
Abstract
Background
In recent decades, there has been a widespread adoption of digital devices among the non-disabled population. The pervasive integration of digital devices has revolutionized how the majority of the population manages daily activities. Most of us now depend on digital platforms and services to conduct activities across the domains of communication, finance, healthcare, and work. However, a clear disparity exists for people who live with severe quadriplegia, who largely lack access to tools that would enable them to perform daily tasks digitally and communicate effectively with their environment.
Objectives
The purpose of this piece is to (i) highlight the unmet needs of people with severe quadriplegia (including cases for medical necessity and perspectives from the community), (ii) present the current landscape of assistive technology for people with severe quadriplegia, (iii) make the case for implantable BCIs (how they address needs and why they are a good solution relative to other assistive technologies), and (iv) present future directions.
Results
There are technologies that are currently available to this population, but these technologies are certainly not usable with the same level of ease, efficiency, or autonomy as what has been designed for the non-disabled community. This hinders the ability of people with severe quadriplegia to achieve digital autonomy, perpetuating social isolation and limiting the expression of needs, opinions, and preferences.
Conclusion
Most importantly, the gap in digital equality fundamentally undermines the basic human rights of people with severe quadriplegia.
Introduction
The lived experience of those with severe quadriplegia is challenging for non-disabled people to truly understand. We would ask readers to take a moment to imagine the feeling of living day-to-day with severe quadriplegia. You are in tune with your surroundings, emotions, and thoughts, but in many situations, your ability to express yourself or communicate your needs has been stripped away. Imagine the feelings of frustration and isolation that would be almost constantly present as you are excluded from various activities with family and friends due to your disability. From seemingly mundane activities of daily living (ADLs) such as dressing and eating, to the patience and concentration required to navigate instrumental activities of daily living (IADLs), such as communicating with family and caregivers, people with severe quadriplegia often experience challenges navigating a world that is not designed to accommodate their needs and wants. This can be a constant and emotionally draining source of worry for people with disabilities. 1 Crucially, though, it is a problem that could be solvable with access to appropriately designed augmentative communication technology. Here, we argue that current assistive technology offerings do not adequately address certain key functional needs of people living with severe disability, particularly those with locked-in syndrome resulting from conditions such as severe amyotrophic lateral sclerosis (ALS), whereby a person is not able to move or speak but is cognitively healthy. If correctly designed, implanted brain–computer interfaces (BCIs) represent a class of technologies that have the potential to address many current technological pitfalls. The ability to accurately evaluate and measure the functional utility of these emerging technologies will be crucial, and will specifically inform if and how they have the potential to improve the safety, wellbeing, and independence of people living with severe quadriplegia.
Unmet Needs of People With Severe Quadriplegia: The Case for Medical Necessity and Perspectives From the Community
The Case for Medical Necessity
Severe Quadriplegia, Loneliness, and Social Isolation
People who have a communication impairment live with a greater risk for social isolation and loneliness. 2 The severity of these social impacts are likely to be more pronounced in people who have greater functional limitations and more severe communication difficulties (P < .001), R2 = .114, F(9,725) = 10.345, P < .001. 2 In people with severe quadriplegia, including locked-in syndrome and ALS, interactions with the outside world can be made more difficult by bulbar or other vocal dysfunctions. These communication challenges can result in the loss of participation in regular daily activities. 3 The loss of independence and fear of embarrassment associated with functional limitations can further limit social interactions. 4 Prell et al 5 noted that one of the strongest predictors of poor emotional well-being in people with ALS was the feeling of embarrassment in social situations. Relatedly, Schlüter et al 6 found stigma to be a powerful predictor for social withdrawal in people with ALS, and noted that social withdrawal was associated with worse motor disability, increased anxiety and depression, and even poorer bulbar function.
