
Abstract
Background
The negative discrepancy between residual functional capacity and reduced use of the contralesional hand, frequently observed after a brain lesion, has been termed Learned Non-Use (LNU) and is thought to depend on the interaction of neuronal mechanisms during recovery and learning-dependent mechanisms.
Objective
Albeit the LNU phenomenon is generally accepted to exist, currently, no transdisciplinary definition exists. Furthermore, although therapeutic approaches are implemented in clinical practice targeting LNU, no standardized diagnostic routine is described in the available literature. Our objective was to reach consensus regarding a definition as well as synthesize knowledge about the current diagnostic procedures.
Methods
We used a structured group communication following the Delphi method among clinical and scientific experts in the field, knowledge from both, the work with patient populations and with animal models.
Results
Consensus was reached regarding a transdisciplinary definition of the LNU phenomenon. Furthermore, the mode and strategy of the diagnostic process, as well as the sources of information and outcome parameters relevant for the clinical decision making, were described with a wide range showing the current lack of a consistent universal diagnostic approach.
Conclusions
The need for the development of a structured diagnostic procedure and its implementation into clinical practice is emphasized. Moreover, it exists a striking gap between the prevailing hypotheses regarding the mechanisms underlying the LNU phenomenon and the actual evidence. Therefore, basic research is needed to bridge between bedside and bench and eventually improve clinical decision making and further development of interventional strategies beyond the field of stroke rehabilitation.
Keywords
Introduction
Stroke is among the leading causes of long-term disability in adults and the worldwide population of stroke survivors is predicted to increase to 70 million within the next decade, clearly challenging national health care systems. 1 One of the most disabling and persisting consequences of stroke is the paresis of the upper extremity (hand/arm).2,3
One frequent clinical observation is a decreased use of the contralesional hand in spite of latent functional ability and an increased functional reliance on the less-/nonimpaired upper extremity over time. 4 This discrepancy between residual functional capabilities of the impaired extremity and yet reduced usage in everyday life has been termed Learned Non-Use (LNU) and is assumed to be brought about by an interaction between postlesion neural reorganization and mechanisms such as negative reinforcement.5,6 This conceptual framework goes back to the work of Charles Sherrington and colleagues who observed the reduced upper extremity use after surgical interruption of the sensory tracts (deafferentation) in monkeys.7,8 Following up on this seminal work, Edward Taub and coworkers were the first to suggest learning psychological mechanisms to be involved in the development and maintenance of functional disuse of the deafferented forelimb.9,10 They subsequently transferred the LNU concept into the field of neurorehabilitation and developed an intensive training regimen (initially termed forced use therapy 11 ) targeted at counteracting the non-use phenomenon and regaining the lost upper-extremity function. 12 This work has inspired ample experimental and clinical work analyzing the effects of a range of behavioral strategies such as increased dosage, systematic scaling, and sequencing practice of the affected upper extremity in addition to constraining the less affected upper extremity in humans recovering from stroke. 13 Despite the success of this therapeutic approach in the acute and most remarkably in the chronic stage, the definition of LNU has remained rather indistinct throughout the years. Moreover, the diagnostic verification of the actual presence of LNU has received little attention and is oftentimes left to anecdotal findings and subjective descriptions of the patient’s behavior.
In summary, no transdisciplinary14,15 definition exists to date, which would allow a clear and unambiguous description of the LNU phenomenon. Furthermore, so far, no gold standard diagnostic tool exists allowing the identification of the LNU phenomenon in differentiation from other alternative symptom complexes causing the limited use of one extremity, which clearly obscures the evaluation of the effect of therapeutic interventions in clinical populations.
Therefore, the objective of the present work was two-fold: first, to generate a comprehensive transdisciplinary definition of the LNU phenomenon; and second, to facilitate a synthesis of the available assessment strategies and required methodological components for the diagnosis of LNU in patient populations. We, therefore, chose the Delphi method as a structured group communication among clinical and scientific experts in the field of LNU, aiming at integrating the knowledge base resulting from work in healthy and clinical human populations as well as from work with animal models.
Method
The Delphi technique is defined as a group communication process involving an interaction between the researcher and a group of identified experts on a specified topic, usually through a series of questions or questionnaires.16,17 The Delphi method was developed by Olaf Helmer and his colleagues at the Rand Corporation in the early 1950s 18 and has been used to gain a consensus regarding future trends and projections using a systematic process of information gathering.
