
Abstract
Background. Controlled whole-body vibration (CWBV) training has been applied to people with stroke. However, it remains inconclusive if CWBV reduces fall risk in this population. Objective. To (1) assess the immediate and retention effects of CWBV training on fall risk factors in people at postacute and chronic stages of stroke and (2) examine if CWBV dosage is correlated with the effect size (ES) for 3 fall risk factors: body balance, functional mobility, and knee strength. Methods. Twelve randomized controlled trials were included. ES was calculated as the standardized mean difference, and meta-analyses were completed using a random-effects model. Results. CWBV training may lead to improved balance and mobility immediately after training (ES = 0.27, P = .03 for balance; ES = 0.34, P = .02 for mobility) but not at the 3-month follow-up test (ES = 0.02, P = .89 for balance; ES = 0.70, P = .11 for mobility). CWBV affects knee strength capacity with mild ES (ES = 0.08 and 0.11, respectively, for immediate and retention effect; P ≥ .68 for both). Metaregression indicated that the immediate ES is strongly correlated with training dosage for balance (r = 0.649; P = .029) and mobility (r = 0.785; P = .036). Conclusions. CWBV training may benefit balance and mobility immediately, but the training effect may not persist among people with stroke. Additionally, the CWBV dosage correlates with the ES for body balance and mobility. More high-quality studies are needed to determine the retention effects of CWBV training.
Keywords
Introduction
Approximately 3% of the adult population in the United States suffers a stroke. 1 Falls are common in people poststroke and result from disease-induced decline of neuromotor performance, such as muscle weakness, balance impairment, mobility limitation, and sensation loss. 2 Up to 73% of stroke survivors have experienced at least 1 fall in the preceding 6 months. 2 As many as 15.9 of every 1000 persons with stroke fall daily. 3 These falls result in physical injury or death, with fracture rates up to 4-fold higher than in the general population. 4 Falls also impose significant burdens psychologically (eg, developing anxiety and fear of falling 5 ) and economically (eg, incurring large medical costs). Among individuals with stroke, the health care costs for those with falls in the past year are significantly higher than those without ($26 648 vs $16 909 per person). 6 Recent reviews concluded that high-quality research is needed to develop evidence-based fall prevention paradigms for individuals poststroke.5,7 Various exercise-based fall prevention training programs have been developed, with a range of outcomes being reported.5,8
Controlled whole-body vibration (CWBV) training emerged as an alternative to improve neuromuscular functions and fall risk in the physical therapy field.9-11 In general, during CWBV, trainees stand on a vibrating platform. Two main types of vibrating platforms exist: side-alternating (oscillating) and vertical (linear). 12 Both platforms primarily create vertical mechanical oscillation. The transmission of such mechanical vibrations to the human body causes the tonic vibration reflex (TVR), a complex spinal and supraspinal neurophysiological reaction.12,13 The TVR increases muscle activation and improves functional performance.14-16 CWBV has been applied to people with stroke; however, the conclusion regarding the effects of CWBV in reducing the risk of falls among this population is mixed.17-22 For example, a meta-analysis found no effect of CWBV on functional performance in stroke patients (effect size [ES]: 0.15 and P = .30 for knee strength; 0.23 and P = .74 for body balance, and 50.40 and P = .14 for gait performance). 18 Another meta-analysis reported varied ES of CWBV training in improving body balance (ES: 0.08, P = .91), muscle strength (0.23, P = .36), and mobility (0.45, P = .33) in stroke. 21 A later meta-analysis in stroke survivors documented mild to moderate ES of CWBV on body balance (ES: 0.28) and knee strength (0.16) in favor of CWBV. 19 Given that CWBV is becoming an increasingly popular therapeutic modality, 10 learning more about the overall effects of CWBV is highly relevant and meaningful to the rehabilitation field.
Several factors could lead to biases in meta-analysis results and contribute to the inconsistency in findings among prior studies.18,19,21 First, some of the previous meta-analyses included a very small number (2-4) of studies.18,21 Second, the calculation of the ES in previous publications was based on the difference in the posttraining outcome measure between groups.18,21 Such an approach creates bias when the baseline measurements are imbalanced between groups. Third, 2 meta-analyses combined investigations that examined the acute effect after a single CWBV session and the short-term effect after weeks of CWBV training.19,21 This increases the heterogeneity between studies and may lead to biased results. Finally, no meta-analysis examined the retention of the CWBV training effect. Because the retained training effect is critical for avoiding falls, conclusions obtained from previous meta-analyses could be incomplete. New CWBV-based randomized controlled trials (RCTs) in stroke have been conducted recently, and an updated and more comprehensive meta-analysis with rigorous calculation of ES is needed to clarify the effects of CWBV training on changing fall risk factors in people with stroke.
Another previously overlooked issue is the relationship between CWBV training dosage and the degree of improvement in fall risk factors among individuals poststroke. Dosage is important in designing CWBV-based fall prevention programs. Recent work postulated greater improvements in outcomes following longer training duration, more training sessions, or more intense vibration stimulation in stroke. 23 However, there are 2 possible issues associated with this postulation. First, no direct data support this notion so far. Second, the training dosage in previous studies was largely represented either by the number of sessions 23 or the level of platform acceleration.24,25 These results have led us to further explore a novel measurement that combines both the training duration and the platform acceleration to reflect the training dosage. It would be of interest to examine how this new dosage interacts with the training effect based on the published RCTs.
Our purpose was to try to clarify the effects of CWBV in altering the fall risk factors among people poststroke. Specifically, we sought to determine (1) whether CWBV improves body balance, functional mobility, and lower limb muscle strength and (2) if the effect from CWBV training correlates with the training dosage in stroke. Because the 3 fall risk factors are closely related to falls in people with stroke, our findings will provide critical evidence for the rehabilitation field to design CWBV-based fall prevention interventions for this population.
Methods
Research Question
Our goal was to determine the immediate and retention effects of CWBV in improving 3 fall risk factors among people with stroke at postacute or chronic stages within the PICO (patient, intervention, comparison, and outcome) framework. 26 The patient (P) was defined as an individual with postacute or chronic stroke. The intervention (I) was CWBV training, which was delivered to the experimental or training group. The experimental group was compared (C) with the control group, which did not undergo CWBV training. The outcomes (O) were defined as the changes in fall risk factors from pretraining to the posttraining assessment (for the immediate effect) and from pretraining to the follow-up assessment (for the retention effect).
Systematic Review
A thorough search of the literature was performed conforming to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) statement. 27 We searched for the effects of CWBV on 3 fall risk factors: body balance, functional mobility, and muscle strength. Body balance was quantified by the Berg Balance Scale Test, Mini Balance Evaluation Systems Test, or the Sensory Organization Test; functional mobility was measured by the Timed-Up-and-Go Test or the Timed 10-Meter Walk Test; and strength measurement was the isometric knee extensor strength capacity on the paretic side. Our search began with November 2018 and continued through March 2019. PubMed, Web of Science, ProQuest Dissertation and Theses, and Google Scholar databases were searched. The search terms and strategy used were as follows: (vibration training OR WBV OR CWBV) AND (stroke) AND (randomized controlled trials OR RCT).
