
Abstract
Background
The impact of hand dominance on the expected (motor and functional ability and daily use) improvement of the affected upper extremity (UE) in subacute stroke has not yet been investigated.
Objectives
To compare between the affected dominant and affected nondominant UE (1) on rehabilitation admission (T1) for motor and sensory abilities, functional ability, and daily use and (2) 6 weeks poststroke onset (T2) and the UE recovery between T1 and T2 regarding percent change, improvement effect size, and percent of participants achieving minimal clinical important difference (MCID).
Methods
Multicenter longitudinal study.
Results
Thirty-eight participants with affected dominant and 51 participants with affected nondominant UE were recruited. On T1 and T2, between-group differences were not seen for all UE variables. Significant improvement in the motor and functional ability, daily use, and perceived recovery between T1 and T2 were seen for the affected dominant (z = −3.01 to −4.13, P < .01) and nondominant UEs (z = −4.59 to −5.32, P < .01). Effect size improvement values were moderate and large in the affected dominant and nondominant UE (respectively). In addition, 14% to 40% of the participants in both UEs achieved MCID.
Conclusions
Significant and similar clinical meaningfulness in UE improvement can be expected during subacute rehabilitation; however, improvement magnitude and percent improvement is different for the UE domains of the affected dominant and the affected nondominant UEs. These findings highlight the distinct roles of the dominant and nondominant hands during bimanual daily activities, which can guide clinicians during stroke rehabilitation.
Introduction
Motor impairment of the affected upper extremity (UE) is a very common symptom poststroke and even after intensive rehabilitation, the affected UE often remains nonfunctional with limited daily use. This affects the person’s ability to perform functional tasks independently 1 and reduces participation in daily function. 2
Many studies have aimed to identify factors that can predict successful UE improvement poststroke hoping that the findings can be addressed in therapy to promote successful rehabilitation. Initial UE motor and sensory impairments, for example, have been consistently identified as being strongly associated with UE improvement following stroke. 3 Cognitive impairments, which often coexist in individuals with stroke, and specifically executive function and attention deficits, have also found to be associated with UE improvement poststroke. 4 Hand dominance of the affected UE may also affect functional improvement poststroke.
In healthy right-handed individuals, the (right) dominant hand has superior hand function, motor performance and coordination compared with the (left) nondominant hand. 5 The norms of grip strength 6 and dexterity7,8 also demonstrate clear differences between UEs, which are better in the dominant versus nondominant UE. The use of both hands is essential for performing bimanual activities, such as opening a jar or wrapping a gift, accounting for most activities of daily living. Therefore, it is surprising to see that differences in amount of daily use have been demonstrated between hands showing more use of the dominant UE than the nondominant UE in varied daily activities. 9 In healthy older adults, 10 a significant interaction effect was found between hand use (dominant vs nondominant) and sex; women used their dominant hand more than men used their dominant hand, as was measured by wrist accelerometers worn for a week. However, it is unclear if these differences apply to individuals with stroke and if functional improvement of the affected UE poststroke is influenced by hand dominance.
Despite the relevance to rehabilitation, interestingly, not many studies have researched handedness or motor lateralization in stroke. Sainburg 11 developed and ran different reaching lab experiments to assess the dynamic dominance hypothesis in stroke but specially focused on the ipsilateral (less-affected) hand. Hand dominance has been assessed in other studies, but most of them being cross-sectional. For example, hand dominance was not found to be associated with daily use of the affected UE in 60 participants with subacute stroke 12 and 32 participants 12 months poststroke. 1 However, in both studies improvement of the sensomotor or functional abilities was not compared between participants with an affected dominant versus affected nondominant UE. Harris and Eng 13 who researched the impact of hand dominance on the affected UE in individuals with chronic stroke, found that motor ability of the affected nondominant UE was more impaired compared with the affected dominant UE.