Selection of Experts as Participants
Experts for the present study are defined as being author/coauthor of international peer-reviewed publication on the focus topic “learned non-use” identified by a database (PubMed, EMBASE) search [combinations of key words: learned non-use, experience dependent non-use, disuse, compensation, stroke, brain lesion, upper extremity, upper limb, forelimb, human, stroke model]. The identified experts were contacted by email (see below) in English and German language.
We decided to offer the coauthorship of the expected publication of the planned Delphi study’s results for two main reasons: (1) Following the example of published work in the field of rehabilitation (eg, Luedtke et al 19 ), our reasoning was that offering a coauthorship represents a valid and appropriate acknowledgement of the participants’ time investment. (2) Since the results of the Delphi study vitally depend on the experts’ motivation to share their expertise and opinion throughout several rounds of the Delphi process, we aimed at assuring constant adherence throughout the study as well as meaningful responses by offering a coauthorship. The direct involvement of the respondents’ motivation in the topic of concern and their high-level motivation of has been defined as a key element to the success and value of a Delphi study. 20
We regard the potential bias that this procedure might incorporate as limited and of minimal danger with respect to potential interference with the results of the study. Due to the Delphi study’s methodology that uses feedback of the answers to the participants after each round, we are confident that including the participants as coauthors has not diminish the value of the outcome and is strictly in line with the advantages of this methodical approach to capture and combine the knowledge and abilities of a diverse group of experts with the “democratic virtues of transparency and openness to criticism” as initially proposed for the Delphi method. 20
Experts identified according to the aforementioned criteria were contacted via email two weeks before the planned start of the structured group communication process and asked to express their interest in participating in the Delphi study by replying to the email, that is, active informed consent. Concise information on the purpose, the procedures of the study, as well as data protection was given in this first email to enable their general decision for or against participation in the Delphi study. All recipients of the initial email were informed that it would be possible for the research personnel directly involved in the data acquisition and analysis to map the answers to the individual participants. Automatic email responses were not considered and no response to the initial email was taken as withheld consent. After active response to the initial email, experts were registered as participants in the Delphi study and received the link to the online survey. From initially 41 identified international experts, 21 actively consented to participate in at least one round of questions. The final sample represented clinicians and scientists in the area of applied clinical research and basic sciences working with human and animal data in England, France, Germany, Netherlands, Spain, Switzerland, and the United States of America.
During the group communication process, the participants of the study remained anonymous toward each other. No personal data except the online available information on the experts (personal webpage, institutional webpage) was acquired. Since a coauthorship was offered to all experts who participated in the group communication, personal information (name and affiliations) is revealed of those who agreed to the coauthorship.
Procedure
Based an initial literature search (March-April 2017) to identify experts described above and a second search (July 2017), we screened the retrieved literature to gather information about (1) existing descriptions of and (2) procedures to identify the LNU phenomenon. The resultant information was used to deduce a system of main categories, which served as the basis to formulate the questions for the first round of the group communication. The group communication was performed with an established online survey tool (SurveyMonkey Inc, www.surveymonkey.com) that suffices common data protection regulations.
Starting from two initial questions (Textbox 1), the group communication followed an iterative process in which the responses of each question round were fed back to the study participants with the two main goals: (1) to reach a consensus with regard to the definition of the phenomenon and (2) to synthesize the components of the diagnostic process.
Initial Questions of First Delphi Round.
The phase of the structured group communication comprised of three rounds of questions and responses and took place between May 2017 and September 2017 (overview of the full process of the Delphi study is given in Figure 1).
