
Abstract
Background: Persistent deficits in arm function are common after stroke. An improved understanding of the factors that contribute to the performance of skilled arm movements is needed. One such factor may be self-efficacy (SE). Objective: To determine the level of SE for skilled, goal-directed reach actions in individuals with mild motor impairment after stroke and whether SE for reach performance correlated with actual reach performance. Methods: A total of 20 individuals with chronic stroke (months poststroke: mean 58.1 ± 38.8) and mild motor impairment (upper-extremity Fugl-Meyer [FM] motor score: mean 53.2, range 39 to 66) and 6 age-matched controls reached to targets presented in 2 directions (ipsilateral, contralateral). Prior to each block (24 reach trials), individuals rated their confidence on reaching to targets accurately and quickly on a scale that ranged from 0 (not very confident) to 10 (very confident). Results: Overall reach performance was slower and less accurate in the more-affected arm compared with both the less-affected arm and controls. SE for both reach speed and reach accuracy was lower for the more-affected arm compared with the less-affected arm. For reaches with the more-affected arm, SE for reach speed and age significantly predicted movement time to ipsilateral targets (R2 = 0.352), whereas SE for reach accuracy and FM motor score significantly predicted end point error to contralateral targets (R2 = 0.291). Conclusions: SE relates to measures of reach control and may serve as a target for interventions to improve proximal arm control after stroke.
Introduction
Persistent deficits in arm function are common after stroke. Although rehabilitation interventions can improve arm function, recovery is often incomplete, with large variation in response to training across individuals.1,2 Additionally, improvements in functional capacity do not always translate into increased arm use in everyday life.3,4 Further understanding the factors that contribute to the performance of skilled arm movements after stroke may help inform the development of novel approaches to arm rehabilitation.
Skilled reach performance, as measured by kinematic measures of speed and accuracy, can characterize sensorimotor recovery after stroke, 5 providing important information about proximal arm control,6,7 especially in individuals with milder motor deficits.8,9 The ability to effectively and efficiently transport the arm is important for a variety of functional tasks, including placement of the hand to allow object manipulation. An understanding of the variables that contribute to the control of skilled reaching may inform the content and design of interventions aimed at improving proximal arm control after stroke. One important variable may be self-efficacy (SE).
SE is one of several personal factors that are proposed to combine to determine an individual’s motivation, affect, and performance related to a given behavior. 10 Specifically, SE refers to an individual’s confidence or perception of the prospective capability to perform a behavior at a specific level or in a given situation.10,11 This perception goes beyond holding a belief that engaging in a behavior will lead to a specific outcome (outcome expectations). SE relates to whether the individual believes that she or he can actually perform the required behavior in order to achieve the desired outcome. 12 SE is not a general or trait variable but is specific to a domain of activities or behaviors and is predictive of future behavior; higher confidence can both reflect and lead to higher levels of accomplishment and behavioral engagement.10,12,13
After stroke, SE has been shown to be a significant predictor of falls,14,15 physical function,16,17 gait function, 18 and walking activity.19,20 Overall, individuals with higher SE have fewer falls, better physical and gait function, and increased levels of walking activity than those with lower SE. SE for skilled upper-extremity (UE) tasks after stroke has not been extensively studied to date. Recently, SE and feedback indicating successful performance has been shown to relate to arm choice in a reaching task in individuals poststroke.21,22 However, it is currently not known if SE for skilled reaching predicts reach performance.
The purpose of this study was to determine the level of SE for skilled, goal-directed reach actions in individuals with mild motor impairment after stroke and whether SE for reach performance correlates with actual reach performance. We hypothesized that SE would be lower for reaches with the more-affected arm compared with the less-affected arm and nondisabled controls. Additionally, we hypothesized that SE would significantly correlate with reach performance such that individuals with lower SE would reach more slowly and with less accuracy than individuals with higher SE.
Methods
Participants
Individuals in this study were part of a parent study that investigated the control of reach extent after stroke.23,24 Participants had to be premorbidly right-hand dominant, 25 have a history of stroke at least 3 months prior, and have some movement capability in the more-affected arm (UE Fugl-Meyer [UE FM] motor score 26 ≥28). Potential participants were excluded if they presented with cognitive impairment (score <25 on the Mini-Mental State Exam 27 ), hemispatial neglect (score <52 on the BIT star cancellation test 28 ), current pain in either arm, botulinum toxin injection in the more-affected arm within the previous 3 months, or surgical intervention in either arm within the previous 6 months. All participants provided written informed consent prior to participation through a protocol approved by the Health Sciences Institutional Review Board at the University of Southern California.
Several clinical measures were performed to determine arm motor status. The UE FM motor score 26 and Action Research Arm Test (ARAT) 29 were used to determine level of arm motor impairment and arm motor function, respectively. The Stroke Impact Scale (SIS) Hand domain, 30 a patient-reported outcome measure, was used to determine perceived hand function. SE for UE functional activities was assessed using the Confidence in Arm and Hand Movements Questionnaire (CAHM). The CAHM is a 20-item questionnaire that asks the individual to rate his or her level of confidence to perform a series of functional tasks that involve the weaker arm or both arms on a scale of 0 to 100; a rating of 0 indicates very uncertain/unconfident about being able to successfully perform a task, whereas a rating of 100 indicates very certain/confident.
