
Abstract
Background. Recovery of the sit-to-stand (StS) movement early after stroke could be improved by targeting physical therapy at the underlying movement deficits in those people likely to respond. Aim. To compare the movement characteristics of successful and failed StS movements in people early after stroke and identify which characteristics change in people recovering their ability to perform this movement independently following rehabilitation. Methods. Muscle activity and kinematic (including center of mass, CoM) data were recorded from 91 participants (mean 35 days after stroke) performing the StS movement before (baseline), immediately after (outcome), and 3 months after (follow-up) rehabilitation. Three subgroups (never-able [n = 19], always-able [n = 51], and able-after-baseline [n = 21]) were compared at baseline with the able-after-baseline subgroup compared before and after rehabilitation. Results. The subgroups differed at baseline for quadriceps onset time (P = .009) and forward body position when quadriceps peaked (P = .038). Following rehabilitation, the able-after-baseline subgroup increased their forward position (P < .001), decreased the time difference between bilateral quadriceps peaks (P < .001) and between quadriceps and hamstrings peaks on the nonhemiplegic side (P = .007). An improved performance in the always-able subgroup was associated with a number of baseline factors, including forward positioning (P = .002) and time difference between peak activity of bilateral quadriceps (P = .001). Conclusions. This neuromechanical study of StS before and after rehabilitation in a sample of people early after stroke identified the importance of temporal coupling between forward trunk movement and quadriceps and hamstrings’ activity. These findings advance the science of stroke rehabilitation by providing evidence-based therapy targets to promote recovery of the StS movement.
Introduction
Rehabilitation is known to improve physical function after a stroke. 1 Movement repetition is the key principle for this rehabilitation 2 with the quality of movement considered important in traditional theories. 3 Clarifying the characteristics of a movement that should be emphasized during practice could optimize outcomes through tailoring rehabilitation activities (targeted therapy). This could be achieved by distinguishing the kinematic and muscle activity variations between successful and failed attempts at functional tasks performed by impaired populations as well identifying the variables associated with improved ability after rehabilitation.
Considered to be one of the most physically challenging functional movements, 4 the sit-to-stand (StS) task is nevertheless performed frequently as part of everyday activities. 5 An impaired ability will inevitably threaten an individual’s ability to live independently. 6 Recovering this movement is therefore included in stroke rehabilitation guidelines with a recommendation for frequent practice. 7
Laboratory-based biomechanical studies of healthy people have identified 2 key features of a successful StS movement. First a forward trunk lean while seated measured between 22.2° ±7.8° 8 and 38.8° ± 8.1°, 4 to the vertical. This movement is typically performed at velocities around 87 deg/s. 9 Although this relatively high velocity is considered desirable in terms of efficiency it is not essential to success. 10 Second, the generation of a downward force on the ground that exceeds body weight during the rising phase.11-13 Studies of failed StS attempts have complemented these findings. Reduced forward displacement while seated and vertical forces less than body weight have both been described during failed attempts by older adults (n = 13) affected, predominantly, by vestibular hypofunction and in a single case of traumatic brain injury.14,15 While contributing to our understanding of StS these findings have a limited influence on stroke rehabilitation practice.
A biomechanical approach to analyzing movement is clearly informative but provides only indirect evidence of the underlying muscle activity. This is particularly limiting if the population of interest has a neurological impairment. Electromyographical (EMG) studies of the StS movement in healthy participants point to a consistent temporal pattern of muscle activation, in particular, the agonist muscle activity (hip and knee extensors) needed to create the vertical force to lift the body up during the rising phase. Quadriceps and hamstring muscle groups are observed to reach simultaneous levels of peak activity around the commencement of the rising phase.16-19 Generating the force necessary to lift the body is clearly easier if both legs contribute equally. 20 Symmetrical activation of the hip and knee extensors to produce this net moment, while not an absolute determinant of success, is likely to be an important factor 11 for safe and frequent movement. EMG studies of the StS movement among people after a stroke are inconsistent in their findings but generally report altered muscle activation times on the hemiplegic side.17,21 The value of these studies to understanding recovery of this movement after stroke is limited by the recruitment of participants long after their stroke (eg, 3.5 years 21 ), lack of data before and after rehabilitation, and not including failed StS attempts in the analysis.