Differences in improvement over time was demonstrated in one study following bilateral arm training in individuals with chronic stroke comparing side of brain lesion (not specifically hand dominance). Improved affected UE function was reported only for individuals with left hemispheric lesions compared with individuals with right hemispheric lesions. 14
The smallest difference (improvement) that patients perceive as beneficial, termed minimal clinically important difference (MCID) 15 has been found to be smaller in the affected dominant UE compared with the affected nondominant UE for grip strength and hand function poststroke. 16 In other words, more improvement is needed in the affected nondominant UE for the patient himself to notice it. Perhaps this is due to the importance of the dominant UE.
Therefore, the aim of this longitudinal study was to understand the impact of hand dominance on the improvement of the affected UE during the subacute stage poststroke. This understanding is important for defining accurate therapeutic goals and planning intervention to improve function and daily use of the affected UE. Specifically, we aimed to compare the differences between the affected dominant to the affected nondominant UEs (1) on rehabilitation admission (T1) in terms of motor and sensory abilities, functional ability, and daily-use and (2) 6-weeks poststroke onset (T2) and the UE recovery between T1 to T2 regarding percent change, improvement effect size, and percent of participants achieving MCID of the UE motor and functional abilities and daily use.
Methods
Study Design
This is a multicenter longitudinal study. Data were collected from 4 rehabilitation centers on rehabilitation admission (T1) and 6 weeks following stroke onset (T2). During the study, participants received the usual rehabilitation treatments, which are similar in all 4 centers.
Study Population
We included adults who were admitted to stroke rehabilitation and met the following inclusion criteria: (1) up to 4 weeks post a stroke (determined by computed tomography or magnetic resonance imaging), (2) full UE function prior the stroke, (3) Understand simple commands and could cooperate, (4) intact or corrected vision and hearing, and (5) without neurological or orthopedic conditions other than stroke.
Patients who agreed to participate provided written informed consent.
Tools
The following clinical assessments were administered to assess motor and sensory ability, functional ability, daily use of the affected UE.
Motor Ability
The Fugl-Meyer Motor Assessment–upper extremity subtest (FMA) 17 is a valid and reliable tool 18 to assess the motor impairment poststroke. Score ranges from 0 (no active movement) to 66 points (full active movement). The motor impairment was also assessed by the Shoulder Subluxation Test. 19 Participants sat on the edge of bed with their affected UE hanging freely and the examiners used their thumb to palpate the separation between the acromion and the head of the humerus. This was scored as none (0), minimal (1) or substantial (2). The Jamar Dynamometer 20 was used to assess grip strength of the affected UE by calculating an average of 3 trials in kilograms.
Sensory Ability
The Thumb Localization Test (TLT)21,22 was used for assessing proprioception. The participants’ eyes are closed and the affected UE is moved by the examiner to 4 different locations in space and each time they are asked to find and grasp their affected thumb with the less-affected UE. The final score is determined by the worst performance of the 4 locations ranging from 0 (intact proprioception) to 3 points (severe proprioception deficit). To assess touch localization, the examiner lightly touched the participants’ fingertips and palm in 6 set locations while their eyes were closed. Participants were asked to point with their less-affected hand where they were touched. This was scored as normal (5-6/6), partial (3-4/6), or impaired (0-2/6) touch localization. Stereognosis was assessed by placing the following 3 objects (1 at a time) in the participants’ palm while their eyes were closed: fork, toothbrush, and key. The score was determined by number of objects correctly identified (0-3) and the total time to identify all 3 objects in seconds was recorded.
Functional Ability
The Box and Block Test (BBT) 7 is valid and reliable to assess manual dexterity, 23 an important component of hand function. Participants are requested to move blocks from one side of a box, over a divider to the other side, one block at a time. The number of blocks transferred in 1 minute was recorded.
The Action Research Arm Test (ARAT) 24 is a valid and reliable test to assess the functional ability of the UE. This test includes grasping, pinching, and lifting objects of various sizes. Score ranges from 0 (a nonfunctional UE) to 57 points (a fully functional UE).