Reaching Task
The reaching task has been described in detail previously. 24 Briefly, individuals performed 3-dimensional reach movements to 6 targets (3.8 cm sphere) presented in 2 directions (+45°, −45°) and at 3 distances (8, 16, 24 cm; Figure 1) in a virtual environment (VE; Innovative Sports Training, Inc, Chicago, IL). Finger position was represented in the VE as a 2-cm white sphere, or cursor, that moved in real time as the participant moved the finger. At the start of each trial, the participant placed the cursor onto a Home position (2.5-cm blue sphere) that aligned with a physical start switch. After a variable foreperiod (1.3, 1.6, 1.9 s), the Home position and the cursor position disappeared and a single target appeared, at which time the participant reached to the target; the trial ended when the velocity dropped below 3 cm/s. The target was visible while reaching, but the arm and virtual cursor that represented finger position were not, thereby eliminating online visual feedback during movement. Visual postresponse feedback was provided after each trial, which showed the proximity of end point finger position to the target. If the cursor overlapped with the target (error tolerance of 2.9 cm based on object radius), the target turned green on feedback, indicating successful hit of the target on that trial. If the cursor did not overlap with the target, the target remained red during feedback. Participants were instructed to “reach to the target as fast as possible when ready”; instructions prioritized speed of movement over accuracy because one goal of this study was to investigate anticipatory planning of ballistic, goal-directed reaches to targets that varied in distance.23,24 However, the task did not impose any external time constraints on the speed of reach performance for an individual trial.
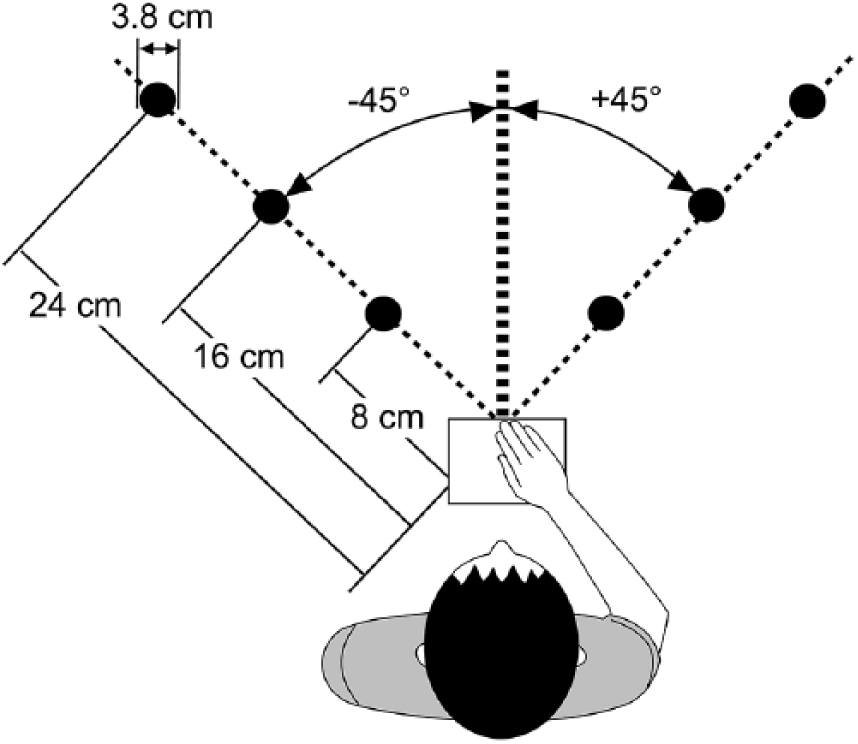
Schematic of reach paradigm. Six targets were presented in 2 directions (+45°, −45°) and at 3 distances (8, 16, 24 cm) in a virtual environment. The start switch (open square) was aligned with the sternum.
Index finger position was collected from an electromagnetic sensor at a sampling rate of 120 Hz throughout each reach trial and analyzed using a custom script in MATLAB (Mathworks, Inc, Natick, MA). Position data were filtered with a low-pass second-order Butterworth filter with a 10-Hz cutoff and differentiated to determine velocity and acceleration. 31 For each trial, peak velocity (first peak after movement onset), movement time, and end point error (3-dimensional linear distance between target and finger position at movement offset) were extracted using previously described methods. 24 Because of the well-described effect of movement direction on the magnitude of kinematic variables,32,33 data for each target direction were analyzed separately. Target direction was converted to indicate either an ipsilateral reach (right arm reaching to +45° targets, left arm reaching to −45° targets) or contralateral reach (right arm reaching to −45°, left arm reaching to +45° targets) for group analyses (see Figure 1). The effect of target distance on measures of reach performance has been previously reported in detail. 24 In the current analysis, we utilized the mean of each kinematic variable across all target distances to quantify overall reach performance similar to previous analyses. 23
Reach Self-efficacy
SE for reach accuracy and reach speed were collected prior to each block of reach trials. Before the start of data collection, participants were shown a Visual Analog Scale for rating SE that ranged from 0 (not very confident) to 10 (very confident) for 2 questions: “How confident are you that you will reach to the target accurately on the next set of trials?” and “How confident are you that you will reach to the target quickly on the next set of trials?”. Accurately was defined as receiving green on feedback (an indication of being on target); quickly was defined as reaching to the target within the allotted trial time. Participants rated accuracy SE and speed SE verbally prior to each of the 7 blocks of reach trials.