This study aimed to provide therapy targets for StS training early after stroke by comparing the neuromechanical characteristics of successful and failed StS movements and then identifying the movement characteristics associated with a change in ability (ie, changing from failed to successful movement) and performance immediately following a 6-week rehabilitation intervention and 3 months thereafter.
Methods
The study reported here was embedded in an observer-blind, multicenter, randomized controlled early phase trial. Full protocol details, including the intervention, are provided in an earlier publication. 22
Briefly, baseline measures were conducted with participants who were subsequently randomized to 1 of 3 subgroups: conventional physiotherapy (CPT), CPT + movement performance therapy (MPT), or CPT + functional strength training (FST). The intervention period lasted 6 weeks. Outcome measures were recorded immediately after the end of the intervention period and 12 weeks thereafter. The local Research Ethics Committees covering the clinical centers granted ethical approval (Merton and Sutton Ethics Committee, 205cl01). The trial was registered on a clinical trials database (NCT00322192).
Our previous publications reported no statistical difference in StS performance across the 3 intervention subgroups.22,23 The analysis reported here therefore considers the sample as a single group.
Participants
All participants provided written informed consent and met the following criteria:
In-patients aged 18+ years who were between 1 and 13 weeks of a stroke (hemorrhage or infarction) in the territory of the anterior circulation.
Able to produce some voluntary contraction of their paretic lower limb muscle (ie, scoring at least 28/100 on lower limb section of the Motricity Index. 24
Able to follow 1-step verbal commands and were independently mobile, with or without aids, prior to the index stroke with no lower limb orthopedic surgery or trauma in the lower limb in the previous 8 weeks or any previous history of neurological disease other than stroke.
Interventions
The CPT group received 9.2 (SD 6.9) hours of rehabilitative exercises/activities as determined by the clinical physiotherapist which included, but was not limited to: soft tissue mobilization, facilitation of muscle activity, facilitation of coordinated multijoint movement, tactile and proprioceptive input, resistive exercise, and functional retraining. 22
The CPT + MPT group received 23.0 (SD 10.4) hours of an intervention that combined CPT (as described above) and MPT, which emphasized the recovery of movement quality through movement repetition with facilitation and feedback provided by a therapist. 22
The CPT + FST group received 23.5 (SD 10.0) hours of an intervention that combined CPT (as described above) and FST, which focused on repetitive, progressive resistive exercise during goal-directed functional activities. The differential for this treatment group was the use of graded resistance by manipulating the gravitational moment acting on the whole body and limbs, increasing the range of movement or distance over which bodyweight was transported, and simply changing the weight of external objects. 22
The StS Movement Task
Participants were instructed to stand up 5 times from a plinth adjusted to the height of their knee. The starting position for all participants was sitting on the plinth with both thighs parallel to the ground, both ankles directly below the knees and the trunk perpendicular to the thighs. The upper limbs were positioned so that they hung freely alongside the thighs. Participants were asked not to use their hands for support or to push up from the plinth during the movement attempt. Participants wore tight fitting clothing to improve the quality of the motion capture and footwear usually worn for therapy sessions. To ensure the activity did not result in a fall, a physiotherapist supervised all attempts but did not provide any physical assistance. An audio trigger instructed the participant to commence the task, this trigger was also used to synchronize the measurement instruments.
Only movements that met the task success criteria (no hands, aids, or support used) and had every segment tracked throughout the movement with complete data, were used for analysis. In cases where the movement was not successfully completed (ie, a failed attempt) the first clear purposeful attempt (where the body moves forward with a clear attempt to lift the body) was used for analysis.
Data Collection and Analysis
Kinematic Data
Eight Vicon motion cameras (Oxford Metrics, Oxford, UK) captured the 3-dimensional trajectories of retroreflective markers attached to the body at anatomical locations at a sampling rate of 120 Hz. The trajectories were then processed by filling any small gaps (<10 frames) with a spline fill function and filtered with a low-pass (cutoff frequency 6Hz) sixth-order Butterworth filter to reduce the noise content of the signal. Once processed a geometric model, consisting of 15 body segments (head, trunk, upper arms, forearms, hands, pelvis, thighs, lower legs, and feet), was constructed using proprietary software (Nexus, Oxford Metrics, Oxford, UK), which allowed anatomical angles and the overall center of mass (CoM) to be calculated from the weighted average of the 15 tracked segments. These data were used to derive the following temporal events commonly used in sit to stand analysis.
Onset event: First occurrence (time point) of a forward movement of the CoM that lasted at least 10 frames.