One qualitative study summarized themes of the non-disabled population discounting or underestimating a person’s abilities or assigning negative attributes to people with quadriplegia. These negative societal views perpetuate the model that people with severe quadriplegia do not have the ability to participate in a meaningful way in society, lead an active lifestyle, 7 or do not have the “desire” to develop romantic and/or sexual relationships, despite this being considered a normal part of identity for a non-disabled person. 8 Disengagement in romantic and sexual relationships have a direct effect on feelings of loneliness, helplessness, and overall quality of life. 9
The physiological impacts of social isolation and loneliness are well documented in the non-disabled population (Figure 1). Valtorta et al 10 found that poor social relationships were associated with a 29% increased risk of incident coronary heart disease, a 32% increased risk of stroke in the general population, as well as increased risk of cancer and infectious diseases. 11 Further, loneliness has been associated with a 40% increased risk of dementia 12 and can have profoundly negative effects on mental health. 13 Brown et al 14 found higher levels of reported loneliness to be associated with higher blood pressure and inflammatory reactivity to acute stress. Sleep quality and general cognitive decline have also been shown to be adversely impacted by these 2 constructs. 15
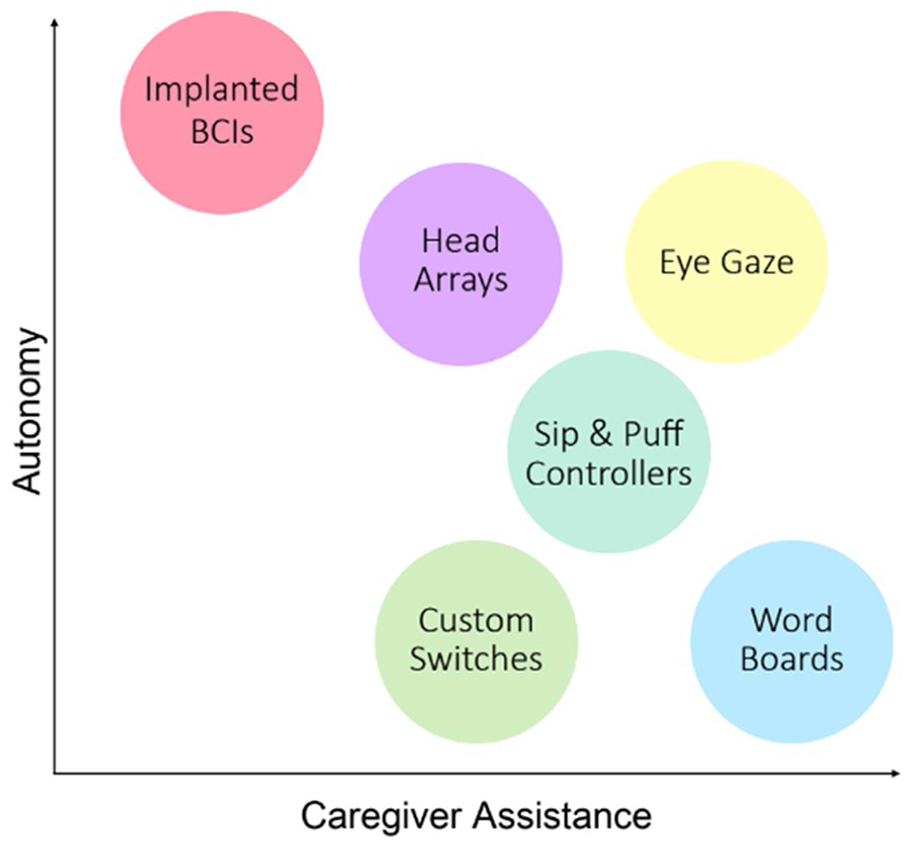
A visual representation the amount of caregiver assistance versus the autonomy able to be achieved for various assistive devices in people with severe quadriplegia.
