
Abstract
Background. Sedentary behavior is a growing public health concern and may have particular relevance for the Parkinson disease (PD) population. However, the influence of sedentary time on factors associated with quality of life (QOL) in PD is unknown. The primary purpose of this study was to examine relationships between sedentary behaviors and markers of PD-specific QOL. A secondary purpose was to examine relationships between physical activity behaviors and QOL. Methods. We assessed sedentary and active behaviors using objective and interview measures and examined relationships between these behaviors and a measure of PD-specific QOL in individuals with PD. Results. Results demonstrated that sedentary time was significantly related to several aspects of QOL, including perceived deficits in the domains of mobility, cognitive processing, and communication. Additionally, results showed that time spent watching television was more strongly associated with lower levels of QOL than other more engaging sedentary activities. For physical activity, relationships between objective measures and QOL were weaker and only significantly associated with mobility. Time spent doing housework was associated with lower levels of QOL, whereas time spent in recreational activity was associated with lower levels of discomfort. Discussion. These results suggest that targeting decreases in sedentary behaviors (eg, reducing time spent watching television, breaking up prolonged bouts of sedentary time) may be effective for improving QOL in individuals with PD.
Introduction
Parkinson disease (PD) is the second most common neurodegenerative disease in older adults and is associated with functional decline and decreased quality of life (QOL).1,2 Characterized by cardinal symptoms, including tremor, slowness (bradykinesia), rigidity, and postural instability, individuals with PD are also at increased risk for falls and cognitive decline.3,4 Current front-line treatments, including medications and surgery, decrease the severity of many symptoms, but the majority of individuals with PD continue to experience lower levels of QOL than their peers.5,6 Exercise is beneficial for PD and has been shown to improve QOL in this population.7,8 However, adherence to a physically active lifestyle is poor and decreases with disease progression. 9 Thus, identifying additional modifiable behaviors with potential for promoting well-being and maintenance of function is warranted.
Time spent sedentary may be one such set of behaviors. Distinct from inactivity, sedentary time refers to time spent sitting or lying down while awake with a low level of energy expenditure. 10 Over the past decade, sedentary time has received an increasing amount of attention as a modifiable behavior linked with higher risk for a variety of deleterious health outcomes, including diabetes, cardiovascular disease, and depression among others.11,12 Notably, this increased risk is seen even in individuals who meet public health recommendation for physical activity, suggesting it is an independent predictor of health and well-being.11,13,14
Sedentary behavior may have particular relevance for PD. Prevalence of sedentary time increases with age and is higher in individuals with chronic health conditions.15,16 Reflective of this, there is evidence that persons with PD are highly sedentary, spending a large number (~10 hours) of their waking hours in sedentary behaviors. 17 Moreover, research shows that these individuals accumulate their sedentary behavior in longer bouts than peers without PD, 18 a pattern of accumulation that has been associated with mobility disability in older adults and other patient populations.19,20 Finally, individuals with PD often have a fear of falling, which may result in increased sedentary time.21,22 However, the influence of sedentary time, including different patterns of accumulation and domains, on factors associated with QOL in PD is unknown.
The primary purpose of this study was to examine relationships between sedentary behaviors and markers of PD-specific QOL. Relationships between physical activity behaviors and QOL were also examined and descriptively compared with those for sedentary time. We hypothesized that higher amounts of sedentary time, and especially that which is accumulated in prolonged bouts, as well as lower amounts of physical activity would be associated with poorer QOL.
Methods
Participants
Participants were community-dwelling individuals diagnosed with PD who were recruited from the counties surrounding Iowa State University using an existing registry and through word of mouth at a statewide convention for individuals with PD. Inclusion criteria were a diagnosis of PD, the ability to walk without an assistive device, and no cognitive impairment (Mini-Mental Status Exam > 25). Data were collected throughout the year during 2015 and 2016. The institutional review board at Iowa State University approved the procedures of this study, and informed consent was obtained from all participants.
Procedures
Participants completed a demographic form and underwent a cognitive assessment with the Mini-Mental State Examination to determine study eligibility. 23 A subset of the sample (n = 17) also completed the Unified Parkinson’s Disease Rating Scale (UPDRS) and provided information on disease duration. They were then issued 2 activity monitors to objectively assess active and sedentary behaviors. Monitors were worn during waking hours for approximately 1 week: the ActiGraph GT3X+ accelerometer (ActiGraph, LLC, Fort Walton Beach, FL), worn on the hip, and the activPAL3 (AP; PAL Technologies Ltd, Glasgow, UK), worn on the thigh. Appropriate placement for both monitors was demonstrated, and each participant put the monitors on in front of one of the study personnel to ensure accuracy. Participants were also asked to complete a log sheet for each day the monitor was worn that detailed wear time as well as the time they went to bed and awoke each morning. Participants returned the monitors 1 week later and completed additional assessments of sedentary time, physical activity, and QOL, as described below.