Daily Use
The Rating of Everyday Arm Use in the Community and Home (REACH) 25 is a valid and reliable self-report measure, which captures how the affected UE is used outside of the clinical setting. Scores (levels) range from 0 (no use/exercise only) to 5 (full use). The test consists of 2 different versions based on the typical use for the affected dominant and nondominant UE.
In addition, participants were asked to rate the perceived recovery of the affected UE since stroke onset (0%-100%). This question was derived from the Stroke Impact Scale (SIS). 26
The study population was also described in terms of cognitive function, using the Mini-Mental State Examination (MMSE), 27 which includes orientation, attention, memory, language and visual-spatial skills, score range from 0 to 30 points. The presence of Unilateral Spatial Neglect (USN) was screened using a cutoff score of less than 44/54 stars on the Star Cancellation subtest from the Behavioral Inattention Test (BIT). 28 Independence in basic activities of daily living (BADL) was assessed using the Functional Independence Measure (FIM). 29 The FIM total score was taken from the patient’s medical file, it ranges from 18 to 126 points, higher scores indicate more independence. In addition, demographic and stroke information regarding the date, type and side of the stroke (taken from medical file), hand dominance (based on self-report) and functional ability in BADL prior the stroke (full/partial independence).
Procedure
Prior to the study, assessors underwent specific training to verify that they administer and score the clinical assessments in the same manner. Eligible patients were approached within the first week of rehabilitation and provided an explanation regarding the study. On T1 and T2, clinical assessments, which took approximately 1 hour to administer, were administered by experienced occupational therapists. If on T2 participants were already discharged, a home visit was conducted to administer the assessments. All clinical assessments were administered on T1 and T2 but only the following assessments were analyzed on T2: FMA, ARAT, BBT, grip strength, perceived recovery, and REACH.
For data analysis, based on self-report, participants were divided into 2 groups according to dominance or nondominance of their affected UE.
Statistical Analysis
Descriptive statistics were used to describe the affected UE on T1 and T2 of participants with an affected dominant and nondominant UEs in terms of demographic, stroke information, cognition, and independence in daily activities. Since variables of the affected UE did not distribute normally, data are presented as median and interquartile range (IQR) and nonparametric tests were conducted.
Differences between groups on T1 and T2 were tested by Mann-Whitney U test for continuous variables and chi-square test for the qualitative variables. To describe the improvement over time of the affected dominant and nondominant UEs, Wilcoxon signed-rank test was used. Percent change of the affected UE in each group between T1 to T2 was calculated [{(T2 − T1)/T1} × 100]. To examine the magnitude of the changes for UE in each group, the improvement effect size (for Wilcoxon signed-rank test) was calculated (r = z/√n). 30 Effect size was considered as large if r was more than 0.5, moderate or small effect size were considered if r was 0.3 and 0.1, respectively. 31 In addition, the percent of participants in each group who achieved MCID in the UE variables was calculated.
Results
Data were collected between January 2017 and March 2019, during this time 89 participants were eligible and agreed to participate in the study. Their median (IQR) age was 73.0 (66.0-81.5) years, most of them (87.6%) were independent in BADL prior the stroke and the majority (88.7%) of them had an ischemic stroke. Thirty-eight (42%) participants had an affected dominant UE and 51 (57%) participants had an affected nondominant UE. Participants with an affected dominant versus nondominant UE did not differ significantly regarding the demographic, stroke information, or functional status (see Table 1).
Characteristics on Admission (T1) of the Participants With an Affected Dominant and Affected Nondominant Upper Extremity (UE).