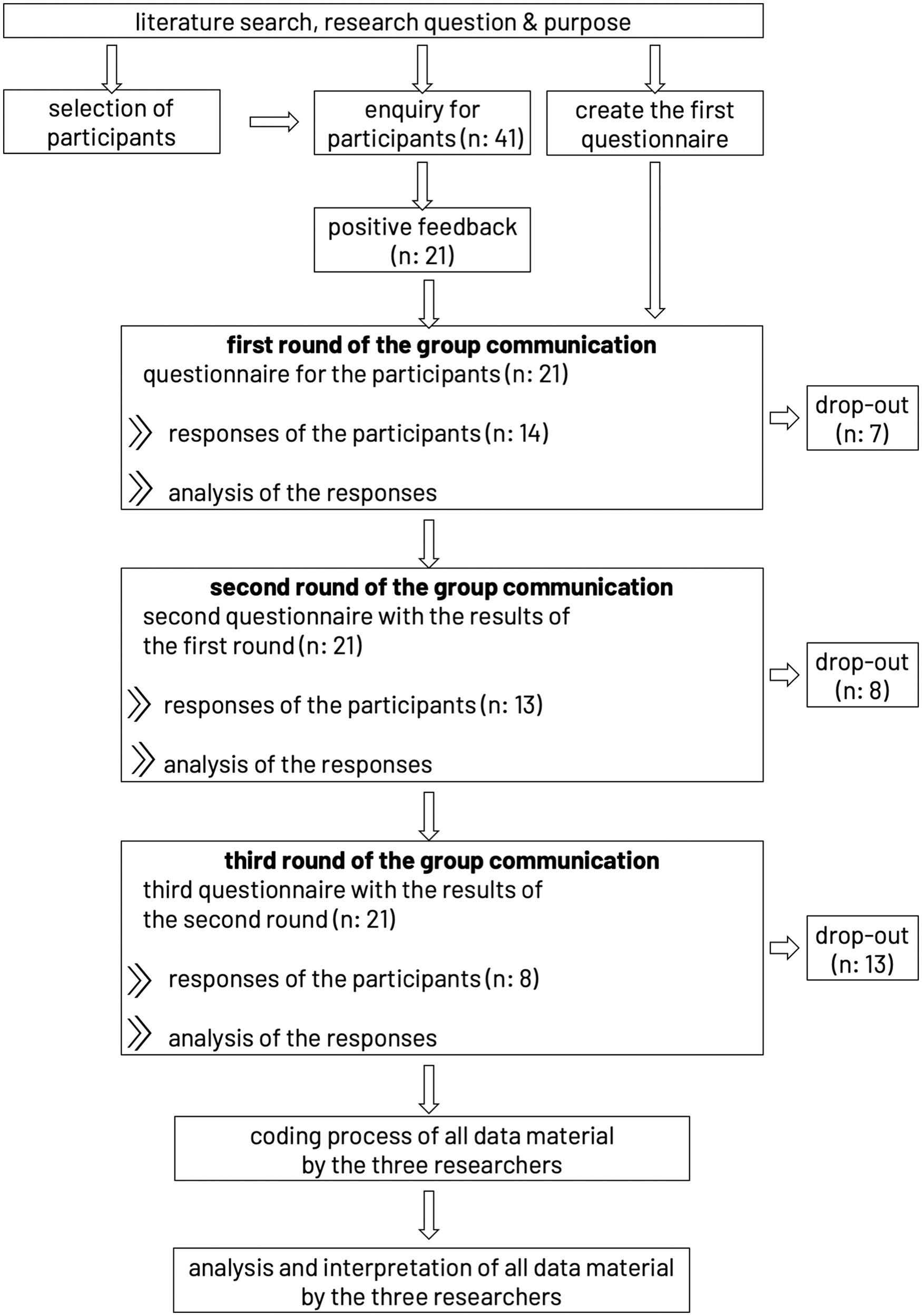
Flowchart of the methodological approach of data acquisition and analysis and attrition of participating experts throughout the Delphi study. In each round, all 21 participants received the questions. The respondents of one round do reflect a different subgroup and not merely a subset of the preceding round.
Data Analysis
The data material gathered in the three rounds of open questions was subjected to a qualitative text analysis following Kuckartz, 21 which consists of a category-based analysis approach of the text material. The main goal of the structured qualitative content analysis is defined as developing main and subcategories, which structure the content of the data and reduce the material allowing for consensus and synthesis. We chose this method because both, the research question and the goal require an exploratory approach in the data collection and analysis rather than the verification of an a priori hypothesis. Hence, the qualitative content analysis allows a stepwise development of the central topics of the subject area, which is optimally suited for the systematic integration of deductively and inductively generated new knowledge and opinions under methodologically well-controlled conditions.
