
Abstract
Despite the substantial progress in motor rehabilitation, patient involvement and motivation remain major challenges. They are typically addressed with communicational and environmental strategies, as well as with improved goal-setting procedures. Here we suggest a new research direction and framework involving Neuroeconomics principles to investigate the role of Motor Decision-Making (MDM) parameters in motivational component and motor performance in rehabilitation. We argue that investigating NE principles could bring new approaches aimed at increasing active patient engagement in the rehabilitation process by introducing more movement choice, and adapting existing goal-setting procedures. We discuss possible MDM implementation strategies and illustrate possible research directions using examples of stroke and psychiatric disorders.
Keywords
Introduction
The main goal of motor rehabilitation is to restore normal real-life functioning. Motor rehabilitation techniques have been developing generally from passive and reflexive approaches, such as Brunnstrom movement therapy and proprioceptive neuromuscular facilitation towards approaches with more active patient participation like goal-oriented movement,1,2 arm ability training, 3 and constraint-induced therapy. 4 Regardless of the progress achieved in the field, still the success of motor rehabilitation, for instance after stroke, is far from satisfactory. As it was recently shown, one of the major factors to achieve clinically meaningful changes even in chronic stroke patients is intensive program with long hours of the motor rehabilitation activities per day, 5 comparable with training time spent by professional athletes. To achieve these long hours of motor rehabilitation, especially after a hospitalization period, patient involvement and motivation come as the major issues. 6 Here we argue that it may be possible to increase active patient participation in the rehabilitation process by introducing more movement choice, and by adapting existing goal-setting procedures using neuroeconomics (NE) approaches. In this Point of View paper, we suggest possible directions for future research in the field of neurorehabilitation based on NE principles. Currently, Motor Decision-Making is actively studied in healthy individuals,7,8 justifying the importance of NE principles for motor control. DM and motor recovery are linked to the same brain areas9-11 and neurochemical systems. 12 Moreover, there are first promising findings suggesting the relatedness of DM to motor impairment. 13 Thus, we argue that it is timely to further develop this line of research by investigating the role of the MDM parameters in motor impairment with an idea to adapt existing NE approaches to neurorehabilitation, aiming primarily to increase patient motivation, possibly leading to an increased number of movements performed, but also at making every movement more engaging.
The Problem
Lately, the aspect of motivation for motor rehabilitation attracts more attention. One recent study provides the results of a survey where health care professionals listed their common strategies to increase patient’s motivation. 14
According to the results, rehabilitation specialists strongly rely on their communicational skills, since the most common approaches were active listening, praising, and enjoyable communication. In addition to undeniably important good social skills and welcoming rehabilitation environment, we suggest that revisioning the motor task structure might also be crucial for motivational aspects. Rehabilitation approaches are becoming more personalized, and some branches of rehabilitation, like occupational therapy (OT) are specifically dedicated to train complex tasks related to patient personal needs and current functional motor status. However, movement/goal choice definition remains a challenging topic, and patient NE profile may add specificity to the goals and training environment. Moreover, in many cases, including most of the available gamified motor rehabilitation approaches, tasks are designed in a way that while playing a game patients should deal with a single goal (e.g., reach, grasp or avoid it, etc.), and the goal choice is fixed. We believe that the motivation for motor rehabilitation can be increased by providing patients with the possibility to choose from various goals in the rehabilitation framework and by considering individual characteristics known to modulate decision-making (DM) when adjusting these goals. Acknowledging that any action is a choice, many parameters influencing it have been extensively investigated in healthy subjects in the last decade in the field that is currently referred to as motor decision-making (MDM).8,15,16 We think that it is time to discuss in more detail how this framework can be applied to patients with motor impairment. The aim of this article is to call for more interdisciplinarity in motor rehabilitation research by integrating the neuroscience of DM (aka NE) into it. We suggest that the presence of a goal choice and an acknowledgement of a patient's MDM profile may be the next step towards increasing patients’ motivation and participation in a rehabilitation process. To justify our opinion, we briefly outline the DM principles applied to MDM investigation in healthy subjects, which, we suggest, may be transferred to motor rehabilitation research. Then we illustrate possible directions for research in the field of neurorehabilitation implying NE principles using examples of motor impairment due to stroke and psychiatric illnesses.
