
Abstract
Background
Post-stroke depression (PSD) is a frequent psychiatric complication, however very few studies have investigated its relation to the affected upper extremity (UE) post-stroke. Objective. To compare the affected UE in terms of motor impairment, functional ability, and daily-use in individuals with and without PSD during the first 6 months post-stroke.
Methods
This study analyzed data from a previous cohort; participants were assessed at rehabilitation admission (T1), 6 weeks (T2), and 6 months (T3) post-stroke. At each time point we compared between participants with and without PSD (Geriatric Depression Scale score ≥ 5). The Fugl-Meyer Motor Assessment assessed motor impairment, Action Research Arm Test assessed functional ability, and the Rating of Everyday Arm-Use in the Community and Home assessed daily-use. Independence in daily activities and cognition were also assessed.
Results
A total of 116 participants were recruited, 38% had PSD at T1. No significant differences were found between groups at T1 and T2. However, significant differences (z = −5.23 to −2.66, p < .01) were found between groups for all UE measures at T3; participants with PSD had lower motor and functional ability and less daily hand-use than participants without PSD. At T3 participants with PSD were also less independent in daily-living.
Conclusions
PSD is associated with greater UE motor, functional, and daily-use disability at 6 months post-stroke. Our findings underscore the negative impact of PSD on UE during the crucial transition period when individuals return home and integrate back into the community. Further research is needed to delineate the effect of change in PSD status on UE outcomes post stroke.
Introduction
Stroke is considered the primary cause for serious long-term disability worldwide. 1 Common deficits following stroke include motor, sensory, cognitive, and emotional dysfunction. 2 These deficits contribute to difficulties in performing basic and instrumental activities of daily living (BADL and IADL), resulting in long-term disability.3,4
The recovery of the affected upper extremity (UE), contralateral to the brain lesion is challenging. Only 50% of all individuals with an affected UE regain some useful functional ability at 6 months post-stroke. 5 Sixty percent of the individuals with severely impaired affected UE and 30% with a moderately impaired affected UE have a non-functional UE at 6 months post-stroke. 6 Furthermore, improvement of functional ability of the affected UE after clinic-based interventions do not automatically generalize to daily-use of the affected UE in real world settings. 7
Daily-use of the affected UE, also termed real-world use and actual arm use, is defined as the spontaneous integration and use of this UE in the real-world. 8 From the perspective of individuals with stroke, daily-use is considered the most important indicator for UE recovery. 9 Previous studies have identified motor and sensory deficits as key factors that contribute to daily-use of the affected UE. 10 Recent studies have expanded the literature and identified additional factors associated with daily-use including personal factors, environmental factors, and task characteristics, in chronic stroke, 8 as well as UE self-efficacy. 11
Post-stroke depression (PSD) is a common psychiatric personal factor present in about 30% of the individuals with stroke, including those with mild stroke.12,13 PSD is a consequence of stroke, defined as the presence of depressed mood or loss of interest or pleasure along with 4 other symptoms of depression lasting 2 or more weeks.14,15 In a comprehensive systematic review, the presence of PSD was consistently related to poor daily function and decreased independence in BADL. 16 Notably, few studies have investigated PSD and its relation to recovery of the affected UE. The limited literature on PSD and UE outcomes is not consistent. During the subacute phase post stroke, 2 studies found no correlation of PSD with UE motor recovery 17 and functional ability, 18 while another study demonstrated significant negative correlations between PSD and UE motor and function ability. 19 Improvement of UE functional ability of 20 individuals with chronic stroke following a Repetitive Task Practice Program, was found for individuals with and without PSD, but surprisingly a greater improvement was seen in the participants with PSD compared to without. 20 The authors suggested that the group with PSD may have had less motor ability prior to the intervention leaving more “room” to improve. The existing literature on PSD and UE outcomes demonstrate inconsistent findings and notable gaps that warrant further investigation. Most studies focused on the first 3 months post-stroke, assessing a single time point. Examining multiple time points may provide a more comprehensive understanding of the relationship of PSD and UE function and daily-use. The existing studies have focused on UE outcomes specific to motor impairment and functional ability with very little available literature examining the impact of PSD on daily-use post-stroke.
In order to address this gap in the literature, we conducted a secondary analysis of a longitudinal study collected during 6 months post-stroke. We compared the affected UE of participants with and without PSD by assessing UE motor impairment, functional ability, and daily-use at 3 time points during the first 6 months post-stroke. We hypothesized that participants with PSD would demonstrate lower motor and functional abilities, and less daily-use of the affected UE compared to participants without PSD, at all 3 time points during the first 6 months post-stroke. These comparisons will enhance our understanding of the impact of PSD on the affected UE and improve our ability to define accurate treatment goals to improve the UE post-stroke.
Methods
Study Design
This study analyzed data from a previous cohort collected at 3 time points: rehabilitation admission (T1), 6 weeks (T2), 6 months (T3) since stroke onset. A comparison was conducted between 2 independent groups of participants with and without PSD at each time point.
Study Population
We included adults after stroke who were admitted for rehabilitation to 1 of 4 rehabilitation centers. The 4 rehabilitation centers were similar in terms of rehabilitation intensity and length of stay. Participants were eligible if they met the following inclusion criteria: (1) up to 4 weeks post-stroke (determined by computed tomography or magnetic resonance imaging), (2) had full UE function prior the stroke, (3) could understand simple commands, (4) had intact or corrected vision and hearing, and (5) did not have neurological or orthopedic conditions other than stroke.
