
Abstract
Background
It is unknown whether assessment of autonomic pathway integrity in newly injured traumatic cervical spinal cord injury (SCI) patients contributes to their neurological prognosis.
Objective
The objective is to investigate the relationship of heart rate variability (HRV) and sympathetic skin response (SSR) at initial evaluation of American Spinal Injury Association Impairment Scale (AIS) A/B tetraplegic patients, with their short-term neurological recovery.
Methods
In this prospective cohort study, short-term HRV indices and SSR to supra-lesional stimuli were computed in 24 acute traumatic cervical AIS A/B SCI patients at admission for rehabilitation. The relationship of these autonomic parameters with motor and sensory score improvement, AIS grade improvement, and time taken for recovery was tested, respectively, with Spearman’s correlation coefficient test, Fisher’s exact test, and Kaplan–Meier analysis.
Results
SSR was present in 11 (45.8%) patients at initial evaluation. After rehabilitation, 5 (20.8%) patients improved from AIS A/B to AIS C (greater recovery), while the rest remained at AIS A/B (lesser recovery). Both AIS improvement and mean time for ‘greater’ recovery did not associate with the presence/absence of SSR. Further, HRV indices did not correlate with improvement in motor or sensory scores.
Conclusions
Interim neurological recovery was not related to autonomic parameters of short-term HRV indices and SSR in the AIS A/B tetraplegic patients of our study. Interestingly, about half of the patients with clinically complete SCI had evidence of preserved autonomic function. Our data add to the knowledge base of autonomic findings in cervical SCI patients and will promote research relating neurophysiological parameters and recovery.
Keywords
Introduction
Predicting recovery following traumatic cervical spinal cord injury (SCI) helps to plan the rehabilitation strategy. The International Standards to document remaining Autonomic Function after Spinal Cord Injury (ISAFSCI) endorses recording the autonomic function of SCI patients from history and clinical examination during their initial evaluation.
1