Starting from the a priori deductively developed system of main categories (see above), additional main and subcategories were inductively developed based on the data material. In the present case, the data material consisted of English and German responses, which were left in their original language in this first analysis phase in order to retain the original source information as closely as possible. This initiating analysis of the data material comprised of a first identification of important statements and the collection of main ideas with the overall objective to summarize the information. This phase was carried out by TH for all three Delphi rounds in communication with KFH and MB with the goal to extract the main information, to generate the feedback to the participants and to formulate the follow-up questions for the subsequent Delphi rounds. In a second phase, the main categories, which were a priori deductively developed from the available body of literature (see above), were complemented by additional main categories developed inductively from the data material after the third Delphi round. We followed an open coding strategy of newly developed topics. This step was carried out on approximately 10% of the data material in order to test the specific applicability of the existing categories for the present data material by MB and KFH independently from each other. Consensus regarding the main categories was achieved in a communicative process involving all three researchers (TH, MB, and KFH). In a third phase, the coding process of the complete data material was accomplished. Independently from each other, all three researchers (TH, MB, and KFH) coded all available data material focusing on defined subtopics, which were related to a sub-set of research questions from all three Delphi rounds. Every single section of the available data material was admitted to coding and received single or multiple categories defined in phase 2. After this step, another communicative step among all three researchers (TH, MB, and KFH) yielded consensus regarding the coding of the respective others’ data material. As a result of this step, the category system was further specified, and the coding was re-evaluated. The next phase yielded a summary of the coded material and a further inductive definition of subcategories. The final phases comprised a second coding process of the whole data material geared at achieving a further differentiated category system. As an intermediate step, a systematic case summary was produced employing a framework analysis, which resulted in a theme matrix. By permuting the data within the category system, we aimed at condensing the data material and achieve a pointed description of aspects relevant to our research question. Finally, the analysis and interpretation of the data, including the visualization of results, constituted the last phase. For publication purposes, responses in German language were translated into English and translations were validated by all three researchers (TH, MB, and KFH).
Despite the clear differentiation of the seven phases in this overview, it is necessary to point out that the individual phases were interleaved and partially repeated throughout the process of data analysis until consensus among the three researchers was achieved. We furthermore included an additional step involving the expert participants of the Delphi study to comment on the results and their final interpretation, which received recognition in the discussion section. All experts listed as coauthors were involved in the writing and approved the final version of the manuscript.
Ethics Statement
The protocol and all procedures of this study complied with the ethical requirements as approved by the Social and Societal Ethics Committee of the KU Leuven (SMEC protocol number G-2017 06 841).
Results
The questions formulated based on the initial literature search as well as the questions derived from the subsequent Delphi rounds are given in supplemental online material. As depicted in Figure 1, the synthesis of the responses from one round was integrated into the questions of the subsequent round, and all available data material was analyzed in its entirety within each analysis step throughout the process. Therefore, the results are presented in the permutated order of deductively and inductively developed main and subcategories (overview given in Figure 2 with references to subheadings or keywords in italics in the text below) and are hence generally free from the chronological order of data acquisition. Citations of original responses are presented in English, that is, German responses are presented in their translated version without explicitly stating as such, and are referenced with the internal identification scheme to keep the anonymity of participants.