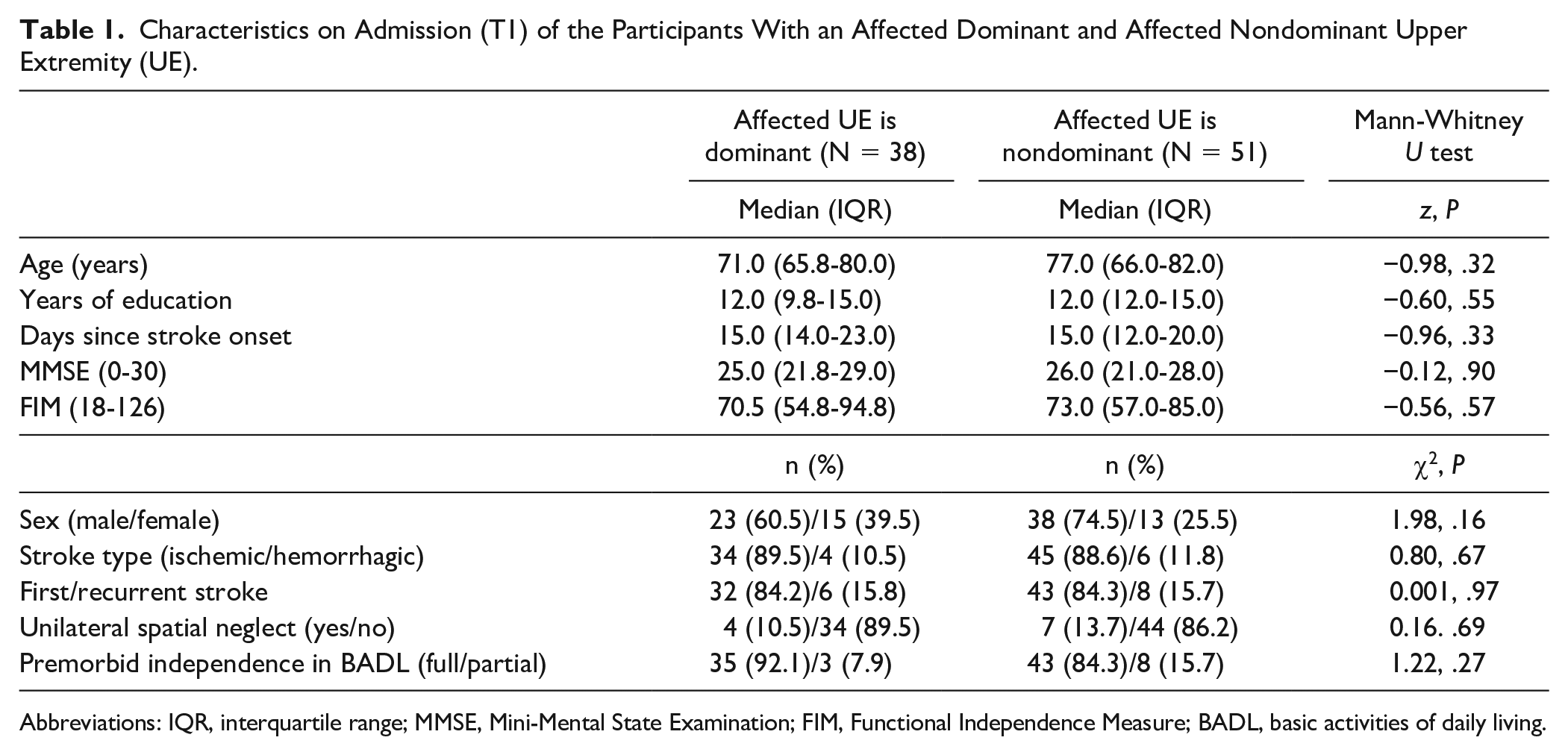
Abbreviations: IQR, interquartile range; MMSE, Mini-Mental State Examination; FIM, Functional Independence Measure; BADL, basic activities of daily living.