Seat-off event: First occurrence (time point) of increasing upward CoM velocity that lasted at least 10 frames.
End event: First occurrence (time point) of the CoM reaching it maximal vertical displacement.
These events allowed the movement to be separated into 2 phases; phase 1: onset to seat-off; phase 2: seat-off to end, as well as a value for total movement duration (onset to end).
Muscle Activity
A surface telemetric electromyography (EMG) system (MT8, MIE Medical Research Ltd) was used to record the electrical activity of 2 agonist/antagonist muscle pairs: quadriceps/hamstrings and tibialis anterior/gastrocnemius on both sides during the task. Data from 8 muscle groups were therefore available for analysis; however, only the hamstrings and quadriceps muscles on both sides were analyzed. The consistent pattern of their activity, close temporal coupling and function as prime movers to lift the body distinguished these muscles as being fundamental to movement success compared to the tibialis anterior/gastrocnemius pair which are more inconsistent in their activity and considered to act, primarily, as stabilizers and not prime movers. 18 The system sampled the data at 1080 Hz and was synchronized with the kinematic capture software (Nexus, Oxford Metrics, Oxford, UK) using a synchronization pulse. The preparation and positioning of the EMG electrodes followed SENIAM guidelines. 25 The raw EMG signals were processed into a linear envelope (full wave rectification low-pass filter [cutoff frequency 6 Hz] and integration) using a custom-made Matlab (Mathworks Inc, Natick, MA, USA) program. Muscle onset times were identified from a threshold detection algorithm of the signal exceeding a baseline mean (+3 standard deviations), 18 which was calculated from 1000 frames preceding the start signal. The time of peak muscle activity was identified with a peak detection function (Matlab, Mathworks Inc, Natick, MA, USA). Muscle onsets and peaks were timed relative to the movement onset event. Temporal relationships between muscle pairs (hamstrings and quadriceps on each side and quadriceps on opposite sides) were calculated as an absolute time difference.
Demographic (age and gender) and stroke specific information (time since stroke, and hemiplegic side) were recorded from the medical notes. The presence of neglect was assessed with the star cancellation test 26 with a score between 0 and 49 indicating neglect. The Modified Rivermead Mobility Index 27 and gait speed (measured over a flat 10 m walkway) were recorded by the research team.
Statistical Analysis
The demographic, stroke, clinical, and neuromechanical variables at baseline were summarized for the 3 separate subgroups: never-able; always-able; and able-after-baseline. The neuromechanical variables were selected a priori based on the available literature. Chi-square and T tests were used to compare the able-after-baseline and never-able subgroups. A 1-factor analysis of variance (ANOVA) tested for statistically significant changes in the neuromechanical variables of the able-after baseline subgroup between baseline, outcome, and follow-up.
Finally, a statistical analysis was undertaken to identify factors associated with improved StS performance after rehabilitation in the always-able subgroup (n = 51), this was the only subgroup with successful attempts at each time point. A linear regression model was fitted using the outcome of movement time separately for each variable and then a variable selection technique was used to identify which factors were independently associated with improvement.
All analyses were conducted using standard statistical software packages (Minitab, version 17 and Stata version 14).
Results
Full data sets were available from 91 participants at 3 time points (baseline, outcome, and follow-up, a CONSORT diagram is available in the supplementary material.
Baseline Differences
The baseline characteristics were described for the 3 subgroups and statistically tested between the never-able and able-after baseline subgroups (see Table 1). CoM position at the time of peak quadriceps activity (hemiplegic side) was statistically different (P = .038), with the never-able subgroup less far forward (68.86 ±82.70 mm) than the able-after-baseline sub-group (128.87 ± 73.55 mm). Quadriceps onset time (hemiplegic side) was also statistically different (P = .009), occurring much earlier in the never-able subgroup (0.91 ± 0.63 seconds) compared to the able-after-baseline subgroup (1.73 ± 1.08 seconds).
Summary of Participants and Their Sit-to-Stand Neurobiomechanical Characteristics, Mean (SD) and Count (Percentage) at Baseline, Separated Into the 3 Sit-to-Stand Ability Subgroups.