Clinical Assessments
Depressive symptoms were assessed using the Geriatric Depression Scale-short form (GDS), 21 a self-report measure of different aspects of depression over the last week (e.g., do you feel that your life is empty? Are you afraid that something bad is going to happen to you?). Each of the 15 items are rated by dichotomously (0 or 1) and a total score is calculated. Higher scores indicate more depressive symptoms. A score of 5 points or more suggests depression. The GDS, first created Yesavage et al, 22 and Sheikh et al 23 has been tested and used extensively with the older population to measure depression but has also demonstrated strong diagnostic sensitivity and specificity in younger adults. 24 At each time point GDS scores were used to dichotomize the sample into with PSD (GDS ≥ 5) and without PSD (GDS < 5) groups. 25
Five standardized UE assessments were administered to assess motor impairment, functional ability, and daily-use. Motor impairment was assessed using the Fugl-Meyer Motor Assessment—UE subtest (FMA) 26 and dynamometry. FMA is a reliable and valid assessment to assess motor impairment post-stroke. Score ranges from 0 (no active movement) to 66 points (full active movement). The Jamar Dynamometer was used to assess grip strength in kg in a standardized position. The score is based on the mean of 3 trials. Functional ability was assessed using The Box & Block Test (BBT) 27 and the Action Research Arm Test (ARAT). 28 BBT is a reliable and valid assessment to assess unilateral manual dexterity. 29 Participants were asked to move 1 block at a time from 1 side of a box, over a divider to the other side. The score is the total number of blocks transferred in 1 minute. ARAT is a reliable and valid assessment to assess the functional ability of the affected UE. Total score ranges from 0 (a non-functional UE) to 57 points (a fully functional UE). The Rating of Everyday Arm-Use in the Community and Home (REACH) 30 was used to assess daily-use. REACH captures how the affected UE is used in daily life outside of the clinical setting. Scores (levels) range from 0 (no use/exercise only) to 5 (full use). The test consists of 2 different versions based on typical use for the affected dominant and non-dominant UE. REACH has excellent inter-rater reliability, and has moderate to high correlations with other measures of UE use (Motor Activity Log and accelerometers), functional ability (Action Research Arm Test, Stroke Impact Scale Hand subtest), and impairment (Chedoke–McMaster Stroke Assessment). 30
Our study participants were characterized in terms of independence in daily living and cognition at each timepoint using the Functional Independence Measure (FIM) 31 and the Mini-Mental State Examination (MMSE), 32 respectively. The FIM total score ranges from 18 to 126 points, higher scores indicate more independence. The MMSE assesses orientation, attention, memory, language, and visual-spatial skills; scores range from 0 to 30 points. The IADL Questionnaire (IADLq)33,34 was used only at T3 to assess independence in IADL. This is a self-report questionnaire which assess the ability to perform 8 IADLs. Total score ranges from 0 (not independent in IADL) to 23 points (totally independent in IADL). In addition, demographic and stroke characteristics of the study population were collected at admission from medical records (date, type, and first/ recurrent stroke) and self-report (full/partial independence in BADL prior to the stroke).
Procedure
The study was approved by the Helsinki Committee and the University Ethics Committee at each of the 4 rehabilitation centers. Eligible patients were approached within the first week of rehabilitation and provided an oral explanation regarding the study. Participants who agreed to participate provided written informed consent.
At each of the 4 sites, an experienced occupational therapist administered the clinical assessments in the inpatient setting at T1 and T2 (with the exception of 3 participants who were already discharged home). At T3, data were all collected at the participants’ homes during a home-visit.
Statistical Analysis
Descriptive statistics were used to describe participant characteristics at admission, including stroke information, cognitive status, and independence in BADLs. Since variables did not distribute normally, all descriptive data are presented as median and inter quartile range (IQR) scores, and additional analyses were conducted using non-parametric tests. Median and IQR were used to report scores on UE outcomes, cognition, and BADL independence for the 2 groups at the 3 time points. In order to answer our research question, we decided to look at each time point separately, rather than longitudinally, because the presence of depression in participants was not consistent at all time points. Differences between groups were assessed separately at each time point using the Mann–Whitney U test. Effect size (for Mann–Whitney U test) was calculated [using the formula (r = z/√n) 35 to examine the magnitude of differences found between the 2 groups. Effect size was considered large if r was more than .5, moderate if r was less than .5, or small if r was less than .3. 35 At T3, we further differentiated the PSD group into (1) Always PSD and (2) Converted into PSD subgroups; the Without PSD group was further differentiated into (3) Never PSD and (4) Converted out of PSD subgroups. At T3, the Kruskal–Wallis H test was used to compare between the 4 subgroups. The Mann–Whitney U test was used for post hoc pairwise comparisons between subgroups. Analyses were conducted using SPSS (SPSS, Inc., Chicago, IL, USA), version 27. Statistical significance was set at a threshold of p < .05.
Results
Data were collected between January 2017 and March 2019. During this time, 116 participants were eligible and agreed to participate in the study. They were recruited within 15 (12.0-20.0) days post-stroke, their median age was 71.0 (65.0-80.8) years, and 89.7% had an ischemic stroke. The percentage of PSD at each time point was: 38% of 116 participants at T1, 35% of 105 participants at T2, and 28% of 88 participants at T3. There were no significant differences between the 2 groups in terms of demographics, stroke information, cognition, or in BADL at T1 (see Table 1). See Figure 1 for the progression of the participants throughout the study period. Note the 4 subgroups at T3 for the 83 participants with data at all 3 time points.
Characteristics at T1 for All Participants, and Participants With and Without PSD.
