
Abstract
Background
Therapeutic dancing can be beneficial for people living with Parkinson’s disease (PD), yet community-based classes can be difficult to access.
Objective
To evaluate the feasibility and impact of online therapeutic dancing classes for people in the early to mid-stages of PD.
Methods
Co-produced with people living with PD, physiotherapists, dance teachers and the local PD association, the ‘ParkinDANCE’ program was adapted to enable online delivery during the COVID-19 pandemic. Participants completed 8 one-hour sessions of online therapeutic dancing. Each person was assigned their own dance teacher and together they selected music for the classes. A mixed-methods design enabled analysis of feasibility and impact. Feasibility was quantified by attendance and adverse events. Impact was determined from individual narratives pertaining to consumer experiences and engagement, analysed with qualitative methods through a phenomenological lens.
Results
Attendance was high, with people attending 100% sessions. There were no adverse events. Impact was illustrated by the key themes from the in-depth interviews: (i) a sense of achievement, enjoyment and mastery occurred with online dance; (ii) project co-design facilitated participant engagement; (iii) dance instructor capabilities, knowledge and skills facilitated positive outcomes; (iv) music choices were key; and (v) participants were able to quickly adapt to online delivery with support and resources.
Conclusions
Online dance therapy was safe, feasible and perceived to be of benefit in this sample of early adopters. During the pandemic, it was a viable form of structured physical activity. For the future, online dance may afford benefits to health, well-being and social engagement.
Introduction
Therapeutic dancing can be beneficial for people living with Parkinson’s disease (PD), yet community-based classes can be difficult to access and are not always tailored to individual needs.1-9 During the COVID-19 pandemic, there have been many times when people have been confined to the home setting. 10 Because people with PD have not been able to attend community-based dance classes or physiotherapy, a rapid rise in demand for online physical activities has occurred.11-14 In response, health professionals and community services have quickly pivoted to digital modes of therapy.15-17
Globally, trials on dance therapy for PD have been rapidly accumulating.18-24 Despite many studies on community-based dancing for PD, little is understood about the feasibility or impact of online dance for Parkinsonism and related disorders. One recent trial by Seidler et al. investigated the feasibility and effectiveness of group online adapted tango for people with PD. They reported that, in the initial stages of PD, online telerehabilitation classes could operate safely and effectively without in-person contact from a dance instructor. There were comparable benefits for balance and motor function for digital and face-to-face delivery. Virtual delivery is arguably a viable method for increasing access to an effective intervention for people with PD and other chronic health conditions. 14
In Australia, community-based ‘ParkinDANCE’ programs were adapted to online delivery during the COVID-19 pandemic. ‘ParkinDANCE’ is a structured therapeutic dancing intervention co-produced by people living with PD, physiotherapists, dance instructors, researchers from La Trobe University and Parkinson’s Victoria, Australia. ‘ParkinDANCE’ was originally implemented as a community-based group intervention. The aims of this mixed methods study were to explore the feasibility and impact on consumer experience and engagement of the transition to online delivery of ‘ParkinDANCE’, through the lens of people living with PD.
Methods
The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist 25 was used as a guide to ensure components of the qualitative study design were comprehensively reported. Reporting of the feasibility study was informed by the recommendations of Lancaster et al 201926,27 The online delivery was informed by guidelines from the 2020 Clinical Trials Project Reference Group. 28 Compliance with the Teletrials Compendium aimed to ensure that the rights, safety and well-being of all participants in this study were protected, consistent with recommendations in the Declaration of Helsinki. Ethical approval was granted by La Trobe University Human Ethics Committee (HEC18520). The study was registered a-priori and prior to publication on 14 October 2020 (ACTRN12620001042932).