Experimental Procedure
Participants completed the reaching task with the ipsilesional arm first followed by the contralesional arm with a 30- to 60-minute break between arm sessions. For ease of discussion and presentation of results, we will refer to these as the less-affected and more-affected arms, respectively. The order of arm used first in control participants was counterbalanced. Each session began with 24 practice trials. Participants then completed 7 blocks of 24 trials (total of 168 reach trials) with each arm; the first 2 blocks were dropped from data analysis to eliminate any effects related to adjusting to the VE similar to previous analyses,23,24 leaving 120 reach trials (5 blocks) for analyses. Within each block, targets were presented in a pseudorandom order such that no consecutive trials were to the same target and each target was presented 4 times. A rest period of 2 to 5 minutes was provided between blocks.
Verbal cues related to accuracy and speed were provided throughout data collection. Cues were general in nature and primarily aimed at keeping the participant engaged in the task for the primary purpose of the experiment to investigate the planning of reach actions. Examples of accuracy verbal cues provided include “Good job” and “Close.” Examples of speed verbal cues include “Keep moving quickly” and “Good speed.”
Statistical Analysis
All data or their log transforms met the criteria for normality using the Shapiro-Wilk test (P > .05). Measures of reach performance (end point error, movement time, peak velocity) and SE (accuracy SE, speed SE) did not change over blocks in either group (P > .185 for main effect of block; see Supplemental Figures). Therefore, for group analyses, we used a mean value for reach performance and SE across blocks for each participant. A mixed-model analysis of variance with within-group factors of arm and SE type (accuracy, speed) and a between-group factor of group (control, stroke) was used to examine differences in SE. Significance level was set at P <.05 for all comparisons.
Correlation analyses between SE and kinematic measures of reach performance were performed using Pearson’s r. Because of the proposed specificity of SE, accuracy SE was correlated with a measure of reach accuracy (end point error) and speed SE with measures of reach speed (peak velocity, movement time). Additionally, the relationship between reach SE and clinical measures of arm function (UE FM, ARAT, SIS hand, CAHM) was investigated. In the control group, both arms were combined in a single comparison. Significance level for correlations was set at a corrected P <.0167.
Forward stepwise linear regression modeling was conducted to examine what variables combined to best predict reach performance with the more-affected arm. Possible predictors included SE (accuracy, speed), arm motor status (UE FM, ARAT, SIS hand, CAHM), and demographic variables (age, time poststroke). Variables that showed a bivariate correlation with reach performance (P < .1) were entered into the model (P < .1 to enter, P > .15 to leave). SPSS 22 (IBM Corp, Armonk, NY) statistical software was used for all analyses.
Results
Participants
A total of 20 individuals with chronic stroke and 6 age-matched nondisabled controls participated in this study (Table 1). Individuals in the stroke group presented with a mix of right and left arm hemiparesis and, overall, had mild motor impairment (UE FM motor score range 39-66). 34 Participants poststroke reported continued difficulty performing functional tasks with the more-affected hand (Hand SIS) and reduced confidence in completing functional tasks with the more-affected arm (CAHM). As expected, reaches with the more-affected arm were slower and less accurate than reaches with both the less-affected and control arms (Table 2). Additionally, reaches to contralateral targets were slower than reaches to ipsilateral targets with both arms (P < .001), whereas reaches to contralateral targets were less accurate than reaches to ipsilateral targets for the more-affected arm only (P = .02).
Participant Demographics. a
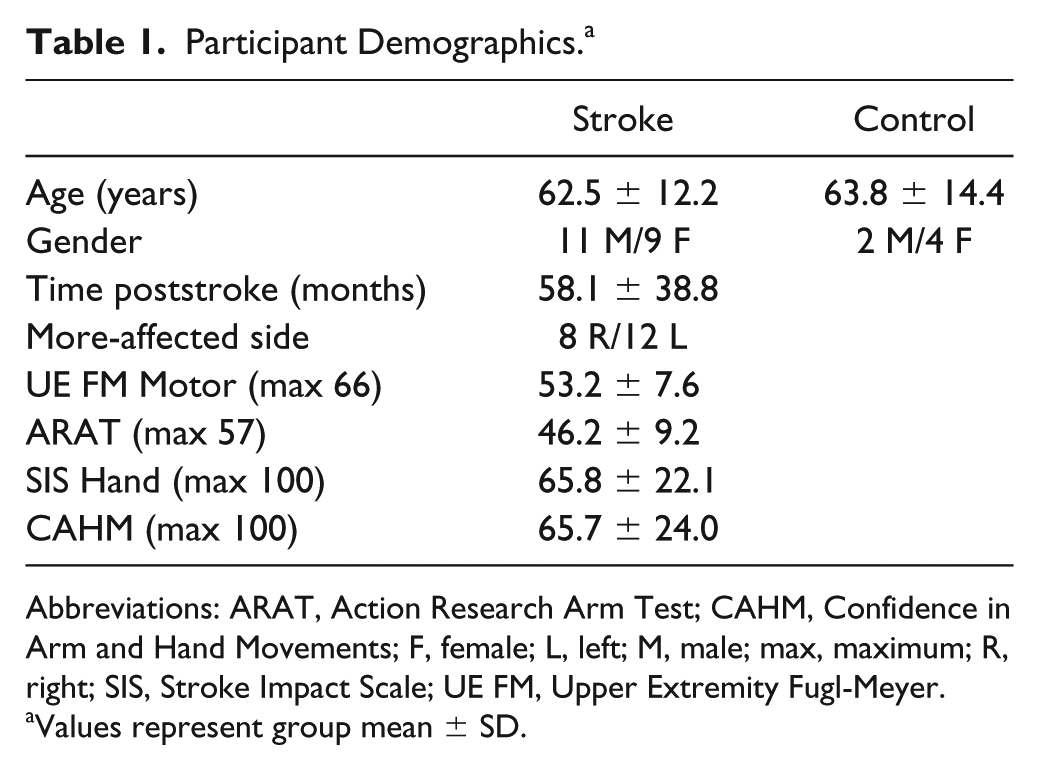
Abbreviations: ARAT, Action Research Arm Test; CAHM, Confidence in Arm and Hand Movements; F, female; L, left; M, male; max, maximum; R, right; SIS, Stroke Impact Scale; UE FM, Upper Extremity Fugl-Meyer.