Those with severe quadriplegia who experience loneliness may not only be predisposed to negative health sequelae and have poorer clinical outcomes, but may have higher hospitalization rates and an increased cost of care as a result, 16 irrespective of their underlying disease course. Importantly, poor emotional well-being is associated with more rapid disease progression in people living with ALS. 5
Beyond the unaddressed humanitarian crisis of lack of access to assistive technology, there is unfulfilled medical necessity to provide communication assistance to people with severe quadriplegia. In the non-disabled population, social isolation and loneliness can have substantial negative impacts on a person’s mental and physical health. The absence of social relationships has been linked to an almost 30% increased risk of all-cause premature mortality. 17 Social isolation and loneliness are similar but independent notions; social isolation refers to objectively having few relationships, social interactions and roles, and links within the community, whereas loneliness is a subjective state, whereby there is a perceived isolation between a person’s preferred and actual social experience.18,19
Timeliness and Ease of Medical Communication
In addition to being able to communicate effectively to reduce feelings of isolation, people living with severe quadriplegia often need to communicate urgent needs to their primary caregiver or home health aide in order to avoid severe health sequelae. A correlation can exist between the speed and efficiency with which a person with severe disability can communicate discomfort, pain, or a need and the severity of the outcome. For instance, the faster a person can communicate that they’re experiencing pain or heat on their skin that may lead to a pressure sore, the quicker their care team can engage in remediation techniques such as changing position or adjusting padding or mattress settings to avoid skin breakdown. 20 Not being able to express themselves in a timely manner can cause substantial frustration for people with severe quadriplegia. In this day and age, there is a heavy focus on technology innovation, but at present, technology is failing people with severe quadriplegia.
Perspectives From the Community
Table 1 highlights real-life scenarios from people who are listed authors of this piece as well as anonymous patient authors who are people living with severe quadriplegia or their caregivers. These people were interviewed to understand common scenarios that highlight how specific daily lived experiences represent failure to live up to the general principles of the Convention of Rights of Persons with Disability. 21 Whether it be to communicate a care need, alert the care team to an emergent medical issue or even report abuse, it is clear that members of the disability community with severe quadriplegia face a critical, unmet need that impacts their very ability to survive. Quality of life and important clinical outcomes have the potential to be substantially impacted by a person’s ability to communicate continuously and autonomously.22-24 As we attempt to conceptualize what a solution to these issues might look like, the concept of a technological interface that is continuously active no matter the environment, able to be independently activated by the user without the need for calibration, and at a minimum, able to provide a single digital output. This is an extremely challenging set of technological needs, but with the advancement of invasive BCI technology, there is hope that these needs might be met.
Real Life Limitations of Technology Against the Principles of the Convention of Rights.

Abbreviations: AAC, augmentative and alternative communication; ALS, amyotrophic lateral sclerosis; BCI, brain–computer interface; SCI, spinal cord injury.
Current Landscape of Assistive Technology for People With Severe Quadriplegia
Non-Implanted Technologies
As we close out the first quarter of the 21st Century, along with the rise of affordable and accessible consumer electronics, we have seen a rapid proliferation of assistive technologies for people with severe quadriplegia. This includes a wide array of assistive technologies that are available for independent home use, including custom switches that can be activated with isolated limb movements, head arrays that can be activated with directional head movements, 40 technologies that harness facial expressions to control digital devices, 41 a variety of sip-and-puff controllers, 42 eye tracking technologies, 43 and electroencephalography (EEG)-controlled or “non-invasive” BCIs. 44 Although these technologies have all demonstrated the potential to restore lost autonomy to a severely paralyzed person under the correct circumstances, these technologies often require significant setup from a caregiver or home health aide, regular recalibration, and typically only work in a controlled, closed environment thereby offering limited options for the user outside of their home (Figure 2). Per the World Health Organization’s multinational survey, around 85% of people with a disability need at least 1 assistive product, while 31% of those are unable to access the technology they need. 45 When viewed through the lens of optimizing user safety, this represents a significant limitation of augmentative communication technology. Similarly, low or no-tech solutions, such as word boards, rely on a caregiver to facilitate the scan, recall the selections correctly, and determine the communication in a timely, sometimes urgent, manner. Current technology does not allow for effective and rapid communication with the outside world, limiting social interactions and the ability for people with severe disability to express their needs, opinions, and preferences. Furthermore, the medical connotation and visible machinery of many current devices may contribute to stigma, affecting self consciousness and the willingness to socialize, 46 which may contribute further to the social isolation and exclusion that people with severe quadriplegia experience.