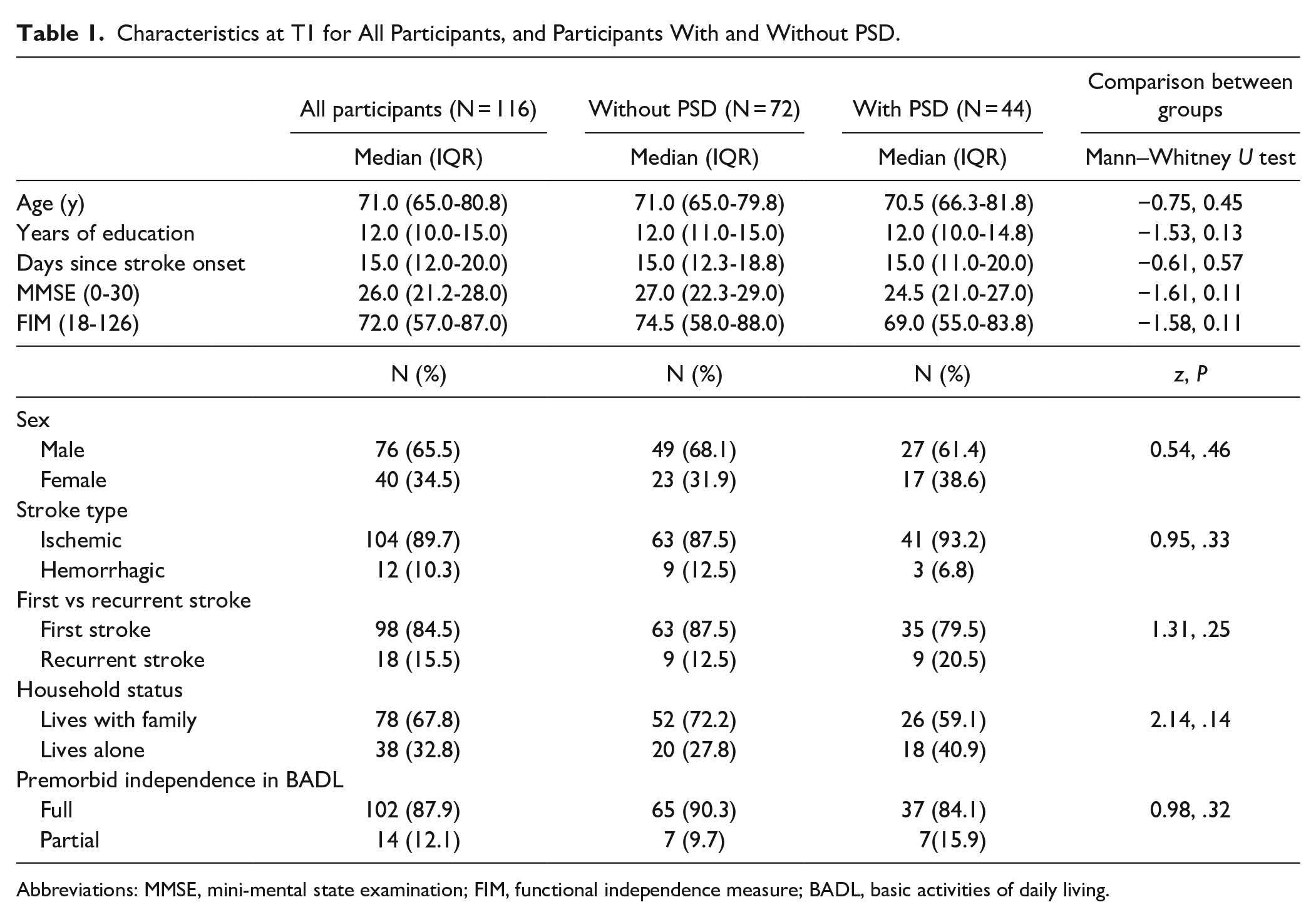
Abbreviations: MMSE, mini-mental state examination; FIM, functional independence measure; BADL, basic activities of daily living.
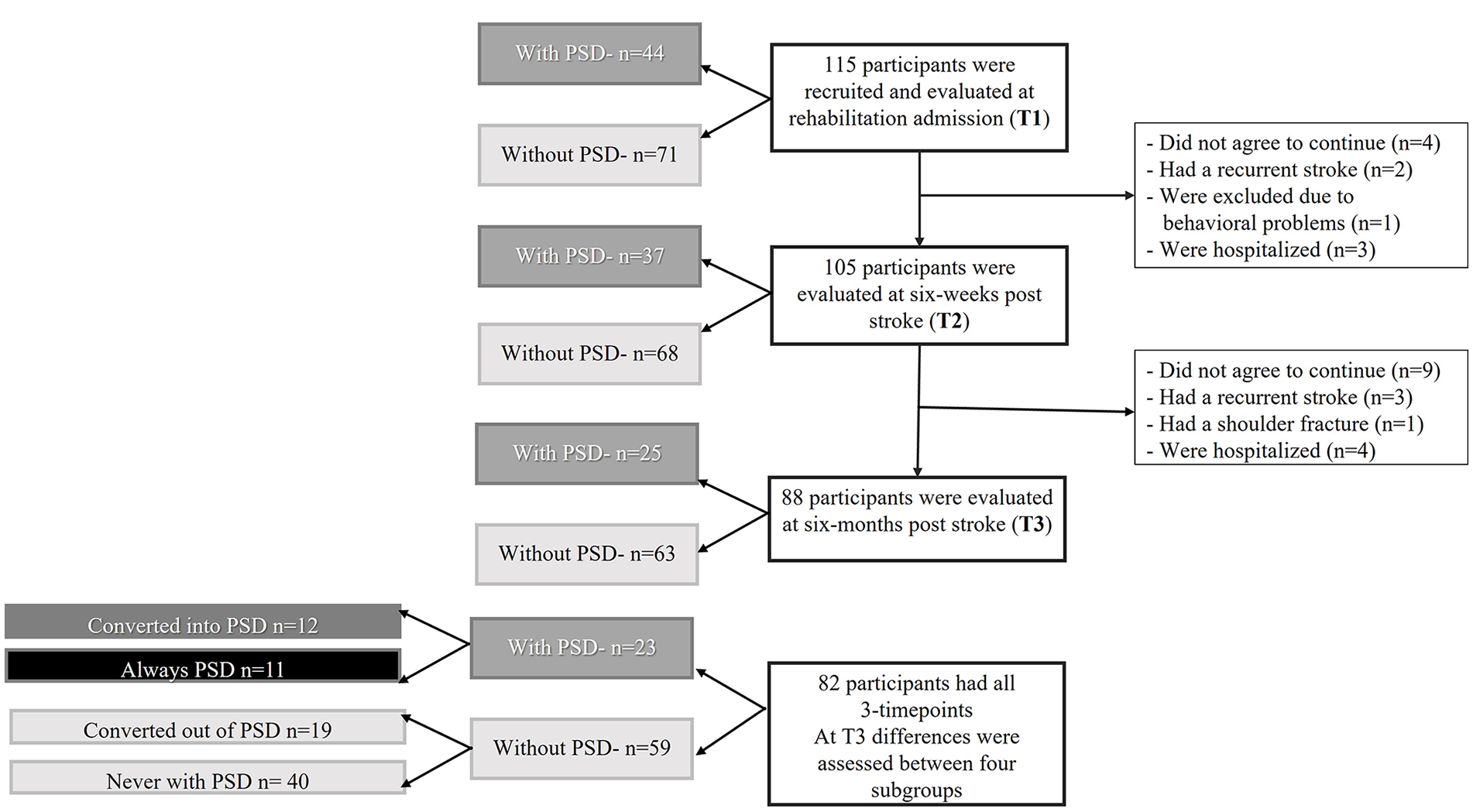
Flow-chart describing the progression of the participants throughout the study period. Note that at T3 differences were assessed also between 4 subgroups of PSD status overtime.
Motor impairment, functional ability, and daily-use of the affected UE were compared at each time point between groups with and without PSD. At T1 and T2, no significant differences (with small effect size) were found in all UE outcomes. However, significant differences (with small, medium, and large effect) were found between the 2 groups at T3. The median (IQR) score for FMA was 62.0 (53.0-66.0) for participants without PSD compared to 31.0 (4.0-56.0) for participants with