
Abstract
Background
Determining the discharge destination after acute stroke care is important to prevent long-term disabilities and improve cost efficiency.
Objective
The aim of this study was to investigate where stroke patients are discharged to after acute treatment and to identify personal, social, stroke-related, and clinical predictors of discharge destination.
Methods
The present study included a secondary exploratory analysis of a prospective observational study. Patients with acute ischemic stroke, transient ischemic attack, or intracerebral hemorrhage were recruited consecutively over a 15-month period. A hierarchical multinomial logistic regression was performed to identify predictors of the primary outcome of discharge destination.
Results
We included 1026 stroke patients (48.7% female) with a mean age of 73.3 years (standard deviation 12.9 years) in the analysis. Overall, 55% of the patients were discharged home, 33% to a rehabilitation center, 3% to a residential facility, and 8% to another acute care hospital. Predictors that statistically significantly influenced the odds of the discharge destination were age, living situation pre-stroke, living location pre-stroke, stroke type, stroke severity, treatment type, and length of stay. Higher stroke severity was associated with discharge to all four inpatient facilities.
Conclusions
In line with previous research, predictors such as stroke severity and living situation pre-stroke significantly influenced the odds of the discharge destination. In contrast, pre-existing conditions and functional impairment pre-stroke had no significant impact on the primary outcome. This discrepancy could be due to a rather functional study sample before stroke and the use of clinical and patient-reported outcome measures.
Introduction
People aged 25 and above have a 25% global lifetime risk of suffering from stroke which is associated with long-term consequences and causes disabilities such as motor control impairments, cognitive and language impairments, and emotional disturbances.1–5
Inpatient or outpatient rehabilitative care follows acute stroke care. As patients are affected to varying degrees by disabilities after stroke, the type of follow-up care needed differs. 6 For follow-up care, timely discharge to rehabilitation facilities or home with outpatient care has been shown to improve patients’ chances of recovery.7,8 In contrast, a rapid discharge without previous discharge arrangements is often associated with discontinued care and a delay in discharge is associated with increased mortality.8,9 Additionally, finding appropriate follow-up care strongly impacts the time and cost-efficiency of stroke care, which is important considering limited time resources at the hospital and high stroke care costs.9,10
In their review, Thorpe et al 11 revealed that a discharge home becomes more likely with a better outcome on scoring systems for the assessment of acute stroke such as the National Institutes of Health Stroke Scale (NIHSS). 12 However, they concluded that outcome measures are not sufficient to predict discharge destination. Patients with low performance scores were more likely to be discharged to rehabilitation, and patients with high performance scores were more likely to be discharged home, but discharge destination could not be predicted well for patients with mid-range scores. 11 In these cases, additional factors are needed to enable the prediction of the discharge destination. In another review, support at home, living with others, being married, and living at home before stroke onset indicated a greater likelihood of a discharge home. 13 Moreover, while the impact of age and sex was less clear, a better pre-stroke functional and post-stroke cognitive status increased the likelihood of being discharged home. 14 In conclusion, different reviews recommend further research on age, sex, type of stroke, patient-specific biopsychosocial factors, other stroke-specific outcome measures, and global socioenvironmental determinants.11,13-15
Therefore, we aimed to assess where stroke patients are discharged after acute treatment and to identify personal, pre-stroke, stroke-related, and clinical predictors of discharge destination.
Methods
Design and Recruitment
We performed a secondary exploratory analysis of a prospective observational study with a longitudinal design to evaluate patient-reported outcome (PRO) measures (PROMs) after stroke in routine clinical practice. 16 Patients were recruited over a 15-month period during initial treatment in the stroke unit of a university medical center after diagnosis of acute ischemic stroke (AIS), transient ischemic attack (TIA), or intracerebral hemorrhage (ICH). Outcomes were assessed at admission and discharge. All patients aged 18 years or older referred to the stroke unit were screened for study participation consecutively via electronic medical records. Patients were excluded in cases of severe disturbances in their ability to communicate or insufficient knowledge of the German language. More information on the study design of the original study is reported in the study protocol. 16
Written informed consent was obtained from patients or authorized guardians. An ethics committee of physicians approved the study protocol. This study was registered at ClinicalTrials.gov.
