
Abstract
Closed-loop vagus nerve stimulation (VNS) paired with rehabilitative training has emerged as a strategy to enhance recovery after neurological injury. Previous studies demonstrate that brief bursts of closed-loop VNS paired with rehabilitative training substantially improve recovery of forelimb motor function in models of unilateral and bilateral contusive spinal cord injury (SCI) at spinal level C5/6. While these findings provide initial evidence of the utility of VNS for SCI, the injury model used in these studies spares the majority of alpha motor neurons originating in C7-T1 that innervate distal forelimb muscles. Because the clinical manifestation of SCI in many patients involves damage at these levels, it is important to define whether damage to the distal forelimb motor neuron pools limits VNS-dependent recovery. In this study, we assessed recovery of forelimb function in rats that received a bilateral incomplete contusive SCI at C7/8 and underwent extensive rehabilitative training with or without paired VNS. The study design, including planned sample size, assessments, and statistical comparisons, was preregistered prior to beginning data collection (https://osf.io/ysvgf/). VNS paired with rehabilitative training significantly improved recovery of volitional forelimb strength compared to equivalent rehabilitative training without VNS. Additionally, VNS-dependent enhancement of recovery generalized to 2 similar, but untrained, forelimb tasks. These findings indicate that damage to alpha motor neurons does not prevent VNS-dependent enhancement of recovery and provides additional evidence to support the evaluation of closed-loop VNS paired with rehabilitation in patients with incomplete cervical SCI.
Keywords
Introduction
Spinal cord injury (SCI) affects 276, 000 individuals in the United States and millions more worldwide.1,2 The cervical spinal region is the most common site of injury, accounting for over 55% of all SCIs.3-5 Injury to the cervical spinal cord at or above the levels containing upper limb motor neurons carries a poor prognosis, and many cervical SCI patients experience long-term loss of upper extremity function that leads to chronic disability.6-8 The development of interventions to improve recovery of function after cervical SCI is of key importance.
Plasticity in spared networks represents a substrate for recovery after incomplete SCI.9-13 We have developed a novel technique to boost synaptic plasticity in conjunction with rehabilitation and improve recovery after neurological injury.14,15 This strategy involves closed-loop stimulation of the vagus nerve triggered by forelimb movement during rehabilitative training to engage neuromodulatory networks and drive specific and long-lasting synaptic plasticity in the central nervous system.16-20 Previous studies demonstrate that vagus nerve stimulation (VNS) paired with rehabilitative training significantly improves recovery of forelimb function compared to rehabilitative training without VNS in multiple animal models of neurological injury, including incomplete unilateral and midline SCI, stroke, intracerebral hemorrhage, and traumatic brain injury.21-29 Moreover, emerging evidence from clinical trials highlights the translational potential of VNS therapy to improve recovery of motor function in chronic stroke patients.30,31
While initial findings support the notion that VNS paired with rehabilitative training enhances recovery after cervical SCI, the C5/6 injury model employed in these studies produced damage primarily to the white matter tracts above the distal forelimb motor pools while largely sparing the alpha motor neurons originating in C7-T1. 29 These spinal levels comprise the motor pools that control distal musculature, including extensor carpi ulnaris, flexor carpi ulnaris, extensor pollicis longus, digitorum profundus, extensor digiti quarti, palmaris longus, and flexor carpi radialis. 32 The clinical manifestation of cervical SCI often results in damage to the spinal levels containing alpha motor neurons that control distal upper limb musculature in combination with white matter injury. Substantial damage to these motor neuron pools could limit the benefits of plasticity-enhancing therapies if reorganization cannot compensate for the reduction in alpha motor neurons. Alternatively, synaptic plasticity within spared spinal networks may be sufficient to leverage remaining alpha motor neurons to support recovery. Here, we sought to model these complicating clinical features and determine whether direct damage to the distal forelimb motor pools would prevent VNS-dependent enhancement of recovery. To do so, we assessed recovery of forelimb motor function in animals that received a bilateral incomplete contusive SCI at C7/8 and underwent extensive rehabilitative training with or without paired VNS.
Materials and Methods
Experimental Design
All experimental procedures, group sizes, outcome measures, statistical comparisons, and exclusion criteria were preregistered on Open Science Framework before beginning data collection (https://osf.io/ysvgf/). The final study design deviated from the preregistration in the inclusion of generalization assessments and change in histological processing. Procedures used in this study were approved by the University of Texas at Dallas Institutional Animal Care and Use Committee (Protocol 14-10). Adult female Sprague-Dawley rats (n = 58) weighing approximately 300 g were obtained from Charles River Laboratories. Rats were trained to proficiency on the isometric pull task, as in previous studies.21,24-26,28,33-36 After reaching proficiency, rats underwent bilateral contusive injury at level C7/8 of the spinal cord and were implanted with a vagus nerve cuff electrode (Figure 1A). Eight weeks after SCI, rats underwent a baseline assessment and were dynamically allocated to receive either Rehab or VNS + Rehab. To ensure balancing across groups, rats were assigned to a treatment group based on post-SCI median pull force to minimize between-group differences. Rats in the Rehab group (n = 8) received rehabilitative training, which consisted of freely performing the isometric pull task for two sessions daily for 6 weeks (weeks 9-14). Rats in the VNS + Rehab group (n = 10) received equivalent rehabilitative training, but a 0.5-second burst of VNS was paired with forelimb movement on appropriate trials during training (Figure 1B). No VNS was delivered during the final week of rehabilitative training (week 14) to allow assessment of effects lasting beyond the cessation of stimulation. At the conclusion of behavioral testing, the spinal cord was removed for histological processing. Forty rats were excluded from the study based on predefined criteria listed in the study preregistration: mortality (n = 6), inability to perform the task after injury (n = 4), significant autophagia (n = 20), or VNS device failure (n = 10). Autophagia was observed almost exclusively in the hindpaw and is likely due to the tracts damaged by the C7/8 injury model. Similarly, the exclusion of animals due to inability to perform the task after injury is expected based on previous studies. 29 All source data indexed across animals can be found in Supplementary Tables 1 to 5 (available online).