Design
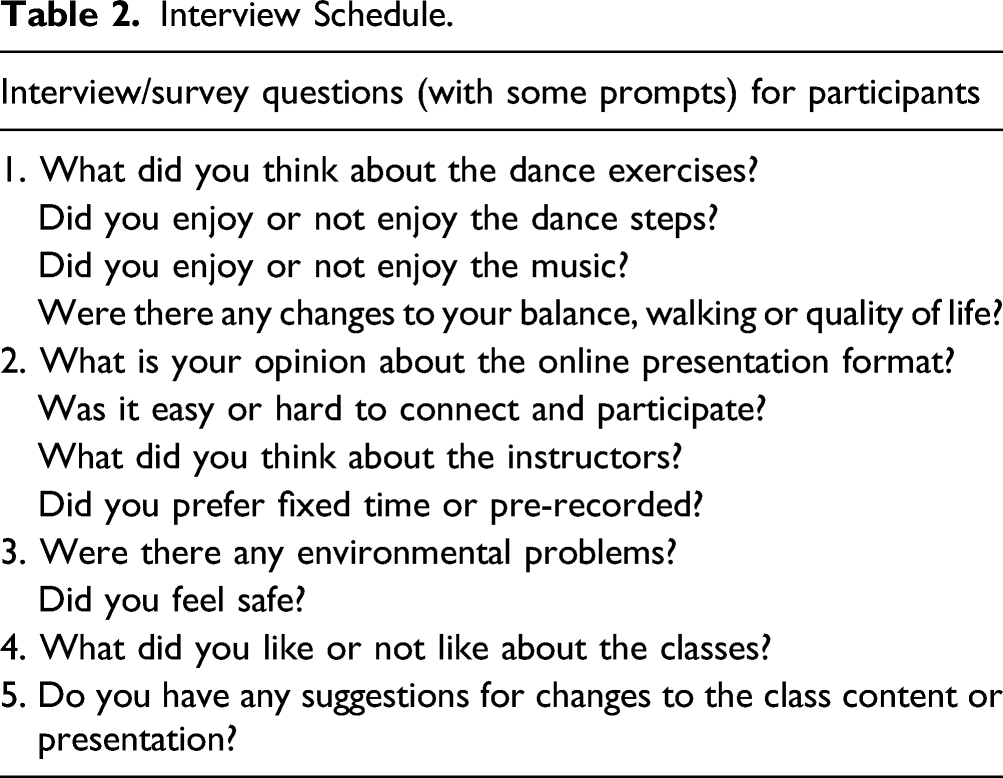
There were two parts to this investigation. A feasibility analysis was directed towards quantifying attendance and adverse events associated with digital dance classes. Adverse events were defined as any adverse medical or psycho-social occurrence or event in a PD participant during the dance classes, testing or trial, monitored by the dance teachers, research team and participants. Impact on consumer experience and engagement was determined from individual narratives that were analysed using qualitative methods through a phenomenological lens. The impact analysis used qualitative methods consisting of individual online semi-structured interviews 29 to explore the experiences of people with PD.
Participants
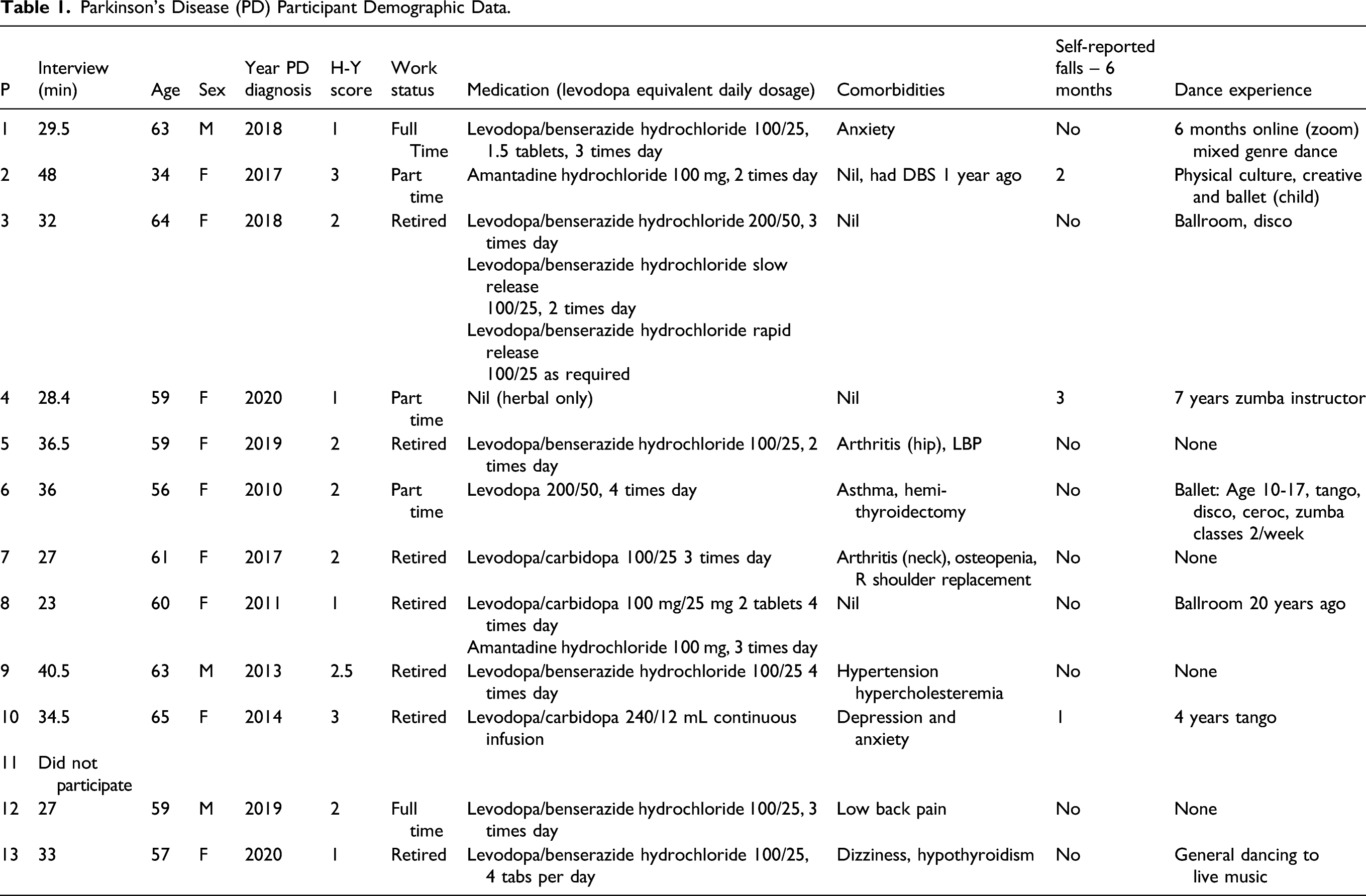
The dance participants were people living with idiopathic PD and dance instructors trained in ‘ParkinDANCE’. Thirteen potential dancers who expressed an interest were contacted and 12 agreed to participate in the online classes. The people with PD were eligible to participate in the online therapeutic dance if they met the following inclusion criteria: Hoehn & Yahr stages 0–3; 30 aged between 18 and 65 years; safe to do independent exercises, physical activities and dance steps in their own home, by themselves; no comorbidities or any other medical conditions that prevent safe exercise, by themselves, in their own home setting; willing to volunteer for a home-based telemedicine research trial; and have internet access and are willing to use it for the purpose of this trial.
Parkinson’s Disease (PD) Participant Demographic Data.
Recruitment
Convenience sampling 31 was used to recruit participants with PD. At the outset, we had a pool of people with PD who had expressed interest in a previously planned face-to-face therapeutic dancing study. The sudden changes brought about by the community restrictions caused by COVID-19 paused recruiting for the face to face ParkinDANCE clinical trial. At the same time, the online nature of delivery of this trial removed geographic restrictions enabling participants from regional and other areas to join. Potential participants were emailed a letter of invitation by the movement disorders nurse and followed-up with a phone call or email. They were provided with a project summary including the change to online delivery to facilitate access during COVID-19 restrictions. If participants expressed interest, they were checked for eligibility and emailed the Participant Information Statement, Informed Consent Form and project screening documents (medical release, doctor’s screening assessment, deidentified medical information and safety at home screening). These were completed, returned by email and transferred into a secure research drive.
