-pdf-2-nnr-10.1177_15459683241300456 for Discordance Between Balance Ability and Perception Is Associated With Falls in Parkinson’s Disease: A Coordinated Analysis by Jason K. Longhurst, Andrew Hooyman, Merrill R. Landers, Martina Mancini, Erika Franzén, Breiffni Leavy, Hanna Johansson and Daniel Peterson in Neurorehabilitation and Neural Repair
Supplemental Material
sj-pdf-3-nnr-10.1177_15459683241300456 – Supplemental material for Discordance Between Balance Ability and Perception Is Associated With Falls in Parkinson’s Disease: A Coordinated Analysis
Supplemental material, sj-pdf-3-nnr-10.1177_15459683241300456 for Discordance Between Balance Ability and Perception Is Associated With Falls in Parkinson’s Disease: A Coordinated Analysis by Jason K. Longhurst, Andrew Hooyman, Merrill R. Landers, Martina Mancini, Erika Franzén, Breiffni Leavy, Hanna Johansson and Daniel Peterson in Neurorehabilitation and Neural Repair
Supplemental Material
sj-pdf-4-nnr-10.1177_15459683241300456 – Supplemental material for Discordance Between Balance Ability and Perception Is Associated With Falls in Parkinson’s Disease: A Coordinated Analysis
Supplemental material, sj-pdf-4-nnr-10.1177_15459683241300456 for Discordance Between Balance Ability and Perception Is Associated With Falls in Parkinson’s Disease: A Coordinated Analysis by Jason K. Longhurst, Andrew Hooyman, Merrill R. Landers, Martina Mancini, Erika Franzén, Breiffni Leavy, Hanna Johansson and Daniel Peterson in Neurorehabilitation and Neural Repair
Footnotes
Author Contributions
Jason K Longhurst: Conceptualization; Data curation; Funding acquisition; Methodology; Project administration; Resources; Writing—original draft; Writing—review & editing. Andrew Hooyman: Data curation; Formal analysis; Methodology; Project administration; Resources; Software; Visualization; Writing—review & editing. Merrill R Landers: Methodology; Resources; Writing—review & editing. Martina Mancini: Funding acquisition; Methodology; Resources; Writing—review & editing. Erika Franzén: Methodology; Writing—review & editing. Breffni Leavy: Methodology; Writing—review & editing. Hanna Johansson: Methodology; Writing— review & editing. Daniel Peterson: Conceptualization; Data curation; Funding acquisition; Methodology; Project administration; Resources; Writing—review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the support of the Saint Louis University Applied Health Research Council, the Irma Ruebling Endowed Research Fund, the Michael J. Fox Foundation (under Grant #008373), Department of Veterans Affairs Grant No. I01 RX001075, NIH, NIA Grant No. R01AG006457, and NIH grant No. R25HD105583-03.
ORCID iDs
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.