Study Inclusion and Exclusion Criteria
Studies meeting the following criteria were considered for review: the study (1) was conducted among individuals at the postacute or chronic stage of stroke recovery prior to the enrollment; (2) was a RCT, meaning that the participants underwent CWBV training in 1 arm of the RCT and placebo/sham/conventional treatment/other exercise programs in the other arm; (3) assessed the short-term (multiple CWBV sessions over at least 2 weeks) therapeutic effect instead of the acute (a single CWBV session) effect of CWBV; (4) examined at least 1 of the 3 fall risk factors of interest; and (5) was published in English. Studies were excluded if participants had any other neurological diagnoses (eg, Alzheimer or Parkinson disease, multiple sclerosis, and spinal cord injury). No published abstracts were included to ensure the rigor of the meta-analysis.
Selection of Studies
A total of 265 publications were originally identified through database searches and review of article reference lists (Figure 1). After removing duplicates and excluding publications in terms of the inclusion and exclusion criteria, 12 articles between 2006 and 2018 were included in the analysis.
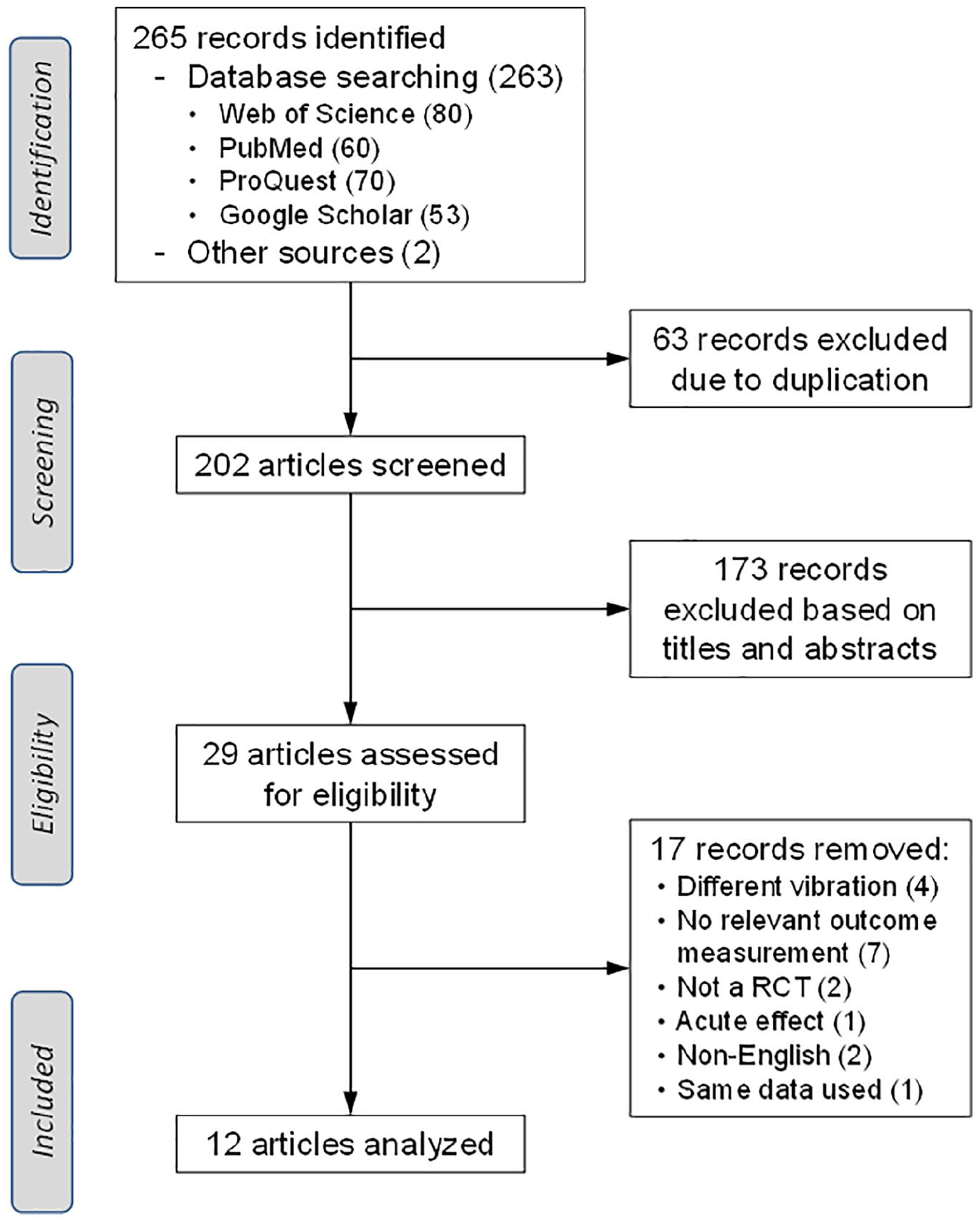
A flow diagram of the number of studies identified, the number excluded and the reason for exclusion, and the final number of studies included in the systematic review and meta-analysis.
Study Quality Assessment and Data Retrieval
All 12 publications were assessed for quality based on the Physiotherapy Evidence Database Scale 28 independently by 2 authors. An average ± SD score of 6.5 ± 1.8 out of 10 points was obtained. Of the 12 trials included in the meta-analysis, 4 conducted a follow-up test approximately 3 months after the initial assessment.29-32 We included the 3-month follow-up assessment in the meta-analysis.
For the meta-analyses, the values for measurements of body balance, mobility, and knee joint muscle strength were extracted in the form of means, SDs, and sample sizes for both the training and placebo conditions at 3 time points (pretraining test, posttraining test, and follow-up test if applicable). The change in fall risk factors from the pretraining to posttraining test (for immediate effect) and from pretraining to the follow-up test (for retention effect), if not given by the article, were calculated from the identified mean and SD, or range, or 95% CI.
We extracted information regarding the frequency and amplitude of vibration, the duration of each training bout, number of bouts within each training session, the weekly frequency of the training session, and the number of weeks for the entire training course. The maximum vibrating platform acceleration was calculated as a = A(2πf)2 (where a is the peak acceleration in m/s2, A the amplitude in m, and f the frequency in Hz or 1/s).12,33 The peak platform acceleration was then expressed as multiples of the gravitational acceleration (g = 9.81 m/s2). The total duration of CWBV exposure (d) was calculated as the product of the duration of the bout, number of bouts per session, weekly frequency of training sessions, and the duration of the entire intervention. The total vibration duration was then converted into hours (number of hours = h). Finally, the peak platform acceleration was multiplied by the total vibration duration to formulate the CWBV training dosage (DS in h•g) for each study: DS = d × a.
Meta-analyses
ES is referred to as the standardized mean difference (SMD), which provides the measurement of differences in the mean outcome after the intervention. 34 The ES was used to determine the immediate and retention effects CWBV had on the 3 fall risk factors. Data collected from the studies were entered into the ES calculator using Review Manager (RevMan) 5.3 software (Nordic Cochrane Centre, Denmark). 35 The data entered into RevMan included the extracted sample size and mean and SD values of the changes in fall risk factors from the pretraining to posttraining test (for immediate effect) and from the pretraining to retention test (for retention effect). The SMD was then calculated using the identified changes in each study. RevMan calculates the statistical significance of the difference between the means and 95% CIs for the mean between-group difference. ES estimates were then combined across studies to obtain a summary statistic.
The results of meta-analyses were presented using forest plots. We quantified the heterogeneity of the included studies using the I2 statistic, which describes the percentage of variation across studies resulting from heterogeneity. The random effects model was used for the meta-analyses. 35 Publication bias was not investigated with funnel plots because there were fewer than 10 publications for each fall risk factor in the meta-analyses because the test power is typically too low to distinguish the change from real asymmetry. 36 Meta-regression analyses were conducted to determine the correlation between the immediate ES and CWBV dosage (in h•g) for all 3 fall risk factors.