On T1, the affected dominant and nondominant UEs presented a wide range of motor and functional abilities, ranging from no movement and function to full active movement and function, however the median assessment scores are relatively high (FMA 45-48/66, ARAT 43-49/57 points) (see Table 2). Accordingly, most participants (87% for the affected dominant vs 80% for the nondominant) had no palpable shoulder subluxation. The majority of the participants in each group were able to successfully identify 3 objects with their eyes closed (stereognosis), in a median (IQR) 8.0 (6.5-12.0) seconds for the affected dominant and 10.0 (6.0-17.0) seconds for the affected nondominant UE. In addition, approximately 60% and 20% of the participants in each group demonstrated intact and a mild proprioception deficit (respectively). See Table 2 for all the clinical measures.
The Median (IQR) of the Affected Dominant and Nondominant Upper Extremity (UE) on T1 and Differences Between Groups.
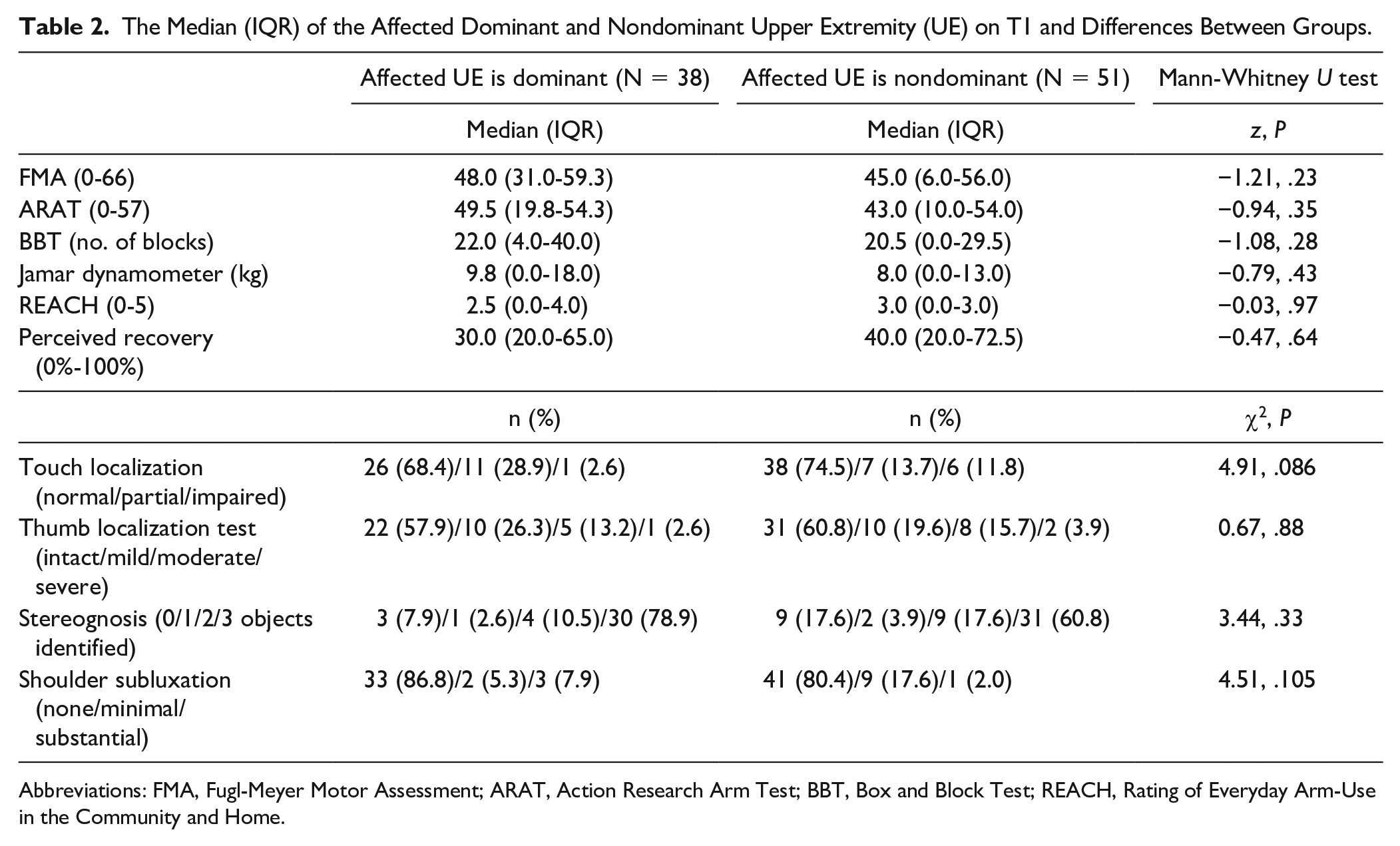
Abbreviations: FMA, Fugl-Meyer Motor Assessment; ARAT, Action Research Arm Test; BBT, Box and Block Test; REACH, Rating of Everyday Arm-Use in the Community and Home.