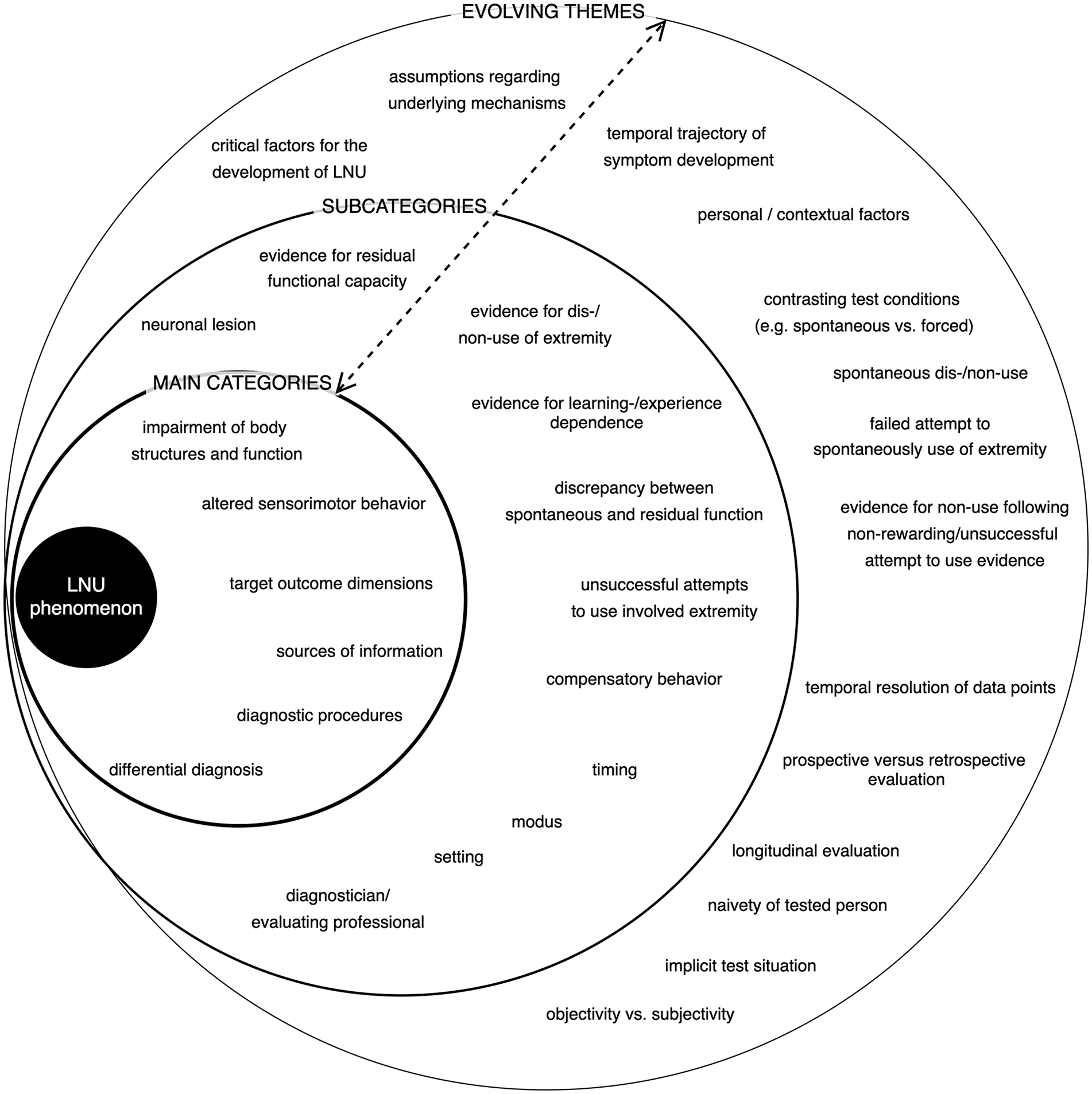
Diagram showing the topics within the main categories, subcategories, and evolving themes (represented by the circles from inside to outside) developed deductively and inductively in the three rounds of the Delphi process. Keywords are shown in the permuted order and are freed from the chronology of the Delphi process. The two sided arrow indicates the interrelation between topics within different category levels and evolving themes.
Definition of Learned Non-Use
The three rounds of questions brought about a wide range of supposedly defining elements of the LNU phenomenon. In this context, two main hypotheses related to the underlying mechanisms were mentioned. On the one hand, this consisted of the initial neuronal injury and the resulting structural impairment and reduction of sensorimotor functioning. On the other hand, experience-dependent processes secondary to the initial lesion were outlined to explain the observed change in behavior over time (timing). In particular negative experiences, such as unsuccessful movements or unsuccessful attempts to move of the contralesional extremity were mentioned in this context by several participants.
All participants agreed on the main characteristic of the discrepancy between the actual spontaneous use and the residual function as the indicator for the conditioned non-use behavior.