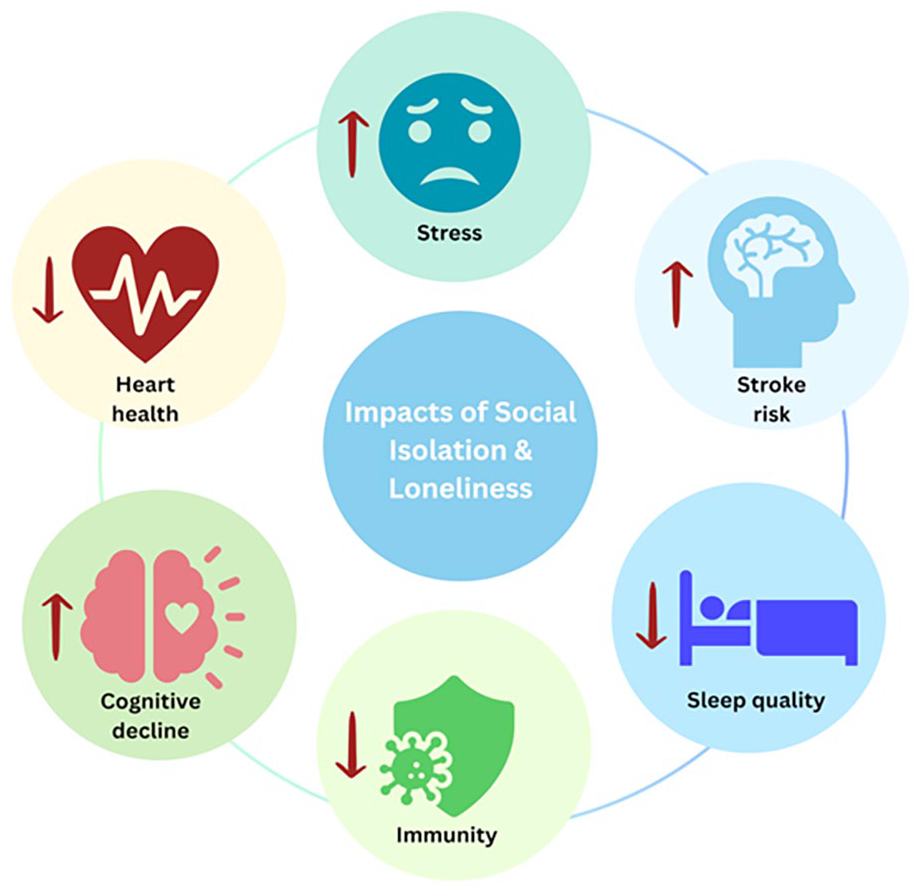
Physical and psychological impacts of loneliness and social isolation on body systems.