On T1, despite the fact that scores look higher for the dominant UE, no significant differences were found for the motor, sensory, and functional abilities of the affected dominant compared with the affected nondominant UE (z = −0.03 to −1.21, P > .05) (see Table 2).
Also on T2, no significant differences between the affected dominant and non-dominant UEs were seen for all UE variables (z = 0.00 to −1.24, P > .05).
The affected dominant (z = −3.01 to −4.13, P < .01) and affected nondominant UEs (z = −4.59 to −5.32, P < .01) improved significantly between T1 and T2 for all UE variables.
For the affected dominant UE, 31.3% improvement was seen for dexterity (BBT) then for daily use (REACH 10.0%), motor ability (FMA 9.1%) and then for grip strength (Jamar dynamometer 4.7%) and functional ability (ARAT 3.6%). While in the affected nondominant UE, 41.0% improvement was found for grip strength, then for daily use (REACH 25.0%), dexterity (BBT 22.7%), motor ability (FMA 10.9%), and only 5.6% for functional ability (ARAT).
Improvement effect size values were mainly moderate (−0.37 to −0.50) for the affected dominant and mostly large (−0.46 to −0.53) for the affected nondominant UE (see Table 3).
The Median (IQR) of the Affected Dominant and Nondominant Upper Extremity (UE) on T1 and T2, Percent Change, and Effect Size.
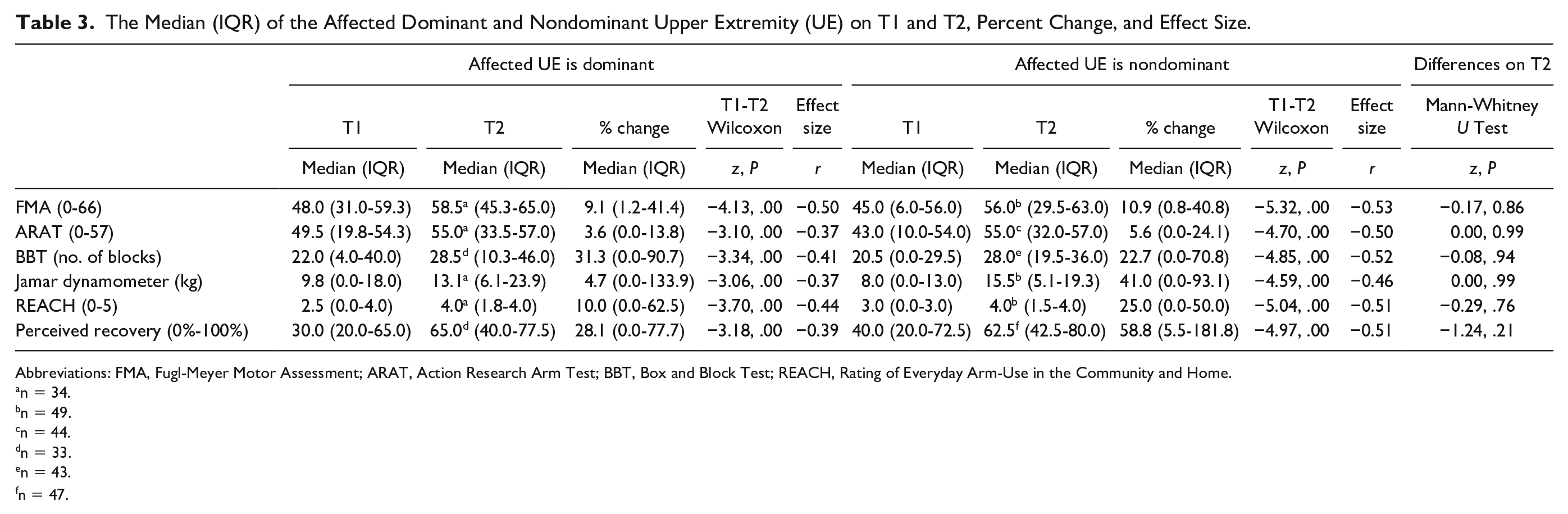
Abbreviations: FMA, Fugl-Meyer Motor Assessment; ARAT, Action Research Arm Test; BBT, Box and Block Test; REACH, Rating of Everyday Arm-Use in the Community and Home.
n = 34.
n = 49.
n = 44.
n = 33.
n = 43.
n = 47.
A total of 41%, 14%, and 29% of the participants with an affected dominant UE achieved MCID for FMA, ARAT, and grip strength (respectively) while 32%, 14%, and 29% of the participants with an affected nondominant UE achieved MCID for these assessments.
Discussion
Most daily functional tasks require the use of both UEs 32 and while fulfilling these bimanual tasks, the dominant and nondominant UEs have unique and complementary roles. The dominant UE, which has superior speed and strength, is used for tasks such as slicing bread with a knife or peeling a cucumber, where movement is efficient and trajectories are precise. 