Neuroeconomics Approaches to Motor Control Assessment
Motor decision-making (MDM) represents a combination of perceptual and value-based processes, which have been extensively studied in healthy subjects during the last decade.7,17-22 Value-based decision processes have received a lot of attention in the field of NE, which provides a set of methods to assess individual preference characteristics. 23 It has already been shown that understanding these individual preferences can be used to enhance existing models of motor control (MDM).8,18,19 MDM can be represented using a fundamental NE principle of utility maximization, where utility is a concept used to describe behavior in value-based choice tasks (for dictionary see Table 1). It represents an ordering of available alternatives in terms of their preference. Any DM task can be conceptualized through the maximization of utility, meaning choosing an option that maximizes the reward given specific constraints. 24 In MDM, the maximization of utility means reward maximization under time and energy constraints. 25 Some researchers consider that a concept related to utility in MDM is “vigor”—the speed of a movement and is suggested to be proportional to the reward in healthy individuals. 15 It was suggested that the vigor of movements may serve as a continuous proxy for the utility of movement goals. Both vigor and utility have been linked to the motivation to pursue a specific activity.26,27
Neuroeconomics Terms Used in the Paper.
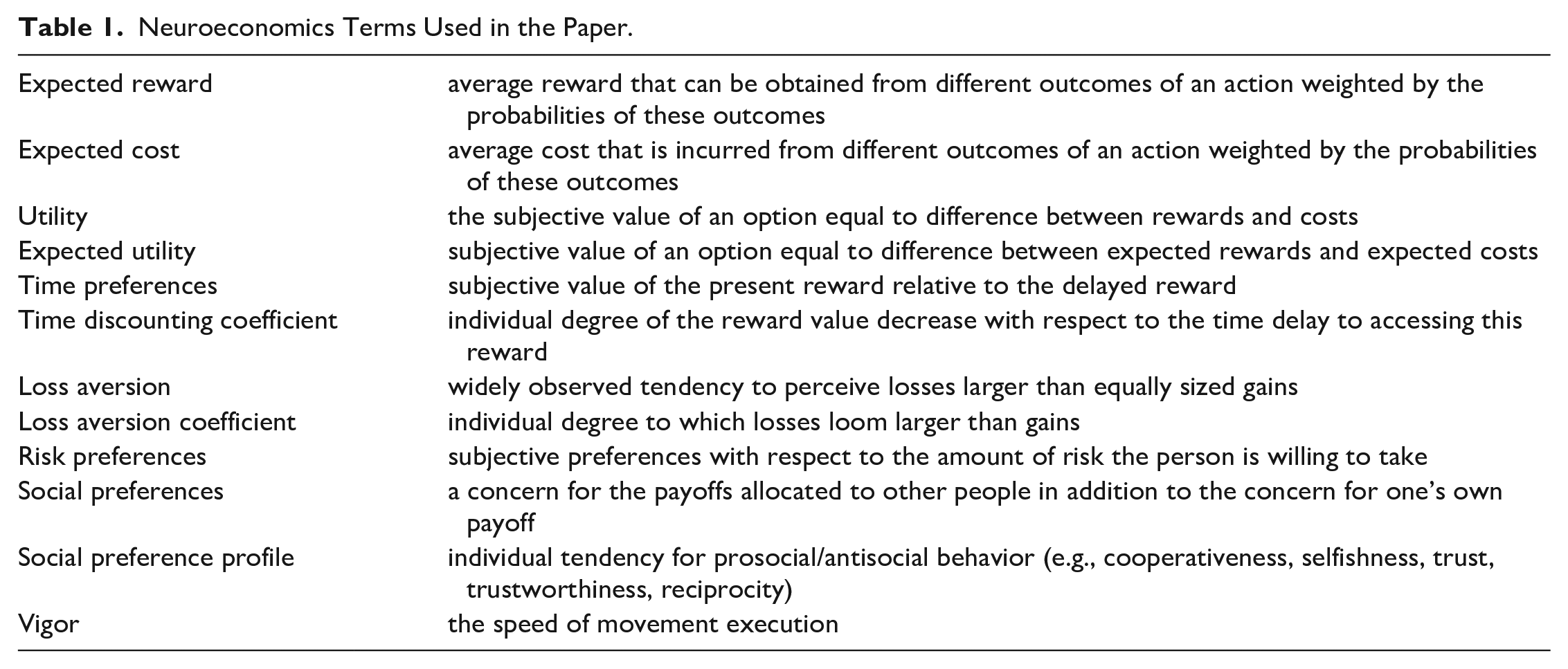
The principle of utility maximization implies that an individual chooses an option that delivers the highest difference between potential reward and the costs of obtaining it. The subjective value of reward may differ from one person to another. For example, individuals may exhibit different sensitivity to reward depending on their personal characteristics, external circumstances, and reward type. A thirsty person would attach a very high value to the first bottle of water, but after one bottle has been consumed, the further bottles will not be valued as highly. However, the speed with which the value of an additional reward unit would decrease may vary among individuals. The costs of obtaining a reward may include not only the cost of physical effort, but also emotional losses if the goal is not reached. Since rewards and costs are often obtained with less than 100% probability, the terms “expected reward,” “expected costs” and “expected utility” are used to describe the choice.