Values represent group mean ± SD.
Summary of Reach Performance. a
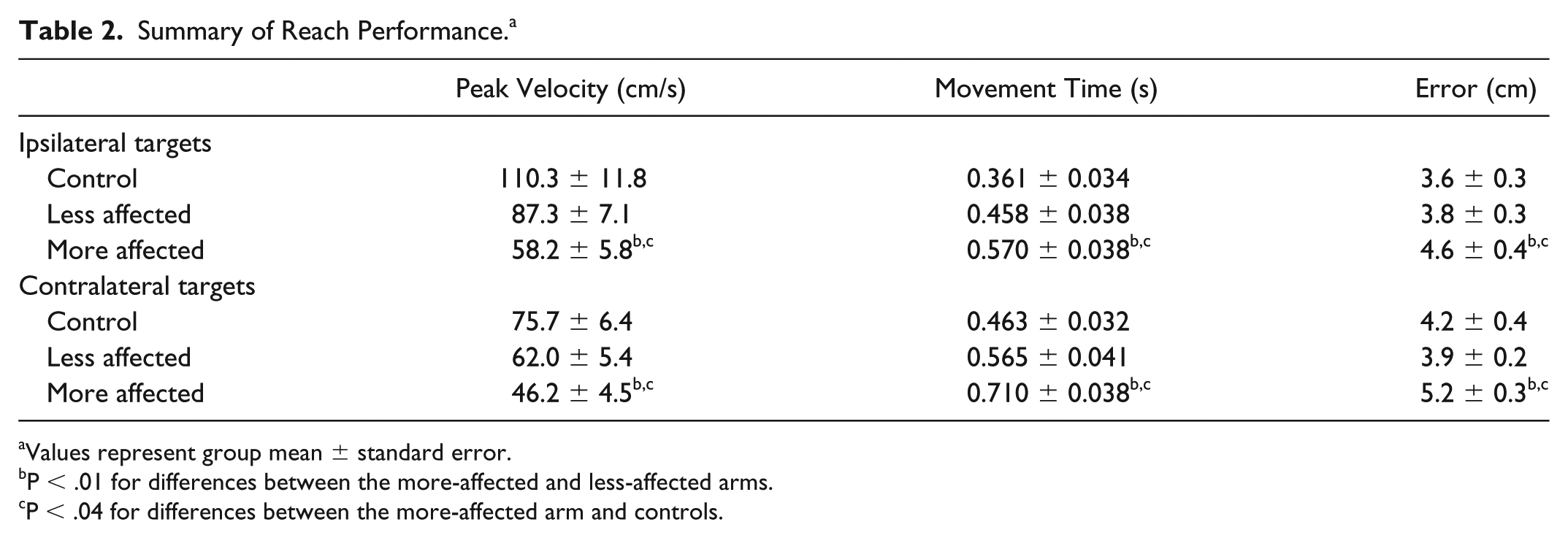
Values represent group mean ± standard error.
P < .01 for differences between the more-affected and less-affected arms.
P < .04 for differences between the more-affected arm and controls.
SE for Skilled Reach Actions
Mean SEs for accuracy SE and speed SE are shown in Figure 2 for both groups. Initial analyses indicated a significant arm by SE type by group interaction (P = .002). Therefore, a repeated-measures ANOVA was conducted separately for each group. In the control group, speed SE (right arm: 7.6 ± 1.2; left arm: 7.3 ± 1.4) was higher than accuracy SE (right arm: 5.6 ± 1.8; left arm: 5.6 ± 7.8) in both arms (P = .027 for main effect of SE type). SE did not differ between the right and left arms (P = .461 for main effect of arm), and there was no arm by SE type interaction (P = .327). In the stroke group, analyses revealed a significant main effect for arm (P < .001) and for SE type (P = .007). Overall, SE was lower in the more-affected arm (speed SE: 5.7 ± 2.0; accuracy SE: 5.0 ± 2.4) compared with the less-affected arm (speed SE: 7.4 ± 1.5; accuracy SE: 6.5 ± 1.8), and speed SE was higher than accuracy SE across arms. Accuracy SE in the stroke group did not differ from the control group for either the less-affected (P = .185) or the more-affected (P = .457) arms. Speed SE was lower in the stroke group compared with the control group for the more-affected arm (P = .01) but not the less-affected arm (P = .933).