Would objective recordings of electrophysiological parameters of autonomic function—heart rate variability (HRV) and sympathetic skin response (SSR) to supra-lesional stimuli—during initial evaluation of traumatic tetraplegic patients help ascertain recovery outcomes? We addressed this question, by investigating the relationship between these parameters and short-term neurological recovery. As clinical outcome prediction in SCI is mostly based on correlates of neuroanatomical proximity,
2
we reasoned that those with intact SSR and higher HRV would have preserved descending supraspinal sympathetic fibers across the lesion (Figure 1) and therefore likely have more undamaged motor and sensory fibers too, resulting in better neurological outcome. HRV indices
3
and SSR4,5 have been used to study the autonomic system in SCI patients. In cervical SCI patients, parasympathetic vagal supply remaining is preserved, and HRV reveals the extent of intactness of descending sympathetic fibers supplying the heart while SSR tests those supplying spinal sudomotor neurons. Schema of autonomic pathways and testing.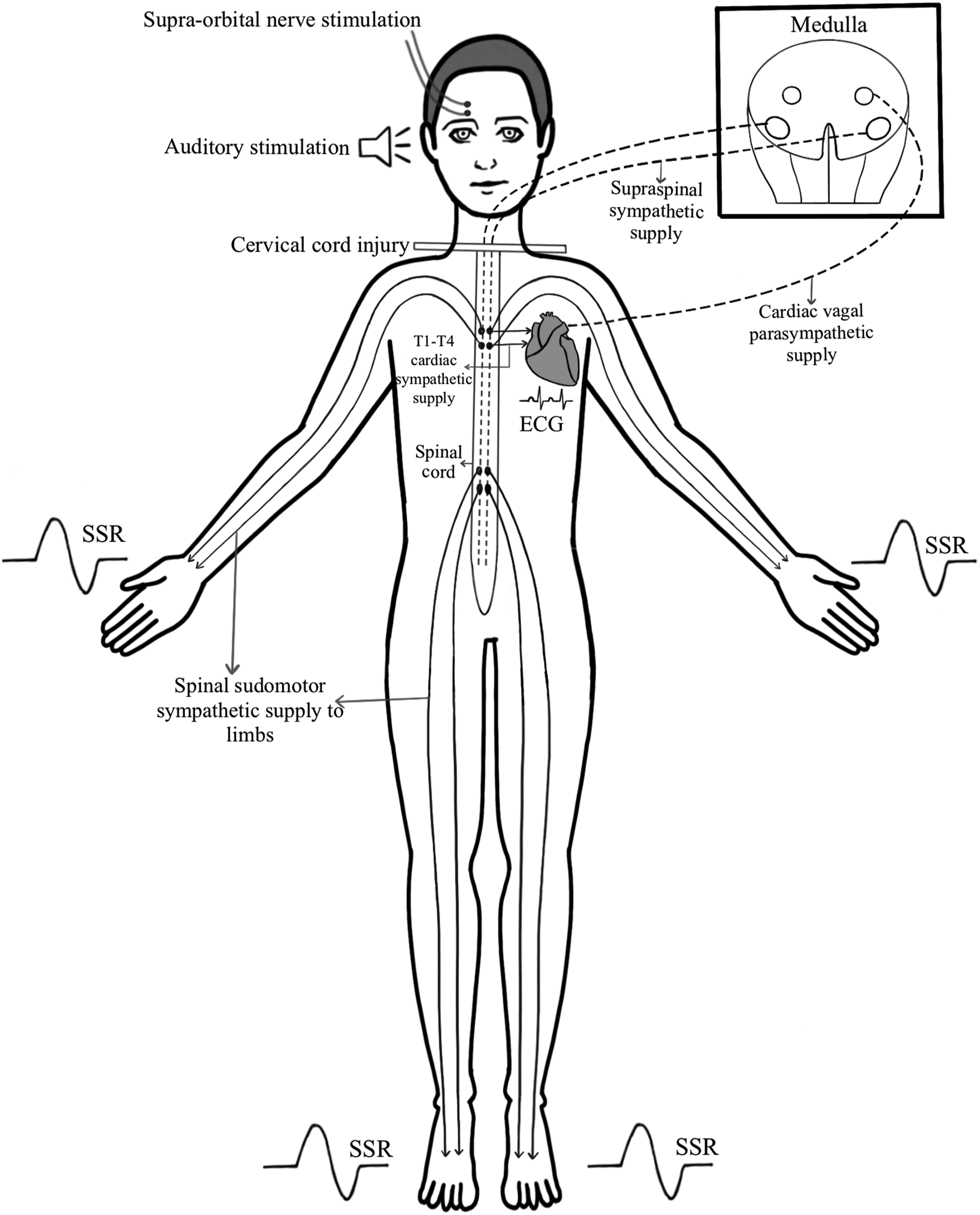
Methods
We designed a prospective cohort study that evaluated the short-term HRV and SSR of traumatic cervical SCI patients with lesions above T1 spinal segment level, presenting as American Spinal Injury Association (ASIA) Impairment Scale (AIS) A/B, on admission for rehabilitation. Patients with progressive spinal cord diseases, cardiac pacemakers, and involvement of T1–T4 spinal segments were excluded. The study was approved by the Institutional Review Board and Ethics Committee and informed consent was obtained from participants.
Clinical Evaluation of Patients
At admission and after inpatient rehabilitation program, the physicians of the Physical Medicine and Rehabilitation Department (blinded to the autonomic tests’ outcome), recorded the patient’s motor and sensory scores and AIS grade, following the ASIA protocol. 6
The improvement was computed as the difference between these scores. Patients who converted from AIS A/B to AIS C/D/E grades were categorized as those with “greater” recovery, while those who remained within AIS A/B as those with “lesser” recovery.