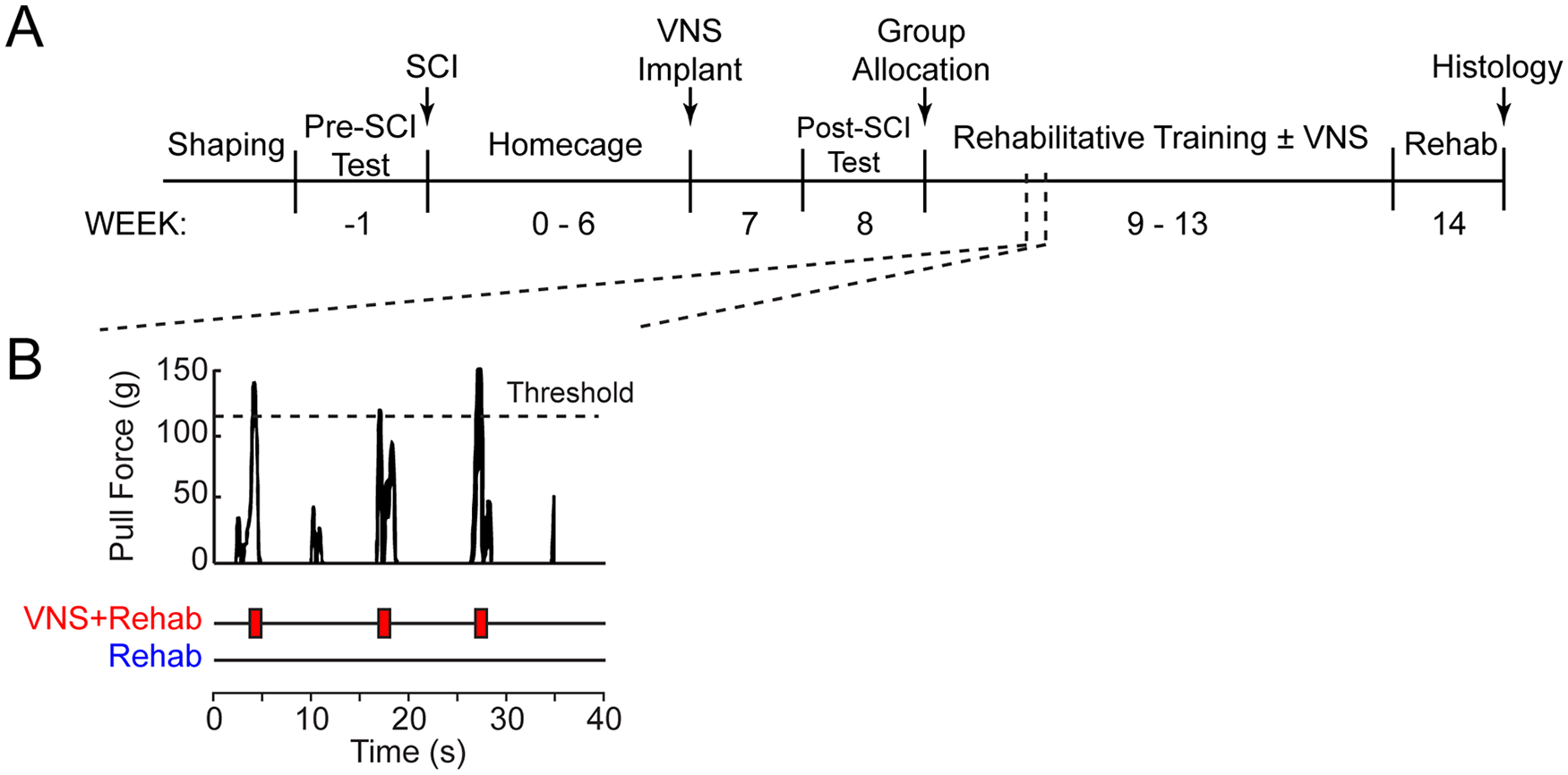
Timeline and experimental design. (A) Illustration of experimental timeline for each subject in the study. (B) Example of forelimb pull forces recorded during rehabilitative training. Five trials are shown. Animals in the VNS + Rehab group received a short 0.5-second burst of VNS (red blocks) paired with trials in which pull force exceeded the stimulation threshold. Animals in the Rehab group performed equivalent rehabilitative training without VNS. VNS, vagus nerve stimulation.