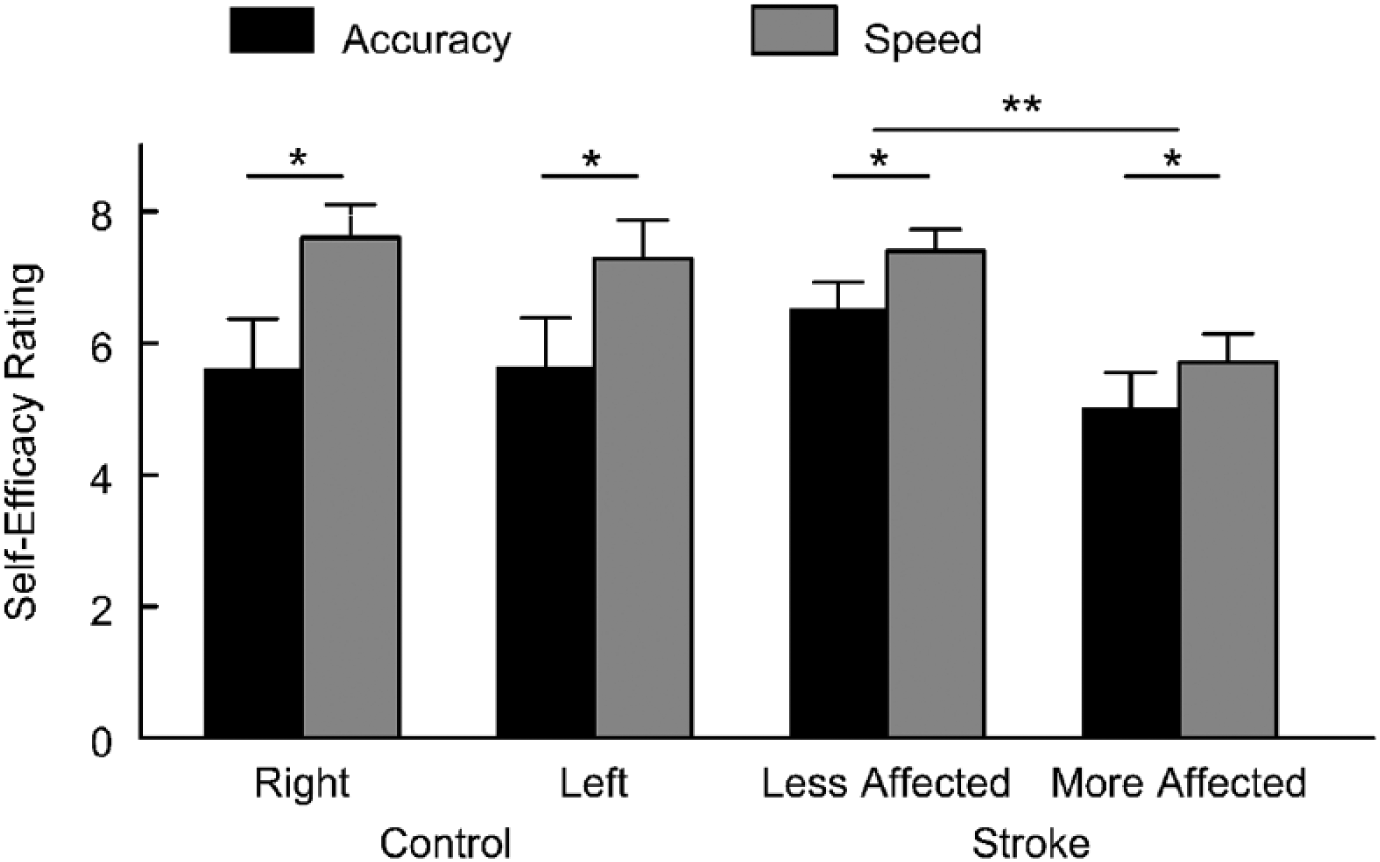
Mean self-efficacy by group and arm. Each bar represents group mean with standard error bar for accuracy self-efficacy and speed self-efficacy. *P <.05 for differences between accuracy and speed self-efficacy; **P <.05 for differences between arms.
Relationship Between SE and Kinematic Variables of Reach Performance
In the control group, accuracy SE showed a negative correlation with end point error that was statistically significant for reaches to contralateral targets (across midline); individuals with higher accuracy SE tended to have lower error (Table 3). Speed SE showed a positive correlation with peak velocity and a negative correlation with movement time; individuals with higher speed SE tended to have higher peak velocity and shorter movement time. Similar relationships between SE and reach performance were found for the less-affected arm in the stroke group (Table 3, Figure 3). For reaches with the more-affected arm, accuracy SE showed a negative relationship with end point error for contralateral targets. Speed SE did not significantly correlate with peak velocity or movement time, although there was a trend for a negative correlation between speed SE and movement time to ipsilateral targets (P = .038). Within the stroke group, neither accuracy SE nor speed SE correlated with UE FM, ARAT, SIS hand, or CAHM score (r < 0.250; P > .289).
Correlation between Self-efficacy and Reach Performance.