Measures
Data were collected using the International Consortium for Health Outcomes Measurement Standard Set for Stroke (ICHOM-SSS). 17 In addition to patient demographics, the ICHOM-SSS 17 measures stroke type and severity, vascular and systemic risk factors, comorbidities, treatment and care, complications, functional outcome, discharge destination, survival and patient-reported health, including the NIHSS. 12 PROs are information on the patient’s health status given by the patients themselves, without a need for interpretation by health care professionals. For this study, only data collected at the first two points of measurement at admission and at discharge were assessed.
The primary outcome was destination after discharge from the stroke unit assessed by the ICHOM-SSS. The discharge destination variable was extended by the item “geriatric rehabilitation” to accommodate the German health system. In Germany, neurological rehabilitation aims to train neurological deficits by making use of speech therapy, physiotherapy, and neurology. In geriatric rehabilitation, on the other hand, improvement in quality of life and social skills is the focus. A residential facility has no rehabilitation services. Hence, the variable was grouped into “living independently or in own household,” “residential facility,” “neurological rehabilitation,” “another acute care hospital,” “patient died in hospital,” and “geriatric rehabilitation”.
Variables included in the analysis were measured at two time points: age, sex, living location pre-stroke, living situation pre-stroke, functional impairment pre-stroke, stroke type (AIS, TIA, ICH), stroke severity (NIHSS), pre-existing conditions (prior stroke, prior TIA, prior myocardial infarction [MI]), alcohol intake, and care level pre-stroke were assessed at admission for index stroke. The variables type of treatment, length of hospital stay, and discharge destination were assessed at discharge.
Living location pre-stroke was defined as having lived at home without support, at home with support, or in an assisted living home, nursing home, skilled care facility, rehabilitation hospital, or in long term care. Living situation was defined as having lived alone or with a partner or other people before stroke. The variable functional impairment prior stroke was computed by summing three variables of the ICHOM-SSS measured as PROs at admission for index stroke event. The variables concerned inquired after the ability to walk, the need for assistance for going to the toilet and for dressing. The resulting variable was continuous and defined no functional limitations as 0 and high functional limitations as 2. Stroke type and stroke severity were assessed by clinicians, using the continuous scale of the NIHSS for stroke severity. Pre-existing conditions were assessed by the patient’s personal history. The variable alcohol was operationalized as having more than one alcoholic drink a day or not. Care level is not part of the ICHOM-SSS and for this study was added to the questionnaire. In Germany, care level defines the individually recognized need for care and assistance of a person according to the Long-Term Care Insurance Act (“Pflegeversicherungsgesetz”). This means that a higher level of impairment and requirement of long-term support to perform everyday tasks, goes along with a higher level of care and higher financial entitlement. The highest level of care is 5. Furthermore, the type of treatment (thrombolytic therapy, thrombectomy, hemicraniectomy), length of hospital stay, and discharge destination were assessed by clinicians.
Statistical Analysis
Descriptive statistics using frequencies and mean values were computed to describe the sample. For the identification of predictors for the discharge destination of stroke patients after initial care at a stroke unit, we conducted a hierarchical multinomial logistic regression model with three chronologically ordered blocks. In multinomial logistic regression, a binary logistic regression is computed for every category of the outcome in comparison to a predefined reference category. Hierarchical regression refers to the blockwise inclusion of the predictors. The first model included a block of predictors that were related to the patient’s condition independent of stroke (age and sex) or related to the time before the stroke incident (living situation, living location, care level, pre-existing conditions, and alcohol use). In the second model, medical predictors regarding the current stroke incident (stroke type, stroke severity, and treatment type) were added. In addition to the first and second block, the third model included a third block (length of stay). The category of patients being discharged to their own household was the reference category. Patients who died in the hospital and cases missing more than 30% of all variables were excluded from the analysis.