Implantable Technologies
BCI is becoming a household phrase with many emerging technologies that have the potential to indelibly change the way that humans interact with technology and the external environment. A BCI is a piece of technology that records neural activity from the brain and uses it to control an external piece of technology such as a personal computer, 47 robotic arm,48,49 or sensory technology, without the need for muscular control.48,49 Recently, the BCI society evaluated feedback from global BCI stakeholders and have provided a formal working definition: “A brain–computer interface is a system that measures brain activity and converts it in (nearly) real-time into functionally useful outputs to replace, restore, enhance, supplement, and/or improve the natural outputs of the brain, thereby changing the ongoing interactions between the brain and its external or internal environments. It may additionally modify brain activity using targeted delivery of stimuli to create functionally useful inputs to the brain.” In addition to this working BCI definition, it is important to make the distinction between assistive and rehabilitative BCIs: a rehabilitative BCIs aim to restore loss of functions by stimulating the recovery of impacted circuits in the brain, whereas an assistive BCIs aim to bypass the damaged circuits by using BCI as an alternative means of communication and control. Over the years, there have been many forms of BCI technologies that range from entirely non-invasive EEG devices, 50 to a variety of different implantable technologies including but not limited to epidural and sub-galeal, 51 direct cortical, 52 and endovascular implants. 47 BCI technologies that aim to exert direct control over the physical environment have enjoyed a history of widely publicized progress. For example, in the United States, the general public were able to witness a woman who had been paralyzed for over 15 years use her thoughts to control a robotic arm to lift a bottle of coffee to her mouth and take a drink. 49 Over a billion people witnessed a young man with paraplegia, wearing an EEG-controlled, robotic exoskeleton, kick a ball to launch the 2014 FIFA World Cup opening ceremony in São Paulo, Brazil.53,54
Despite progress in implantable BCI research, they have not yet successfully transitioned as a technology that can be used independently in the home or without significant assistance from a team of engineers, let alone a home health aide or primary caregiver. 55 The reason for this is multifaceted, and includes patient-related aspects causing individual variability in performance for anatomical, cognitive, or other patient-specific characteristics (eg, age, sex, and lifestyle), and technology-related factors. 56 By contrast, many non-implantable BCI technologies (and advanced assistive technologies such as eye-tracking) have achieved basic home use utility, but often the caregiver burden associated with daily technology setup, paired with the unpredictable performance of the technology and environmental limitations has led to limited uptake. 57 More recently however, BCIs that utilize endovascular implant technology have successfully transitioned to more independent home use, enabling a first generation of patients to experience unsupervised cognitive control of a digital device. 47
The transition to home use for implantable BCI technology is an evolutionary moment in the field, but it has also raised important questions about how to measure the clinical need for such an intervention. The question of “medical necessity” typically guides conversations about reimbursement and access to both implantable and non-implantable advanced assistive technologies. However, more pressing than medical necessity is an argument for the fundamental human rights of those living with severe quadriplegia. In recent decades, people living with a disability have been represented by National and International laws and treaties in order to protect their rights and provide access to services and technology that can drive improvements in autonomy and quality of life. For instance, article 3 of the United Nations Convention on the Rights of Persons with Disabilities 21 asserts that all people with disabilities have a fundamental right to: (1) inherent dignity; (2) individual autonomy; and (3) full and effective participation and inclusion in society. 58 In the United States specifically, Section 504 of the Rehabilitation Act of 1973 serves to protect people from being discriminated against based on their mental or physical disabilities. Whilst there have been great advocacy advancements and technology innovations to improve autonomy and quality of life for people with disability in recent decades, presently these advancements do not fully extend to cover people who are living with severe disability, for example severe quadriplegia, particularly those who are reliant on others for ADLs and IADLs, and communication. Together with participation restrictions and a loss of autonomy that can occur over time in this population, 59 there is a critical need to make technology easily available to this community that will improve social connectedness, reduce loneliness and social isolation, and uphold fundamental rights for people with severe disabilities.