33 The nondominant UE is used for controlling the static posture 32 during the task, for stabilizing the loaf of bread or holding the cucumber. Therefore, our study aimed to investigate the impact of hand dominance on improvement of the affected UE in subacute stroke. Understanding the impact of hand dominance on functional ability and daily use improvement of the affected UE poststroke is important, leading to more accurate therapeutic goals and therapy planning.
On rehabilitation admission, due to our lenient inclusion criteria, the affected UE of our cohort demonstrated a wide range from no active movement or functional ability and daily hand use to nearly full movement and use (FMA 6-59/66, ARAT 10-54/57, BBT 0-40 blocks in 1 minute, REACH 0-4/5). Despite this wide range, overall, the affected UE of our participants was relatively high functioning compared with the samples described in previous studies during subacute stroke.12,34,35 For example, the median FMA of our cohort was 46 points compared with 40 points 12 and 30/66 points 35 in previous studies, the median ARAT was 45 points compared with 32 12 and 20/57 35 points and the median BBT was 21 blocks compared with 12 blocks 34 in a previous study.
When the cohort was divided into 2 groups, the median scores for the motor and sensory abilities and functional ability of the affected dominant UE were not statistically significant different than the affected nondominant UE. These findings support previous studies of 22 participants with subacute stroke 36 and 93 participants with chronic stroke. 13
Significant improvements between T1 and T2 were seen in motor and functional ability, daily use, and perceived recovery in both affected UEs. This finding is in contrast with the improvement seen in a small sample of individuals with chronic stroke following 6 weeks of repetitive bilateral arm training reporting a significant improvement in the functional ability (Wolf Motor Function Test) only for the affected dominant UE, while both hands showed significant improvements in the motor ability (FMA). 14 Possibly the affected dominant and non-dominant UEs of our cohort improved in all measures due to the spontaneous recovery that occurs at the subacute stage 37 and the fact that all participants received inpatient rehabilitation.