Missing data were imputed using multiple imputation. In the process, 538 (3.9%) out of 13826 data points were imputed. To check the robustness of the findings against different approaches to dealing with missing data, we performed a sensitivity analysis with complete cases only. Data were tested for problems with multicollinearity. Throughout all analyses, we considered findings with P ≤ .05 to be statistically significant. All analyses were performed using R, version 4.1.3, package nnet. 18
Results
Sample Characteristics
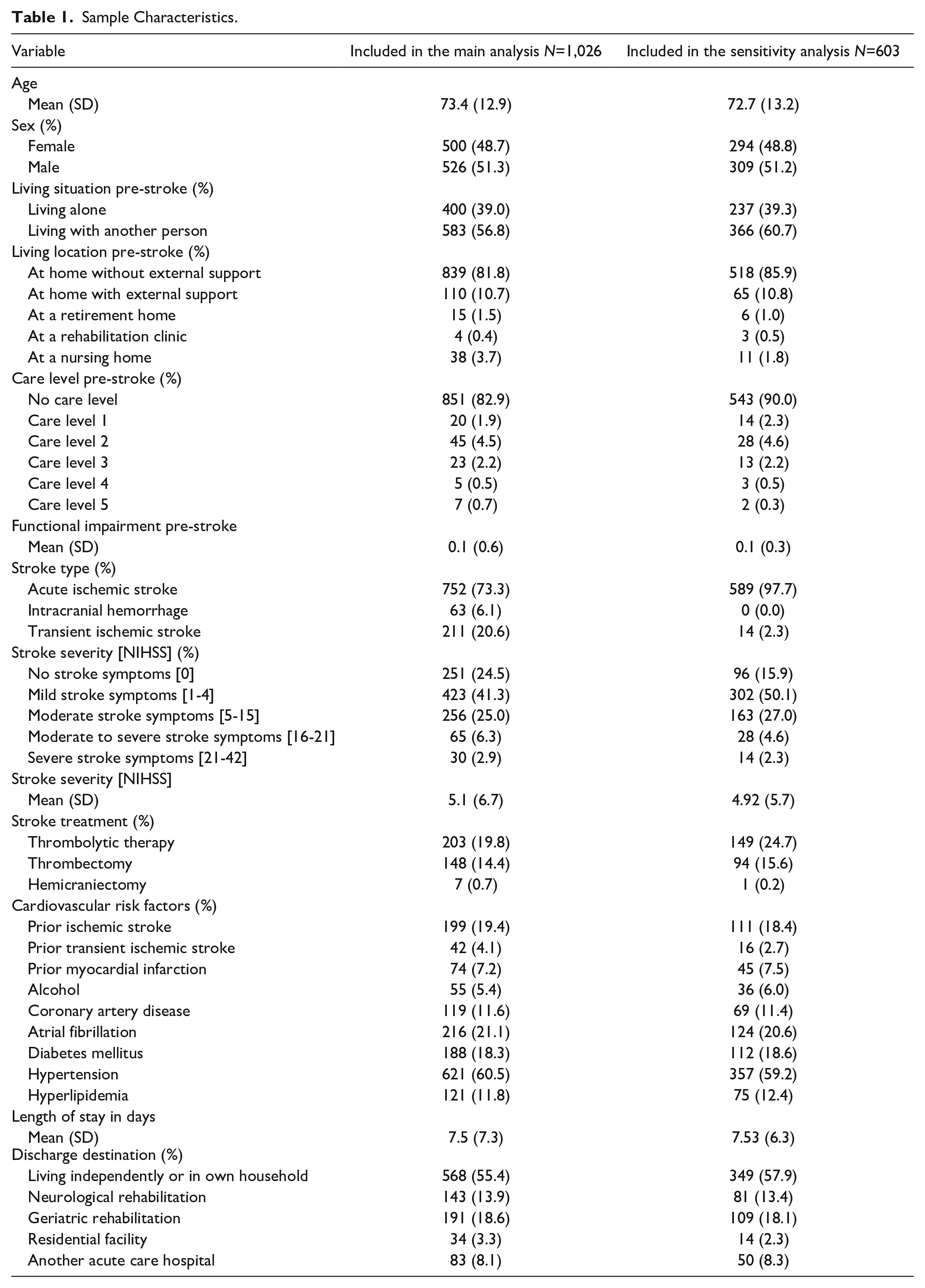
From a total of 1067 patients included in the original study, 19 we included 1026 patients in the present analysis (35 patients died in the hospital, and for six patients the proportion of missing values exceeded 30%). A total of 603 patients provided complete data and were included in the sensitivity analyses. Sample characteristics are displayed in Table 1. The mean age of the sample was 73.4 years (standard deviation, SD = 12.9 years), and 48.7% were female. Before stroke, more than half of the participants lived with a partner or another person and mainly at home without external support. Few patients had care levels pre-stroke, and few had low functional impairment before stroke. The AIS (73.3%) was most common in our study sample, followed by transient ischemic stroke (20.6%), and intracranial hemorrhage (6.1%). Using the NIHSS, most patients experienced no or mild stroke symptoms (65.8%), one-fourth of the patients had moderate symptoms, and 9.2% of the patients had moderate to severe or severe symptoms.