Isometric Pull Task
The isometric force task was used to measure volitional forelimb strength as previously described.21,24-26,28,33-36 The behavioral training chamber consisted of an acrylic box (10 × 12 × 4.75 inches) with a slot in the front right corner through which rats could access a handle manipulandum. Rats were trained to pull the handle, which was attached to a force transducer (Motor Pull Device and Motor Controller, Vulintus LLC, Sachse, TX). A trial was initiated when 10 g of force was exerted on the pull handle. If the peak pull force exceeded an adaptively-scaled threshold within 2 seconds of trial initiation, a reward pellet (45 mg dustless precision pellet, BioServ, Frenchtown, NJ) and VNS, when appropriate, was delivered. The threshold was scaled adaptively based on the median peak force of the 10 preceding trials, with a fixed bounded minimum of 10 g and maximum of 120 g based on previous studies.35,37
Rats underwent training and testing according to the timeline shown in Figure 1. Behavioral training sessions lasted 30 minutes and were conducted twice daily, 5 days per week, with daily sessions separated by at least 2 hours. Rats were trained until they reached proficiency, defined as 10 consecutive sessions in which greater than 75% of trials exceeded 120 g. After attaining proficiency, rats were given a bilateral contusive SCI at spinal level C7/8. Eight weeks after injury, rats returned for behavioral testing were dynamically allocated to balanced groups based on their post-injury performance. Rehabilitative training then continued for 6 weeks. For rats receiving VNS + Rehab, stimulation was triggered by the behavioral software on appropriate trials during rehabilitative training.
Bilateral Cervical Spinal Cord Injury Surgery
All surgeries were performed using aseptic technique under general anesthesia. Rats were deeply anesthetized with ketamine (50 mg/kg, intrapertoneally [ip]), xylazine (20 mg/kg, ip), and acepromazine (5 mg/kg, ip). A bilateral dorsal C7 laminectomy was performed. The vertebral column was stabilized using spinal microforceps. The right and left lateral portions of the spinal cord (1 mm lateral from midline) were consecutively contused using an Infinite Horizons Impact Device fitted with an round impactor tip with a 1.25 mm diameter at a force of 225 kdyn and zero dwell time (Precision Systems and Instrumentation, Lexington, KY). The skin overlying the exposed vertebrae was then closed in layers and the incised skin was closed using surgical staples. All rats received buprenorphine (subcutaneously [sc], 0.03 mg/kg, 1 day postoperative), enrofloxacin (sc, 10 mg/kg, 5 days postoperative), and Ringer’s solution (sc, 10 mL, 5 days postoperative) immediately after surgery and continuing postoperatively.
Vagus Nerve Stimulation Cuff Implantation Surgery
VNS implantation procedures were performed as described in previous studies.21-29 Seven weeks post-SCI, rats were anesthetized with ketamine hydrochloride (50 mg/kg, ip), xylazine (20 mg/kg, ip), and acepromazine (5 mg/kg, ip), and were placed in a stereotactic apparatus. An incision was made down the midline of the head to expose the skull. Bone screws were inserted into the skull at points surrounding the lamboid suture and over the cerebellum. A 2-channel connector was mounted to the screws using acrylic. The rat was then removed from the stereotaxic apparatus and placed in a supine position. An incision was made on the left side of the neck and the sternocleidomastoid, sternohyoid, and omohyoid were blunt dissected to expose and isolate the vagus nerve. The nerve was placed into a custom-built bipolar stimulating cuff electrode, 38 and the electrode leads were tunneled subcutaneously and connected with the 2-channel skull-mounted connector. Incised skin was then sutured closed. All rats received enrofloxacin (sc, 10 mg/kg) following surgery. Regardless of group assignment, all rats underwent implantation of the headmount and cuff. To confirm cuff functionality and proper placement, VNS-dependent activation of the Hering-Breuer reflex was assessed as in previous studies.38,39 To do so, while anesthetized, blood oxygenation saturation during trains of VNS (0.8 mA, 30 Hz, 100 µs pulse width, up to 5-second train duration) was monitored via pulse oximetry both immediately after cuff implant and at the end of therapy. Rats that failed to demonstrate a reliable drop in oxygen saturation, indicative of a failure in stimulation efficacy, were excluded (n = 3).
Delivery of Vagus Nerve Stimulation During Rehabilitative Training
VNS parameters were equivalent to previous studies.24-26,28,36 Each 0.5-second stimulation train consisted of sixteen 0.8-mA 100-µs biphasic pulses delivered at 30 Hz. Trains of stimulation were triggered during rehabilitative training based on an adaptive threshold, and delivered within 0.2 ms on surpassing the adaptive threshold as previously described.27,29 The adaptive threshold was scaled such that stimulation was triggered when the force on a given trial exceeded the median pull force of the 10 antecedent trials or 120 g, whichever was lower. No VNS was delivered on the final week of rehabilitative training (week 14) to assess effects lasting after the cessation of stimulation.
Cylinder Assessment
Spontaneous use of the forelimbs during exploratory activity was measured in all animals, similar to previous descriptions.40,41 Animals were placed in a transparent cylinder and allowed to freely explore for 3 minutes. Video was recorded from directly underneath the cylinder through a clear sheet of acrylic. To assay forepaw usage, the total number of times in a session that the rat contacted the cylinder with the ventral surface of either the right forepaw, the left forepaw, or both forepaws simultaneously, was counted. Assessments were performed before injury (week −1), before therapy (week 8), and after therapy (week 14) by experimenters blinded to group.
Grip Strength Assessment
A custom-made grip strength meter was used to measure the grip strength of the right and left forepaws independently, similar to previous descriptions. 42 The rat was positioned over the 2 horizontal bars attached to separate force transducers such that each forepaw grasped a single bar. Once at least 3 digits on each paw had grasped the bars, the animal was pulled horizontally away from the bars in a smooth and constant motion. The peak force at which grip is released from the bar was recorded for each paw individually. Five trials were performed at each assessment, and the average of the peak grip forces were recorded. Assessments were performed before injury (week −1), before therapy (week 8), and after therapy (week 14) by experimenters blinded to group.