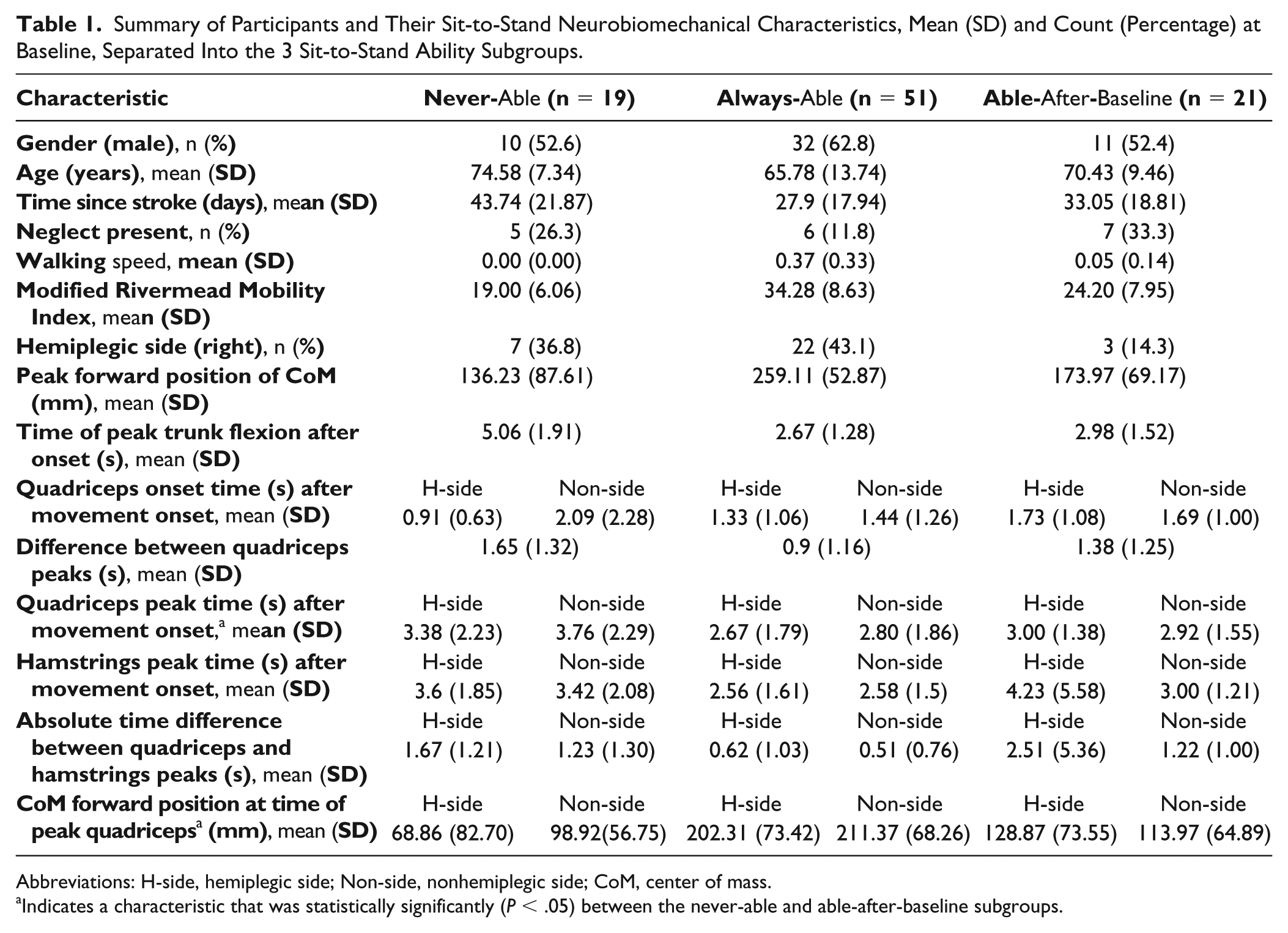
Abbreviations: H-side, hemiplegic side; Non-side, nonhemiplegic side; CoM, center of mass.
Indicates a characteristic that was statistically significantly (P < .05) between the never-able and able-after-baseline subgroups.
Response to Rehabilitation
As the only participants who recovered their StS ability (ie, from being unable to being able), the movement characteristics of the able-after-baseline subgroup were described at each time point (see Table 2). Four statistically significant differences were found using a 1-factor (time), ANOVA:
Peak forward position of the CoM increased from 173.97 (69.17) mm at baseline to 273.20 (57.60) mm at outcome and 279.30 (44.30) mm by follow-up (P < .001).