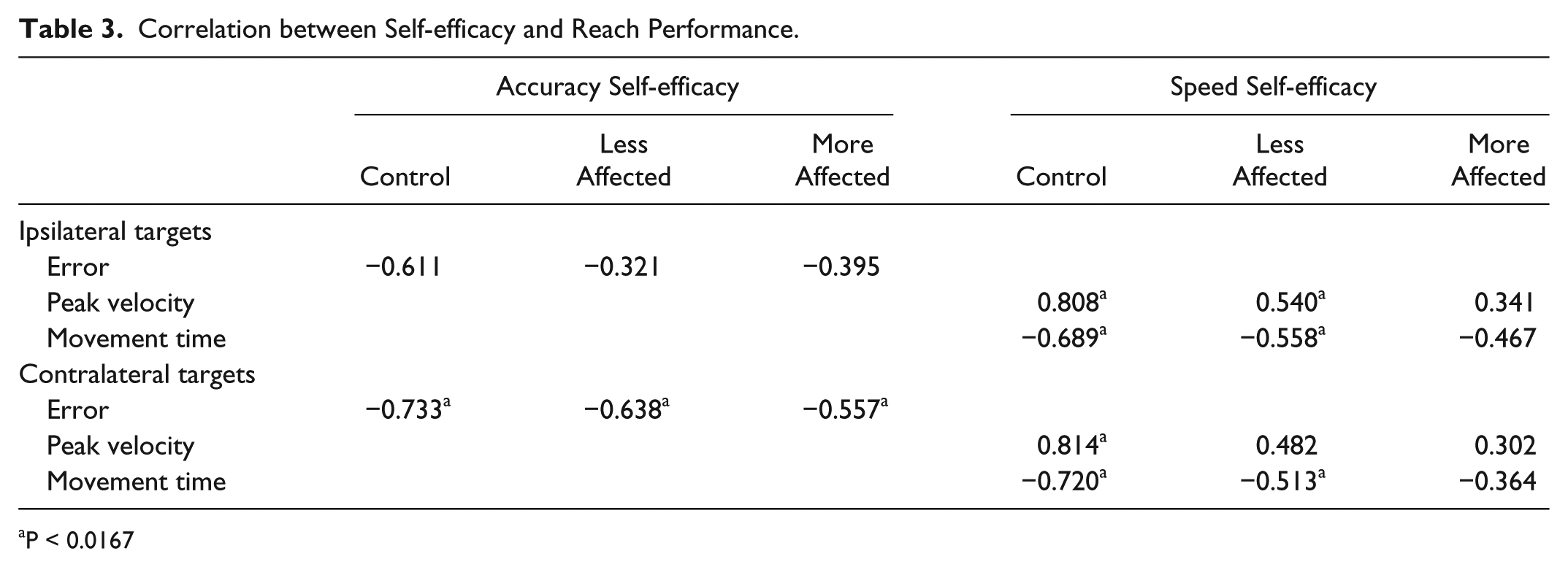
P < 0.0167
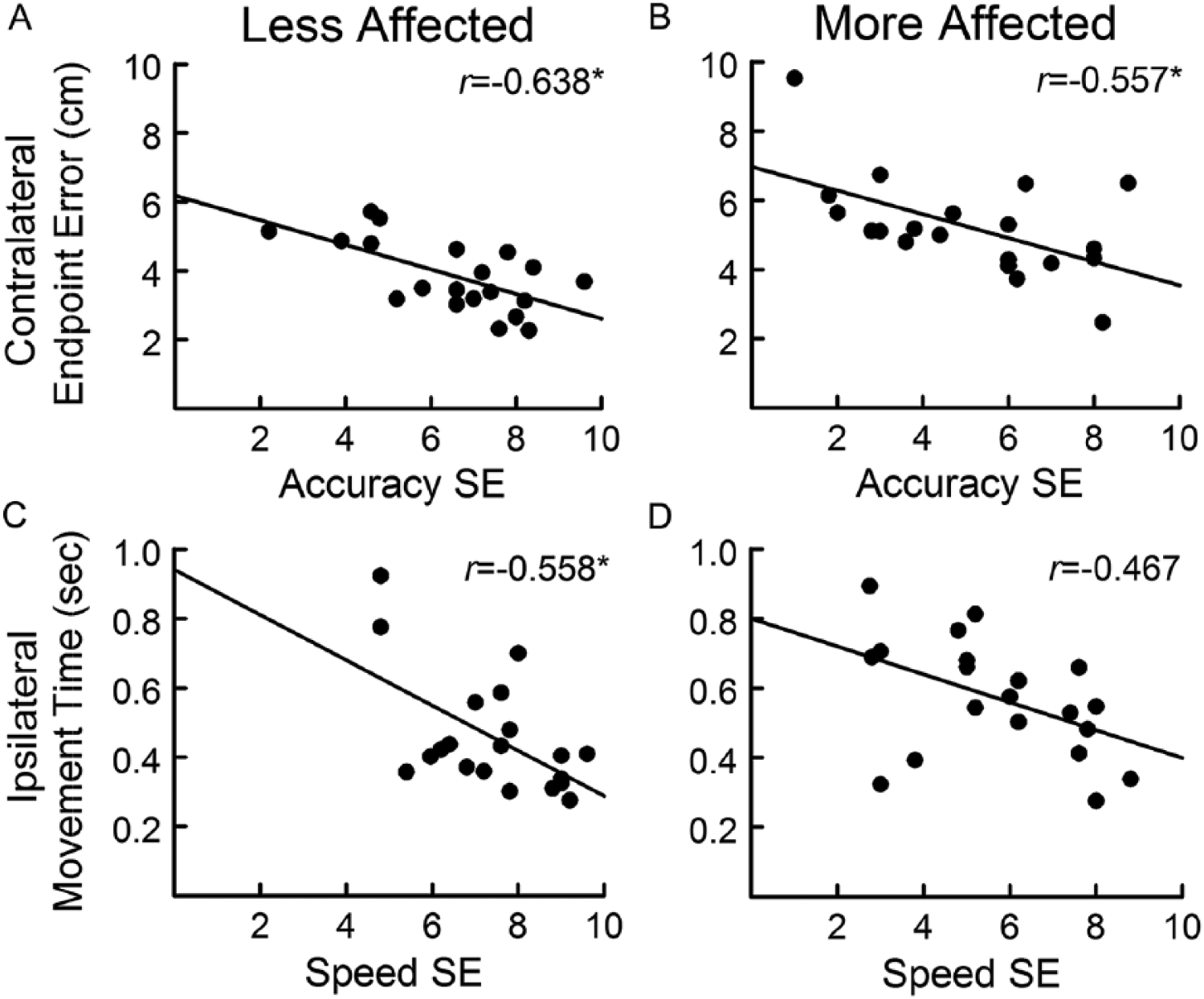
Relationship between self-efficacy and reach performance: the relationship between end point error to contralateral targets and accuracy self-efficacy shown for the less-affected (A) and more-affected (B) arms. The relationship between movement time to ipsilateral targets and speed self-efficacy shown for the less-affected (C) and more-affected (D) arms. *P < .0167 for correlation. Note that the r value in (C) was determined using the log of movement time; raw data are presented here for ease of interpretation.