Lesion Histology and Analysis
At the completion of experimental testing, rats were anesthetized with sodium pentobarbital (50 mg/kg, ip) and transcardially perfused with 4% paraformaldehyde in 0.1 M phosphate buffered saline (pH 7.5). The spinal cord was removed and postfixed overnight, cryoprotected in 30% sucrose for 48 hours, blocked, and frozen at −80°C in Shandon M1 embedding matrix (Thermo Fisher Scientific; Waltham, MA). Spinal tissue was sliced at 50 µm using a cryostat, slide mounted and stained for Nissl and myelin similar to previous studies.37,43 Photomicrographs were taken at 150-µm intervals from approximately C5 to T2.
Statistical Analysis
All group sizes, outcome measures, and planned statistical comparisons were included in the study pre-registration prior to beginning data collection. Performance on the isometric force task was analyzed using a 2-way repeated measures analysis of variance (ANOVA) to assess effects of treatment and time, followed by post hoc Bonferroni-corrected unpaired t tests where appropriate. Paired t tests were used to compare isometric pull task measures within subjects from pre- to post-SCI and from week 13 to week 14 in the VNS + Rehab group. Unpaired t tests at each time point were used to compare cylinder task data and grip strength across groups at each time point. Statistical tests for each comparison are noted in the text. Figures depict mean ± standard error of the mean (mean ± SEM).
Results
Rats were trained to perform the isometric pull task, an automated reach-to-grasp task that measures volitional forelimb strength.21,33,37 On achieving proficiency on the task, all rats underwent bilateral contusive impact at spinal level C7/8 to impair function of the trained forelimb (Figure 2, Supplemental Figure S1.). As expected, SCI at C7/8 resulted in a substantial reduction in volitional forelimb strength (Figure 3A; PRE vs. Wk 8; paired t test, t(17) = 18.79, P = 8.23 × 10−23). Hit rate, defined as the percentage of trials in which pull force exceeded 120 g, was also significantly reduced by SCI (Figure 3B; PRE vs. Wk 8; paired t test, t(17) = 24.84, P = 8.45 × 10−15). No differences in any measures were observed between groups prior to beginning therapy (Figure 3; Rehab vs. VNS + Rehab at Wk 8; peak force: unpaired t test, t(16) = 0.99, P = .33; hit rate: unpaired t test, t(16) = 1.07, P = .30).
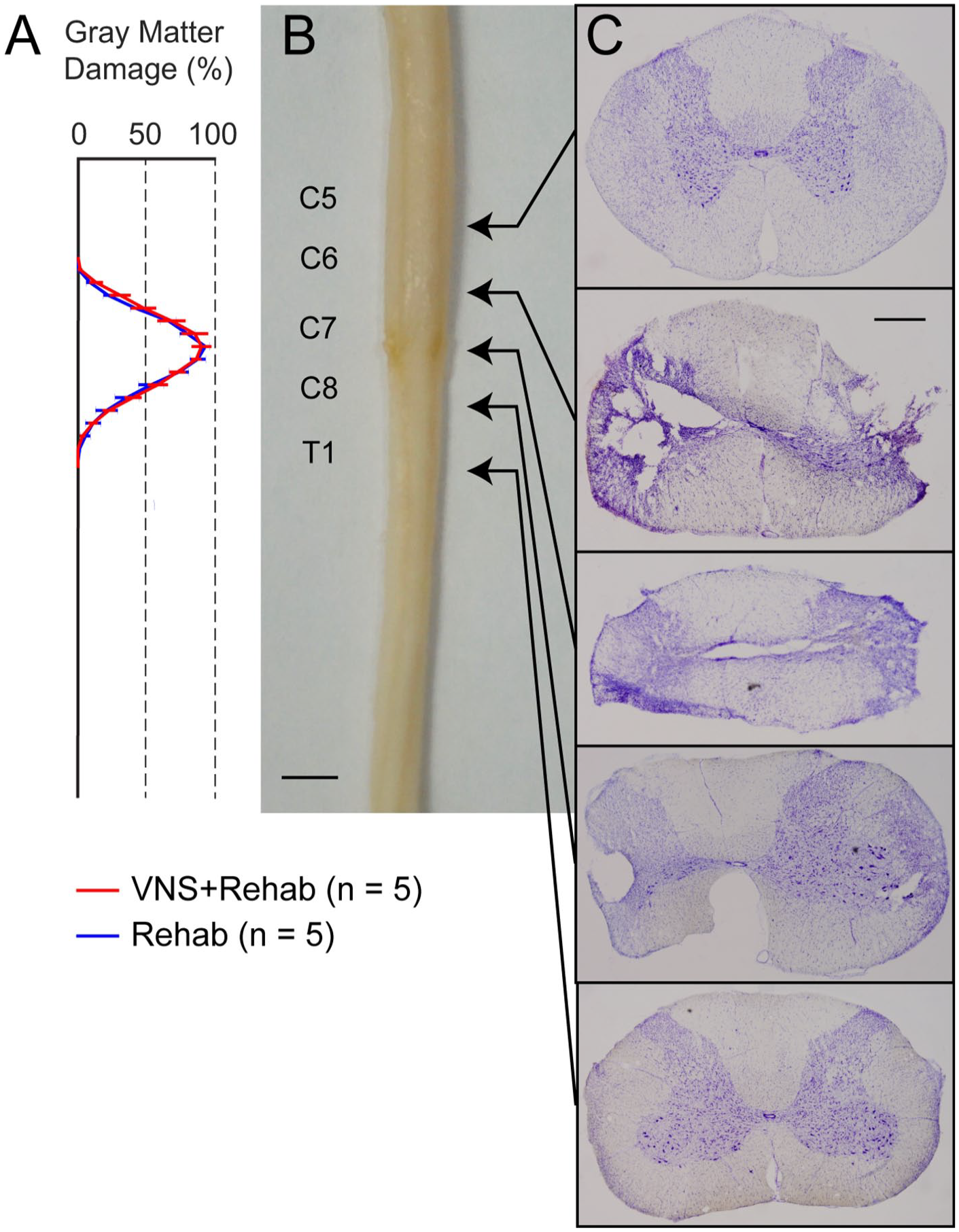
Spinal cord injury (SCI) causes bilateral damage between spinal levels C7 and C8. (A) Damage to gray matter of the spinal cord is centered between C7 and C8, and extends rostrally and caudally. No difference in lesion extent were observed between VNS + Rehab or Rehab groups. Additional lesion quantification can be found in Supplementary Figure S1. (B, C) Representative examples from a range of levels illustrating the extent of damage through the cord. Substantial damage was observed near the lesion epicenter, with minimal injury to levels above and below. Scale bars indicate 3 mm in panel B and 500 µm in panel C. VNS, vagus nerve stimulation.