The 4 qualified dance instructors were recruited using convenience sampling. They all had more than 10 years dance instructor experience and they were all trained in the ParkinDANCE methods. MEM and JW educated them in how to adapt dance programs taking into account the movement disorders and non-motor symptoms associated with PD. The PD dance instructors also attended weekly video-conference meetings with the project manager to develop choreography, provide further education about PD and establish measures to ensure safety. They were trained to ensure safety and access to a positive dance class, tailored to individual needs. A dance instructor manual was co-produced to standardise the class format and content. Class ‘dress rehearsal’ sessions were conducted for each dance instructor with either the project manager or another member of the research team acting as the participant.
Research Team
The research team included health professionals and clinical research experts in PD, physiotherapy, nursing, medicine and movement disorders (MEM, IB, JW, VM and MEH). It also included postdoctoral researchers with qualitative research skills (SCS and SH) and project management and exercise prescription expertise (SCS, MEM and JW). There were two blinded assessors (AB, KC), both who were registered physiotherapists expert in movement disorders. The members of the research team were not known to any of the participants.
Procedure
Prior to dance classes, a safety check of health and home safety was completed by each participant together with an assessor. The safety of furniture and equipment at home, and clothing and footwear, was carefully reviewed and emergency contact numbers, medications and health conditions were documented. Assessments of mobility, balance and quality of life were also performed.
Safety was also monitored using screening questions delivered by the dance instructors at the beginning of each dance class. They monitored responses to previous classes, environmental safety, clothing and footwear. The four dance instructors conducted the one to one online one-hour dance sessions twice a week for eight consecutive sessions. Online questionnaires were completed by each dancer and teacher immediately after each class and the dancers were re-assessed by the same movement disorders physiotherapist within one week after completion of the dance therapy intervention. All of the PD participants agreed to individual interviews via a video-conferencing platform following completion of the 8-session program. All data were entered into a password protected Redcap (Research Electronic Data Capture) 32 repository.