PSD; median (IQR) ARAT score was 57.0 (49.0-57.0) for participants without PSD compared to 24.0 (0-56.0) participants with PSD and the median (IQR) REACH score was 4.0 (3.0-5.0) for participants without PSD and 2.0 (1.0-3.5) for participants with PSD. In addition, significant between-group differences were found for cognition and independence in BADL and IADL (z = -2.66-5.23, P < .001) at T3. See Table 2 for summary of group comparisons at all time points. Figures 2 to 4 are Box Plots which illustrate comparisons of the FMA, ARAT, and REACH scores between participants with and without PSD at each time point, with the between-group differences at T3 being notably pronounced.
Comparison of UE Outcomes, Cognition, BADL, and IADL for Participants With and Without PSD at T1, T2, and T3.
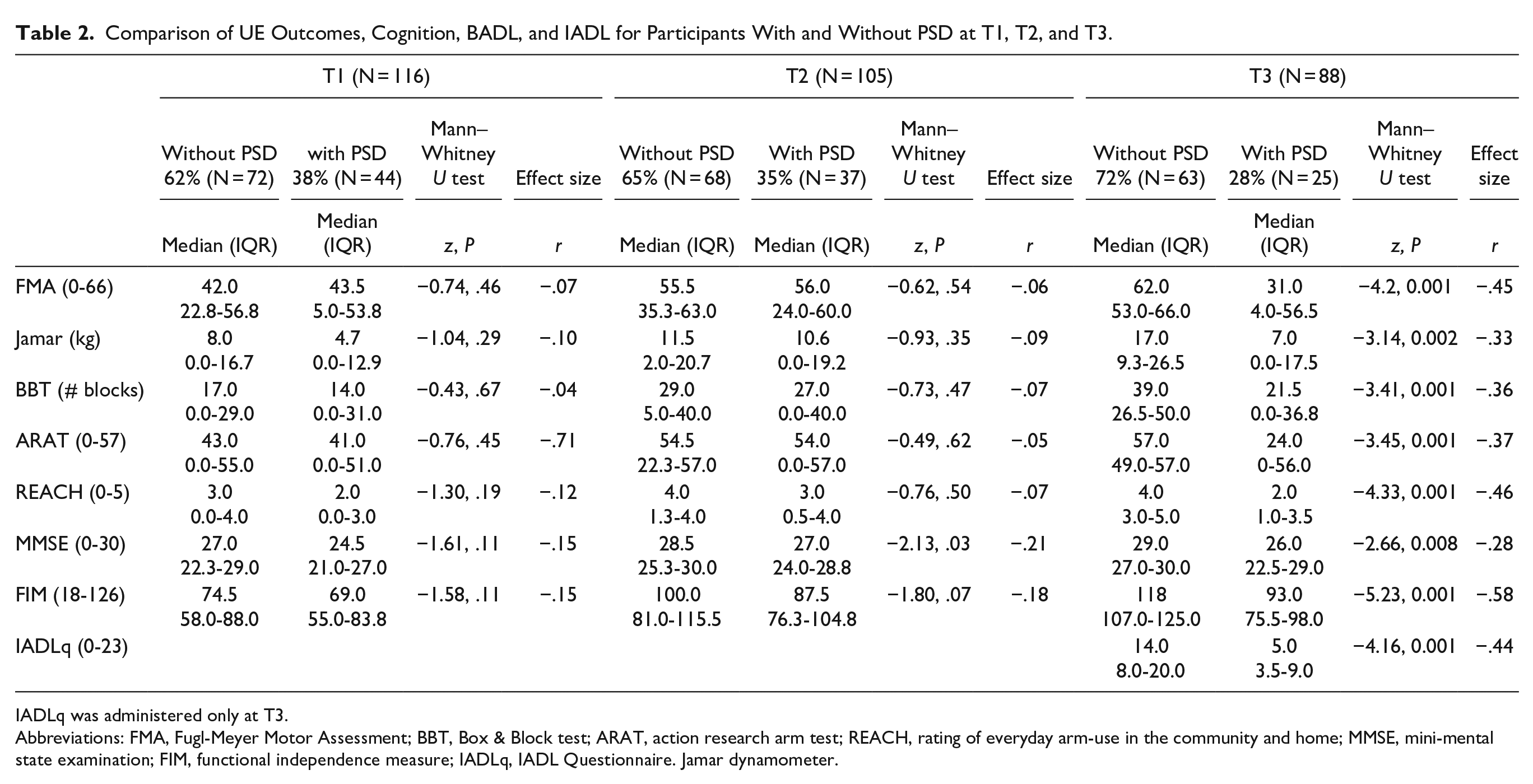
IADLq was administered only at T3.