The principle of utility maximization may explain stroke patients’ reluctance to use their affected limbs in their “daily life tasks.” Consider an individual with a hemiparesis choosing which arm to use to reach for a cup of coffee (Figure 1). The chances to successfully picking up the cup are lower for the affected limb compared to the unaffected one. Performing an action with an affected limb also gives a rise to various kinds of costs. For example, a patient may have to exert higher physical and mental efforts to focus and to perform the movement. Employing the affected limb will also take longer time to reach the goal, increasing the temporal costs. Additionally, if the cup breaks, it will lead to material (cost of the cup) and emotional losses due to the negative outcome. As a result, the utility of using an affected limb will be lower compared to the unaffected one, making the choice of the affected limb suboptimal.
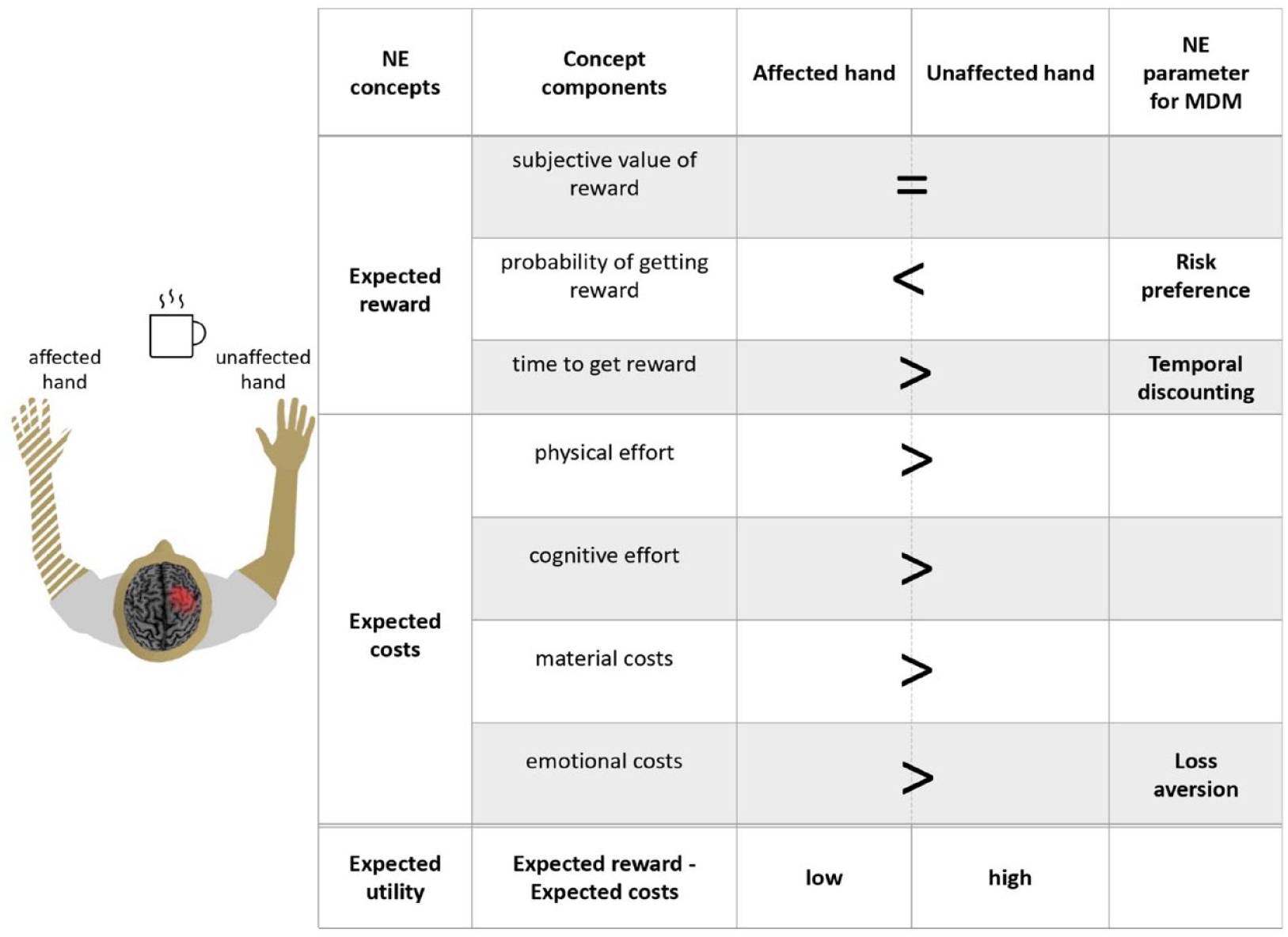
An example of a stroke patient deciding which hand to use to reach the cup of coffee. Performing an action with an affected limb is associated with lower expected rewards and higher expected costs resulting in a lower expected utility compared to the unaffected limb. The term “expected” means that the rewards/costs may be realized with less than 100% probability. All mentioned components are subjectively estimated by the patient. The chances to successfully pick up the cup are lower for the affected limb compared to the unaffected one. The signs >, < and = indicate whether a given feature is more/less or equally pronounced for the affected/unaffected hand.