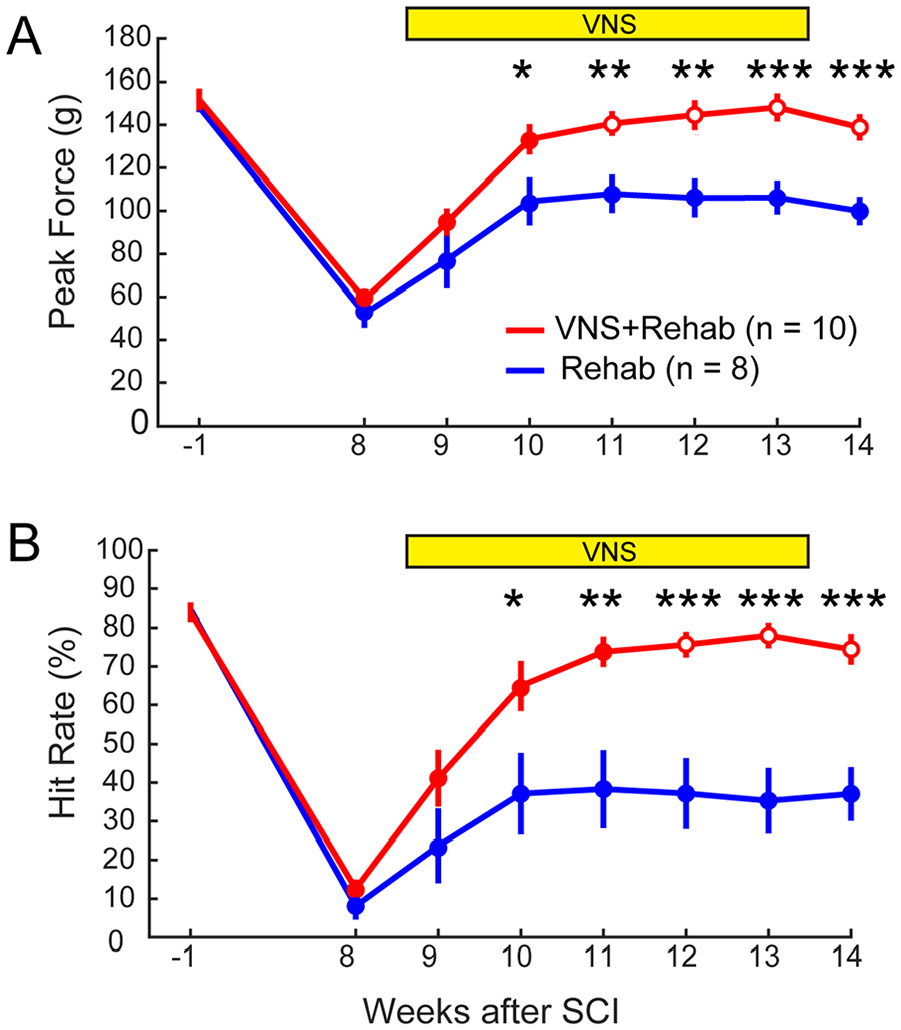
Vagus nerve stimulation (VNS) paired with rehabilitative training enhances recovery after C7/8 spinal cord injury (SCI). (A) VNS paired with rehabilitative training (VNS + Rehab) significantly improves recovery of volitional forelimb strength compared to equivalent rehabilitative training without VNS (Rehab) after bilateral SCI at C7/8. VNS-dependent benefits remain on week 14 after the cessation of stimulation, indicating lasting recovery. (B) Similarly, VNS + Rehab significantly increases hit rate on the isometric pull task compared to Rehab after SCI, measured as the percentage of trials on which peak forelimb pull force exceeds 120 g. *P < .05, **P < .01, ***P < .001; unpaired t tests comparing VNS + Rehab and Rehab at each time point. Filled markers indicate a significant reduction compared to pre-SCI performance at each week (paired t test vs. week −1, P < .05). Error bars indicate mean ± standard error of the mean (mean ± SEM).