Sample Characteristics.
Discharge Destination
Half of the patients were discharged home (55.4%), few were discharged to a residential facility (3.3%) or another acute care hospital (8.1%), and collectively, more than one-third were discharged to neurological (13.9%) or geriatric (18.6%) rehabilitation (Table 1).
Main Analysis of Predictors of Discharge Destination
Due to the low number of patients who underwent hemicraniectomy, this variable was excluded from analysis. Due to categories with low frequencies, the variables care level pre-stroke (yes/no) and living location pre-stroke (at home/in institution or at home with help) were dichotomized. In addition, we summarized the three variables concerning pre-existing conditions into one variable. Preparatory analyses suggested that there was no concern with multicollinearity (Tolerance = 0.41-0.98; VIF = 1.03-2.40).
The results of the main analyses for predicting discharge destination are displayed in Table 2, results including confidence intervals are displayed in Supplemental Table 1. Being discharged to a neurological rehabilitation facility in contrast to being discharged home was statistically significantly associated with stroke type, stroke severity, and length of stay. Patients with the stroke type AIS in comparison to those with TIA had 7 times higher odds of being discharged to a rehabilitation facility. Additionally, having more severe stroke symptoms (odds ratio [OR] = 1.23 per grade) and an increased length of hospital stay (OR = 1.21 per day) were also associated with higher odds of discharge to a neurological rehabilitation facility instead of home.
Results of Multinomial Logistic Regression Analysis.
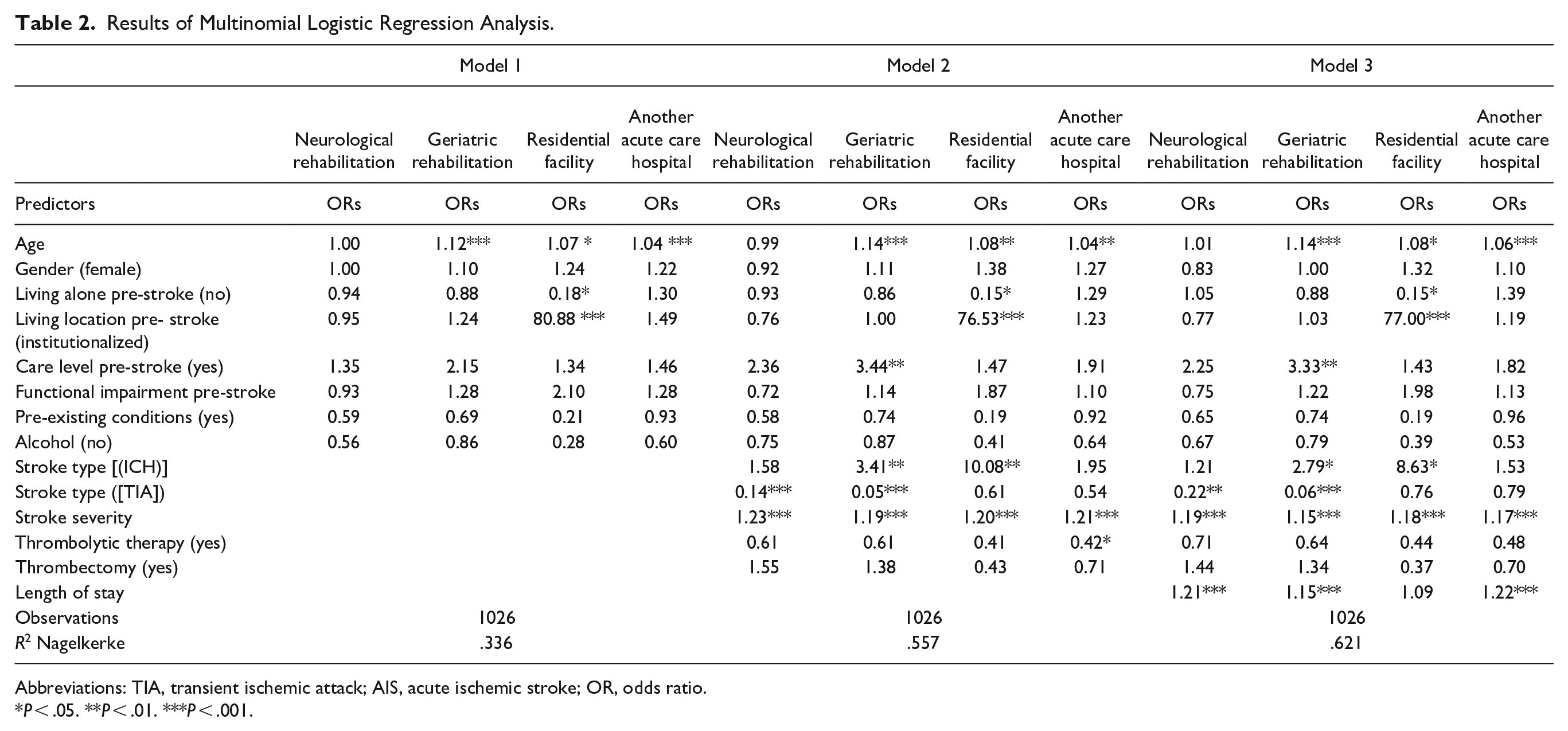
Abbreviations: TIA, transient ischemic attack; AIS, acute ischemic stroke; OR, odds ratio.
P < .05. **P < .01. ***P < .001.
Whether patients were discharged to geriatric rehabilitation or home was statistically significantly predicted by age, stroke type, stroke severity, and length of stay. With an increase in age, stroke severity, and length of stay, the odds of a discharge to geriatric rehabilitation were higher. Additionally, patients with the stroke type ICH in comparison to those with AIS were 3.4 times more likely, and patients with AIS compared to those with TIA were 20 times more likely to be discharged to geriatric rehabilitation.