Thus, to stimulate individuals with hemiparesis to use their affected limb, the cost/benefit ratio of the motor task needs to be deliberately improved in a way that even high-cost movements of the affected limb will be associated with high reward in a neurorehabilitation framework. This idea is already used in many existing rehabilitation techniques, where an effort is rewarded by points in a rehabilitation game. However, how much the affected limb movement associated with additional costs should be rewarded for an optimal performance in a concrete patient in a concrete task remains a challenging question. Some of the mentioned components of this utility, for example, physical effort, can be already measured in a neurorehabilitation framework, 28 while for measuring other components, e.g., subjective value of reward or individual tolerance to losses, neuroeconomic assessment tools may be very useful.23,29
Below we briefly outline the parameters of the NE profile, highlighting them as possible factors deserving separate investigation in the field of motor rehabilitation. Specifically, we will offer a more detailed description of the three domains important for utility function maximization: (1) risky choice (risk/loss aversion) (2) intertemporal choice (time discounting), and (3) social choice (tendency towards cooperative/selfish behavior) (see Figure 2). Additionally, we provide a dictionary with the used neuroeconomic terms (Table 1).
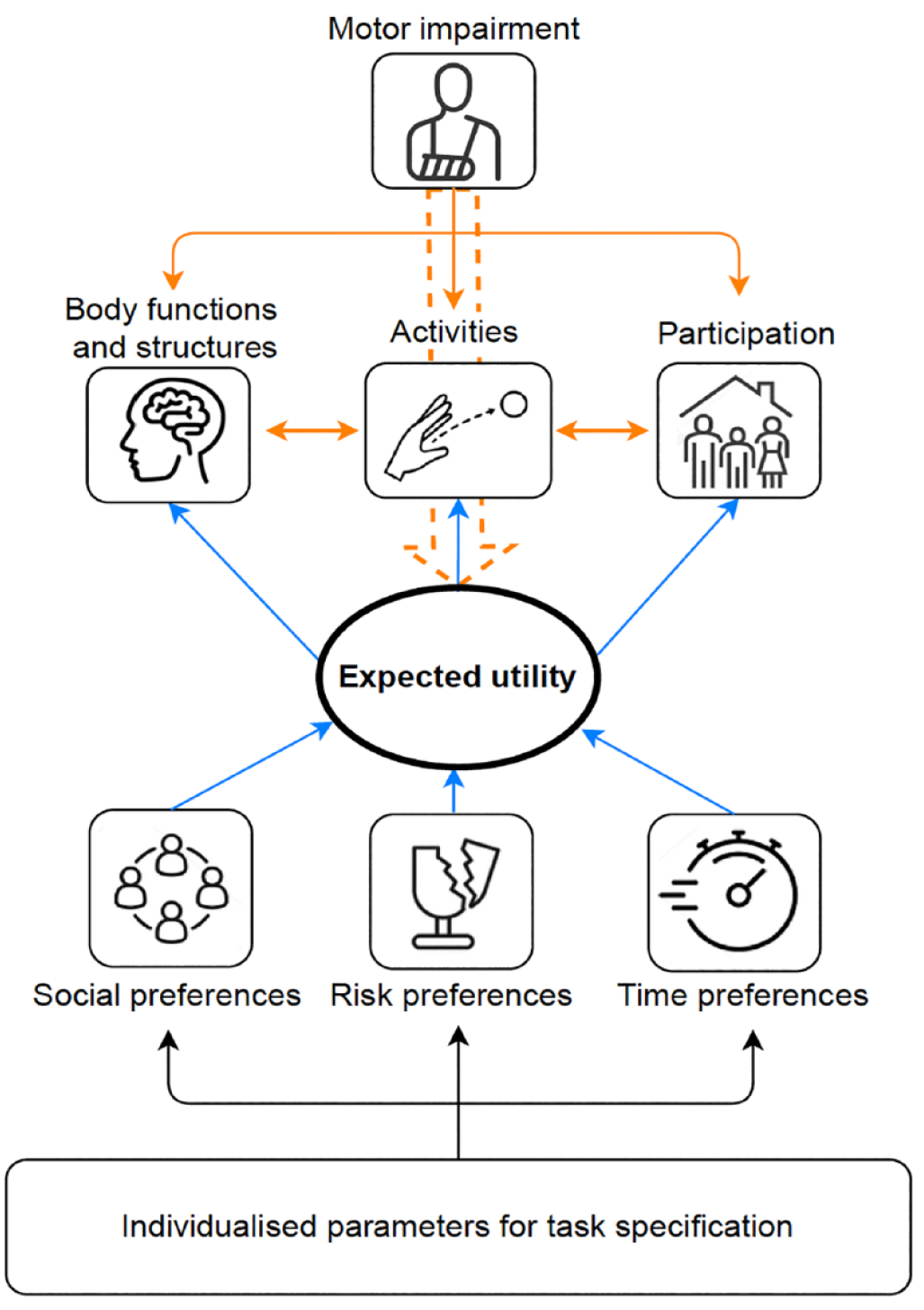
Neuroeconomics (NE) parameters in MDM studies. Orange arrows—negative effects of motor impairment on health-related indicators of functioning (from the WHO (2001) ICF classification), blue arrows—possible compensatory effect of NE parameters implementation. In patients with motor impairment expected utility of the affected limb is decreased, NE parameters implementation in rehabilitation techniques might normalize expected utility, hence helping to restore spontaneous use of the affected limb.
Choice Under Risk and Uncertainty