Assessment of Autonomic Parameters
Published patient and laboratory preparations for autonomic testing were followed.3-5 After 10 minutes of supine rest, 5 minutes of Lead II ECG (for HRV analysis) and the SSR were recorded on a validated physiological data recorder (developed by the institution’s Bioengineering Department). An HRV analysis software (Nevrokard aHRV ver.12.0.0, Medistar, Slovenia), by fast Fourier transformation, computed the frequency-domain indices of low frequency (LF) (.04–.15 Hz), high frequency (HF) (.15–.47 Hz), total (LF+HF) powers, and the LF/HF ratio, following published guidelines. 7 The LF and HF powers reflect the cardiac sympathetic and parasympathetic activity, respectively. 7
SSR was recorded from the two hands and feet simultaneously, following published guidelines.4,5 Pre-recorded startling loud sound, and right supraorbital nerve electrical stimulation with a single pulse wave of 35 mA, for .25 ms—an established technique to evoke SSR in tetraplegic SCI patients 4 —were the stimuli applied above the level of injury, to elicit the SSR below the level of lesion, to study the integrity of descending sympathetic fibers across the site of injury (Figure 1). Each stimulus type was applied twice at 1-minute interval with a 5-min interval between the two stimulus modes. If the above sets of stimuli elicited no response in any of the limbs, then SSR was considered to be absent; while SSR was considered to be present if a response was recorded from any limb.
Statistical Analysis
Spearman’s correlation coefficient tested the correlation between the magnitude of improvement in motor and sensory scores and the HRV indices. Fisher’s exact test studied the association between SSR and recovery. Mantel–Cox log-rank test compared the Kaplan–Meier estimates of mean time for “greater” recovery in patients with and without SSR. Mann–Whitney U test compared the changes in motor and sensory scores between those with and without SSR. This study was conducted on calculated sample size (80% power; 5% alpha error) of 24 patients. Analyses were conducted on SPSS 16.0 software. A P-value <.05 was considered statistically significant.
Results
Individual Patient Details of Injury, SSR, HRV Indices, and Improvement after Rehabilitation (n = 24).
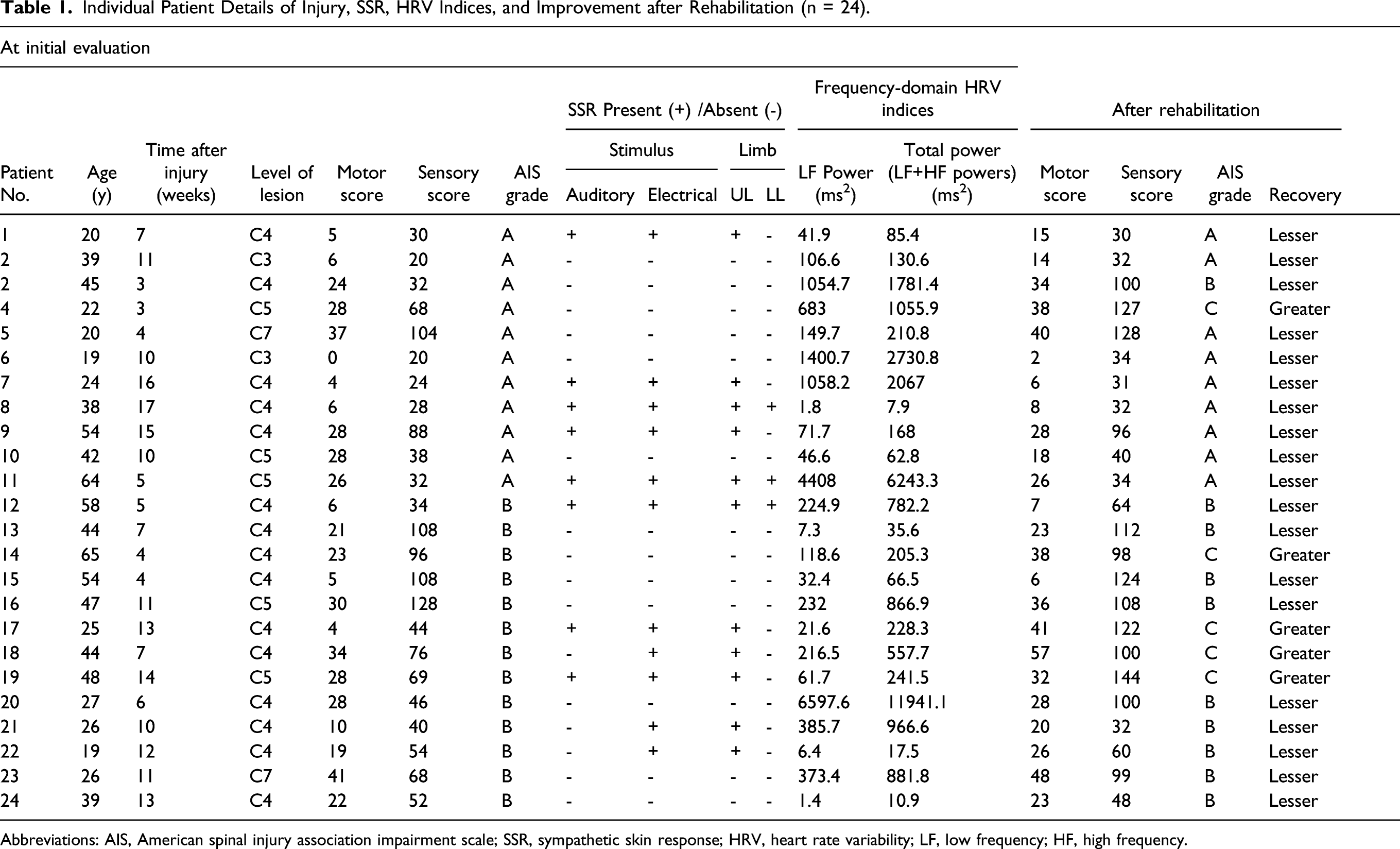
Abbreviations: AIS, American spinal injury association impairment scale; SSR, sympathetic skin response; HRV, heart rate variability; LF, low frequency; HF, high frequency.
Discussion