ParkinDANCE Online
The design of the online therapeutic dancing classes was co-produced with people living with PD, physiotherapists, dance instructors, researchers from La Trobe University and Parkinson’s Victoria. Parkinson’s Victoria is a not-for profit member organisation that provides research support and information, education, advice and peer support to people living with Parkinson’s, their families and health care professionals. The current study is the first to report the outcomes of ParkinDANCE.
People with PD performed carefully scripted dance steps and routines, at home, using the internet and connected in real-time to the dance instructors. Each ‘ParkinDance’ class lasted for 1 hour. The classes included a warm-up phase (5–10 minutes), an active dance and exercise phase (30–45 minutes) and a cool down phase (5–10 minutes). The warm-up phase included stretching and torso/limb mobility exercises, breathing and postural alignment. For the active phase, there was a mixture of dance steps, routines and genres (Tango, Irish, Tap, Salsa and Waltz etc.) and rhythmical music types, matched and personalized to the preferences of each participant and conducted in sitting, standing and travelling across the room. The cool down phase included stretching, breathing and relaxation. The participants completed 8 one-hour sessions of online therapeutic dancing. Each person was assigned to their own dance teacher and together they selected music for the classes.
A co-designed participant workbook provided advice for people living with PD on key elements on which to focus, for example, ‘focus on your feet; focus on the fast tapping of your fingers; focus on your breathing; focus on your balance and hold the chair…’ as well as how to safely structure the environment. The participants received a co-designed video-conferencing manual and IT orientation and used their own devices (computers or laptops) to access the online classes.
Data Collection and Analysis
Interview Schedule.
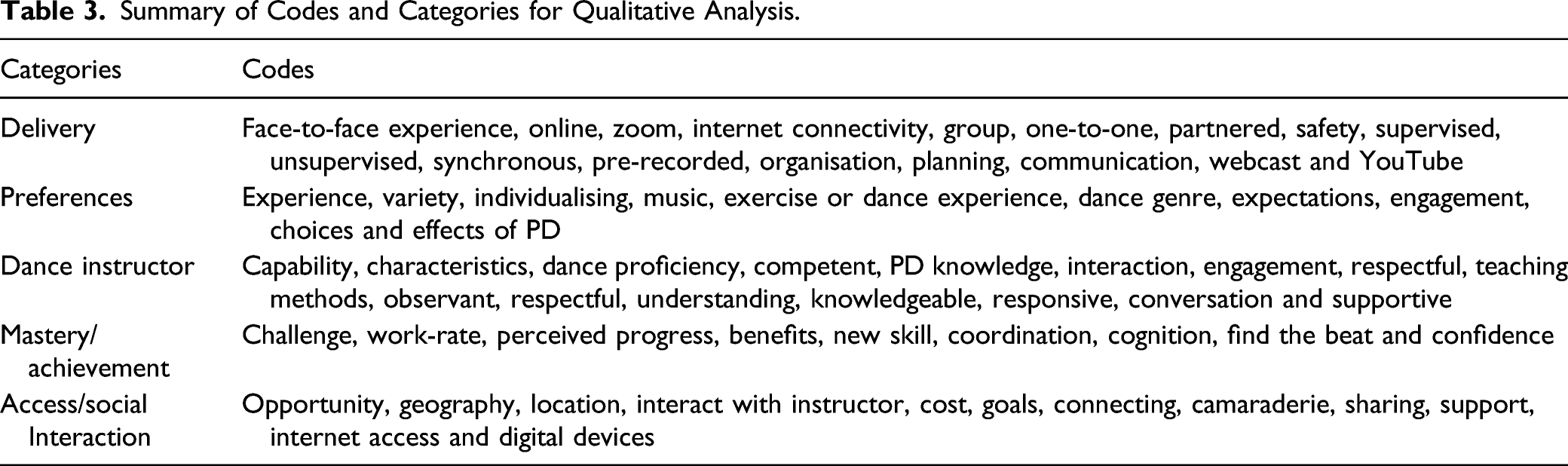
For the qualitative analyses, transcribed interviews were analysed by MEM, SS and SH inductively within a thematic framework. 29 The first step was independent familiarisation with the content by each analyst reading the transcripts and making field notes. A thematic framework was then created for the transcripts, with each researcher independently recording a ‘code’ against what was described or thought to be important. The qualitative data were interpreted, in order to identify emergent connections, concepts or themes, and by comparing across rows, columns, and sections, to identify patterns, characteristics or constructs. After discussing the findings, the final ‘codes’ were agreed upon and incorporated into ‘categories’. 33 The remaining transcripts were coded and categorised, and video-conference meetings were held to discuss convergence and divergence and reach consensus. Preliminary themes were developed, and two consensus meetings were held with a third researcher (MEM) to finalise the themes and select a smaller number of the most representative quotations. When categories were finalised, a document was created for each category and all related participant quotations were entered to support the categories. A consensus meeting was held to select a pool of representative quotations. Minutes of all meetings were stored on the research drive.