The success of a movement is often not guaranteed; thus, motor decisions are usually made under uncertainty. The economic concept of expected utility allows agents to compare and choose among different options, bringing the rewards with less than 100% probability. Motor uncertainty is conceptualized as the variability of movement endpoints in a given environment under time constraints. The optimal choice is the movement trajectory that minimizes the costs and maximizes the expected value.30-33 Both classical economic theory and its prospect theory adaptations 34 assume that people differ in their tolerance to risk, their propensity to avoid losses and their optimism in probability perception. These individual differences help to explain and predict the variation in risky behavior among people. Recent NE studies suggest various experimental techniques for measuring these components of individual preferences under risk.23,35
The adaptation of classical theory of choice, i.e., Prospect Theory, postulates that one derives utility not only from the current state itself but also from the changes occurring to its state relative to some reference point. For example, a person may experience positive emotions if they are offered an unexpected pay rise, but they may also experience a sense of loss if this rise happens to be below the expectations. The same principle may also be relevant for MDM in the rehabilitation framework. We suggest that individual risk preference profile (tolerance to risk) also affects MDM in patients with motor impairment. Recently it has been shown that loss aversion is a factor that influences effort-based decision-making. 36 The study shows that healthy individuals and patients with Parkinson's disease have different profiles of loss aversion. While these results are not readily transferable to other patient groups, they highlight the potential importance of assessing loss aversion as an important MDM factor in patients with motor impairments, such as patients with motor stroke.