Results
The literature search of databases identified a total of 265 studies (Figure 1). After the removal of duplicates (63) and titles or abstracts not pertaining to the research purpose (173), 29 potentially relevant articles were identified. From these studies, 13 matched the inclusion and exclusion criteria. Among the remaining 13 articles, 2 were based on the data collected from the same trial.31,37 One of the 2 articles was excluded to avoid possible duplication publication bias, yielding 12 studies included in this meta-analysis.
A total of 447 participants were tested in the 12 studies (Table 1). Among them, 256 and 161 were male and female patients, respectively; the sex for 30 participants was not specified. 38 Average age of the participants ranged from 53.8 to 74.5 years (Table 1). People with both ischemic and hemorrhagic stroke were included (Table 2). The right side was affected by stroke among 187 participants and the left side in 152 participants. The affected side was not specified for 108 participants (Table 2). Three studies examined the effects of CWBV on fall risk factors in the postacute phase of stroke,39-41 and the remaining studies focused on the chronic stage. Interventions adopted for the control group included no treatment, 30 sham24,29,31,38,42 or low-intensity vibration, 43 routine physiotherapy,39,41,44,45 and exercise therapy with music 32 (Table 3). The duration of the intervention spanned between 3 weeks 44 and 12 weeks. 42 The vibration frequency and amplitude varied from 5 Hz 42 to 45 Hz 39 and from 0.44 mm 31 to 4 mm,29,38,39 respectively. The peak platform acceleration ranged from 1g 38 to 25g. 29
Demographic Information About Participants for Each Trial Included in the Current Meta-analysis.
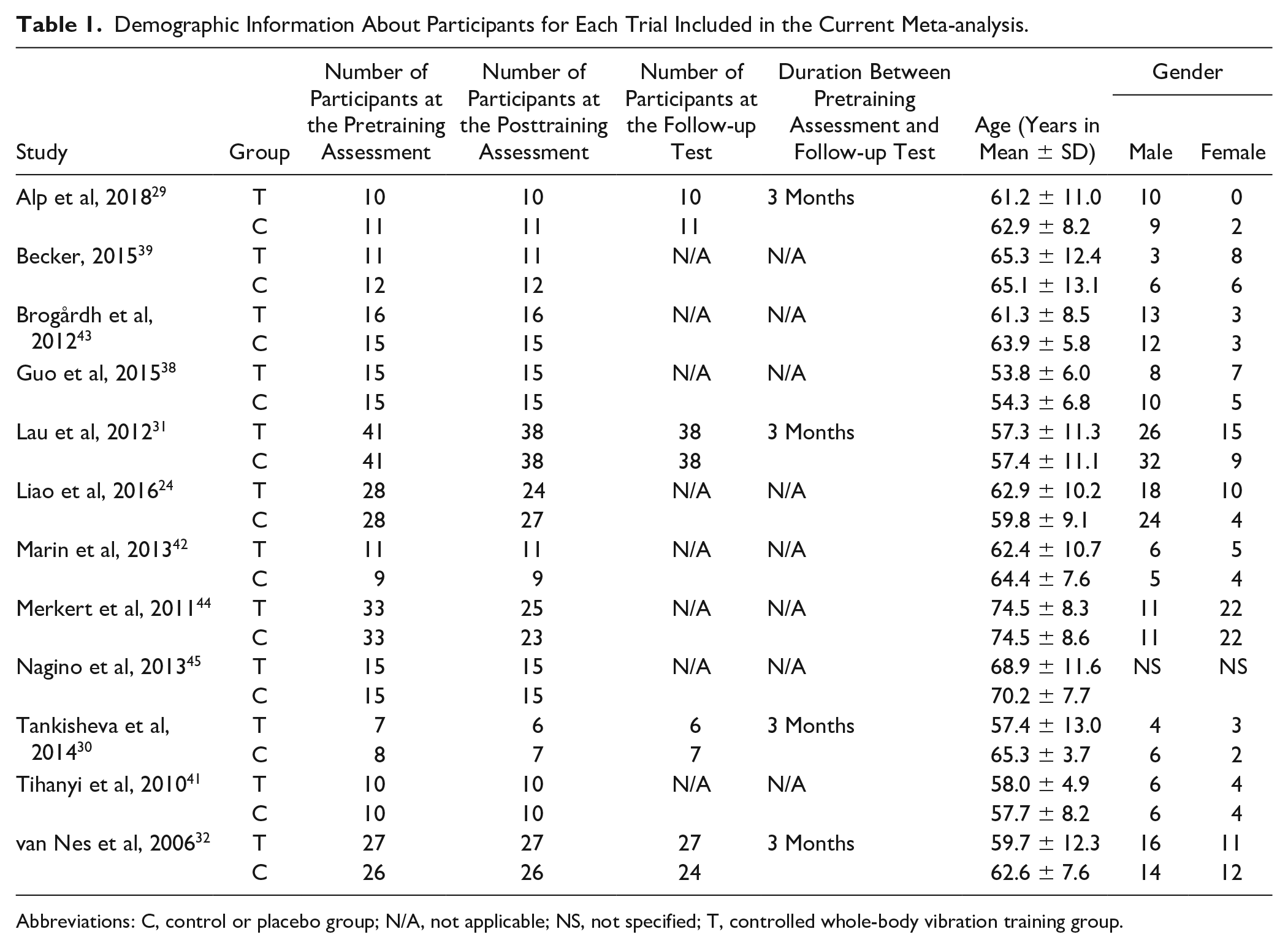
Abbreviations: C, control or placebo group; N/A, not applicable; NS, not specified; T, controlled whole-body vibration training group.
Disease Information About Participants for Each Trial Included in the Current Meta-analysis.