Discharge to a residential facility rather than to one’s own home was statistically significantly associated with age, living situation pre-stroke, living location pre-stroke, stroke type, and stroke severity. Living alone before stroke was associated with 5.56 times higher odds, and an increase in age was associated with 1.07 times higher odds. Patients who lived in an institution before the stroke incident had an 80.88 times higher likelihood of being discharged to a residential facility. The odds were 10 times higher if patients had ICH than if they had AIS. A higher stroke severity made discharge to a residential facility 1.20 times more likely per grade.
For patients who were discharged to another acute care hospital rather than to their own home, age, stroke severity, type of treatment and length of stay were statistically significant predictors. An increase in age resulted in a relative change of the odds of 1.04 per year, in stroke severity of 1.21 per grade and in length of stay of 1.22 day.
Assessment of the blocks used in the hierarchical analysis revealed that the explanatory power of the model benefitted from the inclusion of the second block and third block of predictors. The Nagelkerkes pseudo R2 was highest with all 13 predictors included (pseudo R2 = .622). A higher pseudo R2 indicates a higher proportion of variation explained by the predictors.
Sensitivity Analysis of Predictors of Discharge Destination
The analysis of complete cases only confirmed the results of the main analysis. Deviations were noted in stroke type, pre-existing conditions, and alcohol intake. The distribution of the sample differed regarding the type of stroke with no ICH and over 95% AIS. For this reason, the treatment type ICH could not be investigated in the sensitivity analysis. For pre-existing conditions, the deviation was notable with smaller odds, although in the same direction, of discharge to a residential facility than home. The detailed results of the sensitivity analysis are displayed in Supplemental Table 2.