For example, stroke patients with hemiparesis execute movements under great uncertainty: they do not know if they will successfully grasp a cup of coffee or spill the coffee and break the cup. Therefore, the decision to move is influenced by a possible gain (drinking coffee), a possible loss (breaking a cup), and the estimated probabilities attached to these outcomes. Losses have a significantly more powerful psychological effect on decision-making than gains, as it was formulated in the Prospect Theory. 34 Importantly, individual sensitivity to losses is experimentally testable using NE tools. For example, to measure individual loss aversion, a participant may be offered a list of binary choice questions where one option represents a sure gain while an alternative represents a lottery with a possible larger gain and a loss. Varying the amount of loss in the second option and observing at what point a sure gain would become more preferable, allows one to measure individual tolerance to losses. We suggest that neurorehabilitation tasks for a particular patient may be also adjusted considering their individual loss-aversion coefficient. So, the rewards offered for a successful movement may override the negative effects of loss aversion stimulating the affected limb use.
Moreover, we hypothesize that the well-known problem of the learned non-use (LNU) after a stroke may be in part explained by loss aversion. We suppose that a low-loss environment may be especially beneficial for some patients with a high degree of loss aversion. In line with this, we also hypothesize that the lack of negative feedback is playing a role in such common practices in physical therapy as performing a movement with closed eyes or hiding real visual feedback from the affected limb during mirror therapy.37,38 Supposedly, a low loss environment achieved either with goal setting and/or the lack of negative feedback might augment the utility of using an affected limb and increase the motivation for a rehabilitation program.
Intertemporal Choice
Performing an action takes time. The majority of the rewards are also not available immediately. Economic theory suggests that the utility of a reward decreases with the time needed to obtain it (time discounting), while the discount factor is individual (please see Table 1). It was shown that the time discounting coefficient also affects the speed of a movement: if a reward is very distant in time, a high discount rate will make it less valuable and may decrease the vigor of the movement towards the goal associated with it. 25 Several papers have discussed the relationship between the temporal discounting factor and the perception of effort.39-41 Recently it was reported that postponed reward presentation decreases motor learning efficiency in healthy individuals, 42 confirming the importance of temporal domain for MDM even for a short time (millisecond) range. We suggest that reward temporal discounting may serve as a component in temporal costs associated with an impaired limb use. Let’s consider again the example of an individual choosing between the affected and unaffected limbs to reach for a glass of water. If an affected arm is used, the movement will be slower and, hence, the reward will be obtained at a later time point, which reduces its value in accordance with the individual temporal discounting factor, and as a result, reduces the utility of using the affected limb.
It has already been shown that time discounts the reward following а hyperbolic function both in cognitive and motor decision domains.43,44 In a typical NE delay discounting task, the delay is manipulated until it becomes as likely for a subject to choose a small reward as a large reward. We suggest that by assessing individual discounting factors in the motor domain one may also investigate the effects of manipulating goal parameters for a motor task in a rehabilitation framework (e.g., difficulty, reward presentation time and reward magnitude) at a personalized level.
Social Choice
Decisions are often made in situations implying social interactions where the decisions of one person affect the outcomes of others. Social context may have a significant impact on choices in various tasks. For example, participants involved in a social context while solving a cognitive Balloon Analogue Risk Task, demonstrated a higher preference for risk in either cooperation or competition conditions, compared to participants who performed the task individually. 45 It has also been shown that risk-taking tendency is augmented with an increased number of competitors in an all-pay auction condition (when the prize is assigned to the player with the best performance). 46 A similar idea of incorporating the social interaction context has recently been applied to the motor domain, suggesting that one way to optimize MDM may be through competition with an opponent. 47 When playing a competitive reaching game with opponents, risk-taking subjects switched from more risk-taking to a more risk-averse behavior in such a way optimizing their DM strategy. Recently, the effects of observation, cooperation and competition in MDM have been compared, showing that competition had the greatest effect on the optimization of DM policy 48 : when playing with a risk-averse virtual opponent, participants prone to risk-taking behavior optimized their decision-making policy in motor domain. Moreover, it has been shown that both competition and cooperation affected MDM,49,50 resulting in an increased number of effortful trials. 51
To the best of our knowledge, the idea of combining social choice and NE approaches in the context of neurorehabilitation has not yet been extensively explored. We propose that knowledge of a patient's social preference profile can help shaping the social environment to promote the use of the affected limb. We hypothesize that if a patient is highly prosocial in neuroeconomic games, this information can be used in the design of rehabilitation tasks, for example, by creating an environment in which the use of the affected limb is linked to the outcomes received by the other players and thus to the outcome of the group as a whole. Different social situations with real or virtual “opponents” can then be tested in gamified motor training.
The relationship between the described contexts (risk/uncertainty, time and social) and their link with motor impairment consequences via the concept of expected utility is schematically represented in Figure 2.