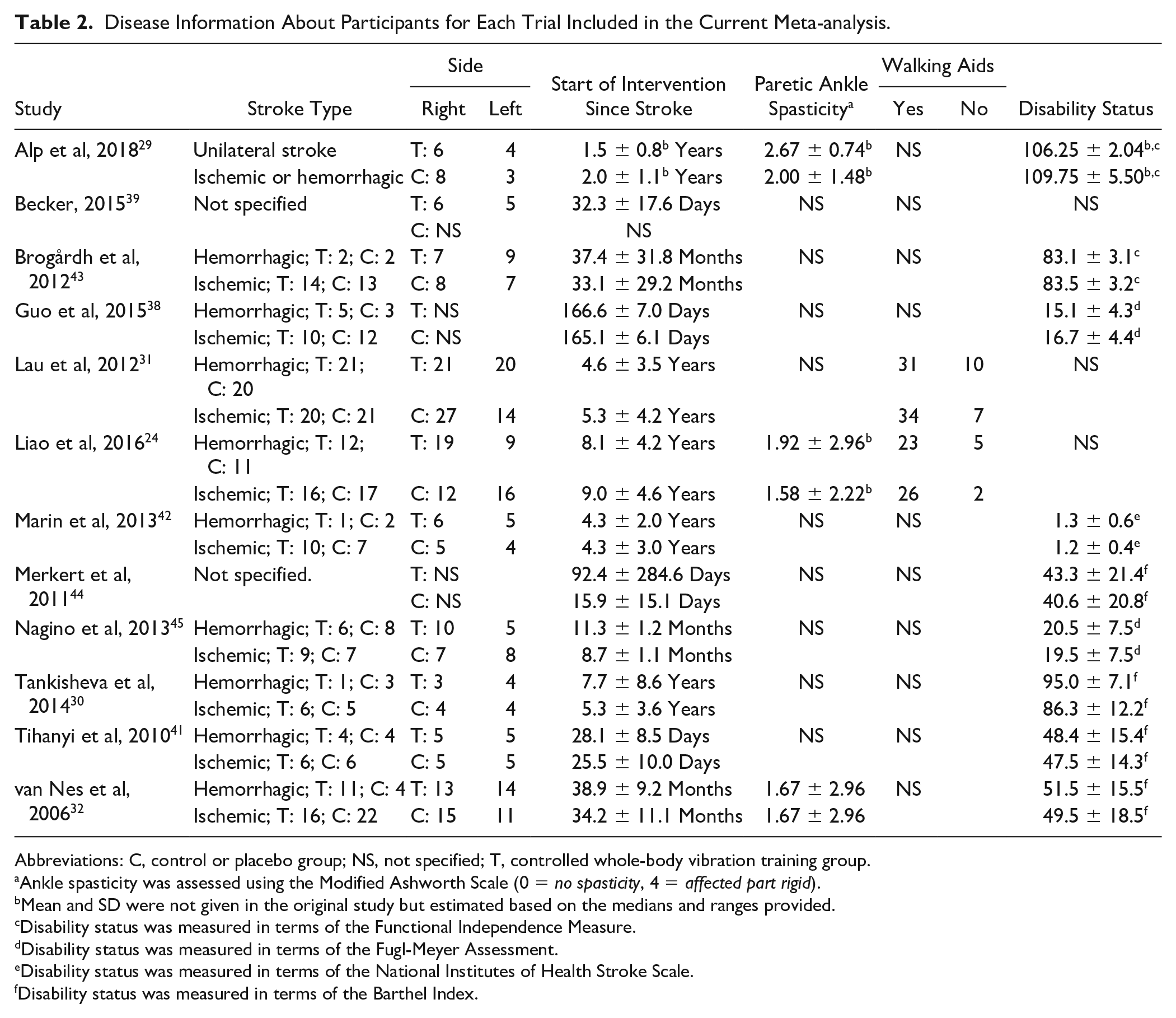
Abbreviations: C, control or placebo group; NS, not specified; T, controlled whole-body vibration training group.
Ankle spasticity was assessed using the Modified Ashworth Scale (0 = no spasticity, 4 = affected part rigid).
Mean and SD were not given in the original study but estimated based on the medians and ranges provided.
Disability status was measured in terms of the Functional Independence Measure.
Disability status was measured in terms of the Fugl-Meyer Assessment.
Disability status was measured in terms of the National Institutes of Health Stroke Scale.
Disability status was measured in terms of the Barthel Index.
Information About Controlled Whole-Body Vibration (CWBV) and Placebo Interventions for Each Individual Trial Included in the Present Meta-analysis.
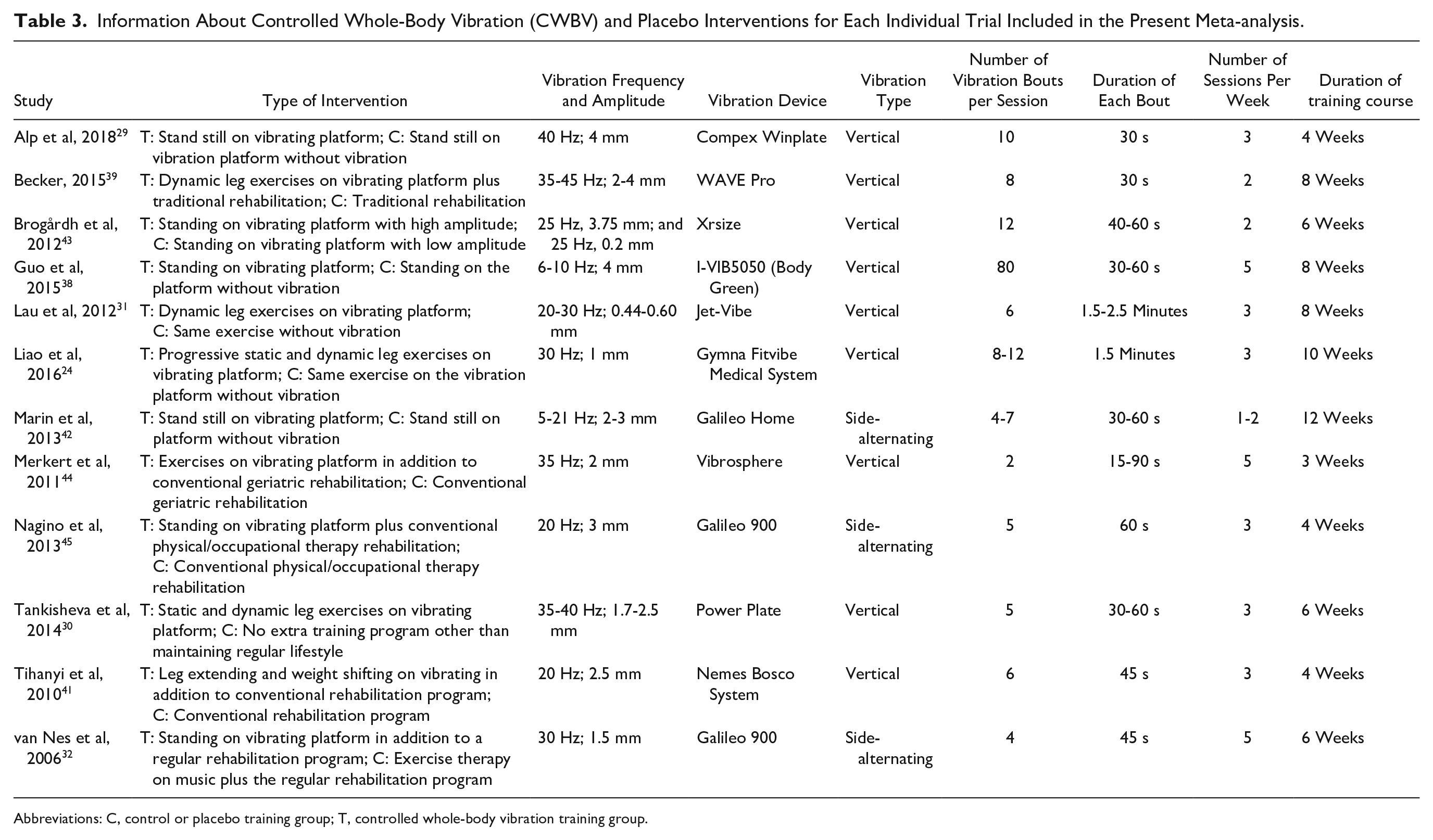
Abbreviations: C, control or placebo training group; T, controlled whole-body vibration training group.
For all trials, 16 of 224 (7.1%) participants in the vibration group dropped out of the study during the training. For the 4 studies that included a follow-up test, 85 participants initially were enrolled in the vibration group at baseline, and 4 of them withdrew from the study before the 3-month follow-up, making the attrition rate 4.7% (4/85; Table 1).