Discussion
In this study, the discharge destination after acute stroke treatment was associated with personal, pre-stroke, stroke-related, and clinical predictors. Age, living situation pre-stroke, living location pre-stroke, stroke type, stroke severity, treatment type, thrombolytic therapy, and length of stay were predictors that significantly influenced the odds of the discharge destination of stroke patients. In contrast, no significant associations were found between sex, care level pre-stroke, functional impairment pre-stroke, pre-existing conditions, thrombectomy or alcohol use, and the likelihood of a specific discharge destination.
We found that a higher stroke severity increased the odds of discharge to one of the four inpatient destinations compared to discharge to one’s own home, as expected. A similarly high change in the odds was observed if patients had been living in an institution before stroke, although only in regard to being discharged to a residential facility. The impact and change in the odds of patients’ stroke type differed. Patients with ICH had higher odds of not being discharged home than those with AIS when compared to discharge to geriatric rehabilitation or a residential facility. Patients with AIS were more likely to be discharged to one of the rehabilitation facilities than patients with TIA. A TIA is often associated with a milder progression of disease, which may explain why patients are discharged home more often than to a rehabilitation. Differences in the outcomes between the neurological and geriatric rehabilitation facilities revealed that older patients and patients with ICH were more likely to be discharged to a geriatric rehabilitation facility. Patients who had not been treated with thrombolytic therapy were more likely to be discharged to another hospital rather than home. Last, patients with longer inpatient care had a higher likelihood of being discharged to one of the rehabilitation facilities or another acute care hospital. The sensitivity analysis confirmed these findings.
In line with other research, stroke severity was an important predictor.11,20,21 As expected, patients with a higher grade of stroke severity needed further and more extensive care. Future research should focus on how stroke severity interacts with other variables as a predictor of discharge destination. Other studies support 14 and contradict 20 our outcome regarding sex, and no consensus seems to be reached on its role regarding discharge destination.14,20
Discharge to a residential facility was impacted by the living situation before stroke. Patients who had lived alone before stroke were 5.56 times more likely to be discharged to a residential facility. In our sample, nearly 40% of the patients had lived alone and 26% had lived alone at home before stroke. A quarter of patients had been affected by the stroke incident to a degree that they had to be discharged to a residential facility after acute care. This emphasizes the importance of pre-stroke living situation as a predictor of discharge destination and the benefit of social support and having a caregiver at home after stroke. Other studies have investigated the relationship between discharge home and the availability of a caring spouse or other person at home.13,22,23 Similarly, the presence of a caregiver at home was associated with increased discharge to home, although Dutrieux et al 22 found this effect only in the patient group aged 70 years and above. Furthermore, living in an institution or at home with external help before stroke was a significant predictor of discharge to a residential facility. However, the comparison in our study was being discharged to a residential facility or to one’s own household, which in the case of patients living in an institution before stroke would mostly be a residential facility. This explains the high outcome for living in an institution before stroke and discharge to a residential facility.
Another outcome of this study was the significant impact of longer hospital stay on discharge to one of the rehabilitation facilities or another hospital. The reason could be associated, for example, with the severity of stroke or with organizational problems. To our knowledge, length of stay has rarely been included in analyses of discharge destination from stroke units. Some studies have included length of stay to assess discharge after rehabilitation but not after acute care.24,25 The reason for this association should be investigated further since this may be an aspect that can readily be influenced by clinicians. The hierarchical model of this study showed that length of stay is an important addition to the prediction of discharge destination.