Abbreviations: FMA, Fugl-Meyer Motor Assessment; BBT, Box & Block test; ARAT, action research arm test; REACH, rating of everyday arm-use in the community and home; MMSE, mini-mental state examination; FIM, functional independence measure; IADLq, IADL Questionnaire. Jamar dynamometer.
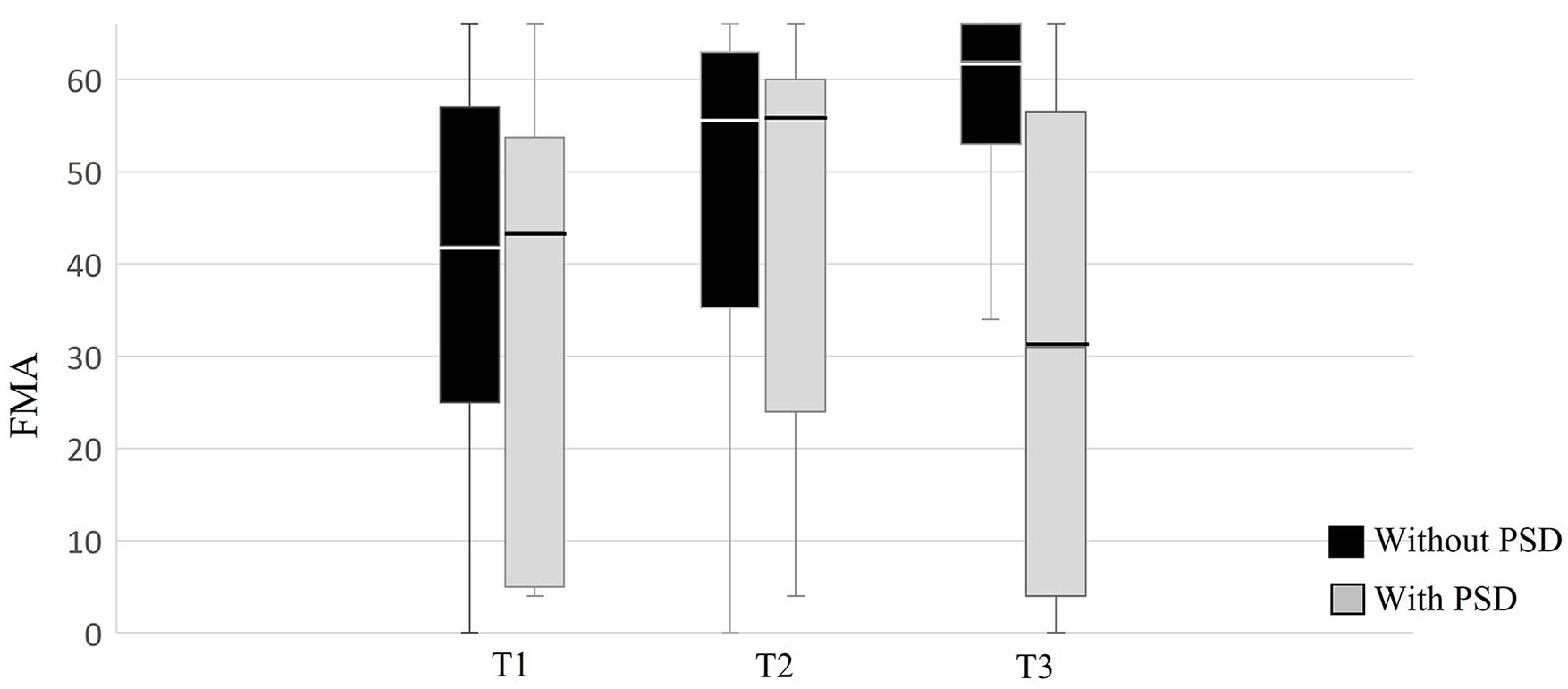
Comparison of the motor impairment as assessed by the Fugl-Meyer Motor Assessment (FMA) between participants with and without PSD at each time point.