Measures
Activity Monitors
The ActiGraph GT3X+ (AG; ActiGraph LLC, Pensacola, FL) is a small (4.6 × 3.3 × 1.5 cm3), light (19 g) triaxial accelerometer that records acceleration ranging between ±6g. It samples acceleration at a rate of 30 to 100 Hz, which is then digitized through a 12-bit analog-to-digital converter. The GT3X+ was initialized at 100 Hz, and data were preprocessed into 1-s epochs using the ActiLife software (version 6.5.1). For the purposes of this study, counts per second from each of the 3 axes were utilized for further processing, as detailed below.
The AP is a small (35 × 35 × 7 mm3), light (15 g), capacitive, triaxial accelerometer that collects data in the range of ±2g. The AP digitizes acceleration data (sampled at 20 Hz) through an 8-bit analog-to-digital converter. In the current study, the AP was placed on the midpoint of the anterior surface of the right thigh. For the purposes of this study, the activity classification component (sitting, standing, stepping) and the boundaries between different activities (eg, change from standing to stepping) were utilized from the AP software’s Events.csv output file.
Questionnaires
Sedentary and active behaviors were also assessed via interview. Sedentary behavior was assessed using the Sedentary Behavior Questionnaire. 24 This questionnaire asks about sedentary behaviors across different domains (eg, watching television/movies, computer use). Each activity is queried for weekdays and weekend days, with choices including none, 15 minutes or less, 30 minutes, and 1 to 6 hours in hourly increments. Average sedentary hours per day is then calculated as well as hours per day specific to each domain. Physical activity was assessed using the International Physical Activity Questionnaire. 25 This questionnaire was designed to assess physical activity in different domains of life (eg, recreation, transportation) over the past 7 days. This questionnaire has demonstrated acceptable levels of validity for assessing physical activity in older adults.26,27 For the purposes of this study, minutes per day for moderate and vigorous physical activity (MVPA) were calculated for each domain as well as in total. For both interview assessments, the interviewer was blinded to accelerometer data.
PD-specific health-related QOL was assessed with the Parkinson’s Disease Questionnaire-39 (PDQ-39). 28 This questionnaire is widely used in PD and results in 8 dimensions (mobility, activities of daily living, emotional well-being, stigma, social support, cognition, communication, and bodily discomfort) and an overall score referred to as the PD Summary Index. Scores for each domain were summed and expressed as a percentage. A higher percentage indicates a greater disruption or dissatisfaction within a domain. The total PDQ-39 summary index score was determined by summing the scores across all 8 domains and dividing by the total number of domains (ie, 8). 29 The index can range from 0 (indicative of perfect health) to 100 (worst health).
Data Processing and Statistical Analyses
ActiGraph and activPAL monitors were initialized and downloaded on the same computer, such that their internal time stamps would match to facilitate postprocessing, as detailed below. These data were first processed using their associated software packages (ActiLife 6.13.3 and PAL Analysis 7.2.32) with outputs at the 1-s epoch. Days that included at least 10 hours of wear time were considered to be valid days. These data were integrated via their timestamps and further analyzed using the Sojourns Including Posture method. 30 This method has been shown to provide a high level of validity for the full range of behaviors from sedentary to vigorous in comparison to both direct observation and indirect calorimetry. 30 Output from this processing method was then used to calculate the primary behavioral outcomes for the study, including minutes of sedentary and light-intensity physical activity, sedentary time accumulated in longer (>30 minutes) bouts, and minutes of MVPA and steps. To be included in the analyses, participants had to have a minimum of 4 valid days, including 1 weekend day.
The distribution of all scores for all metrics was tested for normality using the Shapiro-Wilk test. All subscales for the PDQ-39 violated normality as did several metrics associated with self-reported sedentary time and physical activity. Therefore, nonparametric statistics were performed for analyses that included these variables. To characterize active and sedentary behaviors, means and SDs (or medians and interquartile ranges, for nonnormal variables) for primary outcomes were calculated from the self-report and accelerometer data.
To explore relationships between sedentary and active behaviors and health-related QOL, Spearman’s ρ correlations were then calculated between interview and objective measures and the summary index and subscales of the PDQ-39. A follow-up linear regression analysis was then conducted on the subset of the sample with clinical data to further examine the influence of active and sedentary behaviors in conjunction with the potential contributions of clinical markers on QOL. In this analysis, independent variables included prolonged sedentary time, MVPA, disease duration, and disease severity (total UPDRS), and the PDQ Index was the outcome variable. For all analyses, significance was accepted at level P <.05. Analyses were performed using SPSS Statistics 24 (IBM, 2016).
Results
A total of 52 participants with PD enrolled in the study, and 45 had complete accelerometer data. The full sample was 67.8 ± 7.9 years of age, and 56% were male. They were 98.1% white; 80.8% were married, 69.2% had a college degree, and 89% were retired. Participants were 1.7 ± 0.1 m tall and weighed 79.0 ± 16.5 kg with a body mass index in the overweight range at 26.4 ± 4.1. In the subset of participants who completed the UPDRS, total scores averaged 57.4 ± 19.4, and these individuals reported having PD for an average of 10.0 ± 6.7 years. PDQ-39 data are shown in Table 1, and sedentary and active behaviors are shown in Tables 2 and 3.