Neurophysiological Basis of Neuroeconomics Approach to Motor Rehabilitation
According to the results of invasive animal studies, a number of areas critical for movement preparation and execution are also encoding MDM parameters.10,52-55 Recently it has been suggested that prefrontal cortical areas such as DLPFC, responsible for goal valuation during decision-making under risk, 56 also modulates motor output, speeding up movement execution. 57 Some evidence suggests the orbitofrontal cortex involvement in encoding values for the movements’ endpoints. 55 The dorsal premotor cortex, the primary motor cortex and cerebellar activity was also shown to be related to reward processing and vigor of the movements.10,58 Motor cortex excitability during transcranial magnetic stimulation has also been reported to be associated with reward magnitude. 9 These findings suggest that we might improve participation and motivation by engaging patients into motor tasks implying various choices, while influencing the activity in the areas critical for movement preparation, execution and motor learning. Regarding deep biological connection between DM processes and motor rehabilitation, it is also worth noting that monoamine neurotransmitters such as serotonin and dopamine, well known for their key roles in the DM processes, 59 are also actively discussed in the context of stroke recovery. Drugs such as levodopa and carbidopa, and citalopram and fluoxetine are intensively tested for many years as possible new drug therapy options in stroke. 60 Moreover, there are animal studies showing that dopamine transmission is important to drive motor rehabilitation after stroke through motivational aspects and suggesting that augmented motivation and reward feedback could be an interesting strategy to increase the effectiveness or rehabilitation. 12
Possible New Directions to Study DM and MDM in Motor Rehabilitation Framework
Providing that the activity of different brain areas is linked to decision-making parameters, one may expect that the detrimental effect of brain damage, together with the psycho-social factors accompanying any disorder will result in a modified DM profile in patients, in both cognitive and motor domains. In the next section, we will elaborate on our suggestion that introducing NE tools to motor rehabilitation might be helpful to make it more successful (see Figure 2). We will use the examples of LNU after stroke and motor impairment in psychiatric conditions, primarily functional movement disorders (FMD), to illustrate our point.
Stroke
Lesions after stroke often compromise both motor and cognitive functions, including DM in classical NE tasks. For instance, stroke patients show preferences for disadvantageous choices 61 and increased risk-taking in gambling tasks. 62 Studying DM in patients with brain lesions has already provided important insights into the functional roles of specific brain areas, known to be involved in DM in healthy people.63-65 For instance, the orbitofrontal cortex (OFC) damage in humans was shown to increase risk-taking behavior. 66 Damage of the ventromedial prefrontal cortex (vmPFC) resulted in decreased performance in the decision-making task, possibly due to the insensitivity towards reward magnitude. 67 In patients with insular cortex and supramarginal gyrus lesions, including stroke, the compromised emotional processing has been associated with impaired performance in DM tasks. 68 Generally, it was suggested that DM impairment may be attributed to impaired connectivity patterns within prefrontal, somatosensory, motor, and insular cortices, as well as basal ganglia (specifically, the amygdala).68-70 Similarly to the cognitive domain, we expect to observe differences in risk preferences, loss aversion and other aspects of the DM in the motor domain in this clinical population.
For instance, we suggest that LNU after stroke is, at least in part, an example of distorted MDM. LNU represents a big problem for motor rehabilitation, being a frequent clinical observation from the beginning of the 20th century.71,72 LNU is thought of as the difference between the functional capacity of an affected limb and its actual use in daily life. However, LNU etiology, mechanisms and even its clear definition are disputed. 73 To deal with LNU, constraint-induced motor therapy (CIMT) was suggested several decades ago, 4 and then proven to be effective for increasing “the confidence to use the arm for a given level of function.” 74 However, CIMT is applicable only for a limited fraction of stroke patients 75 and in-hospital CIMT courses are not always sufficient for the continuous therapeutic effect. To deal with this issue, a special model to define the motor threshold of the arm spontaneous use was suggested, 76 determining whether the performance will deteriorate or improve after guided-therapy termination.
We suggest that measuring the utility of using affected and unaffected limbs in different experimental settings and assessing patient individual loss aversion in both cognitive and motor domains could be a new fruitful area of LNU research. We also suggest that individualized LNU parameters such as the temporal discount factor, the degree of risk and loss aversion, and the propensity for cooperative/competitive behavior, transformed into an individualized MDM profile, could be tested for their added value as quantitative input for individual SMART goal formulation in stroke in general. If some of these parameters prove to be relevant for the rehabilitation success, they could be then implemented in rehabilitation program assortment or soft-coded (adjusted by a customer/user) in motor rehabilitation, including robotics/game-based rehabilitation. DM profiles may potentially be helpful in motor rehabilitation prognosis and stratification of the risks associated with other types of motor impairment after stroke, such as pathologic synergies, or risk of falls.