Risk of Bias in Qualitative Analyses
Control of risk of bias for the qualitative data was enhanced by a priori eligibility criteria. We also ensured that participants had a range of experiences to answer the research question. There were reproducible data collection and analysis procedures, audio-recording and verbatim transcription. All data were independently analysed by at least two researchers, with acknowledgement of potential researcher bias. There was team consensus and all findings were supported by data from participants.34,35
Theoretical Framework for the Qualitative Analysis
Summary of Codes and Categories for Qualitative Analysis.
Results
ParkinDANCE Online was found to be highly feasible in this group of early adopters. Attendance was high, with dancers attending 100% sessions. Three participants each experienced one incident of internet outage, but they rescheduled and completed all of the eight classes. Compliance with the protocol was excellent with all except one post-class survey completed by the dancers and all surveys completed by the dance instructors with data confirming that the dance classes were delivered as planned. There were no safety issues or adverse events.
Five themes were identified in the qualitative data: (1) a sense of achievement, enjoyment and mastery occurs with dance; (2) participant experience and preferences influence engagement; (3) there are important dance instructor capabilities, knowledge and skills that are key to successful participant engagement; (4) music choices facilitated engagement and enjoyment; and (5) participants were able to quickly adapt to online delivery of therapeutic dancing. The themes are elaborated in the text below, and are supported by quotations from the participant data and accompanying participant code and transcript line numbers.
Theme 1: A Sense of Achievement, Enjoyment and Mastery
All of the participants reported their self-confidence improved by mastering dance steps and sequences (Text box 1). They also felt more able and motivated to venture into public spaces for other forms of physical activity. Many reported being physically and mentally challenged by the dance activities yet had a sense of accomplishment with their perceived progress. There was a feeling that the dance steps and sequences were appropriately tailored to their capability (Text box 1).
‘It gave me more confidence to go “Well, I can stand up and dance and learn a dance move and not fall over”… I’m quite hesitant about going for my morning walk because I’m as stiff as a board or I can’t move properly, and it just gave me a bit more confidence to approach those things’ P2, line 83, 101.
‘It’s just nice dancing. And I used to dance when I was younger and slowly but surely Parkinson’s took everything away from me and I was turned into a shuffler when I danced, one of those people who just stays in the same spot. And it was just nice to be encouraged that this is something I can do’ P2, line 63–67.
‘I found that combination both doing the exercise, which wasn’t too aerobic – so you had to count the steps and you had to think about what move you’re doing – I found that whole process to be really good, to be beneficial…we were doing different steps, so she got me thinking the whole time. I think that cognitive aspect to the whole procedure was really good’ P12, line 44–46, 51.
‘You’re developing a skill, you’re learning something new and whenever you want to learn something new most people will feel good about it. You have that kind of satisfaction, the feel good factor’ P12, line 4102.
‘I was already interested in doing movement since the diagnosis of Parkinson’s, because I could understand, I could feel that that would be a good thing to do. Learning a dance genre is really challenging but I really like the challenge’ P13, line 20–22.
Each of the participants indicated recognition that achievement and skill acquisition can promote motivation, confidence and a flow-on effect into activities of daily living. When they perceived improvement, it acted as a catalyst to continue participation and improved their self-image as an active and independent person (Text box 2).
‘Once the body starts failing it really wreaks havoc on your self-confidence… I think the dancing is really good… I really think it has a place for people who’ve lost a lot of self-confidence’ P2, lines 139, 145.
‘I would not do my exercises or go for a walk beforehand, but afterwards (after dancing) I felt like I could because I’d kind of achieved something…It (dancing) was kind of like that starter motor starting or getting me started to face the day’ P2, line 335, 338.
‘It put me in touch with what I’m capable of doing…It’s a bit of a confidence booster’ P7, line 165, 178.
‘I think just doing the dance steps, putting it all together…I think I felt boosted by it… the achievement of steps and that kind of thing, and just the connection’ P8, line 271.
‘I noticed it afterwards, after doing the class. For over an hour or so afterwards it was ... almost like you were continuing that flow of dance…, it was a lot more of that freedom of movement… I wanted to move around. I’d go out and do some gardening and things like that as well too, because it felt like the body was still relaxed’ P9, line 113–115.