Scores on the PDQ-39 (n = 52). a
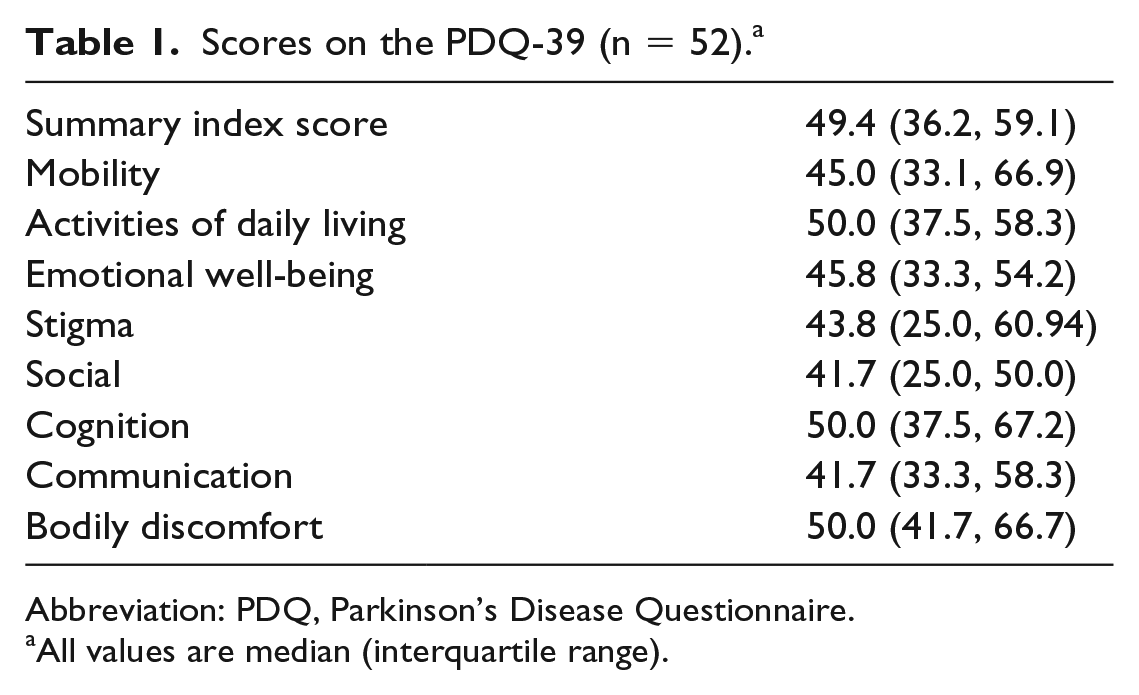
Abbreviation: PDQ, Parkinson’s Disease Questionnaire.
All values are median (interquartile range).
Sedentary Behaviors (n = 45).
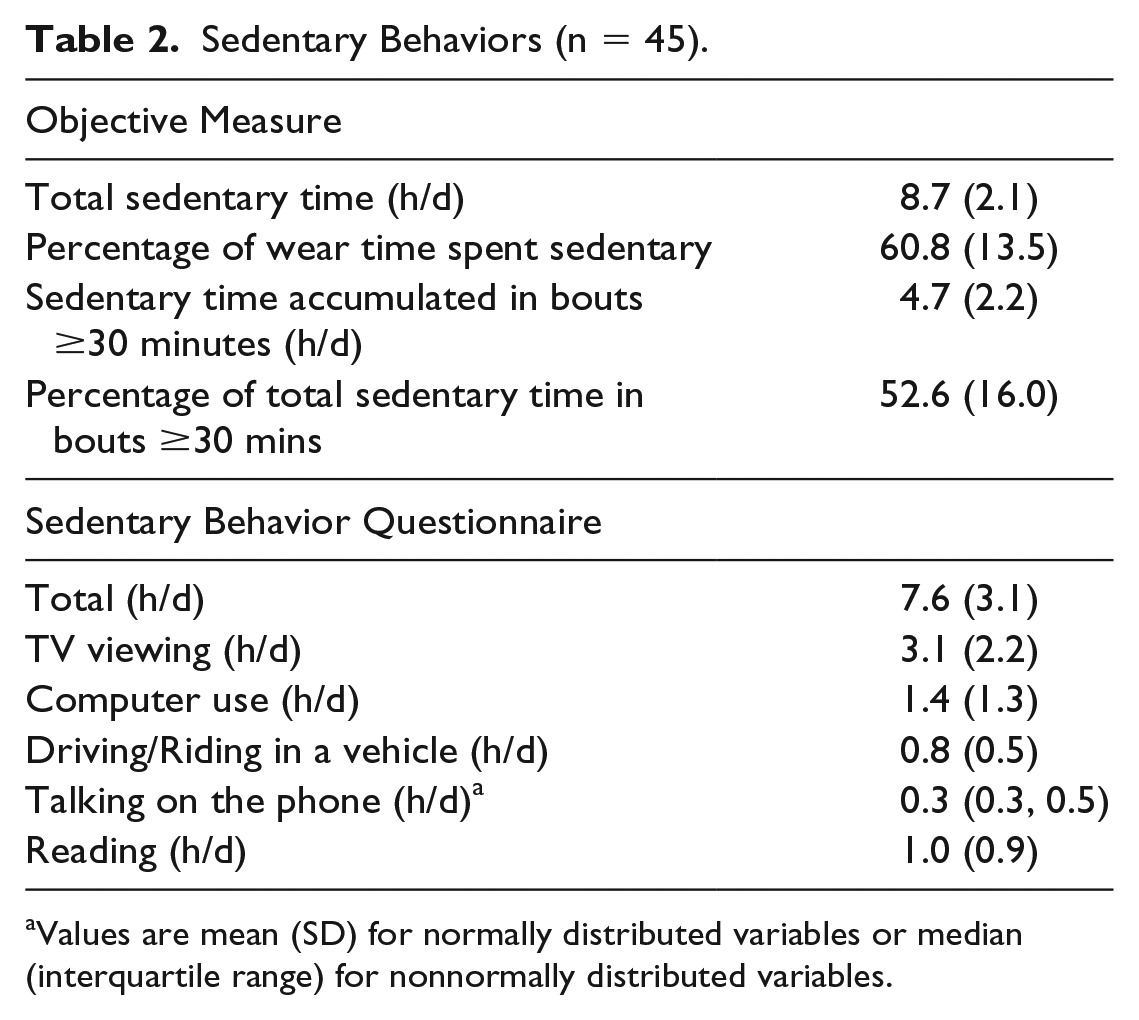
Values are mean (SD) for normally distributed