Based on the results of the correlation analysis for the more-affected arm, the regression models focused on end point error to the contralateral targets and movement time to the ipsilateral targets as dependent variables. For end point error, only accuracy SE (r = −0.557; P = .011) and UE FM motor score (r = 0.459; P = .042) showed a significant bivariate correlation with error and were entered as possible predictors. In the first step, UE FM score was entered into the regression model and was a significant predictor of end point error (R2 = 0.167; F = 4.80; P = .042). In the second step, accuracy SE was added to the model and accounted for additional variance in end point error (R2 = 0.352;F = 6.15; P = .01). For movement time, speed SE (r = 0.467; P = .038) and age (r = 0.463; P = .04) were included as possible predictors. In the first step, age was a significant predictor of movement time (R2 = 0.170; F = 4.90; P = .04). In the second step, speed SE accounted for additional variance in movement time (R2 = 0.291; F = 1.89; P = .021).
Discussion
This study examined SE, a patient-reported measure, for skilled, goal-directed reach actions after stroke. Overall, SE for reach performance was lower for reaches with the more-affected arm compared with the less-affected arm; this decrease in SE corresponded to a decrease in actual reach performance with the more-affected arm, consistent with previous studies.35-37 SE for reach accuracy and reach speed appeared distinct, with accuracy SE reported as being lower than speed SE in both the more-affected and less-affected arms as well as in controls. Additionally, reach SE significantly correlated with actual reach performance in the more-affected arm, suggesting that individuals with mild motor impairment caused by stroke have insight into their ability to perform a skilled reach task.
There have been limited studies that have investigated the relationship between SE and reach performance after stroke (see Rowe et al 38 for an exception). SE related to measures of reach performance for the more-affected arm and remained a predictor of performance even when other clinical and demographic variables were considered. There is a growing body of evidence that supports a significant role for SE in several domains of function after stroke, including fall risk,14,15 physical function,16,17 gait function, 18 and walking activity.19,20 The consistency of these results across studies and task domains suggest that patient-reported confidence may be an important factor in motor skill performance and function after stroke. SE for UE function has received limited attention in the literature to date. An understanding of an individual’s confidence to successfully perform goal-directed UE tasks may provide insight into the reported disconnect between arm movement capacity and arm use after stroke.3,4 Decreased SE to successfully complete a functional task using the more-affected arm may lead an individual to choose a different strategy, such as using the less-affected arm instead. 39 SE is a quick, inexpensive, patient-reported outcome measure that can easily be performed in both the research laboratory and the clinic. Future studies seeking to understand the predictors of skilled arm function should consider including a measure of SE.
SE combined with age to predict reach speed to ipsilateral targets, whereas SE combined with UE FM motor score to predict reach accuracy to contralateral targets. Decreases in movement speed during goal-directed reaching have frequently been associated with increases in age.40-42 In general, increased age shows a positive correlation with movement time to complete a reach task. Because many individuals poststroke are often older, the finding that age also relates to reach speed is consistent with this previous work. In contrast, UE FM motor score correlated with reach accuracy. The UE FM is a measure of motor impairment that asks individuals to move in specific movement patterns in and out of synergy. 26 The motor score reflects how well an individual can perform each pattern, and there is no time constraint for most items. This finding suggests that the UE FM provides information about the ability of individuals with mild stroke-related motor impairment to control arm movements in a manner that supports accurate completion of a reach task.