We sought to determine if VNS paired with rehabilitative training would improve recovery of forelimb strength after SCI. To do so, beginning 9 weeks after injury, rats underwent 6 weeks of either rehabilitative training on the isometric pull task in which a 0.5-second burst of VNS was paired with forelimb use (VNS + Rehab; n = 10) or equivalent rehabilitative training without VNS (Rehab, n = 8). VNS paired with rehabilitative training significantly increased recovery of volitional forelimb strength compared to equivalent rehabilitative training without VNS (Figure 3A, Rehab vs. VNS + Rehab; 2-way repeated-measures ANOVA, F(1, 16) = 16.98; P = 8.02 × 10−4). Post hoc tests revealed significant improvements in forelimb strength in the VNS + Rehab group compared to the Rehab group beginning on the third week of therapy (Figure 3A, Rehab vs. VNS + Rehab at each week; Bonferroni-corrected unpaired t tests, weeks 11 to 14 all P < 8.33 × 10−3). Improved volitional forelimb strength was maintained in the VNS + Rehab group on week 14 after the cessation of stimulation, indicating lasting benefits (Figure 3A; VNS + Rehab, Wk 13 vs. Wk 14; paired t test, t(9) = 1.95, P = .82). A similar VNS-dependent enhancement of recovery was observed for hit rate (Figure 3B, Rehab vs. VNS + Rehab; 2-way repeated-measures ANOVA, F(1, 16) = 17.67; P = 6.74 × 10−4; Bonferroni-corrected unpaired t-tests at each week; weeks 11 to 14 all P < 8.33 × 10−3). These findings demonstrate that VNS paired with rehabilitative training significantly enhances recovery of forelimb motor function compared to rehabilitative training without VNS after bilateral spinal cord damage at C7/8.
We next assessed whether recovery was restricted to the trained task or generalized to similar, but untrained, forelimb tasks. First, we tested spontaneous forelimb use with the cylinder assessment. 41 Although typically used as a measure of forelimb asymmetry after unilateral injury, we used the cylinder assessment to evaluate spontaneous use of both forelimbs. As expected, bilateral C7/8 SCI also reduced spontaneous use of both forelimbs, as indicated by a decrease in the total number of wall touches per session (Figure 4A, Rehab, Pre: 95 ± 13, Post: 21 ± 5, paired t test, t(7) = 5.46, P = 9.47 × 10−4; VNS + Rehab, Pre: 91 ± 7, Post: 18 ± 3, t(9) = 9.75, P = 4.41 × 10−6). After the conclusion of rehabilitative therapy, the VNS + Rehab group demonstrated significantly greater restoration of spontaneous forelimb use compared to Rehab (Figure 4A; Rehab: 31 ± 6; VNS + Rehab: 71 ± 6; unpaired t test, t(16) = 5.14, P = 9.87 × 10−5). Next, we tested forepaw grip strength. Consistent with previous reports, 44 bilateral C7/8 SCI results in a significant impairment in grip strength (Figure 4B; Rehab, Pre: 665 ± 21 g, Post: 289 ± 13 g, paired t test, t(7) = 16.40, P = 7.64 × 10−7; VNS + Rehab, Pre: 635 ± 24 g, Post: 285 ± 12 g, t(9) = 16.29, P = 5.50 × 10−8). VNS paired with rehabilitative training significantly improved grip strength compared to rehabilitative training alone in the trained right forelimb (Figure 4B; Rehab: 369 ± 18 g; VNS + Rehab: 459 ± 24 g; unpaired t test, t(16) = 3.05, P = .008). No significant improvement in grip strength was observed in the untrained left paw (Rehab: 327 ± 22 g; VNS + Rehab: 391 ± 23 g; unpaired t test, t(16) = 2.07, P = .054). Together, these findings indicate that VNS paired with rehabilitative training yields improved recovery of motor function on similar, but untrained, forelimb tasks after bilateral C7/8 SCI.
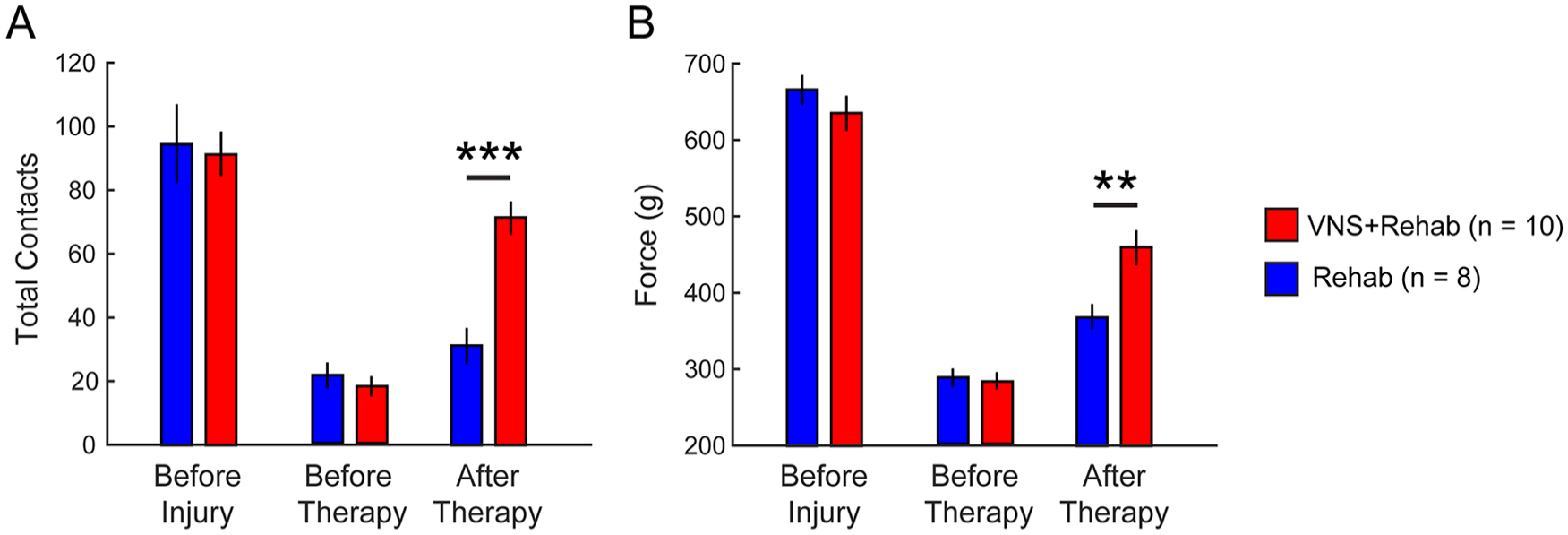
Vagus nerve stimulation (VNS)–dependent recovery generalizes to similar, but untrained, forelimb tasks. (A) Spinal cord injury (SCI) reduces the total number of forepaw contacts on the cylinder task. VNS paired with rehabilitative training on the isometric pull task significantly increases spontaneous forelimb use during exploration compared to rehabilitative training without VNS, indicative of a generalization of forelimb recovery to a similar task. (B) Pairing VNS with training on the isometric pull task significantly increases grip strength compared to rehabilitative training without VNS. Unpaired t tests across groups at each time point; **P < .01, ***P < 0.001. Error bars indicate mean ± standard error of the mean (mean ± SEM).