The Case for Implanted BCIs: Continuous, Independent Digital Control
Implanted BCIs have the potential to allow people with severe quadriplegia to express themselves freely and thereby exercise their first amendment right. There are many features of implanted BCI technologies that position them to solve the complex issue of continuous digital autonomy for those with severe quadriplegia (Figure 3). The first issue that is currently unaddressed is the need for existing augmentative technology to be physically positioned onto or near the user every day by the care team in order for the technology to be productively utilized. Any movement, of the end user or the technology alike, requires a member of the care team to readjust the technology to allow the end user to continue using it productively. Unlike existing, non-invasive augmentative communication or digital control technologies, invasive BCIs have the theoretical potential to be fully implanted into the user, with no requirement that a caregiver be present to regularly adjust or position the technology so that it can be used. A fully implanted system of this nature has the potential to open the door to more seamless, independent use of assistive control technologies for the disability community, and attempts at such a system have been met with early success.47,60
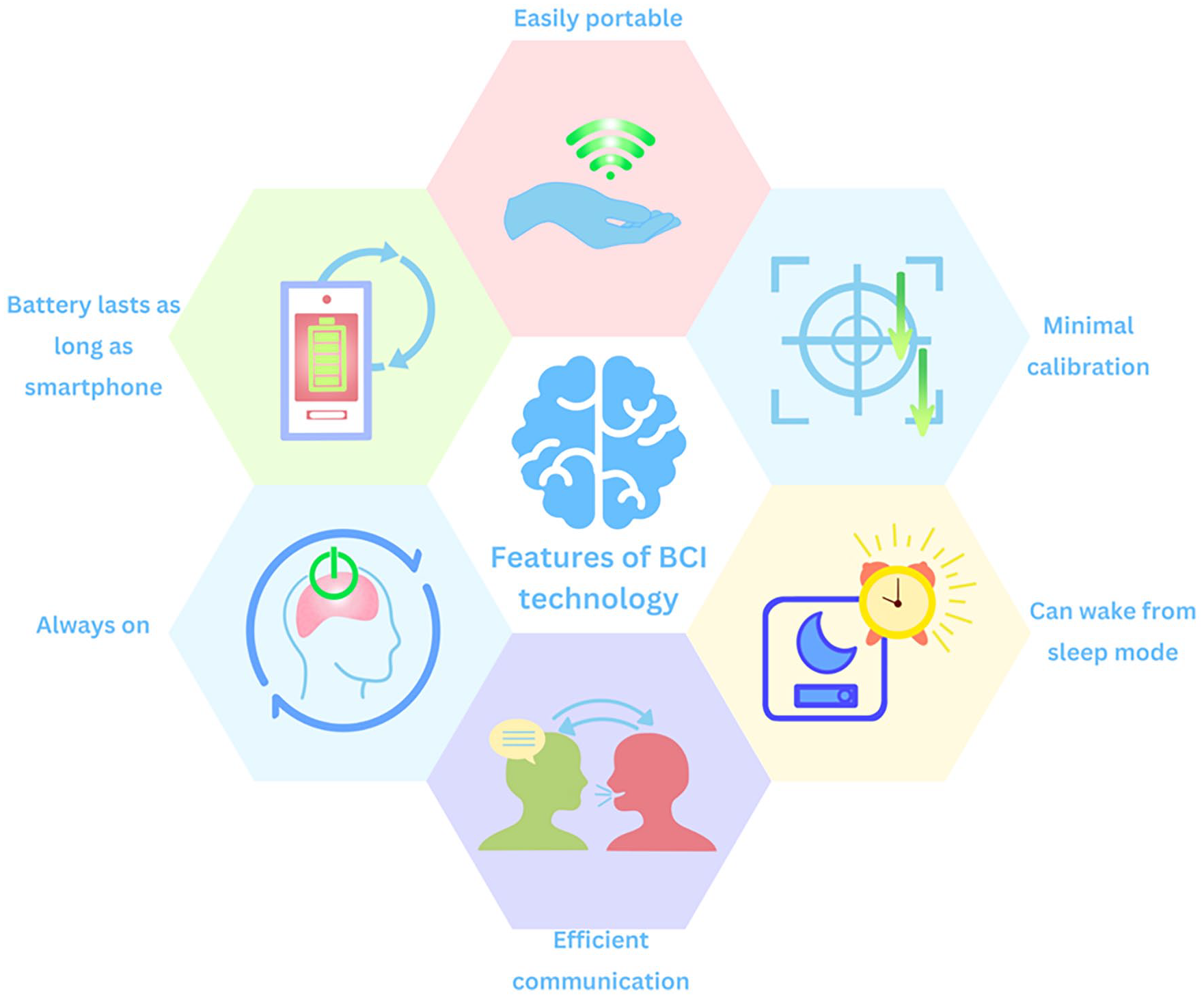
Proposed requirements of implanted brain–computer interface technology.