variables or median (interquartile range) for nonnormally distributed variables.
Physical Activity Behaviors for the Full Sample and Based on PDQ Score.
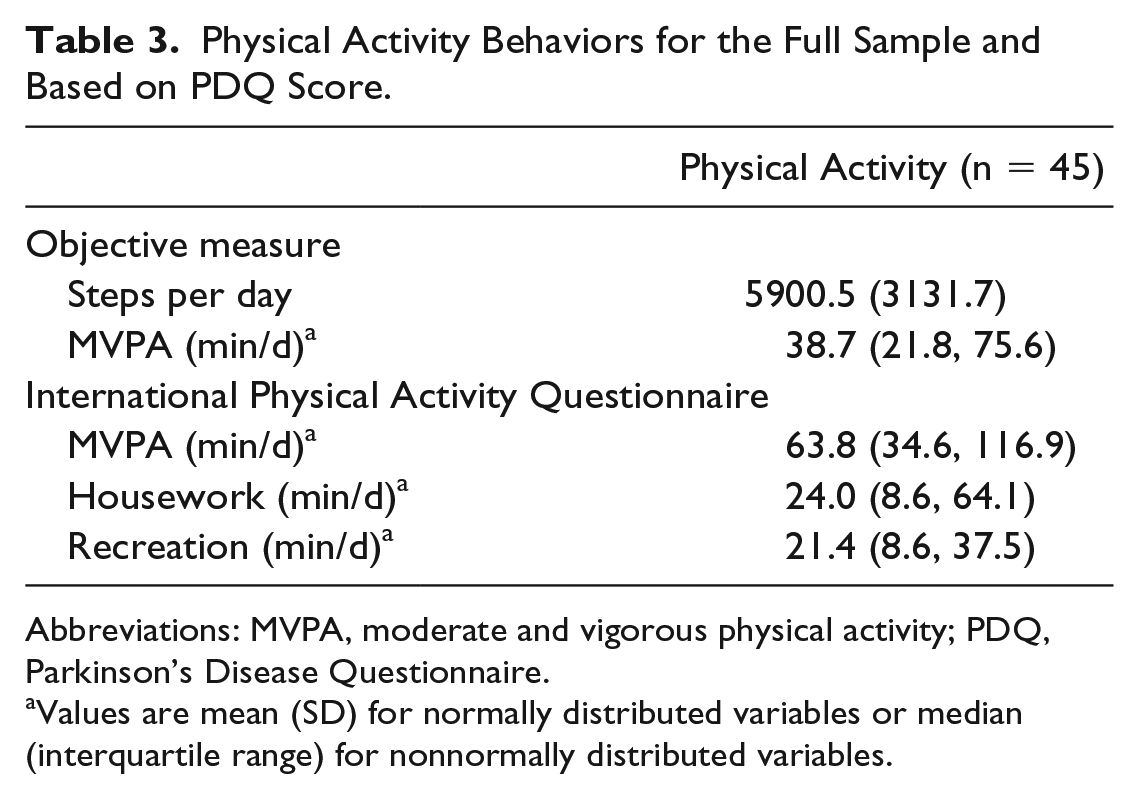
Abbreviations: MVPA, moderate and vigorous physical activity; PDQ, Parkinson’s Disease Questionnaire.