‘I think it’s just getting that confidence and that feeling of safety, especially if you haven’t done it for a long time or ever done it…What I learnt from and picked up in the dance classes you do actually introduce back into other parts of your life and sometimes without even really realising it. It was good’ P9, line 275–276.
‘I think waltzing or slow dancing helps build that confidence at the start and then you can progress to more steps or changing of steps in the same dance routine. Then you can challenge yourself a little bit more and that’s part of continuing to do it too. You embrace it and it challenges you and that’s great’ P9, line 381–383.
All reported that participation and exposure to different dance genres and progression of complexity are achievable with online dance delivery (Text box A in Supplemental Material).
Theme 2: Experience and Preferences Influence Engagement
The participants indicated that familiarity with dance, either before or after their PD diagnosis, helped to prepare them for what to expect about online dance exercises. It also helped them to participate with confidence. Those who did not have any experience of dance had some concerns about what they would have to do and how they well they would perform. Many had participated in face-to-face dance classes and were keen to pursue online delivery one-to-one with a dance instructor during the COVID-19 pandemic (Text box 3; Text box B, Supplemental Material).
‘I just like dance I suppose and music and I’ve often thought, “I wouldn’t mind doing some dancing classes,” so it’s an opportunity that came up and it’s great, especially I suppose in lockdown, it was something to look forward to’ P3, line 25–28.
‘I personally probably would enjoy the classes more with other people than on my own, but initially I actually thought it was really nice having that one-on-one. It’s a bit of a treat, really’ P6 line 300–302
‘I really enjoyed it. I wasn't sure what to expect at the start and that was more from my perspective of myself rather than the dance class…I used to do dance classes many years ago with friends and that. Just a social thing and we enjoyed them’ P9, line 30, 34.
‘I didn't feel I missed anything by doing it on the internet and not in a physical dance studio other than having a partner’ P9, line 174–175.
Each person with PD reported that it was important to have fun and variety; dancing was a way to participate in enjoyable physical activity. The range of dance genres, such as tango, ballet, salsa, hip-hop, ballroom and modern, provided an opportunity for participants to experience variety. They also expressed a desire to try different types of dance and to be challenged. A consistent preference was for an individualized or tailored approach, to factor in past experience of dance and disease progression. There was also a strong preference for a variety of music and dance genres, though not necessarily pre-selected by the participant (Text box B, Supplemental Material; Text box C, Supplemental Material).
Theme 3: Dance Instructor Capabilities, Knowledge and Skills that are Key to Successful Participant Engagement are Key
All participants identified dance instructor qualities and skills that enabled them to engage in therapeutic dancing. These included a perception of dance proficiency, teaching skills and the ability to communicate positively, with respect, empathy, patience and understanding, and to make the dance sessions fun and challenging. Participants were particularly appreciative of the social support (eg, humour and small talk) provided by dance instructors within the context of widespread COVID-19 restrictions (Text box 4).
‘She was easy to understand, easy to follow, patient and knew what she was doing. She clearly had extensive experience in the dance moves’ P7, line 22–24.
‘He led the class very well and we warmed up, we did the dance and then we warmed down. I felt like at the end we got on top of the movements’ P8, line 123-4.
‘I got along really well with her, which was very easy… I found something useful out of the interaction with her because she spent me enough time to talk about it, not just the dance itself’ P10, line 124–125.
‘I became more comfortable with it, over time, and I think that has a lot to do with the instructor. I felt we had a rapport which really helped’ P12, line 86.
‘It was nice to have her modelling the kind of thing, something to aspire to. She did it with ease. Obviously, she’s really good at it’ P12, line 215–216.
‘The more important thing and the way she conducted herself, she was fantastic and for me, it was more just the way that they conducted themselves. They put everything at ease… they were just comfortable with the whole thing’ P12, line 330–333.
All of the participants expressed a preference for the dance instructors to have knowledge about movement disorders and PD, and to demonstrate their understanding of symptoms and fluctuations by appropriately tailoring dance exercises (Text box D, Supplemental Material). They felt that it was important to feel confident and safe with the dance instructor (Text box E, Supplemental Material).
Theme 4: Music Choices Were Important
The music selected by the instructors was important for enjoyment, motivation and to guide movement. A clear beat was key (Text box 5).
‘I liked it and I liked the fact that I could find a beat every time… I could coordinate my next–like if I lost it, I could find it' P2, line 272.
‘It was initially challenging for me to slow right down and do the Rumba. I really enjoyed the music that he played. Initially I was like a duck out of water because it was so slow and it’s like I’ve never had to concentrate so much because I am–at times I can be a little bit stumbly but–and I’m not that way when I dance fast. But ... having to slow it down - it challenged me and I love a challenge' P4, line 82–87.