The percent improvement in the different UE domains varied completely in the affected dominant compared with the nondominant UEs. Interestingly, in affected dominant UE the highest median percent improvement was in dexterity (31.3%) and the lowest of only 4.7% improvement was found for grip strength. However, in the affected nondominant UE, the highest median percent improvement was seen for grip strength (41.0%). These differences in the improvement might be linked to the unique roles of each UE in daily function. Perhaps the need for more dexterity in the dominant UE and more strength for stabilization in the nondominant UE led to these changes. Possibly these abilities were practiced during rehabilitation, in or out of therapy sessions. Due to these distinct roles, perhaps participants were more critical regarding affected dominant UE improvement, rating the recovery by only 28% versus 58.8% improvement rated by participants with an affected nondominant UE. Perceived improvement and its impact on daily use of the affected UE post stroke should be further researched.
Values of effect size for the UE improvement, which is a quantitative measure of the magnitude of change, 30 were found to be large for most domains of the affected non-dominant UE and moderate for the affected dominant UE. This interesting finding may be due to the slightly lower scores of the affected nondominant UE on T1 compared with the affected dominant UE, which allowed for more improvement during rehabilitation and due to the ceiling effect for tools used to evaluate the improvement over time (eg, FMA, ARAT), leaving less room for the affected dominant UE to improve.
The percent of participants who achieved a MCID in the affected dominant was calculated and compared with the nondominant UE for measures that have previously reported it. MCID for grip strength (5.0 kg for the dominant UE and 6.2 kg for the nondominant UE) and for the ARAT (12 points for the dominant UE and 17 points for the nondominant UE) have been established for each hand. 16 Based on these values the improvement seen between T1 and T2 was considered clinically meaningful (MCID) for a similar percent of participants with an affected dominant and affected nondominant UEs for grip strength and ARAT. However, differences in the percent of participants in each group achieving a MCID improvement in the motor ability was found. Fourteen of 34 (41.2%) participants with an affected dominant UE versus 16/49 (32.7%) participants with an affected nondominant UE demonstrated MCID for the FMA (which is 10 points 38 ). However, since the MCID for the FMA was not established separately for the dominant and nondominant UEs, this value might be less accurate to point out differences between UEs.
Study Limitations
This study has several limitations. Our cohort was divided into 2 groups based on self-report of hand dominance. Adding a tool to verify this (such as the Edinburgh Handedness Inventory 39 ) might have been more accurate. In addition, T1 differed slightly in terms of days poststroke onset but was close to rehabilitation admission for all participants and no differences were found between groups. Since T2 was 6 weeks post–stroke onset, the time between T1 to T2 slightly varied between participants. Hand dominance was not confined to the right hand and 3 of the 89 participants (2 participants with affected dominant and 1 participant with affected nondominant UE) had left-hand dominance, while UE improvement for these participants may be different from right-hand dominance participants. Since very few participants experienced unilateral spatial neglect, aphasia or apraxia, we do not know how these variables interplay with hand dominance.
Conclusions
Significant and similar clinical meaningfulness in UE improvement can be expected during subacute rehabilitation; however, improvement magnitude and percent improvement is different for the UE domains of the affected dominant and the affected nondominant UEs. These findings highlight the distinct roles of the dominant and nondominant hands during bimanual daily activities, which can guide clinicians during stroke rehabilitation.
Footnotes
Acknowledgements
We thank Noa Doron and Shelly Perry for their help with recruitment and skillful data collection. We thank the Steyer Family for their support (SHA). We thank all the participants who agreed to participate in the study.
Authors’ Note
This work was performed in partial fulfillment of the requirements for a PhD degree of Samar Hmaied Assadi, Sackler Faculty of Medicine, Tel Aviv University, Israel
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the Elsa and Leo Avramson research fund (DR and ID) for financial support for the research.