CoM forward position at the time of peak quadriceps on both the hemiplegic (P < .001) and nonhemiplegic sides (P < .001). At the time of peak quadriceps activity on the hemiplegic side, the CoM forward position increased from 128.87 (73.55) mm at baseline, to 226.30 (71.40) mm at outcome and was unchanged at follow-up. On the nonhemiplegic side, the CoM forward position, at the time of peak quadriceps, increased from 114.00 (164.90) mm at baseline to 220.30 (78.40) mm at outcome and then 231.90 (43.60) mm by follow-up.
The time difference between peak quadriceps activity on the hemiplegic and nonhemiplegic sides changed significantly over time (P = .000). The time difference decreased from 1.38 (1.25) seconds at baseline to 0.45 (0.59) seconds at outcome and then slightly increased to 0.52 (0.83) seconds at follow-up.
The time difference between hamstrings and quadriceps peaks on the nonhemiplegic side changed significantly over time (P = .007), whereas a significant difference was not found for the hemiplegic side (P = .058). The time difference between hamstring and quadriceps peaks on the nonhemiplegic side decreased from 1.22 (1.00) seconds at baseline to 0.41 (0.52) seconds at outcome and then increased to 0.67 (0.80) seconds at follow-up.
Neuromechanical Characteristics of the Able-After-Baseline Subgroup at Baseline, Outcome, and Follow-up.
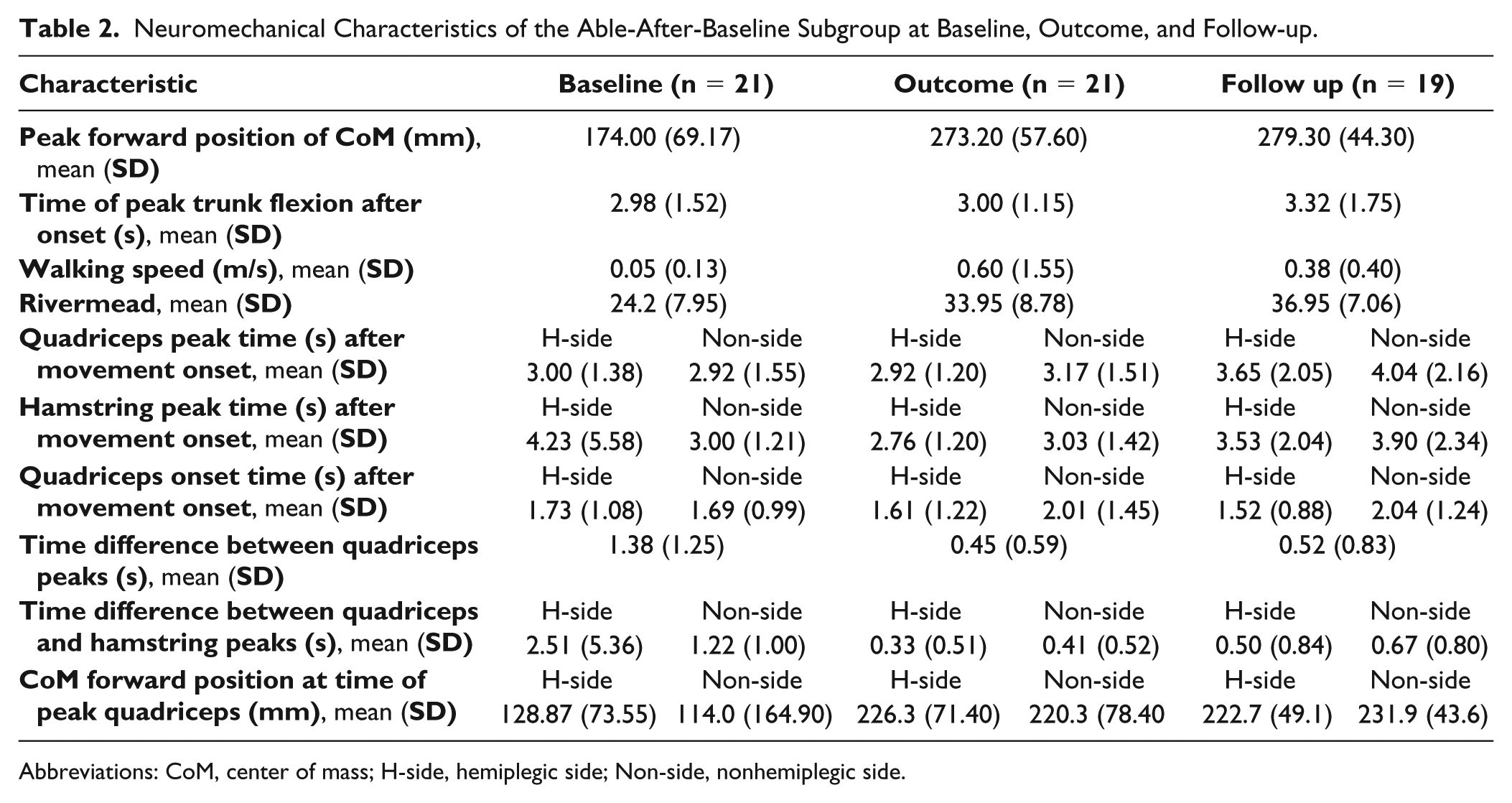
Abbreviations: CoM, center of mass; H-side, hemiplegic side; Non-side, nonhemiplegic side.