In addition to the physical needs and limitations of existing technologies, there are also software requirements that must be met in order to achieve the goal of continuous digital autonomy. Namely, optimal assistive control software must be continuously “on” and running in the background, able to be activated and used independently by the end user at any time and able to be used for long periods (weeks or months) of time without the need for recalibration. To date, there are no non-invasive systems that have the capacity to meet needs such as these, but early attempts at independent home use of invasive systems are showing promising signs that these requirements will be feasible and achievable with emerging technologies. For instance, the Synchron endovascular BCI system has shown that it can feasibly record and implement usable brain signals over a period of 12 months without the need for recalibration after the initial post-implantation training. 47 However, in order to fully address the software requirements for continuous digital autonomy, what remains to be achieved by implantable and non-implantable systems is the ability for the system end user to maintain a stable, functional, and continuous connection to the assistive software system regardless of environment, time of day, or (within similar limits of, say, a cell phone) ability to charge the system.
A final consideration for continuous digital autonomy is the question of a minimal functional level for system utility. If a continuously active system is to be useful to a person with severe quadriplegia, the system must, at a minimum, be capable of quickly and reliably producing a single, digital command output at all times. 35 This final, minimal requirement is easily achievable by many systems, but when achieved in combination with the other previously detailed requirements, it would represent a highly unique and previously unseen assistive technology. Namely, it would produce an assistive technology that would allow for a person with severe quadriplegia to never be without a means for notifying their care team of an emergent need. The peace of mind and safety that such a system would bring to those with severe disability and their caregivers cannot be understated.
Safety Considerations
While there is an ethical imperative to provide better assistive technology to meet the needs of people with severe quadriplegia, this needs to be be balanced with the ethical and safety considerations of implanting a technology on or within the brain. As with other implantable medical devices, there is direct surgical risks associated with implantable BCIs, such as infection, bleeding, damage to areas surrounding the implantation zone and appropraite monitoring during the post-implantation period. Minimizing these risks is the focus of current clinical trials.47,52 Additionally, compatibility and long-term durability of the implants must be considered. One of the most talked about considerations amonst the community is data security and privacy. Ensuring encryption and secruity of signals, and creating policies to prevent misuse of patients data is imperitive.
Cost
The costs associated with implantable BCIs is yet to be determined considering their safety and efficacy is still under investigation in clinical trials. Given the comprehensive nature of the surgical procedure, the advanced technology involved, and the necessity for ongoing maintenance and monitoring, it is likely that implantable BCIs will be in the magnitude of 10-fold more expensive than some non-implanted options. Currently, researchers are working to develop a battery of objective and patient-reported outcome measures to support the case for reimbursement of these devices once they reach the market. These measures aim to provide robust evidence of the clinical benefits and quality of life improvements associated with BCIs. This evidence will be crucial for integrating BCIs into standard medical practice and ensuring that patients who could benefit from this technology have access to it despite the high initial investment. On the topic of cost-benefit analysis, the scientific methodology to investigate this may warrant a clinical trial of implantable BCI versus non-invasive BCI (or another control technology). However, whether there is ethical equipoise to investigate this given the humanitarian need and medical necessity is questionable. In any case, we must continue to urge BCI companies and regulatory bodies to center patient voices and engage in rigorous community co-design, since the true value of any additional amount of restored autonomy enabled by implantable BCI technology can ultimately only be conveyed by the end-user.