‘The music, you can actually do different tempos to it so I might be going faster. You could be going one, two and I can go one, two three, one, two, three. You're going one, two, one, two but you can do it because the music allows you to pick those different speeds' P9, 299–302.
‘But the things I enjoyed about it is really just all the footwork and just trying to keep to the beat of the music. I’m not a musical person – I felt a bit uncoordinated. But as it went on, I really enjoyed it' P13, 125–126.
There were individual preferences for music genre and many people liked having input into the music selected. Participant input into the music selected was directly solicited by the instructors (Text box F, Supplemental Material).
Theme 5: Participants Quickly Adapted to Online Delivery
Moving from face to face to digital delivery helped with access to dance therapy, especially during the COVID-19 pandemic and for regional and rural participants. People could quickly adapt to this modality (Text box 6).
‘I live rurally and so there’s no way I could have taken part in this in any form… for me as someone who lives in a regional area that has been invaluable and I’m really lucky’ P13, line 72.
‘I live in a rural area it’s just been amazing to be connected in this with technology. If that’s what technology’s done well, yay’ P13, line 404.
‘Zoom might be good for people that aren’t in the metro area that can’t get to things especially’ P1, line 313.
‘I'd say, on reflection, those days seemed a little bit more spritely where I had engaged with someone because of the lockdown and things like that, so I'd say that my dancing days were a bit more upbeat’ P7, line 88–90.
‘I didn't feel I missed anything by doing it on the internet and not in a physical dance studio other than having a partner’ P9, line 174–175.
‘Having more contact with people during this COVID season–she’s one of those that I have never met before and I was able to connect with. And it should work on Zoom in the future as well, for other people. But for myself, it worked’ P10, line 64–65.
Online delivery provided a regular interaction and time commitment with a dancing instructor, who in turn had close communication with the research team (Text box E, Supplemental Material). Through the assessment and safety screening the participants developed an understanding of the need to have a safe environment. They also valued the dance instructors conducting safety checks before and during each session (Text box F, Supplemental Material). Online delivery also highlighted the need for stable internet services, access to digital devices such as personal computers or tablets, IT literacy and access to technical support (Text box G, Supplemental Material).
Discussion
The over-arching theme to emerge from this trial was that online therapeutic dancing has impact and is enjoyable, safe and feasible for people in the early stages of PD. In agreement with global studies showing the benefits of ‘face to face’ dancing for people with chronic progressive neurological conditions,20,39-43 the participants in this study reported that online dance therapy enabled them to connect with others and engage in structured physical activity that was of benefit to health and well-being.
One of the benefits of ParkinDANCE Online was engagement in therapeutic exercise. Earhart (2009) 44 reported that dance includes most of the recommended components of exercise for people with PD, such as cueing, facilitating transfers, improving balance and training strength and mobility. A recent study by Fontanesi and DeSouza (2021) 45 compared dance to exercise of matched intensity, showing that therapeutic dance for PD improves walking and the perception of self-efficacy (eg, ‘I can move well’). Self-efficacy in people with PD has been previously reported to be strongly associated with engaging in the regular and sustained exercise46,47 necessary to reap associated benefits including increased fitness, strength and quality of life. The findings of this study align with that viewpoint.
In addition to being effective, exercise interventions for people with PD need to be feasible to implement. Dance classes in locations other than home may be a barrier to attendance. Even though face-to-face community dancing has strong evidence of benefit1-5 it is not always accessible. Two studies that included home-based interventions aimed at improving physical function in people with PD, showed them to be feasible,3,48 with high levels of compliance. A feasibility study that investigated a 5-week ‘in home’ DVD-based program of tango dancing for 10 people living with PD reported improvement in measures of motor skills and quality of life. 49 The authors concluded that despite these positive findings, home-based activities using pre-recorded class activities may not be able to substitute for all the beneficial characteristics of a live class such as the teacher-participant connection and immediate, online feedback. These aspects of our program were highly rated by participants. Because it was ‘live’, our online program delivery model can provide both the benefits and convenience of an in-home dance class together with many of the benefits of a group class.
Co-production of the content and implementation of the dance classes was key to success. People living with PD and Parkinson’s Victoria contributed at each step of setting the research questions, designing the online classes, producing the instruction manuals for people with PD, dance teachers and blinded assessors and implementing the classes online. The implementation sciences literature illustrates the power of genuine co-production and collaborative research in achieving outcomes for individual health and well-being as well as impact for society. Heaton et al proposed that closer collaboration provides the opportunity to produce knowledge together with other key stakeholders that can be readily translated into practice overcoming barriers to implement. 50 In our study, the principles of co-production proposed by Heaton were reflected in the qualitative findings. Having a sense of achievement, close mutual engagement, leadership capabilities, choice and facilitated adaption to a new online delivery captured these co-production principles. There was equity amongst stakeholders, reciprocity and mutuality. Technology, including telehealth and telecare delivery, became more prominent in 2020 due to the disruption caused by social distancing. 51 Our study demonstrated the benefits and impact of adapting the face to face program into a telehealth platform, through co-production.