Baseline Characteristics Associated With Improved Performance
At baseline the movement duration (onset until end) for the always-able subgroup was 3.51 (2.01) seconds, this decreased to 2.56 (1.38) seconds at outcome (P = .001) and to 2.34 (1.39) seconds by follow up (P = .000). The linear regression analysis found 11 neuromechanical and 1 stroke-related baseline characteristic (neglect) to be significantly associated with this improvement by follow-up (Table 3). The neuromechanical characteristics related to the temporal synergy across the muscles involved in raising the body (quadriceps and hamstrings on the hemiplegic and nonhemiplegic sides) and ability to bring the body forward. Participants with neglect showed less improvement.
Association of Baseline Characteristics With an Improved Sit-to-Stand Movement Time at Follow-up for the Always-Able Subgroup.
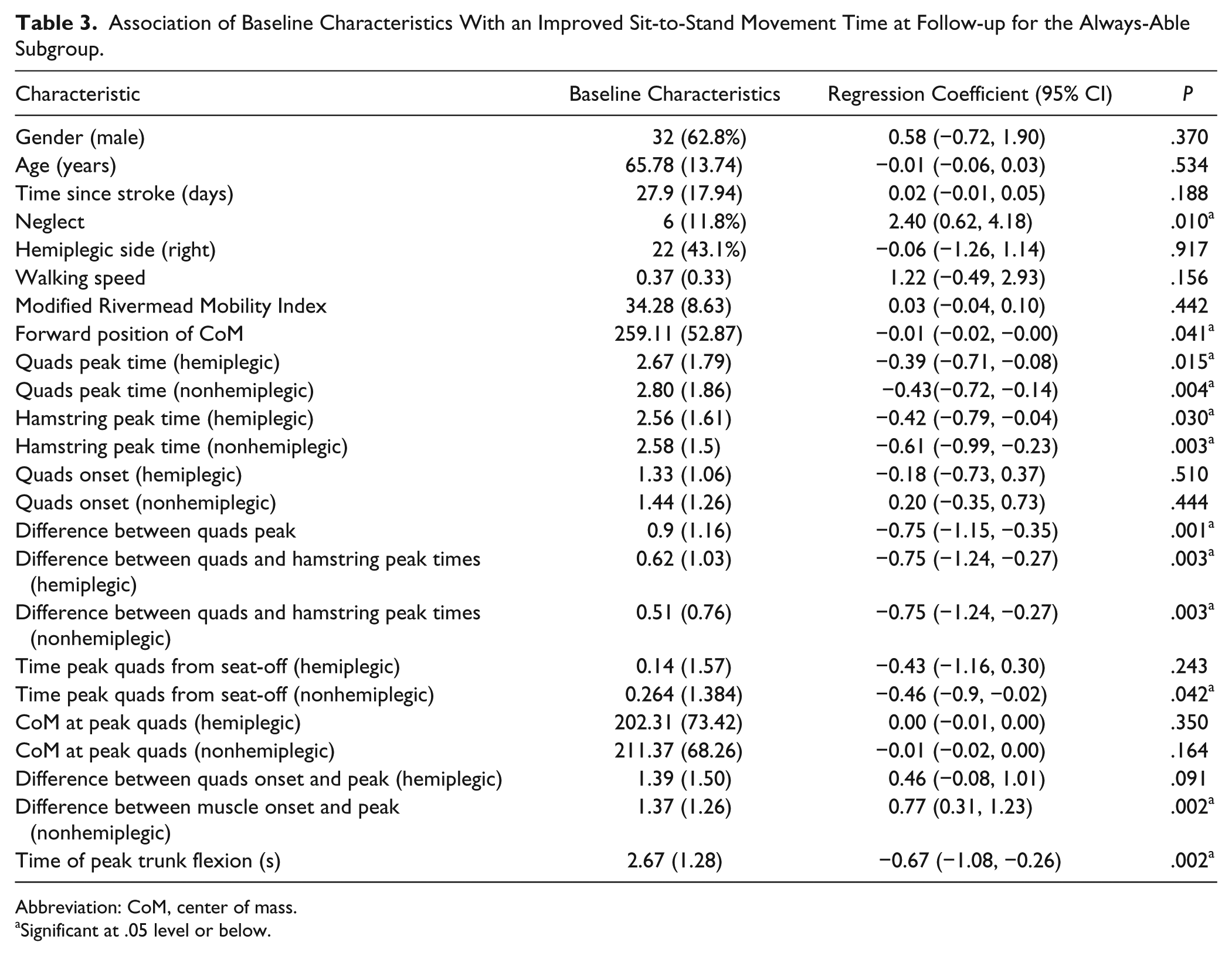
Abbreviation: CoM, center of mass.
Significant at .05 level or below.
Discussion
This study is the first study to describe the neuromechanical differences between successful and failed StS movement attempts in people early after a stroke and then track these movement variables in response to rehabilitation. With an aim of identifying therapy targets, analysis focused on the subgroup of people who recovered StS independence following rehabilitation, that is, participants who changed from being unable to being able. In sum, the able-after-baseline subgroup differed statistically at baseline from the never-able subgroup in their ability to time peak quadriceps activity when the body was much further forward. Following rehabilitation, this subgroup increased the forward movement of their body, reduced the time difference between peak quadriceps’ bilaterally and between quadriceps and hamstrings on the nonhemiplegic side.