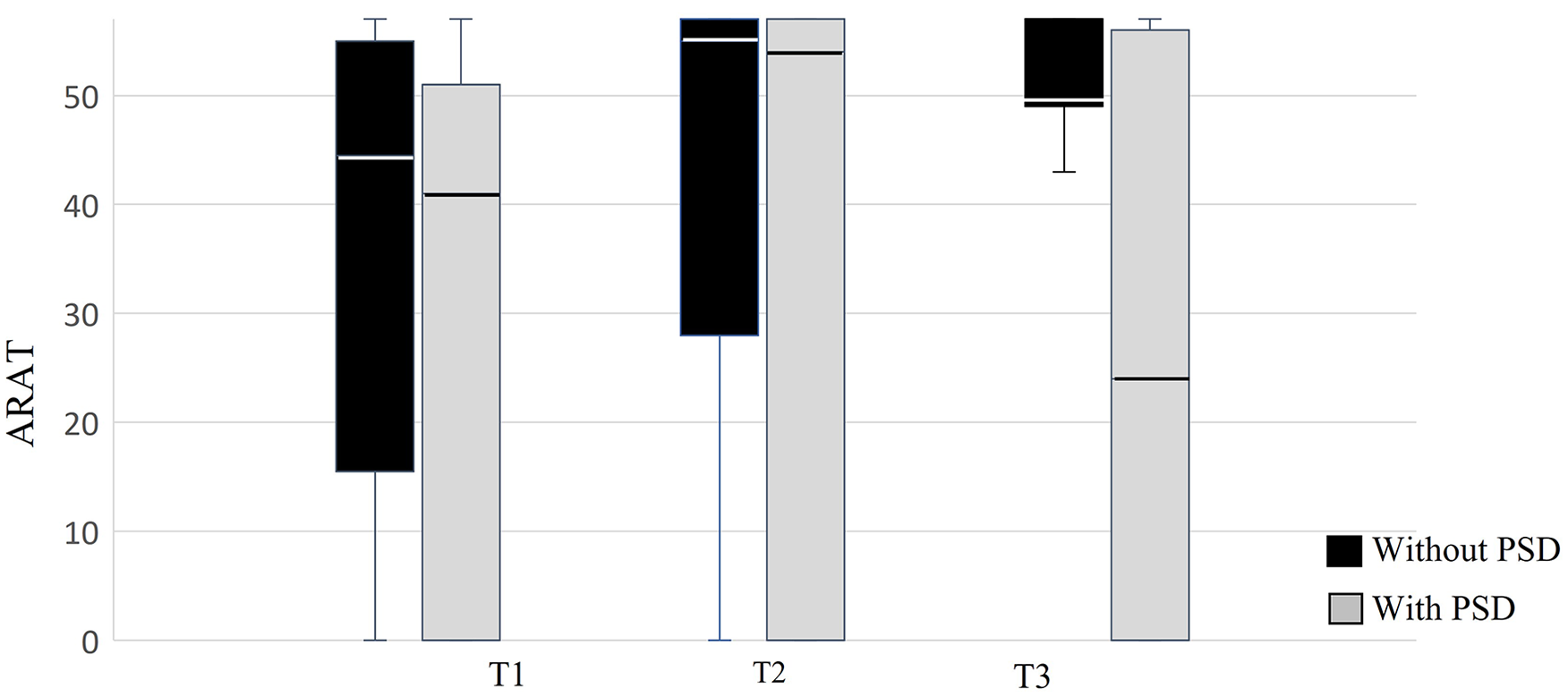
Comparison of the functional ability as assessed by the Action Research Arm Test (ARAT) between participants with and without PSD at each time point.
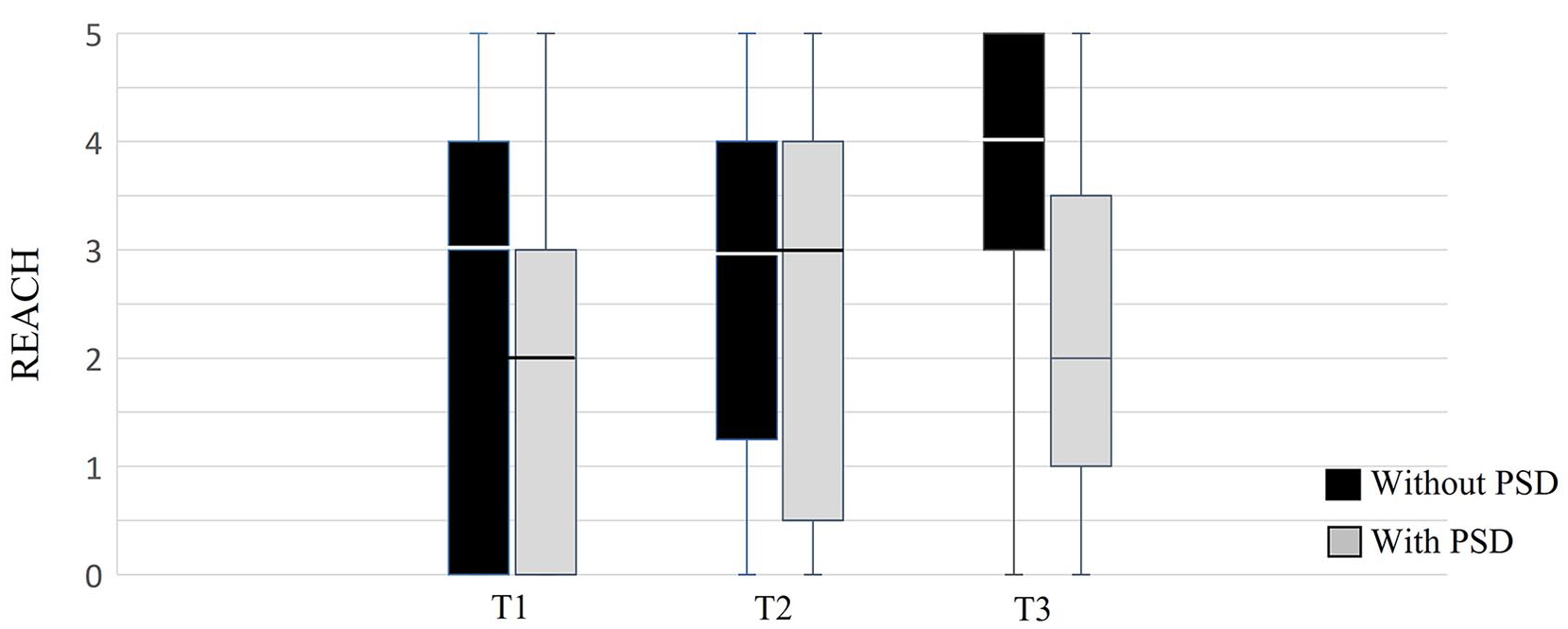
Comparison of daily-use as assessed by the Rating of Everyday Arm-use in the Community and Home (REACH) between participants with and without PSD at each time point. REACH ranges from level 0 (no daily use) to 5 (full daily use).