Body Balance Meta-analysis
Nine studies examined the effect of CWBV intervention on altering body balance tested by either the Berg Balance Scale,31,32,39,42-45 Mini-Balance Evaluation System, 24 or Sensory Organization Test. 30 Considerable variation was observed among trials probing the effect of CWBV on body balance, with ES ranging between −0.07 and 1.13 (Figure 2A). Two studies exhibited negative effects of CWBV on body balance32,42—that is, favoring placebo over CWBV. The remaining 7 trials displayed positive and beneficial effects of CWBV compared with placebo. Overall, meta-analysis on the 9 studies yielded a statistically significant ES (overall ES = 0.27; 95% CI = [0.03, 0.51]; P = .03).
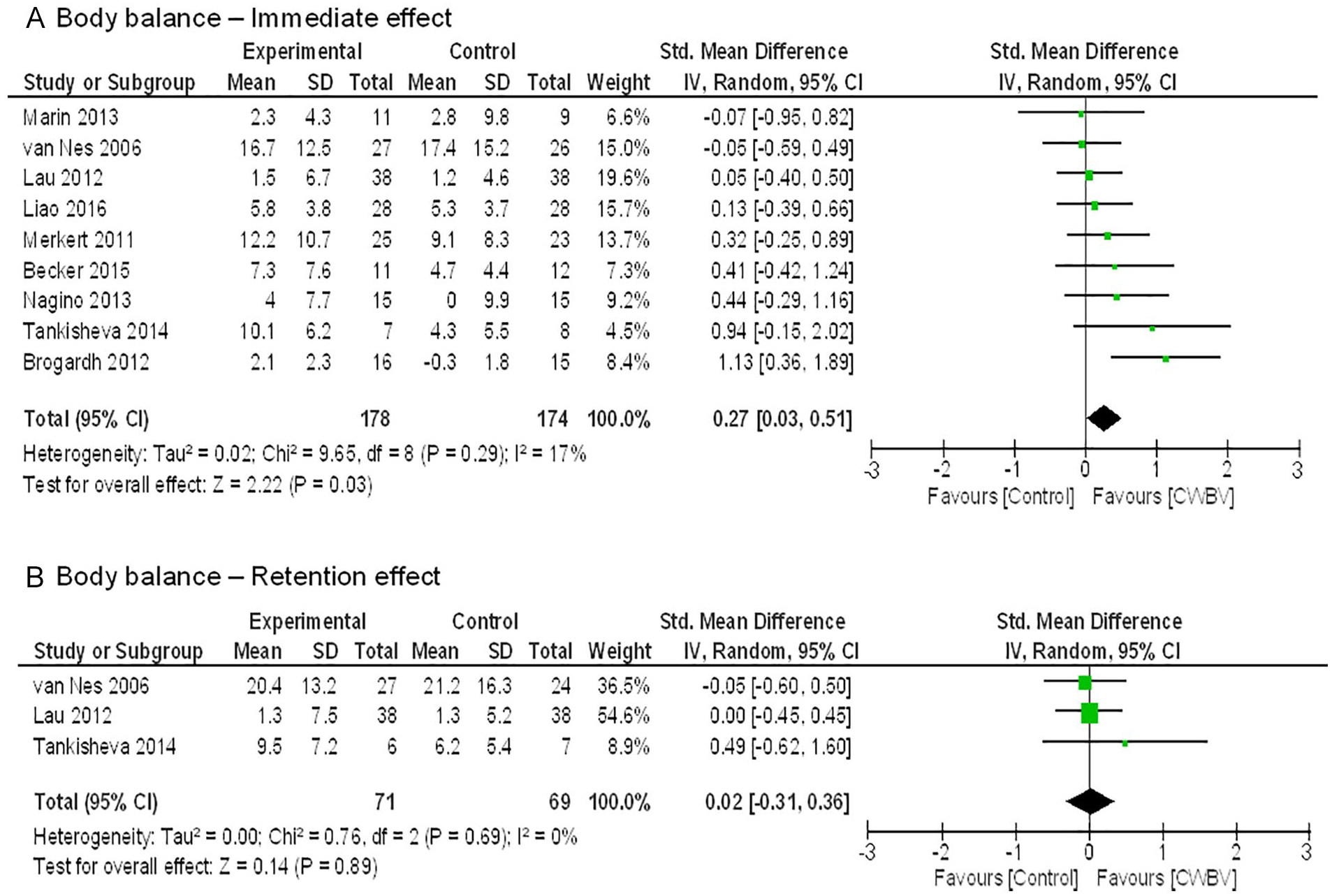
Forest plot of effect sizes from 9 studies that assessed the effect of controlled whole-body vibration (CWBV) training on improving body balance (A) immediately after the training course and (B) during the 3-month follow-up test after the pretraining assessment session.
Three trials conducted an assessment 3 months following the pretraining assessment to examine the persistent effects of CWBV training. The meta-analysis based on these 3 trials indicated that the ES was small and not statistically significant (ES: 0.02 [−0.31, 0.36]; P = .89; Figure 2B).
Functional Mobility Meta-analysis
Seven trials included functional mobility as the outcome measure.24,29,31,38,43-45 Among them, 4 studies adopted the 10-Meter Walk Test29,31,38,45 and 3 used the Timed-Up-and-Go test.24,43,44 The ES was between −0.04 and 1.05 for these studies (Figure 3A). Only 1 of the 7 publications reported negative effect of CWBV on mobility in stroke. 24 The meta-analysis indicated an overall ES of 0.34 ([0.29-1.83], P = .02).
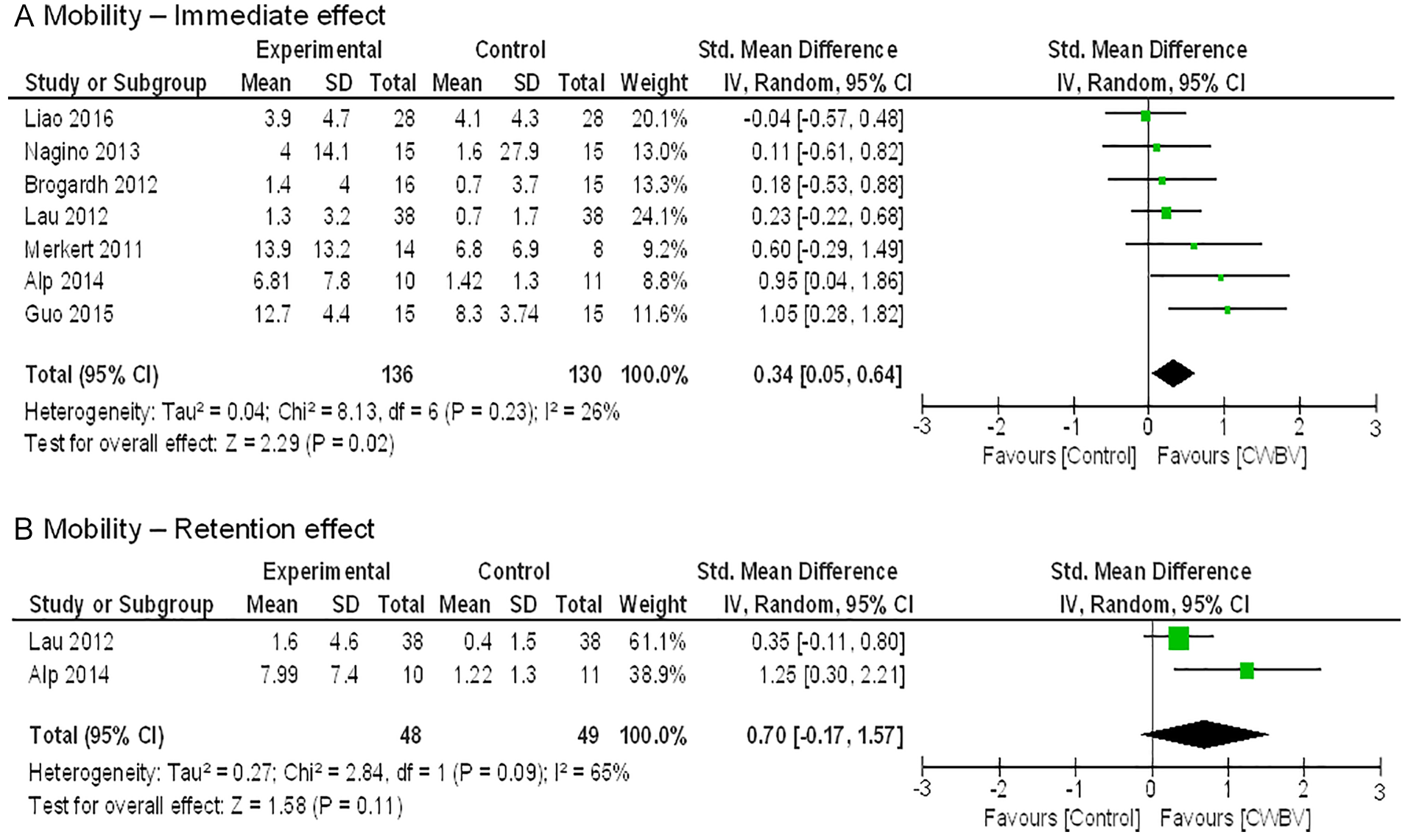
Forest plot of effect sizes from 7 studies that examined the effect of controlled whole-body vibration (CWBV) training on improving functional mobility (A) immediately after the training course and (B) during the follow-up test 3 months after the pretraining assessment session.