Unsurprisingly the subgroups, never- able (n = 19), always-able (n = 51) and able-after-baseline (n = 21) differed statistically at baseline. These differences related to forward movement of the body (CoM) and timing quadriceps’ activity to when a greater amount of this forward movement had occurred. This confirms previous reports on the importance of bringing the body forward before generating peak extensor moments at the hip and knee, to lift the body mass. 28 Generating peak knee extensor activity when the body mass has not been brought sufficiently far forward (eg, only 6 cm in the never-able subgroup) is likely to result in a fall back. 14 Elements of the basic movement pattern appear to be retained in the able-after-baseline subgroup with forward displacement and quadriceps timings similar to the always-able subgroup.
Peak activity of the hamstring muscle group was timed closely with the quadriceps peak in the always-able subgroup (hemiplegic side 0.61 seconds, nonhemiplegic side 0.51 seconds). This co-contraction of agonist/antagonist pairs might seem counterintuitive but has been observed before during StS movements 29 probably due to the need to generate large hip and knee extensor moments, simultaneously, around seat-off.
While age and time since stroke did not vary significantly between the never-able and able-after-baseline subgroups at baseline it is notable that the never-able subgroup were both the oldest and had the longest delay before rehabilitation. Age is consistently cited as a factor in functional recovery 30 and a delay in rehabilitation raises the possibility of confounding factors such as comorbidities. The lack of statistical variance across the subgroups for mobility (Modified Rivermead Mobility Index) and stroke specific factors, such as neglect and hemiplegic side, were surprising but may relate to the small subgroup sizes. Using a baseline Modified Rivermead Mobility Index score of 18.5, Shum et al 31 predicted 88% of patients being able to walk 1 month after stroke, interestingly, in our study, this cutoff was exceeded by the able-after-baseline subgroup (24.20) but very similar to the never-able subgroup (19.00).