At T3 we also wanted to take into account the changes in PSD status over time, therefore we compared UE outcomes (FMA, ARAT, and REACH) between the 4 subgroups. Figure 5 confirms that UE outcomes for the 2 subgroups of individuals with PSD was significantly different from the 2 subgroups of individuals without PSD. In addition, there were no differences for the FMA, ARAT, and REACH between the Converted into PSD and Always PSD subgroups, and the Converted out of PSD and Never PSD subgroups.
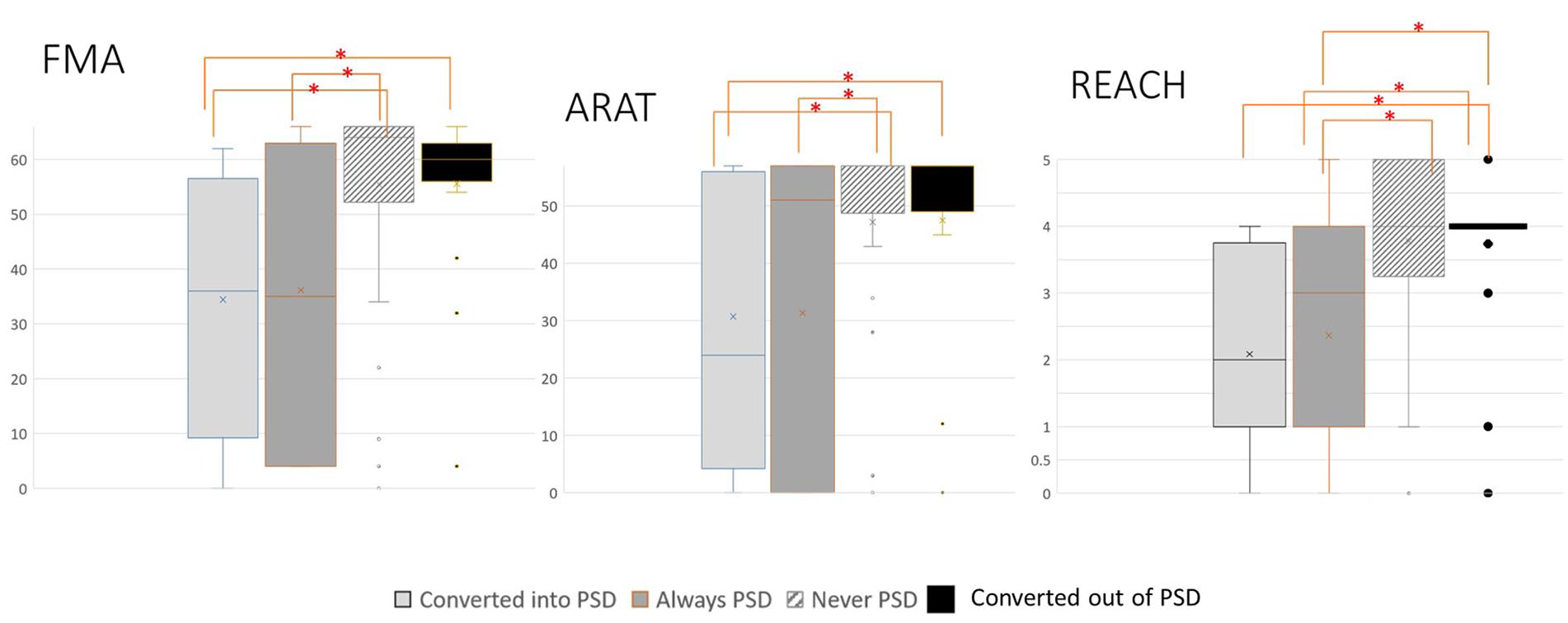
Comparison of Fugl-Meyer Motor Assessment (FMA), Action research Arm Test (ARAT), and Rating of Everyday Arm-use in the Community and Home (REACH) between 4 subgroups at T3; Participants who Converted into PSD, Always PSD, Converted Out of PSD, and Never PSD.
Discussion
Our study examined the relationship between PSD and the motor and functional ability, and daily-use of the affected UE by comparing participants with and without PSD at 3 time points post-stroke. We discuss our main findings in the context of the existing literature in the following sections.