Two studies inspected the possible retention effect of CWBV on altering mobility among people with stroke (Figure 3B).29,31 Both indicated positive effects (ES: 0.35-1.25). The overall ES was large, at 0.70 [−0.17, 1.57], but insignificant (P = .11).
Muscle Strength Meta-analysis
Seven trials adopted the measurement of isometric strength capacity of the paretic knee extensors.24,30,31,41-43,45 The ES spanned over a wide range between −0.42 and 1.17 (Figure 4A). Three of the 7 publications suggested a negative effect of CWBV on knee strength31,42,43; 1 indicated no effect 24 ; and the remaining 3 studies reported a positive effect, suggesting that CWBV could strengthen the knee extensors.30,41,45 Overall, the ES of CWBV on knee extensor strength is limited (ES: 0.08 [−0.30, 0.47]; P = .68). Based on 2 studies,30,31 the meta-analysis indicated little retained effect of CWBV training on improving the paretic knee extensor strength (ES: 0.11 [−0.74, 0.95], P = .81; Figure 4B).
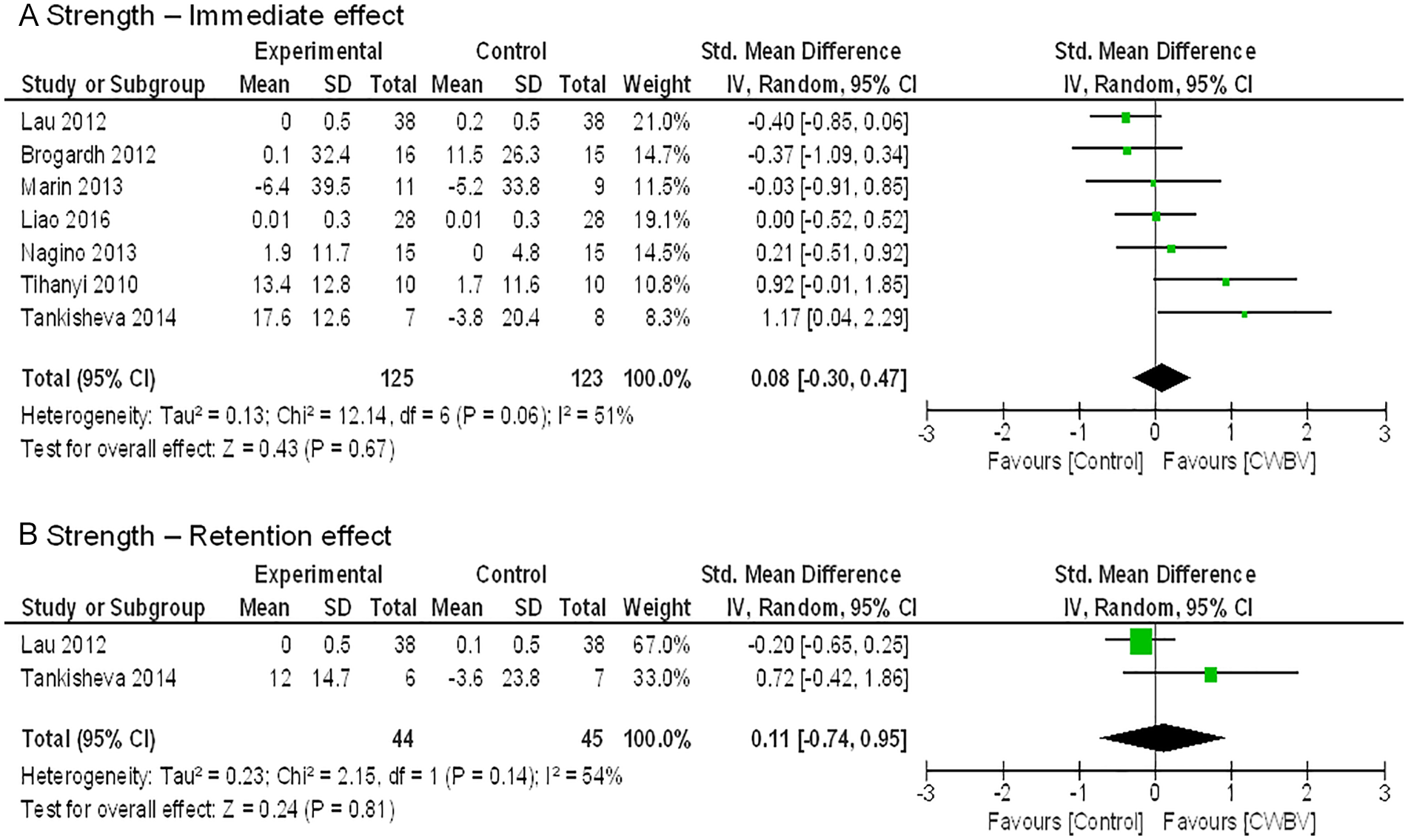
Forest plot of effect sizes from 7 studies that evaluated the effect of controlled whole-body vibration (CWBV) training on improving the isometric knee extensors strength capacity at the paretic side (A) immediately after the training course and (B) during the follow-up test 3 months after the pretraining assessment session.
Correlation Analyses
The meta-regression results indicated that the CWBV training dosage significantly and strongly correlates with the pooled immediate ES for balance (r = 0.649, P = .029; Figure 5A) and mobility (r = 0.785, P = .036; Figure 5B). For knee extensor strength capacity, there was no significant relationship between the training dosage and study ES (r = −0.153, P = .742; Figure 5C).