The qualitative analyses also highlighted the skills, social connections and enjoyment that occurred when engaging with online dance. This arts-health initiative afforded creative expression and enjoyment of the artform, in addition to opportunities for structured exercise and therapeutic movement.52,53 The dance classes used evidence-based therapies such as cueing,54-56 attention strategies57-60 and strengthening58,61 to improve movement control. Care was taken to train the dance instructors, to ensure that they understood the movement disorders associated with PD and how to modify dance steps and routines to ensure safety and benefit.4,22 Music choices were key, as has been shown in trials on singing for PD 62 and music-cued movement for people living with Progressive Supranuclear Palsy (PSP) 42 and dementia. 43
There were several limitations of this investigation. Because we rapidly pivoted from community-based dance classes to online dance therapy, we deliberately tested implementation in a comparatively small number of early-adopters who had mild symptoms associated with PD. Therefore, the sample size of 12 was modest. Further trials are needed to test the feasibility and impact of ParkinDANCE in larger samples of people with PD, including those with more extensive motor symptoms and non-motor symptoms. The participants were in the early to middle stages of PD and under the age of 65 years. It is not clear if this digital modality would be as effective in very elderly people, those with advanced PD or people who are frequent fallers. In addition, we did not attempt to control for PD medications such as levodopa. Dance participants were not available to provide feedback on the written findings. Although each class was held at peak dose of the morning PD medications, the relative contribution of medications and therapy to outcomes awaits verification. This trial included English-speaking participants and there is a need for implementation with a diverse range of people from different cultures, capabilities and comorbidities. Finally, we were not able to directly compare the outcomes of online vs face-to-face modes of delivery as the community classes were paused due to COVID-19 and the evaluations of the face-to-face classes has recently resumed. A strength is that the project follows recommendations for reporting non-randomized pilot and feasibility studies by Lancaster and Thabane(2019) 26 and COREQ reporting guidelines for qualitative studies. 25
Conclusion
To conclude, individuals living with PD were able to quickly adapt to online delivery of the ParkinDANCE program when provided with support and resources, as well as access to classes run by credentialed dance instructors. The one-to-one online format is recommended as a beneficial and engaging form of therapeutic exercise, particularly when access is a priority.
Supplemental Material
sj-pdf-1-nnr-10.1177_15459683211046254 – Supplemental Material for Online Dance Therapy for People With Parkinson’s Disease: Feasibility and Impact on Consumer Engagement
Supplemental Material, sj-pdf-1-nnr-10.1177_15459683211046254 for Online Dance Therapy for People With Parkinson’s Disease: Feasibility and Impact on Consumer Engagement by Meg E. Morris, Susan C. Slade, Joanne E. Wittwer, Irene Blackberry, Simon Haines, Madeleine E. Hackney and Victor B. McConvey in Neurorehabilitation and Neural Repair
Supplemental Material
sj-pdf-2-nnr-10.1177_15459683211046254 – Supplemental Material for Online Dance Therapy for People With Parkinson’s Disease: Feasibility and Impact on Consumer Engagement
Supplemental Material, sj-pdf-2-nnr-10.1177_15459683211046254 for Online Dance Therapy for People With Parkinson’s Disease: Feasibility and Impact on Consumer Engagement by Meg E. Morris, Susan C. Slade, Joanne E. Wittwer, Irene Blackberry, Simon Haines, Madeleine E. Hackney and Victor B. McConvey in Neurorehabilitation and Neural Repair
Supplemental Material
sj-pdf-3-nnr-10.1177_15459683211046254 – Supplemental Material for Online Dance Therapy for People With Parkinson’s Disease: Feasibility and Impact on Consumer Engagement
Supplemental Material, sj-pdf-3-nnr-10.1177_15459683211046254 for Online Dance Therapy for People With Parkinson’s Disease: Feasibility and Impact on Consumer Engagement by Meg E. Morris, Susan C. Slade, Joanne E. Wittwer, Irene Blackberry, Simon Haines, Madeleine E. Hackney and Victor B. McConvey in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
We acknowledge and thank all of the participants, dance teachers and physiotherapy assessors who contributed to the rapid implementation of this online project, as well as Parkinson's Victoria for supporting and co-producing this project. ParkinDANCE is trademarked with Parkinson’s Victoria and La Trobe University.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Parkinson’s Victoria (Australia) and La Trobe University Australia.
ORCID iDs
Supplemental Material
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.