Values are mean (SD) for normally distributed variables or median (interquartile range) for nonnormally distributed variables.
Participants wore their accelerometers for an average of 14.3 ± 1.6 h/d. Of this time, approximately 8.7 ± 2.1 hours was spent sedentary with more than half of this sedentary time (~52.6%) accumulated in bouts of at least 30 minutes. Sedentary time reported during the interview was approximately an hour less at 7.6 ± 3.1 h/d. The most commonly reported sedentary activities were watching television, using the computer, reading, and driving/riding in a vehicle. Less than 10% of participants reported engaging in sedentary behavior while listening to music, playing an instrument, or doing arts and crafts. Therefore, these behaviors were not included in further analyses.
For physical activity behaviors, accelerometer data showed that participants accumulated an average of 5900.5 ± 3131.7 steps per day and a median (IQR) of 38.7 (21.8, 75.6) minutes of MVPA. Based on current recommendations for steps per day, 31 35.5% of participants (n = 16) would be classified as sufficiently active. During the interviews, participants reported a larger amount of MVPA, with a median (IQR) of 63.8 (34.6, 116.9) min/d. The most commonly reported domains for accumulating MVPA were recreation and housework. Because less than 25% of the sample reported any work-related or transportation-related physical activity, these activities were excluded from further analyses.