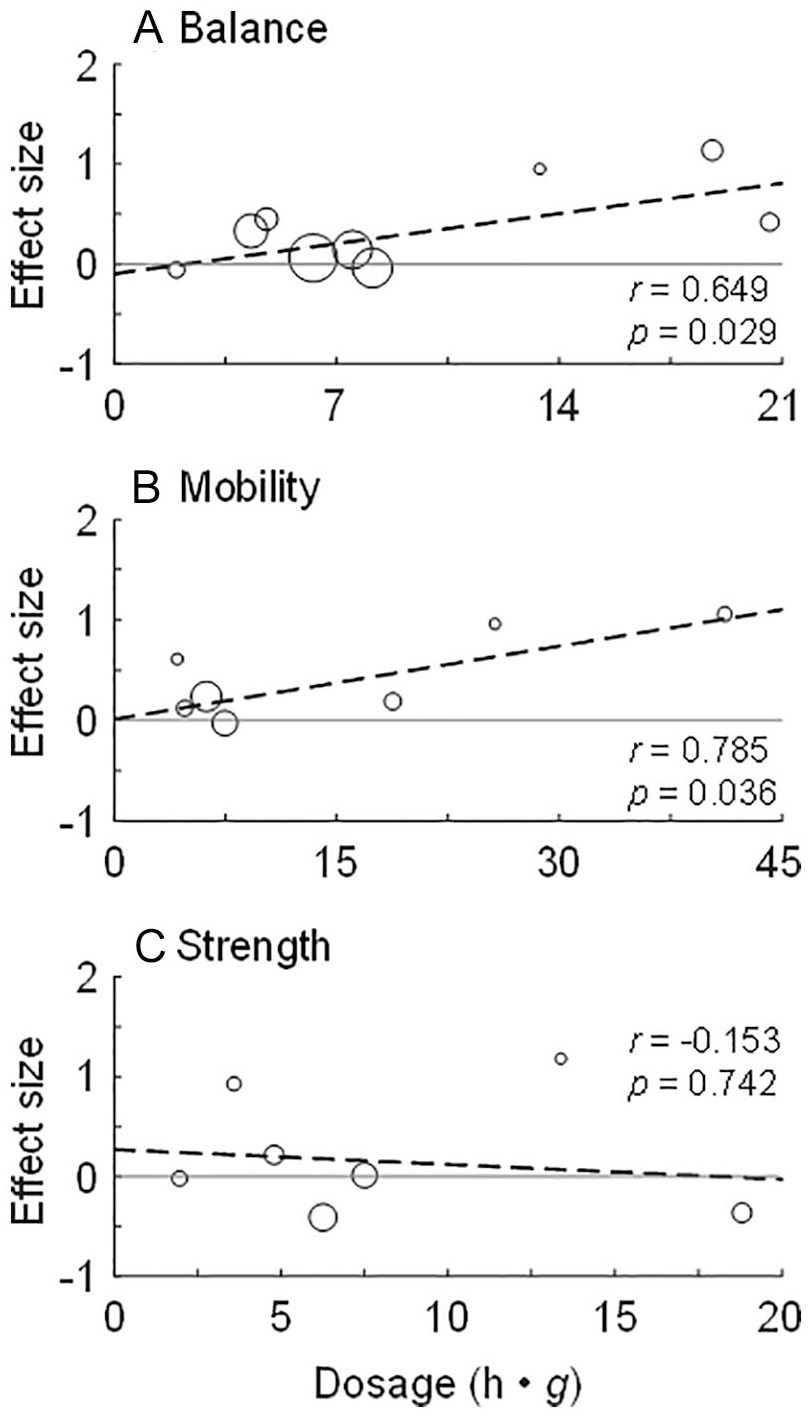
Meta-regression analysis of the relationship between controlled whole-body vibration training dosage (in h•g, where h is the number of hours and g is the gravitational acceleration) and effect size expressed as the standard mean difference for (A) body balance based on 9 studies, (B) functional mobility based on 7 studies, and (C) knee extensor strength capacity based on 7 studies, immediately after the training course. Each effect is represented by an open circle, and the size of the circle indicates the degree of weighting for that data point. The dashed line denotes the line of best fit for the corresponding fall risk factor. Also shown are the P value and the coefficient of correlation (r) for each regression. The horizontal line crossing zero represents an effect size of zero.
Discussion
Our meta-analyses of 12 RCTs demonstrated that short-term CWBV (between 3 and 12 weeks) is associated with a significant change in body balance and functional mobility but not knee extensor isometric strength in people with postacute or chronic stroke. We also found that the ES of CWBV training in improving body balance and mobility is strongly correlated with the training dosage expressed as the product of the peak platform acceleration and the vibration exposure time.
Consistent with previous findings,20,30,45 our study reinforces that CWBV may improve body balance among people with stroke. Similar findings were reported with other populations, such as older adults9,46 and people with Parkinson disease, 47 multiple sclerosis,48,49 and obesity. 50 Although the underlying mechanisms of CWBV is unclear, several factors could contribute to the observed improvement in body balance. First, mechanical vibration causes rapid displacement with high acceleration to the base of support, which can be considered a type of disturbance to the human body. Such a disturbance positions people in a challenging environment demanding considerable effort to maintain body balance. It has been documented that CWBV training is helpful for stimulating the vestibular system, postural improvement, and postural correction. 51 People with stroke may benefit from such balance-challenging conditions to develop neuromuscular skills for maintaining body balance. Second, CWBV training has been suggested to improve the cutaneous sensation on the plantar aspect of the foot.9,49,52 Because people with motor loss often have accompanying sensory loss and sensation is an essential component for keeping body balance, 53 increasing afferent gain through CWBV may result in improved body balance.
Our meta-analysis revealed that CWBV training is associated with a significant change in functional mobility, confirming findings from previous studies.20,29,38 Specifically, 6 of 7 studies favor CWBV training in improving mobility. The overall ES of CWBV to improve mobility in stroke across the 7 studies is 0.34 (Figure 3A). Improved mobility could be associated with the gain in balance control because body balance is fundamental for almost all human locomotion. It has been suggested that balance training could maintain and improve mobility in older adults. 54 On the other hand, mobility skills can also assist one with avoiding or recovering from balance disruptions. 55 A past study found that impaired sensation at the foot and ankle could lead to deficits in balance and mobility in stroke. 53 Presumably, the CWBV-induced plantar sensation improvement may have accounted for the enhanced mobility observed in previous publications.