Changes in the intensity of rehabilitative training could potentially mediate VNS-dependent recovery. No differences were observed in the total number of trials performed over the course of therapy across groups, consistent with previous reports and demonstrating that VNS does not influence the intensity of rehabilitative training (Rehab: 10993 ± 777 trials, VNS + Rehab: 9390 ± 569 trials; unpaired t test, t(16) = 1.81, P = .09). These findings indicate that motivation cannot account for VNS-dependent benefits on recovery. Additionally, no differences were observed in lesion extent across groups (Figure 2A; 2-way repeated-measures ANOVA, F(1, 8) = 0.14; P = .72). These findings are consistent with previous studies and indicate that VNS does not promote neuroprotection to improve recovery. 29
Discussion
In this study, we demonstrate that VNS paired with rehabilitative training significantly enhances recovery of forelimb function compared to equivalent rehabilitative training without VNS after bilateral C7/8 SCI that damages distal motor neuron pools. VNS-dependent benefits last after the cessation of stimulation and extend to other similar, but untrained, forelimb measures. Improved recovery in the VNS-treated group occurred without affecting intensity of rehabilitative training. The findings from this study support the potential for VNS paired with rehabilitation as a therapeutic intervention in SCI and provide and initial demonstration that damage to motor pools does not preclude VNS-dependent benefits.
Previous evidence indicates that VNS paired with rehabilitative training drives synaptic plasticity in spared networks and enhances recovery of motor function after SCI at spinal level C5/6. 29 The injury model used in earlier studies largely spared the alpha motor neurons innervating muscles in the distal forelimb, which predominantly originate in spinal levels C7 to T1. 32 Given the heterogeneity in the clinical manifestation of SCI, the present study sought to evaluate whether substantial damage to the distal forelimb motor pools would preclude VNS-dependent enhancement of recovery. We observe that VNS paired with rehabilitative training results in significant improvements in recovery of motor function compared to equivalent rehabilitative training without VNS after damage to the distal forelimb motor pools. Consistent with previous studies, VNS does not alter the extent or magnitude of spinal damage, suggesting it does not improve recovery via a neuroprotective mechanism. 29 The present study inferred damage to motor neuron pools based on gray matter injury. These findings indicate that damage to these networks is not the sole limiting factor for recovery and suggest that damage to the upper limb motor pools should not necessarily exclude patients from receiving VNS therapy. Although animal models fail to capture the variability and complexity of SCI in patients, this study extends the range of conditions over which VNS paired with rehabilitative training improves motor recovery and supports the evaluation of closed-loop VNS therapy as a post-SCI intervention.
Plasticity in spared brain and spinal networks is widely recognized as a substrate of recovery after SCI.9-13 A number of studies demonstrate that VNS paired with rehabilitative training drives robust enhancement of synaptic plasticity after neurological injury, which likely underlies VNS-dependent benefits.16,27,29 After contusive damage to the rubrospinal and propriospinal tracts, VNS paired with rehabilitative training drives substantial reorganization of synaptic connectivity in the spared corticospinal tracts to increase motor drive onto forelimb alpha motor neurons. 29 Alternatively, after damage to the dorsal corticospinal tract, VNS paired with rehabilitative training facilitates synaptic plasticity in the largely spared rubrospinal and propriospinal tracts to similarly increase motor drive. 29 The improved motor recovery observed in the present study is consistent with the notion that VNS enhances synaptic plasticity in spared motor networks to increase the drive onto the remaining alpha motor neurons controlling the distal forelimb. Considered together, these findings indicate that VNS supports synaptic plasticity to increase motor output to compensate for impairments resulting from damage to either white matter or alpha motor neurons. We elected to utilize a bilateral contusion lesion model in this study, as the vast majority of SCI patients present with incomplete contusive damage that is not strictly localized to a single side of the spinal cord. Because VNS likely improves recovery by enhancing plasticity onto spared networks, the absence of connectivity in a complete injury model or total loss of alpha motor neurons controlling distal musculature would be expected to preclude any VNS-dependent benefits. Incorporating regenerative strategies that restore lost connectivity with VNS to enhance reorganization in newly connected circuits may represent a novel combinatorial therapeutic regimen to intervene after complete SCI.13,45 Future studies are needed to clarify both the nature of VNS-dependent reorganization after SCI as well as the neural mechanisms that support this plasticity.