As shown in Table 4, relationships between objective measures of sedentary time and QOL demonstrated that higher amounts of sedentary time accumulated in prolonged bouts were most consistently associated with worse scores on the PDQ summary index (ρ = 0.34; P < .05) as well as subscales of mobility, cognitive, and communication (ρrange = 0.32-0.41; P < .05). For the interview measures, the most consistent relationships were seen for higher amounts of time spent watching television being associated with lower QOL for the index score (ρ = 0.35; P < .05) as well as for subscales of mobility, emotion, social, cognitive, and communication (ρrange = 0.29-0.39; P < .05).
Spearman’s ρ Correlations Between PDQ-39 and Objective and Self-Report Measures of Sedentary Time (n = 52).
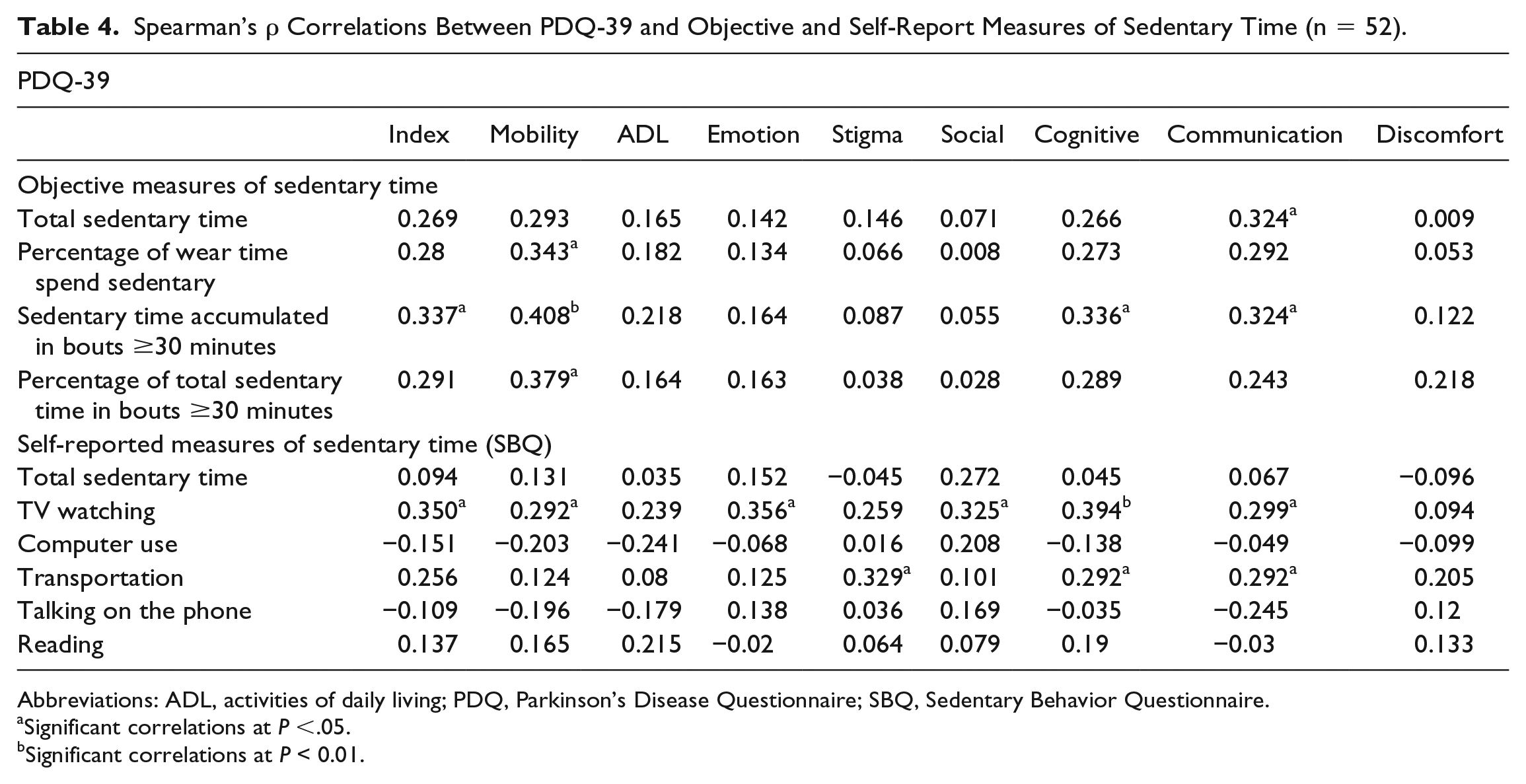
Abbreviations: ADL, activities of daily living; PDQ, Parkinson’s Disease Questionnaire; SBQ, Sedentary Behavior Questionnaire.
Significant correlations at P <.05.
Significant correlations at P < 0.01.
As shown in Table 5, relationships between QOL and physical activity behaviors were less consistent than those for sedentary time. For objectively measured behaviors, accumulating more steps per day was negatively associated with the mobility subscale (ρ = −0.41; P < .05); time spent in MVPA was not significantly associated with QOL. For the interview measure, greater time spent doing housework was associated with poorer QOL for the social, emotion, and stigma subscales (ρrange = 0.29-0.33; P < .05), whereas time spent in recreation was associated with lower levels of discomfort (ρ = −0.33; P < .05).
Spearman’s ρ Correlations Between PDQ-39 and Objective and Self-report Measures of Physical Activity (n = 52).
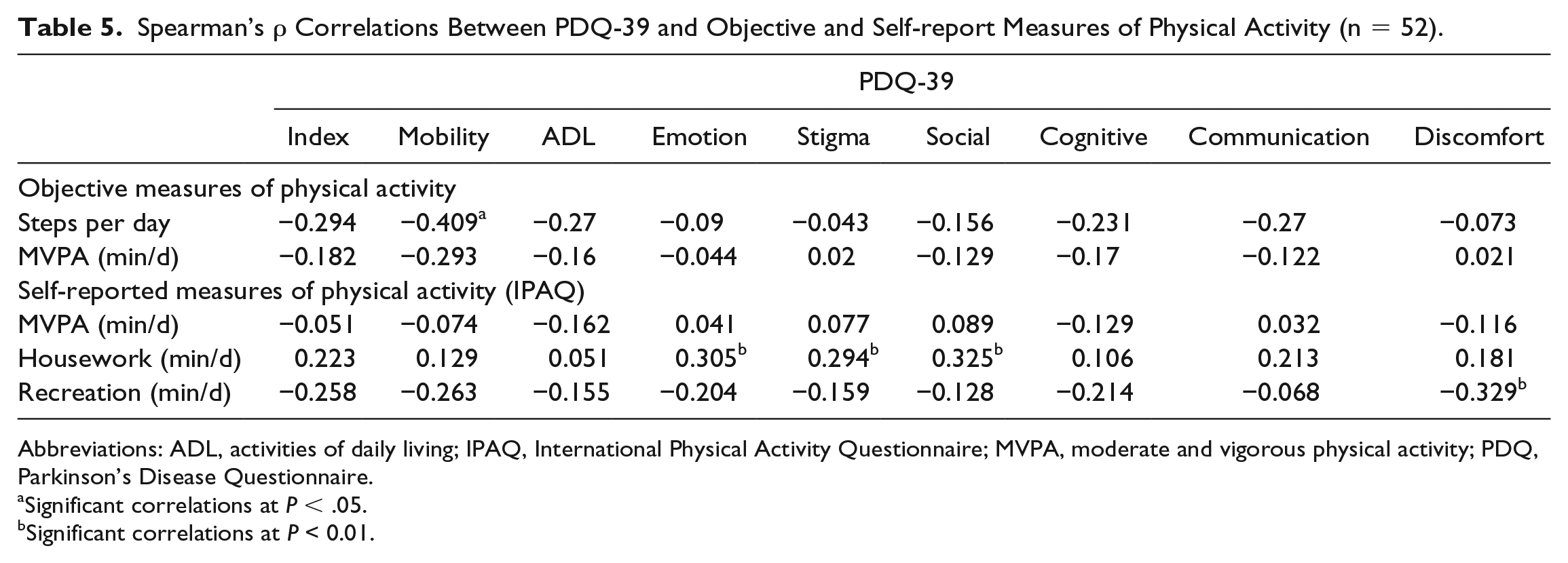
Abbreviations: ADL, activities of daily living; IPAQ, International Physical Activity Questionnaire; MVPA, moderate and vigorous physical activity; PDQ, Parkinson’s Disease Questionnaire.