At T1 and T2, there was no differences in UE motor impairment, functional ability, and daily-use outcomes for participants with and without PSD. A previous study of 117 participants post stroke also found no differences in BADL during hospitalization between participants with PSD compared to without PSD. 17 A possible explanation for our findings may be that all participants receiving in-patient rehabilitation were expected to follow their rehabilitation schedule, to participate in all of the therapeutic sessions and to perform BADLs independently, once possible. Therefore, the overall activity level of participants with PSD was likely to be comparable to those without PSD during in-patient rehabilitation. In addition, the intensive UE occupational and physical therapy during in-patient rehabilitation most likely contributed to continuously improvement of the affected UE, as demonstrated in previous studies.13,36
At T3, participants with PSD had significantly lower motor and functional ability of the affected UE, and less daily-use compared to participants without PSD. At 6 months post-stroke, in contrast to T1 and T2, participants were discharged home from the rehabilitation center and most were no longer receiving outpatient rehabilitation services. Nannetti et al, 17 in their study also found that participants with PSD had significantly lower motor ability compared to participants without PSD at 3 months post-stroke when participants were discharged home. Our study extends the existing literature by demonstrating that individuals with PSD also had decreased UE functional ability and daily-use compared with individuals without PSD at 6 months. The substantial drop in structured inpatient and outpatient therapy services during the transition back into the community is most likely a contributing factor to the sharp differences in UE outcome measures between the 2 groups at 6 months. Scores for all UE outcomes were lower with a large variance for the participants with PSD compared to the participants without PSD. Participants with PSD may have experienced decrease in active daily routines, and less energy to invest the extra (cognitive or physical) effort needed to use their affected UE in everyday activities, factors which have been reported to facilitate UE daily-use. 8
Since there were significant between-group differences at T3, we further categorized the participants into 4 subgroups to take into account participants with consistent PSD status and those who experienced changes in PSD status by T3. Participants who always had PSD or converted into PSD by T3 had the worst performance for all UE outcome measures compared to participants who never had PSD or converted out of PSD by T3. Participants who never had PSD or converted out of PSD demonstrated similar levels of UE functional abilities and daily use at T3. These findings signal that monitoring and addressing PSD within the first 6 months can make a difference in maximizing UE outcomes for individuals transitioning back into the community. Because the sample size of the subgroups was small and uneven, further investigation is needed in order to longitudinally examine the effect of the change in PSD status over time on UE outcomes.
Participants with PSD were also less independent in BADL and IADL and had lower cognition scores compared to participants without PSD at T3. These findings are partially supported by the existing literature. Participants with PSD at the chronic stage have been found to be overall less active and less independent in BADL.16,37 PSD was found to be a strong predictor of dependence in IADL after controlling for the following factors; independence in BADL, age, and cognition. 38 An association was reported between PSD and cognitive impairment in a sample of 106 individuals with stroke, who underwent a neurological, psychiatric, and neuropsychological examination at 3 and 12 months post stroke. 39 The fact that participants were back at home without intense therapy may explain these differences in independence in daily living. It is possible that participants were less active in their daily living, with decreased opportunities to use their affected UE, which may have led to less improvement or decline in motor and functional abilities.
Our findings extend and clarify our current understanding of the relationship of PSD on recovery after stroke. Contrary to our study hypotheses, we found that the relationship of PSD to UE outcomes is not the consistent in the first 6 months post-stroke. More specifically, while PSD is not associated with UE outcomes in the acute and subacute phase of recovery, presence of PSD is negatively associated with UE outcomes in the chronic phase. PSD is also associated with increased disability in BADLs and IADLs in the chronic phase of recovery. We believe the sharp decline in environmental supports (rehabilitation services and structured environment) associated with the chronic phase of recovery may be a contributing factor. Therefore, our findings underscore the importance of addressing depression symptoms into treatment plans particularly when individuals are transitioning back home and into the community. Therapists should guide patients and their families before discharge and during outpatient rehabilitation to be aware for changes and appearance of depression symptoms, which may appear. These symptoms might negatively impact their daily functioning and consequently the ability and use of the affected UE. Interventions during this crucial transition period should reinforce the importance of maintaining moderate level of physical activity and encourage individuals to implement a home program to be overall more active and specifically to continue practicing and using their affected UE.
Limitations
Our study had a few limitations. We did not assess individual changes in depression over time but assessed it at 3 separate time points, therefore, different participants appear in the PSD and without PSD groups at T1, T2, and T3. While we further categorized participants who changed PSD status into 2 subgroups (ie, Converted into PSD and Converted out of PSD), there were additional PSD change patterns within each subgroup that we did not account for. Because of the stated limitations of our dataset, we recommend future studies expand on our results by including a larger sample to follow-up longitudinally how changes in PSD status affect UE recovery over time. We did not collect data regarding outpatient rehabilitation services and treatment for depression, which may have impacted participant’s affected UE status and overall daily function. In addition, it may be interesting to address grief, which is a natural emotional response to a significant loss or life change, which also may be experienced post-stroke.40,41 Daily-use was assessed using a self-report measure and the presence of depressive symptoms might have impacted individual’s subjective reporting of daily-use. Future research could also use accelerometers, as an objective measure of daily hand-use in order to minimize any potential reporting bias for individuals with PSD.
Conclusions
PSD is associated with increased disability in UE motor and functional ability and daily-use particularly in the chronic phase post stroke. Our findings underscore the importance of increased attention to the impact of PSD on UE during the crucial transition period when individuals return home and integrate back into the community. The management of PSD in conjunction with continued UE rehabilitation may mitigate the potential decline in UE motor and functional ability and daily-use for individuals returning home. Further research is needed to expand on our findings and delineate the role of change in PSD status on UE outcomes over the first 6 months after stroke.
Supplemental Material
sj-sav-1-nnr-10.1177_15459683231215332 – Supplemental material for Comparison of Upper Extremity Function and Daily Use in Individuals with and without Post Stroke Depression
Supplemental material, sj-sav-1-nnr-10.1177_15459683231215332 for Comparison of Upper Extremity Function and Daily Use in Individuals with and without Post Stroke Depression by Samar Assadi Khalil, Grace J. Kim and Debbie Rand in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
We thank all the participants who agreed to participate in the study. We thank Inbar Shacham, Noa Doron, and Shelly Peri for their help with patient recruitment and skillful data collection.
Author Contributions
Samar Assadi Khalil: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; and Writing—original draft. Grace J. Kim: Conceptualization; Validation; and Writing—review & editing. Debbie Rand: Conceptualization; Investigation; Methodology; Resources; Supervision; and Writing—review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank the Steyer and Lois and Martin Whitman Families for their support (SAKh).
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.