In contrast to other studies, pre-existing conditions and functional impairment pre-stroke had no significant impact on discharge destination.8,14,21,26 A possible reason for this discrepancy is that the measures used to assess pre-existing conditions or functional impairment were different in our study from those used in other studies.14,21,26 While others made use of clinical assessment tools, that is, the Faurot Frailty Index, modified Rankin Scale or information from patient files, in our study, here these measures were patient-reported. On the one hand, the mentioned scales measure frailty or disability and can assess a patient’s impairments in daily life better than pre-existing conditions or functional impairment. 27 On the other hand, it is also noteworthy that our data were collected with PROMs. The question arises to what extent the assessment of impairments, and thus their influence on the prediction of the discharge destination, changes when the aforementioned or more data were collected in terms of PROs. Additionally, patients in our sample seem to have had low functional impairment before, and few patients had an approved care level pre stroke. Hence, low variance may explain why these factors did not contribute to the prediction of discharge destination.
Overall, most of the results of our study confirmed those of existing research. However, there is an important difference regarding the methods of this study compared to others. In this study, data collection was and still is part of a newly implemented routine of stroke patients’ acute care. The primary goal of the associated project was the implementation and evaluation of clinical and longitudinal PROMs. Insofar, this study provides additional confirmation that PROs are also important for the prediction of discharge destination and the identification of care needs. Moreover, the results of this study suggest that the emphasis should not be on pre-existing deficits but onliving situation, stroke type, and stroke severity. With increasing duration of inpatient treatment, a re-evaluation of the predictors for discharge destination seems to be necessary.
Strengths and Limitations
An important limitation to this study is that was is a secondary analysis. The data were not collected to answer the examined research question and we may have missed important predictors of discharge destination (e.g., patient preferences, availability of institutions, financial and organizational constraints) simply because no data on the concerned variables were collected. For example, it is also due to the reuse of existing rather than the collection new data that we could not use the modified Rankin Scale for pre-existing impairment in stroke patients. Furthermore, our study was exploratory in nature. The identified associations need confirmation from carefully designed and hypothesis-driven replications. Another limitation is the wide regional variation in neurological and geriatric rehabilitation facilities. The possibilities of neurological rehabilitation are limited; thus, availability influences the possibilities of the discharge destination. To some patients who would benefit from neurological rehabilitation this cannot be offered.
A major strength of our study lies in the consecutive recruitment of a large, unselected sample. Additionally, we could investigate the effect of several clinically relevant factors on discharge destination under routine care conditions. Furthermore, we utilized a large amount of available data by using multiple imputation. Finally, applying a hierarchical analysis allowed a detailed evaluation of the unique impact of different blocks of predictors.
Conclusions
Several pre-stroke and acute treatment-related characteristics are associated with discharge destination after stroke. Understanding the predictors for discharge destination may contribute to improving decision-making with regard to discharge and follow-up care, thus reducing the long-term negative consequences of this disabling condition as well as enhancing the cost efficiency of cross-sectional care.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683231166935 – Supplemental material for Predictors of Discharge Destination After Stroke
Supplemental material, sj-docx-1-nnr-10.1177_15459683231166935 for Predictors of Discharge Destination After Stroke by Theresa Schrage, Götz Thomalla, Martin Härter, Lisa Lebherz, Hannes Appelbohm, David Leander Rimmele and Levente Kriston in Neurorehabilitation and Neural Repair
Supplemental Material
sj-docx-2-nnr-10.1177_15459683231166935 – Supplemental material for Predictors of Discharge Destination After Stroke
Supplemental material, sj-docx-2-nnr-10.1177_15459683231166935 for Predictors of Discharge Destination After Stroke by Theresa Schrage, Götz Thomalla, Martin Härter, Lisa Lebherz, Hannes Appelbohm, David Leander Rimmele and Levente Kriston in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
Details omitted for double-anonymized peer review. We thank Hans-Jürgen Bartz and Marc Frese and our colleagues from the Department of Quality management and Clinical process management for the good cooperation in the EPOS project. Also, we thank Lea Schumacher for her support in conducting the analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Innovation Fund of the German Federal Joint Committee with grant number 01VSF16023.
Data Availability
Deidentified individual participant data will be made available upon reasonable request and where necessary after approval of the ethics committee by the corresponding author within 24 months after publication. Additional information can be taken from our study protocol.
Trial Registration
The trial is registered at ClinicalTrials.gov (number omitted for double-anonymized peer review).
Supplementary Material
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.