Significant correlations at P < .05.
Significant correlations at P < 0.01.
These results are consistent with the regression analysis performed on a subsample of the data set. As shown in Table 6, sedentary behavior accumulated in prolonged bouts was a significant predictor for the PDQ Index (β = 0.47; P = .04) as was disease severity (β = 0.52; P = .03). Minutes of MVPA was not a significant predictor in any of the analyses (P = .28).
Regression Analyses Results (n = 17).
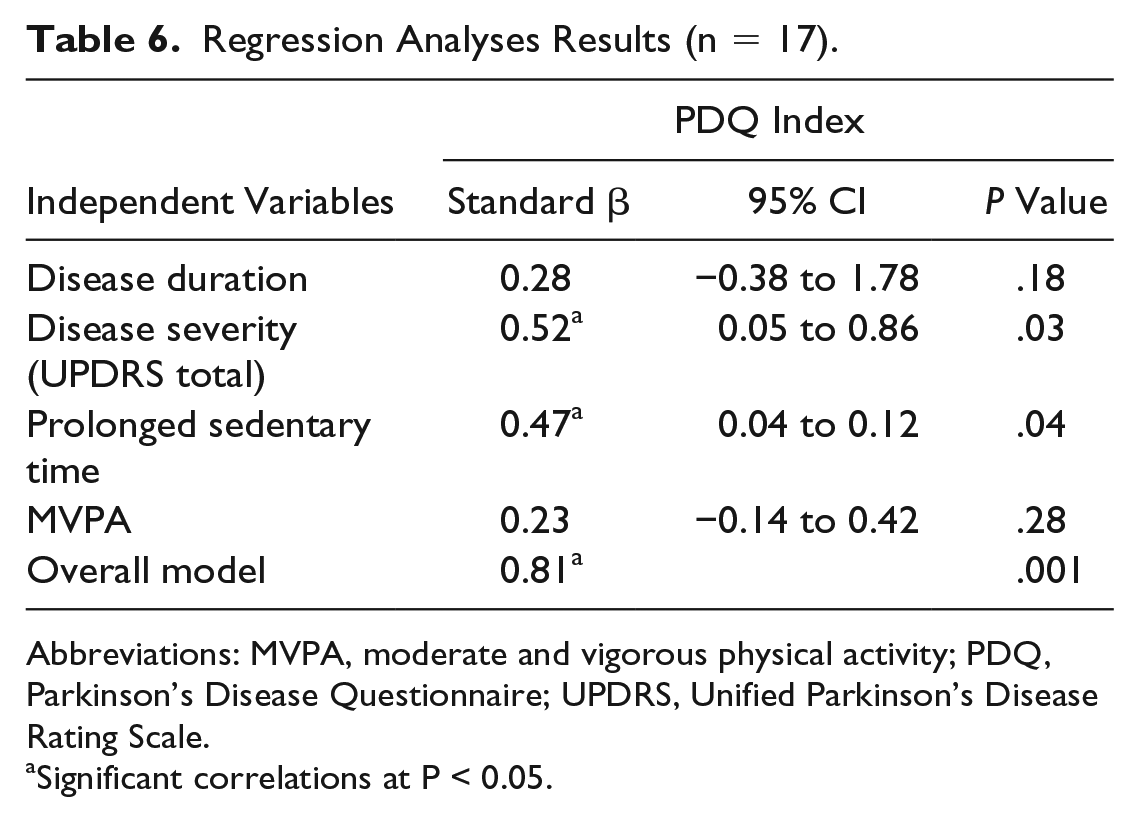
Abbreviations: MVPA, moderate and vigorous physical activity; PDQ, Parkinson’s Disease Questionnaire; UPDRS, Unified Parkinson’s Disease Rating Scale.
Significant correlations at P < 0.05.
Discussion
The present study shows that sedentary behaviors may have important relevance for individuals with PD. Specifically, results demonstrated that sedentary time was significantly related to several aspects of QOL, including perceived deficits in the domains of mobility, cognitive processing (eg, memory, concentration), and communication (eg, difficulty with speech, feeling ignored). Moreover, results showed that sedentary time accumulated in prolonged bouts was more strongly associated with QOL than total sedentary time and that time spent watching television was more strongly associated with lower levels of QOL than other, more engaging sedentary activities such as computer use or talking on the phone.