Short-term neurological recovery was not related to measures of conserved autonomic fibers in the newly injured tetraplegic AIS A/B patients of our study. Somatosensory and motor evoked potentials have been discussed as tools to determine fiber integrity and prognosticate neurological recovery in SCI. 2 However, their usefulness has been established mainly in noncompliant patients. 2 The search for novel approaches to better predict recovery continues, as evidenced by the recent report by Pfyffer et al. 8 on the predictive value of neuroimaging measures of preserved fibers on recovery following SCI.
It is noteworthy that SSR was present in about half of the newly injured AIS A patients of our study, denoting functional preservation of autonomic pathways in spite of severe motor and sensory deficits. Nagarajarao et al. 5 had reported SSR below the level of lesion in 33% of stable ASIA A tetraplegic patients and Claydon and Krassioukov 9 had reported SSR in 40% of chronic complete SCI patients (1 cervical; 5 thoracic).
Our study does not account for the ceiling effect of motor score improvement in different cervical injury levels and did not explore the role of autonomic evaluation for long-term prognosis. It is also limited by the fact that SSR is affected by stimulus type and participant’s emotional status. 10 Further, we could not fix a set time relative to injury for the initial evaluation since surgical stabilization and ICU care, often required during acute stage, preclude autonomic testing. Nevertheless, our data add to the growing evidence of conserved fibers—albeit autonomic fibers—across the lesion in clinically complete cervical SCI patients, indicative of discomplete SCI, although it did not translate to neurological recovery.
Supplemental Material
sj-pdf-1-nnr-10.1177_15459683221081060 – Initial Autonomic Parameters and Subsequent Short-Term Neurological Recovery after Inpatient Rehabilitation, in Traumatic Cervical Spinal Cord Injury Patients
Supplemental Material, sj-pdf-1-nnr-10.1177_15459683221081060 for Initial Autonomic Parameters and Subsequent Short-Term Neurological Recovery after Inpatient Rehabilitation, in Traumatic Cervical Spinal Cord Injury Patients by Latha Nedumaran, Grace Rebekah, Elizabeth Tharion, and George Tharion in Neurorehabilitation and Neural Repair
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research: Institutional research grant from Christian Medical College, Vellore, Tamil Nadu, India, and a grant from the Department of Science & Technology, Southern Hub for Healthcare Instrumentation, Government of India.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.