Based on these elements, a first draft definition was fed back to the participants and a consensus regarding the definition was reached in the third round, suggested by one expert in its final version: Learned non-use is the discrepancy between a retained motor capacity, which can be retrieved when requested, and the spontaneous use of this motor capacity in daily life, a discrepancy that develops due to experience in inept or non-productive perceived attempts to use that capacity. [C6.r2]
A recurring theme, which was controversially discussed among the participants, was the aspect of compensatory use of the ipsilesional side as an inherent characteristic for the LNU phenomenon. On the one hand, compensation was discussed as an inevitable and logic step in the course of the development of new movement strategies and hence as a key marker for the identification of the LNU phenomenon (example responses given in supplemental material box s1.1).
The compensatory behavior was, on the other hand, hypothesized as a potential factor, which might additionally contribute to the manifestation of the non-use behavior (supplemental material box s1.2).
However, compensatory behavior was also discussed as a strategy that is beneficial for regaining independence in daily life activities (supplemental material box s1.2).
Considering these additional aspects, the final definition was amended as follows: Learned non-use is the discrepancy between a retained motor capacity, which can be retrieved when requested, and the spontaneous use of this motor capacity in daily life, a discrepancy that develops due to experience in inept or non-productive perceived attempts to use that capacity. It is accompanied by compensatory motor behavior identifiable in other body parts.
Critical Factors for the Development of the Phenomenon
It became clear from the answers related to the defining characteristics outlined before, that different assumptions prevail with respect to the factors, which are considered critical for the development of the LNU phenomenon. While the neuronal lesion overall was considered the precondition for the development, the participants’ answers showed less agreement regarding the influence of lesion location and size, severity of the initial impairment, or recovery time-course (temporal trajectory of symptom development). The reorganization pattern following the lesion and in particular the degree of bilateral reorganization was assumed to determine and modify the development of non-use of the contralesional hand (example responses given in supplemental material box s2.1).
Moreover, personal and contextual factors were mentioned with overall agreement as defining factors or effect modulators in the development of the non-use. With respect to personal factors, the individual’s psychological and cognitive situation was considered of particular relevance (supplemental material box s2.2).
Likewise, premorbid factors as for example whether the contralesional hand was the dominant or nondominant side were considered relevant individual factors contributing to the development of compensatory strategies and hence non-use behavior.
The self-efficacy in daily life and the individual’s situation of social support was mentioned as relevant contextual factors that could impact on the actual use of the contralesional extremity both, in a positive or negative way (supplemental material box s2.3).
Learned Non-Use Diagnostic Procedure
While it became clear in three rounds of questions that no generally agreed or standard procedure to diagnose the LNU phenomenon exists to date, the basic features of the optimal diagnostic process were consistently described in all three rounds. Additionally, the need for objectively quantifiable outcome parameters was stressed throughout the whole phase of data acquisition.
Process/Approach
One significant criterion widely agreed upon was the multidisciplinary team, including all health professionals (diagnostician) in contact with the patient, to be involved in the diagnostic process. Furthermore, the majority of the participants stressed the requirement of a longitudinal diagnostic time window (timing) spanning the subacute to the chronic phase after the initial lesion. Therefore, acute and rehabilitation clinical, as well as the home environment, were mentioned as potential settings.
The mode of diagnostic procedures was described somewhat multifaceted involving the enumeration of various existing standardized tests for sensorimotor functioning, observation of specific activities, interviews of patients and relatives, and the use of wearables and motion capture technology. Discussed were also the degree of continuity and sampling rate of the data to be acquired. The aspect of comparison of the integration of the contralesional hand into a defined task in different situations was discussed with two main settings, the spontaneous use and the forced or use upon request or instruction, to be compared (supplemental material box s3.1).
In some descriptions of the diagnostic test strategies, typical therapeutic elements of the constraint-induced movement therapy (CIMT) approach (sequencing, grading) were clearly discernable (supplemental material box s3.2).
In this context, the strategy of contrasting the spontaneous daily life situation with the explicit test situation was repeatedly discussed. Whether or not the patient should be aware of the test situation and the potential of implicit measurement methods were additionally raised as relevant aspects (supplemental material box s3.3).
In contradiction to present clinical practice, some of the participants sharply criticized interview-based evaluation methods relying on self-reported and memorized events. This group of participants was instead favoring prospective evaluation methods yielding unbiased information that does not rely on subjective evaluation criteria. The patient’s naivety towards the goal of the test and the avoidance of manual interference of the evaluator were also mentioned as necessary for objectifiable test results.