Our finding that CWBV improves body balance and mobility contradicts previous meta-analyses,18,21 which report that CWBV training has little benefit in altering these 2 factors in comparison with placebo training. Several limitations in the previous articles may have contributed to this discrepancy. First, calculation of the ES could have been problematic in previous meta-analyses. Two studies did not use the change in balance or mobility between pretraining and posttraining assessments when determining the ES.18,21 Instead, the absolute values measured at the posttraining assessment were used. This method of calculation introduces a significant bias to the results especially when the measurements are imbalanced at the baseline assessment between groups. This was apparent in at least 2 studies42,43 included in previous meta-analyses. Second, the number of studies included in previous meta-analyses was low. Although 7 trials 18 and 8 trials 21 were discussed, the previous meta-analyses for each fall risk factor were based on 4 or fewer studies, severely undermining the ground on which the studies can be combined. For instance, only 1 trial was used to examine the ES of CWBV on modifying the mobility in stroke, 21 and 2 articles were used to test the ES of CWBV on balance and mobility. 18 Conversely, in the current meta-analyses, 12 independent trials were included, and at least 7 trials were used for any given fall risk factor. With a relatively large number of trials that included 447 participants, our analysis presumably would draw more comprehensive and reliable conclusions than previous studies. Finally, 2 studies31,37 that demonstrated no effect used the same sample of stroke participants. It is unjustifiable to include both as independent trials in a meta-analysis and would bias the results. 18
Our results illustrate that CWBV has little effect on lower-limb isometric joint strength, particularly the paretic knee extensors. The composite ES over 7 studies was 0.08 (P = .68; Figure 4). Although these results support the findings of previous meta-analyses,18,21 there is some uncertainty on the effect of CWBV training on muscle strength in people with stroke. Seven studies reviewed in the current meta-analysis had an even distribution around the “null effect”; 3 studies favored CWBV and 3 did not. The remaining article had an ES of 0.00, indicating that the effect of CWBV on improving knee extensor strength is comparable to that for placebo training (Figure 4A). A similar trend was described by previous meta-analyses.18,21 Given such a wide-spread of ES and the small number of studies, it is impossible to draw a definitive conclusion about CWBV’s effect on lower-limb strength. Furthermore, only isometric knee extensor capacity on the paretic side was reviewed in the current meta-analysis. It is unknown how CWBV interacts with other muscle groups or joints under other contraction conditions bilaterally. Therefore, well-designed studies with large sample sizes are needed to further examine how CWBV training affects muscle strength among people with stroke in a more systematic way.
CWBV is well tolerated by individuals poststroke as indicated by the low attrition rate (4.7%-7.1%) over the entire study period. The rate is drastically lower than the attrition for other types of exercise-based interventions (up to 43% 56 ). The high adherence rate could be a result of several inherent advantages of CWBV over traditional training paradigms, such as portability, safety, ease of use, and cost-effectiveness. These features make CWBV a simple, safe, and convenient alternative intervention and well suited for use in clinics, nursing homes, community centers, and even homes to train individuals with stroke to reduce their likelihood of falls.12,57
A strength of this study was the correlation analysis between the study ES and the dosage of CWBV. Our results indicate that the ES for both body balance and mobility are strongly correlated with the training dosage (Figure 5). The larger the training dose, the greater the ES for improving body balance and mobility. To our knowledge, this represents the first attempt to examine such correlations. The finding that there is a linear relationship between the ES and CWBV dosage is important because it may provide a reference to design CWBV-based training paradigms for reducing fall risk among people with stroke.
A past meta-analysis explored how CWBV volume affects functional performance following stroke, 19 in which all relevant trials were categorized according to frequency (20 vs 30 Hz), intervention duration (1 session, 4, 6, 8, 10, and 12 weeks), or number of sessions per week (1, 2, 3, and 5 times weekly). 19 This process has an unavoidable flaw because it does not consider other parameters associated with a vibration protocol when controlling only a single variable (frequency, duration, or number of sessions). Therefore, such comparisons are unlikely to yield objective and adequate results. In contrast, we created a new measurement to quantify CWBV training dosage based on both platform acceleration and total exposure time to the stimulation. Previous studies have reported that the platform acceleration is closely related to the stimulation level, as indicated by enhanced lower-limb muscle activity25,58,59 and joint loading. 60 A high vibration stimulation level leads to large improvements in muscular performance, 61 and more training sessions result in higher enhancement in muscle performance. 23 Our novel dosage definition includes parameters related to the effect of CWBV training simultaneously, forming a more comprehensive assessment of the training dosage.
Nevertheless, one must exercise caution in interpreting our calculation of CWBV dosage. Although reflecting both the exposure time and platform acceleration, the metric is rather arbitrary because we assumed that the contributions to the training effect are equivalent between these 2 factors (exposure interval vs acceleration level). This may not be valid because these 2 factors could have different weights on the training effect. Furthermore, how vibration frequency and amplitude individually affect the training outcome is unknown. A systematic and large-scale study is needed to investigate the relative importance between exposure time and acceleration level and between the vibration frequency and amplitude to the CWBV-induced improvements. Furthermore, our operational definition of the CWBV training dosage does not consider the rest time between training bouts, the type of vibration, exercises during vibration, and so on, all of which could influence the training effect. More studies are needed to examine how these factors would have an impact on the effects of CWBV training.
It is noticeable that one study 43 in the balance analysis and another 38 in the mobility analysis showed large ESs, possibly making them influential points for the meta-regression analyses. We conducted sensitivity analyses by removing these studies from the regression processes. The correlation coefficients for the metaregressions were still moderate to high (0.507 for balance and 0.763 for mobility). This indicates that our finding about the positive and strong correlations between the CWBV dosage and the effect of CWBV training in improving body balance and mobility is robust.
Our analyses demonstrated that when comparing the effects of CWBV on fall risk factors with those for placebo, a short-term CWBV program may not be retained (Figures 2B, 3B, and 4B). This might dampen the practical significance of CWBV as an intervention in reducing fall risk for people with stroke. However, it should be pointed out that these unfavorable findings were based on only 2 or 3 studies in which retention was assessed. Such a small sample size could lead to bias in our meta-analysis results. 62 Notably, the ES varies drastically among studies: −0.05 to 0.49 for balance, 0.35 to 1.25 for mobility, and −0.20 to 0.72 for strength. For some studies, the ES for retention could be considered large, implying that short-term CWBV may be more effective in reducing the fall risk factors than placebo training. To definitively accept or reject this notion, more rigorous studies examining the retention effect of CWBV training in stroke are needed.
We acknowledge several limitations of the present meta-analysis. First, only a limited number of fall risk factors were examined in the present meta-analyses. Other factors, such as fear of falling, sensation, and range of motion, were not examined. This was a result of the small number of RCTs that examined these factors. Second, not all studies provided information about disability level, spasticity, and the use of walking aids of participants (Table 2). The lack of information may lessen the clinical implication and generalizability of our findings to the general stroke population. Third, although balance and mobility have been associated with falls in stroke, 63 fall risk factors are not equivalent to a fall because falls are a complex, multifactorial phenomenon resulting from interactions among intrinsic and extrinsic risk factors. 64 Improvements in fall risk factors may not be predictive of the reduction in falls in everyday living situations. Studies that use falls as a primary outcome measure should be conducted to bridge this knowledge gap. Finally, articles not published in English were removed, possibly excluding some studies that concerned the effects of CWBV on reducing the risk of falls among people with stroke.
Conclusion
This meta-analysis indicated that short-term CWBV programs may improve body balance and mobility among people with stroke. It appears that CWBV has little effect on the paretic knee extensor strength. Additionally, the CWBV training effect on body balance and mobility strongly correlates with the training dosage. Our study can furnish some clarity to the current ongoing debate regarding the effects of CWBV training. More well-designed trials based on larger sample sizes are needed to further clarify the effect of CWBV training in comparison with other types of training programs. Even if CWBV is not found to be more effective than other training programs in improving fall risk factors, there is still great potential for this intervention given CWBV’s advantages relative to conventional exercise-based interventions.
Supplemental Material
PRISMA_2009_checklist – Supplemental material for Efficacy of Controlled Whole-Body Vibration Training on Improving Fall Risk Factors in Stroke Survivors: A Meta-analysis
Supplemental material, PRISMA_2009_checklist for Efficacy of Controlled Whole-Body Vibration Training on Improving Fall Risk Factors in Stroke Survivors: A Meta-analysis by Feng Yang and Andrew J. Butler in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
The authors thank Dr Gordon Warren for assistance with the meta-analysis and interpretation of the results.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.