Generalization of functional improvements to similar tasks is a key feature of effective rehabilitative therapies. In addition to task-specific enhancement of recovery observed on the isometric pull task, VNS paired with rehabilitative training yielded increased post-SCI forelimb function on 2 similar, but untrained, tasks. Rats that received VNS paired with task-specific rehabilitative training on the isometric pull task demonstrated increased spontaneous forelimb use as measured by the cylinder task and improved forepaw grip strength. While the cylinder task is typically used to evaluate forelimb asymmetry after unilateral injury, the observations here are suggestive of an improvement of volitional forelimb use after VNS therapy. While we cannot rule out that the increases in grip strength may reflect spasticity, the concordant improvements in volitional forelimb pull force suggest increased motor control. These findings provide an initial demonstration that VNS paired with task-specific training results in benefits that generalize to similar forelimb movements, consistent with previous studies. 27 This generalization of recovery likely arises from synaptic plasticity of inputs to spared alpha motor neurons that contribute to muscular control common across tasks. For instance, reorganization of synaptic connectivity to alpha motor neurons that exert control over digit grasp muscles would improve performance on both the isometric pull task and the grip strength task, as control of grasp musculature is a key feature in executing both tasks. In practical terms, generalization indicates that rehabilitation should include a broader range of task-specific exercises to yield the greatest benefits.
VNS-dependent benefits were observed for 1 week after the cessation of stimulation in the present study. This is consistent with the hypothesis that VNS enhances synaptic plasticity to support recovery. A previous study in a rat model of stroke demonstrates that VNS-dependent motor recovery persists for at least 6 weeks after the conclusion of therapy, indicative of long-term benefits. 27 Moreover, a clinical study in chronic stroke patients provides evidence that motor improvements in subjects receiving VNS paired with rehabilitation persist at 30 days after the completion of stimulation. 30 Thus, we expect that the VNS-dependent improvements in motor function in the present study is likely to be long-lasting. However, future studies should directly evaluate the durability of VNS-dependent recovery in the context of SCI.
A number of other neurostimulation-based therapies, including epidural stimulation, have shown promise to improve function after SCI.45-51 The precise mechanisms that mediate restoration of function remain unclear, but stimulation likely increases excitability in sensorimotor and proprioceptive networks to support motor control. 52 This strategy of directly promoting activity in spinal circuits is distinct from the presumptive enhancement of plasticity supraspinal connectivity onto spared spinal networks driven by VNS paired with rehabilitation. Thus, investigation of the combinatorial interventions that couple pharmacological and electrical stimulation to promote movement with VNS during rehabilitation may leverage the utility of both strategies.
Recent clinical studies evaluating VNS to improve motor function are consistent with results from preclinical studies and highlight the translational potential of this strategy. 15 In a double-blind, placebo-controlled study in chronic stroke patients, VNS paired with rehabilitation was safe and significantly improved upper extremity function compared to the similar rehabilitation without stimulation, confirming results of a preceding open-label study.30,31 The present study builds on the promising clinical and preclinical data and supports the potential of VNS therapy as a strategy to improve motor function after SCI.
Supplemental Material
C78_SCI_supplment_revised_final – Supplemental material for Vagus Nerve Stimulation Paired With Rehabilitative Training Enhances Motor Recovery After Bilateral Spinal Cord Injury to Cervical Forelimb Motor Pools
Supplemental material, C78_SCI_supplment_revised_final for Vagus Nerve Stimulation Paired With Rehabilitative Training Enhances Motor Recovery After Bilateral Spinal Cord Injury to Cervical Forelimb Motor Pools by Michael J. Darrow, Miranda Torres, Maria J. Sosa, Tanya T. Danaphongse, Zainab Haider, Robert L. Rennaker, Michael P. Kilgard and Seth A. Hays in Neurorehabilitation and Neural Repair
Supplemental Material
SCI_C8_SuppFig1_final_BnW – Supplemental material for Vagus Nerve Stimulation Paired With Rehabilitative Training Enhances Motor Recovery After Bilateral Spinal Cord Injury to Cervical Forelimb Motor Pools
Supplemental material, SCI_C8_SuppFig1_final_BnW for Vagus Nerve Stimulation Paired With Rehabilitative Training Enhances Motor Recovery After Bilateral Spinal Cord Injury to Cervical Forelimb Motor Pools by Michael J. Darrow, Miranda Torres, Maria J. Sosa, Tanya T. Danaphongse, Zainab Haider, Robert L. Rennaker, Michael P. Kilgard and Seth A. Hays in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
We would like to thank Andrea Ruiz, Dr. Eric C. Meyers, Tabarak M. Mian, Mays Alshaikhsalama, Wongani Kalengamaliro, Jimmy Tran, Forrest Smith, Armin Seyedahmadi, Mian Yasir Bilal, Mbuini Ghogomu, Eliezer Diaz, Fatima Ahmad, and Nicholas Foreman for technical assistance.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of the article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MPK has a financial interest in MicroTransponder, Inc, which is developing VNS for stroke. RLR is a co-owner of Vulintus, Inc, which makes rodent behavioral testing systems, and owner of Teliatry, which is developing a novel VNS device. All other authors declare no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (NIH) R01 NS094384 (SAH), R01 NS085167 (MPK), and R01 NS103803 (RLR); and the Wings for Life Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.