Our results also demonstrated that physical activity had more limited relationships with QOL. Although objectively measured physical activity was significantly related to perceived deficits in mobility, it was not associated with the summary index score, a measure of overall QOL. Furthermore, when examining physical activity by domain, more time spent doing recreational activity was associated with lower levels of discomfort, whereas greater time spent doing housework had a negative influence on several aspects of QOL. This may reflect that individuals with PD take longer to complete everyday housework because of their disease and may have less time for recreational activities that they enjoy.
When active and sedentary behaviors were included together in the same analyses along with clinical measures of PD, results were largely consistent with the correlations. Specifically, prolonged sedentary time was predictive of QOL, whereas physical activity was not. Additionally, disease severity was also a significant predictor of QOL. Thus, sedentary time may be an important behavior to consider in conjunction with disease severity for promoting QOL in individuals with PD.
The results from this study regarding the influence of physical activity on QOL were surprising because there is substantial evidence that individuals with PD who participate in structured exercise interventions show improvements in QOL.7,8 Furthermore, a recent study by van Uem et al 32 examined the influence of objectively measured physical activity on QOL in patients with PD and found that total energy expenditure was positively associated with QOL in this population, suggesting that regular daily physical activity was beneficial. However, with the exception of this study, little is known about the influence of regular daily activity levels on QOL in this population. The paucity of data in this area suggests that further research is needed to understand what aspects of movement are most beneficial for individuals with PD, including factors such as intensity and type, as well as the domain in which it occurs.
The findings regarding sedentary time are consistent with the single study we are aware of that has examined sedentary behavior and QOL in PD. 32 This study objectively measured sedentary behavior and correlated it with the PDQ Summary Index, Mobility, and Activities of Daily Living subscales and found that average sedentary bout length was significantly associated with mobility and ability to perform activities of daily living. However, their measure of sedentary time included sleep, which is a behavior with profoundly different (and largely positive) health consequences. Therefore, the present work adds to the literature showing that sedentary time is important in PD by parsing out sleep and focusing on waking hours of sedentary time.
The sedentary results are also consistent with a growing body of research examining relationships between sedentary behavior and QOL in older adults and in other geriatric patient populations. A recent critical review authored by an international panel of experts highlighted the importance of sedentary behavior for factors associated with geriatric syndrome, a constellation of conditions that include cognitive, functional, and mobility-related impairments that are common among older adults, including those with PD. 33 Consistent with our findings, the authors highlight evidence to date linking high amounts of sedentary time to mobility limitations, cognitive impairment, and overall assessments of QOL. Similarly, sedentary time has been linked to QOL in older adults with arthritis, 34 dementia, 35 and congestive heart failure, 36 among other conditions. Taken together, the results from the present study add to the literature showing that sedentary behavior has a pervasive influence on QOL, specifically in the domains of mobility and cognition, in the aging population regardless of disease or disability.
Strengths
An important strength of the present work is the use of a validated, objective monitoring device to assess sedentary time in individuals with PD. Additionally, sedentary time was also assessed via interview, allowing the examination of which sedentary activities are most associated with QOL in PD. Because sedentary behavior is ubiquitous for most adults and spans a variety of domains, including passive activities such as watching television, cognitively demanding activities such as computer use, social activities such as enjoying a meal with friends, and instrumental activities such as transportation, it is likely that different activities have different consequences for QOL. Indeed, our results demonstrated that watching television was associated with a decrease in QOL over multiple domains, whereas other sedentary activities were unrelated. Thus, results of this study highlight the importance of using objective measures in conjunction with more descriptive tools when assessing the potential relevance of behaviors such as sedentary time for well-being.
Limitations
This study has several limitations. It is cross-sectional in nature. Thus, the causal direction of relationships between sedentary time and QOL cannot be determined. Additionally, the sample size was relatively small, and there is limited disease-specific information, which may limit the interpretation of the results. The sample was also limited to a demographic area within the state of Iowa. Environmental factors, such as weather, rural living, and access to care, may have influenced the results. As such, the results of this study may not extend to individuals with PD living in other areas. Furthermore, the sample of individuals with PD was relatively active, with more than 30% meeting guidelines for steps per day, and thus, results may differ in individuals with a less active lifestyle. Finally, clinical data were only available on a subsample of participants. Future studies should include measures such as disease severity and duration as well as other clinical measures such as depression and anxiety to understand how this constellation of factors influences QOL.
Conclusion
Behavioral treatments are needed for individuals with PD to improve symptoms and address issues surrounding QOL and maintenance of independence. Although there is evidence that exercise has substantive benefits for these individuals,7,8 adherence is often poor because of barriers that include lack of time, poor health, and depression. 37 Because sedentary behavior is not subject to many of these obstacles and is significantly related to QOL, targeting this set of behaviors may be a viable option for improving symptoms long term and positively influencing QOL in this population. Intervention studies specifically targeting reductions in prolonged sedentary time (eg, decreasing time spent watching television, breaking up bouts of sedentary time with standing or walking) and assessing changes in QOL will be a crucial next step in determining the influence of this set of behaviors on disease progression and QOL.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.