Sources of Information
Different sources of information were detailed by the participants reflecting the variety of strategies currently in use. While spontaneous use and dis-/non-use of the contralesional hand in daily life were among the most often mentioned points, the patient’s subjective perspective concerning his/her movement quantity and quality received less frequent mentioning. The most compound approach was delineated as a combination of the aforementioned, that is, data supporting both, the quantification of the non-use as well as the retained functional capacity (supplemental material box s3.4).
The target dimensions, which the participants focus on in the diagnostic process, can be differentiated into body functions, activities, and daily use. Qualitative and quantitative measures were explained to be mutually considered for the evaluation of the respective dimensions. Among the dimensions stated were those directly related to the upper extremity (hand/arm muscle strength, movement parameters, movement attempts) but also those related to gross motor function, overall constitution, and the cognitive domain (learning, attention).
The direct relevance of the dimensions listed in the answers to the concept of LNU was not always explained and seemed generic to the evaluation of sensorimotor function.
Differential Diagnosis
In order to differentiate the existence of the LNU phenomenon and exclude potential other symptoms, the participants mentioned established neurological, motor-functional, and neuropsychological tests. The leading indicator for the existence of the LNU phenomenon was considered the mainly behavioral phenomenon evidenced by the supposedly apparent discrepancy between spontaneous and forced use of the affected hand. Importantly, there was disagreement on whether the LNU phenomenon is at all differentiable from other syndromes such as motor neglect (supplemental material box s3.5).
Evidencing the Experience-Dependence of Learned Non-Use Symptoms
Depending on the prevailing assumptions about the underlying mechanisms of the LNU phenomenon, sensorimotor, mental, behavioral, and perceptive components were added by the participants to their description of the target dimensions. When investigating the participants’ assumptions regarding indications for the phenomenon’s origin in an experience- or learning-dependent process, it became apparent that no new information was added by the eight experts in the third round. Instead, it appeared as if the theory of the contribution of learning mechanisms to the phenomenon’s development was hardly questioned in itself (supplemental material box s3.6).
Consequently, the description of outcome parameters targeting this assumed learning process remained vague and was only outlined very superficially (supplemental material box s3.7).
The explicit question tailored to explore this aspect further (see supplemental material round 3 question 1) did not yield sufficiently new information aside from the potential quantification of the discrepancy of the spontaneous versus the forced use over time as a potential readout of experience-dependent change over time, which was mentioned already in preceding question rounds (supplemental material box s3.8).
Nonetheless, the lack of evidence for the experience dependence of the non-use behavior in patient populations received a critical evaluation, and the necessity to build a proof for this fundamental assumption was strongly emphasized.
There have been strong studies in rats and non-human primates that have characterized the learning process involved in learned non-use in the early period after CNS injuries. These are not paralleled by similar clinical studies. Such studies are desperately needed, both to firmly establish the degree to which learned non-use contributes to disuse and to start to reveal specific characteristics that could be used for differential diagnosis. [C6.r2]
Due to the saturation of the information acquired in response to this question, no further question round was initiated.
Discussion
In three rounds of the present Delphi study, consensus could be reached on a transdisciplinary definition characterizing the learned non-use phenomenon. While the key elements defining the actual gap between spontaneous use and functional capacity of the contralesional extremity as well as the experience dependence of this phenomenon were uncontentious among the participants, the role of the ipsilesional side was discussed controversially. In the original work building up to formulating the theory of learned non-use, Taub and colleagues observed and described the impact of the increased use of the ipsilesional upper limb in the unilaterally deafferented monkeys.5,9,10 While bilateral deafferentation led to the continuing use of the affected upper limbs, unilaterally deafferented monkeys had to be forced over a longer period of time in order to persistently reduce compensatory behavior. These observations are corroborated by later studies in rodents22-24 and monkeys25-27 employing cortical lesion models giving rise to some possible explanations for the underlying neural mechanisms.28,29 We therefore decided to include the aspect of compensation as an addition to the final definition to allow for a comprehensive characterization of the phenomenon.