For both end point error and movement time, the relationship between SE and reach performance was direction specific. Speed SE correlated with movement time for reaches to ipsilateral targets, whereas accuracy SE correlated with end point error for reaches to contralateral targets. Reach direction had an effect on measures of reach performance for the more-affected arm (shorter movement time to ipsilateral targets, higher end point error to contralateral targets), consistent with previous reports in nondisabled individuals.32,33 Previous research has suggested an effect of target direction on reach SE after stroke. 43 Chen et al 43 found that confidence was lower for targets in the contralateral workspace that required a reach across midline than for targets in the ipsilateral workspace. However, in that study, SE was not separated into speed and accuracy, and the relationship between measures of reach SE and reach performance was not examined. Our findings suggest that accuracy SE and speed SE may also be affected by reach direction, although this was not directly examined in the current study (ie, SE was not reported separately by target direction). Future studies could investigate the interaction of SE type and reach direction in individuals with and without stroke.
Overall, in both groups, participants felt more confident with respect to reach speed than they did for reach accuracy for reaches with both arms. This difference in SE may have been driven by the demands of the task. Participants were encouraged to move quickly, but no time constraints on movement time were present, whereas visual feedback related to accuracy was presented after each trial. This feedback may have increased participants’ focus on accuracy, which may have affected the SE rating. Alternatively, given that the task did not impose any constraints on speed or accuracy, each participant may have selected a reach strategy that optimized both variables for task completion44,45; the self-selected strategy may have affected SE ratings. Although the current study cannot determine why speed SE was rated higher than accuracy SE, the findings suggest that these variables can be rated distinctly by participants with and without stroke. Future studies could examine the effect of task manipulations on speed or accuracy on reach SE.
In general, self-reported measures of SE are thought to be specific to the task or domain reflected in the question posed.10,12 This may explain the finding that measures of reach SE correlated with measures of reach performance but not with clinical measures of motor impairment or function. One might expect reach SE to correlate with a general measure of SE for UE functional activities (CAHM); however, this was not the case. The CAHM asks the individual to rate his or her confidence in performing a variety of unimanual and bimanual functional tasks, many of which require some degree of hand function in addition to transport of the arm. Reach SE in the current study related to one’s ability to transport the arm accurately and quickly to targets in a horizontal plane, and no hand function was required. The lack of relationship between the CAHM and reach SE may suggest that each measure focuses on a specific task domain, functional tasks, and reach control, respectively.
Interventions that seek to improve proximal arm control after stroke should consider the role of SE for reach control found in the current study. SE is thought to play an important role in other domains of health, 13 including disease self-management46-49 and physical activity.50,51 Strategies that aim to improve SE may be particularly important for translation of motor rehabilitation interventions targeting proximal arm function and ultimately arm use in the natural environment after stroke. Such strategies may include a combination of physical practice, social support, and techniques to enhance intrinsic motivation, including goal setting.11,52-54 In fact, recent work has shown that confidence to perform UE functional tasks can change in response to training designed to target both skill performance and confidence.54,55 Future work could examine whether SE for reach control changes with repetitive practice or whether interventions that target improvements in SE benefit arm control, arm use, and overall function.
The frequency and type of verbal feedback provided to participants during reach trials was not controlled or logged in the current study. Comments were general in nature and aimed to maintain participant engagement in the reach task. Instructions and feedback can affect levels of SE.10,12,52 However, we did not see a significant change in SE across the data collection session (no change over blocks), suggesting that the verbal feedback provided had a limited effect on SE in the current study. Future work could examine the effect of instruction, and feedback content and frequency on SE during the performance of a reach task or other skilled UE tasks after stroke.
This study only included individuals with chronic stroke who had mild motor impairment but continued deficits in arm function and confidence. The relationship between SE and reach control in individuals with more severe motor impairment or who are in the acute/subacute period of recovery may be different. The current study was designed to assess confidence during reach performance but not during learning. Neither reach SE nor reach performance changed over blocks in a single session of practice. Future studies could investigate how SE changes over time or in response to a period of motor training and how these changes correspond to changes in reach performance. In the current analysis, reach performance was summarized across target distances, similar to our previous analysis. 23 Although target distance may affect the level of SE after stroke, 43 our study design did not allow us to examine the effect of distance on speed SE or accuracy SE. The findings in the current study support continued investigation into the role of SE in reach control after stroke, including the influence of variables such as target distance. The task used in the current study did not require individuals to grasp or manipulate an object. SE may be different for tasks that require reaching for the purpose of engaging the hand in a manipulation task.
Conclusions
SE for skilled reaching with the more-affected arm was decreased in this group of individuals with mild motor impairment due to stroke. SE for reach speed and reach accuracy appeared distinct and correlated with kinematic measures of reach performance with the more-affected arm; individuals with higher SE tended to reach faster and with less error. SE should be considered as a predictor of reach control in studies seeking to understand reach deficits and may be a target, 13 in combination with performance, of interventions aimed at improving proximal arm control after stroke.
Supplemental Material
Supplemental_Figures_Final – Supplemental material for Self-efficacy and Reach Performance in Individuals With Mild Motor Impairment Due to Stroke
Supplemental material, Supplemental_Figures_Final for Self-efficacy and Reach Performance in Individuals With Mild Motor Impairment Due to Stroke by Jill Campbell Stewart, Rebecca Lewthwaite, Janelle Rocktashel and Carolee J. Winstein in Neurorehabilitation and Neural Repair
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided in part through a Mary McMillan Doctoral Scholarship and a Promotion of Doctoral Studies II Scholarship from the Foundation for Physical Therapy, a grant from the California Physical Therapy Fund, and NIH T32GM081740. The virtual reality system used in this study was provided by Innovative Sports Training, Inc.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.