Patient-centered BCI clinics Given the investigational nature of implantable BCIs at present, clinical models of how these devices will be implanted, evaluated, and maintained in real world scenarios is yet to be determined. Neurosurgeons/neurointerventionalists are likely to continue to be the professionals who manage the implantation and acute care given their specialized expertise in brain surgery. Following the implantation period, neurologist are the clinicans who have traditionally provided outpatient longitudinal care for patients affected by the conditions that would warrant an implantable BCI. Given their expertise in the nervous system anatomy and physiology, these specialists would be well positioned to manage patient care. Regarding long term training and use of the device, there is a compelling case for this new specialty falling under the umbrella of Rehabilitation Medicine, led by physiatrists. This approach aligns with current clinicl models that manage other implantable devices such as vagal nerve and spinal cord stimulators. Rehabilitation specialists are well-equipped to handle the multidisciplinary aspects of post-implantation care, including device calibration, patient training, and ongoing health monitoring. Multidisciplinary clinics (including the above-mentioned specialists, as well as speech and language pathologists, occupational therapists, and physical therapists) are a tried and tested method in the neurological and neuromuscular space that are likely to translate well to the long-term care of people with implantable BCIs. Engagement with all professional stakeholders is essential to solidify these clinical care pathways.
Future Directions
In people with severe quadriplegia, the ability to engage with their environment has been directly linked to quality of life. 61 While there is technology available to assist people with severe quadriplegia, such as assistive augmentative communication or non-invasive BCIs, current methods seldom meet people’s needs in their entirety. The reasons for this are multifactorial, and may include the technology not being able to support the words per minute that the person with severe quadriplegia desires to express, perceptions about the person’s capabilities, or caregivers not having the skills to set up and support the physical aspects of such technologies. Implantable BCI technology is a potential solution for restoring lost continuous digital autonomy, enhancing safety, wellbeing, and autonomy. 62 This opinion piece highlights the fundamental and critical needs of people with severe quadriplegia that are currently unmet.
To support the progress of the implantable BCI field, a critical next step is to create a battery of objective and patient reported outcome measures, specific to BCI, to ensure that we can accurately report on the effectiveness of motor neuroprostheses both in restoring digital motor output, as well as recording how a person with severe quadriplegia feels, functions, and survives. 55 Without these BCI-specific outcome measures, there is a very real possibility that we will not be able to demonstrate efficacy of implanted BCIs, affecting their ability to reach the market with reimbursement. Additionally, as we look away from research, and toward the future of people with an implanted BCI being managed by clinical teams in the healthcare setting, it is critical that these novel outcomes are sufficiently obvious and straightforward to allow reimbursement applications to be completed with sufficient ease for clinicians working in the field, thus reducing the current pressures that reimbursement applications for current technologies can create.
We strongly support the involvement of people with lived experience and their caregivers in all components of BCI research and outcome measure development. People with lived experience and their caregivers hold key insights into the challenges, requirements, and preferences of assistive technology, including BCIs. These emerging technologies can potentially raise important ethical questions related to privacy and autonomy, and as such, involving the end-user throughout the research and commercialization process is imperative.
Footnotes
Acknowledgements
The authors would like to acknowledge Judy Heumann.
Author Contributions
Abbey Sawyer: Conceptualization; Data curation; Methodology; Visualization; Writing—original draft; Writing—review & editing. Lily Cooke: Conceptualization; Writing—original draft; Writing—review & editing. Erica Breyman: Conceptualization; Writing—original draft; Writing—review & editing. Steve Spohn: Investigation; Writing—original draft; Writing—review & editing. Sandy Edelman: Investigation; Writing—original draft; Writing—review & editing. Krisha Saravanan: Conceptualization; Visualization; Writing—review & editing. David Putrino: Conceptualization; Methodology; Supervision; Visualization; Writing—original draft; Writing - review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.