The synthesis of the information related to the diagnostic process reflected the expected lack of a standardized clinical procedure to identify and differentiate the LNU phenomenon from other sensorimotor or neuropsychological phenomena. The participating experts did however agree on key elements required to optimally gather information building up to the identification of non-use in patients. Following the participants’ responses, the ideal diagnostic approach involves a multidisciplinary team of health professionals in addition to the patient and his/her relatives or caregivers in a longitudinal approach starting in the acute phase. Controversially discussed were the degree of objectivity of information sources available to identify the non-use behavior. While the contrast of the spontaneous against the forced usage was mentioned by mostly all participants, the actual modalities of testing were diversely described and miscellaneous measures and readouts were mentioned. In a small number of answers, concerns were raised as to whether LNU could be diagnosed and unequivocally differentiated from other related clinical pictures such as dyspraxia or hemineglect. It is necessary to point out that attempts to objectify LNU in patient populations have been made and used for experimental purposes,30-32 so far however, these rather elaborate approaches have not been implemented into clinical routine.
Obviously, LNU is still more of a so-called anecdotal clinical observation and not contained in the ICD-10 (International Classification of Diseases, Tenth Revision) systematic. Nonetheless, it is necessary to keep in mind, that therapeutic approaches like CIMT are originally legitimized with the non-use phenomenon. However, evidence is accumulating that CIMT, selected here as one example for current therapeutic approaches, is not effective in promoting recovery as a “one-fits-all” solution for every patient.13,33 Hence, in order to select the optimal therapeutic strategy for a patient, more knowledge is needed with regard to (1) the identification of the underlying mechanisms that bring about a certain clinical picture of sensorimotor dysfunction, (2) the subsequent stratification of the patient population, and (3) the response rate of a certain therapeutic approach in the presence of a selected sensorimotor dysfunction. These three points call for a wide range of basic and applied research in the field of rehabilitation.
Strikingly, the described diagnostic procedures currently in use lack a systematic verification of the experience dependence of the development of the LNU phenomenon. While it is necessary to acknowledge, that saturation of information in this regard may have not reached as quickly with a higher attrition rate in the third Delphi round, the experience dependence constitutes one fundamental element of the newly developed definition exposing an important disparity between underlying assumptions and their substantiation by clinical procedures. While learning mechanisms have been convincingly shown to contribute to non-use in animal models, this important proof is still lacking in human populations. First experimental work using immobilization paradigms in neurologically healthy human volunteers underscore as well as contradict34-36 the seminal work of Taub and colleagues. It is obvious that showing the gap between spontaneous and forced use only supports the assumption of a phenomenon of behavioral nature; it does not however allow to draw conclusions about the mechanisms that regulate its development.
Conclusion
In conclusion, we emphasize the need for the development of a structured diagnostic procedure including establishing its validity and reliability and its implementation in the clinical practice. This will allow the identification of patients showing or at risk to develop a non-use phenomenon. This step will improve clinical decision making and consequently lead to an optimized therapeutic intervention targeted at the functional recovery of the upper extremity following a brain lesion.
This step may also allow the transfer of elements of the diagnostic procedure to other clinical areas such as chronic pain or complex regional pain syndrome in which LNU like phenomena have been described. 37
Supplemental Material
sj-docx-1-nnr-10.1177_1545968321999064 – Supplemental material for A First Step Toward the Operationalization of the Learned Non-Use Phenomenon: A Delphi Study
Supplemental material, sj-docx-1-nnr-10.1177_1545968321999064 for A First Step Toward the Operationalization of the Learned Non-Use Phenomenon: A Delphi Study by Theresa Hirsch, Maria Barthel, Pauline Aarts, Yi-An Chen, Susanna Freivogel, Michelle J. Johnson, Theresa A. Jones, Marijtje L. A. Jongsma, Martina Maier, David Punt, Annette Sterr, Steven L. Wolf and Kirstin-Friederike Heise in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
We would like to thank all participants of the Delphi study for their commitment to our project, their time, and their motivation to share their knowledge and expertise.
Author Contributions
KFH conceived the research. TH, KFH, and MB developed the questions for the Delphi study throughout the whole study. TH implemented and executed the data collection and initial structuring of the data material. TH, KFH, and MB analyzed the data. KFH wrote the first draft of the manuscript, and KFH, TH, and MB revised the manuscript together. All other coauthors contributed with sharing their knowledge and experience in the Delphi study and commented on the initial and all revised versions of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Foundation Flanders (FWO) grant (1509816N) to KFH.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.