Two subgroups improved their StS ability following rehabilitation, 19/38 (50%) of individuals unable to perform the movement at baseline, changed to being independent in the movement at follow-up, a success rate similar to previous studies. 32 The movement characteristics that changed in these individuals is arguably the most interesting part of this study as it provides potential therapy targets. Greater forward movement and closer timing between bilateral quadriceps and unilateral hamstrings/quadriceps point to a development in movement skill following rehabilitation, with greater co-ordination between muscles to generate vertical lift at the optimal time. 17 Close timing between quadriceps and hamstrings has been reported previously with Khemlani et al 18 observing virtually synchronous onsets of the rectus and biceps femoris muscles in healthy adults. Finding closer muscle timings between the hemiplegic and nonhemiplegic sides, builds on previous reports of improved symmetry following rehabilitation in this population.23,33
Statistically faster performance times after rehabilitation are common among stroke populations already independent in the StS movement.1,32 In our study, this improvement was associated not only with earlier muscle timings relative to movement onset, as might be expected in a faster movement, but also the retention after stroke of a close synergy between the forward positioning of the body and peak activity of bilateral quadriceps and ipsilateral hamstrings and quadriceps on the nonhemiplegic side. These factors, it would appear, are crucial not only for recovering movement independence, as discussed earlier but also for decreasing movement time which is a commonly used outcome measure in rehabilitation trials. 1
Limitations
A strength of the present study was the preselection of a relatively small number of variables clustered around muscle timing (onset and peak) and position of the CoM, which were informed by previous findings.13,17,21,23,32 Consequently, the study was hypothesis driven. However, this preselection does raise the possibility that we missed an important factor. Knee extension velocity, for example, has been identified as a sensitive measurement for StS. 34 A subsequent study could explore a more extensive range of variables.
The decision to remove tibialis anterior and gastrocnemius muscles from the analysis was intended to reduce the data by focusing on the muscles generating the extension moments for the lifting phase, considered the most demanding part of the StS movement.6,29 Tibialis anterior and gastrocnemius activity has been observed before during the StS movement, particularly during the preparatory period to stabilize the foot and lower leg and may have been useful in understanding motor control in this subgroup. Future studies might explore the role of other muscles during successful and failed attempts before and after rehabilitation.
Another potential limitation is the sample size. Although larger than most studies of this nature, it is possible that some of the associations found in this study might not be representative of a larger population. We recommend these findings are tested in future larger studies.
Despite these limitations, this was a robustly executed study of the StS movement before and after rehabilitation in a large sample of people early after stroke. The findings are an important step toward clarifying the important motor features of a successful StS and identifying potential factors for predicting responders to rehabilitation so that interventions can become more tailored and effective. 35
Practice Implications
Based on our findings, a forward displacement of 20 cm while seated would seem a reasonable therapy target. This can be created by a forward trunk lean of approximately 25° to 30° to the vertical, which is a more clinically accessible metric. The other key targets for rehabilitation are the timings of peak activity in the quadriceps and hamstrings muscle groups relative to each other and the forward position of the body. Although this information is well known among physiotherapists, 36 the present findings confirm this clinical knowledge and provide numerical references. Incorporating this knowledge into the provision of feedback for individuals after stroke would provide a practical way to translate this knowledge into clinical practice. For example, EMG biofeedback systems could be used to provide muscle timing information, perhaps combined with simple motion tracking systems to promote the synchronization between the forward lean and the quadriceps/hamstrings synergy. These findings will help design future prospective trials targeted at recovering independence and improving performance in this important everyday movement.
Conclusion
This large study of failed and successful StS movements before and after rehabilitation in people early after stroke provides therapy targets for regaining independence and improving movement performance. The temporal coupling of bilateral quadriceps with hamstrings activity to coincide with the forward positioning of the body differed significantly between failed and successful attempts before rehabilitation and then changed significantly in the subgroup of participants who regained independence in this movement. This study provides the evidence to support therapy targeting these movement characteristics and lays the foundation to develop feedback methods, including the use of technology, to promote the recovery of this important everyday movement.
Supplemental Material
Supplementary_Material_Consort_flow_chart – Supplemental material for Neuromechanical Differences Between Successful and Failed Sit-to-Stand Movements and Response to Rehabilitation Early After Stroke
Supplemental material, Supplementary_Material_Consort_flow_chart for Neuromechanical Differences Between Successful and Failed Sit-to-Stand Movements and Response to Rehabilitation Early After Stroke by Andy Kerr, Allan Clark and Valerie M. Pomeroy in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
We gratefully acknowledge funding provided by The Healthcare Foundation for the trial into which this experimental study was embedded. We also thank Dr Emma Cooke and Professor Raymond Tallis for their contributions to the concept, design, and conduction of the previously published clinical efficacy trial. In addition, we thank Ashraf Sameja for assistance with data collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by The Healthcare Foundation for the trial into which this experimental study was embedded.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.