Motor Impairment in Psychiatric Illnesses
Another direction of DM implementation for motor impairment may be in psychiatry. Since movements are the behavioral output of complex neural processing, it is natural to expect that it may change when nervous system functioning is compromised. Most psychiatric disorders are characterized by the presence of motor abnormalities. For instance, anxiety is manifested by restlessness and motor agitation, while depression is usually associated with motor retardation. 77 Moreover, there are neuropsychiatric conditions that predominantly manifest in motor symptoms, such as catatonia, obsessive-compulsive disorder (OCD), or functional movement disorders (FMD). It has been shown that psychiatric patients with OCD, Generalized Anxiety Disorder and FMD have abnormal DM profiles, including changes in loss-aversion, risk preferences and intolerance to uncertainty.78,79 Importantly, these pathological DM profiles are associated with the major clinical manifestation of the disease.79,80 At the same time, to the best of our knowledge, there are no reports where NE parameters have been implemented in the motor control investigation in psychiatric patients. Such implementation, however, may be crucial for optimizing treatment strategies due to a general link between the NE parameters and MDM, as described above. For example, in FMD, motor rehabilitation is an important component of the treatment protocol. It implies a gradual increase in training intensity, 81 the speed of which is individually adjusted and, at the moment, depends on the expertise of rehabilitation specialists. We suggest that the estimation of a patient loss-aversion individual profile, using the NE paradigm may help adjusting this speed following quantifiable algorithms. Since the rehabilitation of FMD is challenging both financially and timewise, an additional rationale for using these parameters would be to determine a specific threshold when guided motor rehabilitation can be terminated with minimal risk of relapse, similarly to the threshold described for CIMT guided-therapy termination in stroke. 76
Despite the recent progress in psychiatry aimed at the objectification of diagnostics criteria, 82 the field is still in high need of cost-effective approaches that can be used in large-scale screening for diagnostics and treatment effectiveness estimation purposes. 83 Proceeding further with the FMD example, there are several objective neurophysiological parameters, such as contingent negative variation 84 or reduced drift rate, 79 which might be useful for this purpose. However, these parameters require quantitative analysis of the neurophysiological data (like electroencephalography or magnetoencephalography), which is not always easy to implement in psychiatric premises. We suggest that simple behavioral tests estimating DM and MDM profiles may be a promising alternative for such purposes. 85 For instance, a set of reaching movements towards a number of goals might help estimate the utility of an affected limb or compromised movement patterns. The utility of a movement representing a target for a rehabilitation program might be used as a threshold, which, once reached, suggests that treatment can be terminated with minimal risk of further relapse.
Recommendation
We have several suggestions for the future study of NE in motor pathology and motor rehabilitation: (i) Individualized NE parameters (i.e., risk-taking, loss aversion, temporal discount factor) should be tested as possible predictors of motor recovery and used to individualize patients' motor tasks during the rehabilitation process, and the effects of such adaptation should be evaluated. (ii) In addition, we propose to investigate how motor performance (i.e., accuracy, reaction time) changes in patients with motor impairments of different origins in modified individualized motor tasks. In particular, we hypothesize that the effect of being able to choose between different motor goals in a gamified rehabilitation task should be tested, as well as the effect of changing parameters of the goals (e.g., the distance to the target and the reward value associated with that target). (iii) We also suggest that motor performance could be affected by different social interaction conditions (competition, cooperation, observation) in patients with motor impairment, which should be tested experimentally adopting the MDM parameters listed above. (iv) Finally, we suggest that the added value of the MDM parameters for the optimal threshold/time definition for termination of guided therapy can be tested in further studies. To achieve these goals, we call for more interdisciplinary studies addressing MDM in patients with motor impairments in the context of rehabilitation.
Conclusion
The main premise of this article is that the motor pathology developed due to neurological or psychiatric conditions may have a rather overlooked common denominator—an altered DM in the motor domain. We suggest that NE application in neurorehabilitation should be much wider discussed together by experts from both fields.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article is an output of a research project implemented as part of the Basic Research Program at the National Research University Higher School of Economics.