
Abstract
Introduction. Cognitive impairment after stroke has been associated with lower quality of life and independence in the long run, stressing the need for methods that target impairment for cognitive rehabilitation. The use of noninvasive brain stimulation (NIBS) on recovery of language functions is well documented, yet the effects of NIBS on other cognitive domains remain largely unknown. Therefore, we conducted a systematic review that evaluates the effects of different stimulation techniques on domain-specific (long-term) cognitive recovery after stroke. Methods. Three databases (PubMed, EMBASE, and PsycINFO) were searched for articles (in English) on the effects of NIBS on cognitive domains, published up to January 2018. Results. A total of 40 articles were included: randomized controlled trials (n = 21), studies with a crossover design (n = 9), case studies (n = 6), and studies with a mixed design (n = 4). Most studies tested effects on neglect (n = 25). The majority of the studies revealed treatment effects on at least 1 time point poststroke, in at least 1 cognitive domain. Studies varied highly on the factors time poststroke, number of treatment sessions, and stimulation protocols. Outcome measures were generally limited to a few cognitive tests. Conclusion. Our review suggests that NIBS is able to alleviate neglect after stroke. However, the results are still inconclusive and preliminary for the effect of NIBS on other cognitive domains. A standardized core set of outcome measures of cognition, also at the level of daily life activities and participation, and international agreement on treatment protocols, could lead to better evaluation of the efficacy of NIBS and comparisons between studies.
Keywords
Introduction
Estimations are that 70% to 90% of stroke patients have some degree of cognitive impairment.1,2 Up to 50% of stroke patients have impairments in multiple cognitive domains. 2 The cognitive deficits remain highly prevalent in the long term (>12 months poststroke), both in younger 3 and older stroke patients. 4 Furthermore, as cognitive abilities are related to functional performance,5-8 cognitive impairments can lead to problems in performance in activities of daily living (ADLs) and participation.9-11 Taking these notions into account, it is not surprising that improvement of cognition after stroke has been characterized as a main research priority by stroke survivors, care givers, and health professionals. 12
Noninvasive brain stimulation (NIBS) techniques, such as repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS)*, are deemed promising tools to enhance poststroke recovery because they have the potential to increase or decrease cortical excitability with long-lasting effects. 13 The use of NIBS for motor14-16 and language17-20 recovery is well documented and provides evidence for the potential efficacy of NIBS in rehabilitation, simultaneously pointing out the need for refinement of stimulation protocols to guarantee efficacy and reliability. However, much less is known about NIBS in relation to poststroke recovery of cognitive impairments outside the domain of language and which methodological variables are related to treatment effects.
Therefore, we conducted a systematic review that evaluates and compares the effects of 2 NIBS techniques—namely, TMS (rTMS and TBS [Theta Burst Stimulation]) and tDCS—on poststroke domain-specific (long-term) cognitive recovery. The selected cognitive domains included visuospatial neglect, memory, executive function, global cognitive function, and other cognitive domains (working memory and attention) but not language. We qualitatively evaluated the included studies with the PEDRO Scale and a composed checklist.
Methods
Literature Search
PubMed, EMBASE, and PsycINFO were searched for articles in English, published up to January 2018, with the following criteria in the title and/or abstract: inclusion of patients with ischemic or hemorrhagic stroke, NIBS as therapeutic intervention, existence of a control condition, and outcome measurements that assessed cognitive function. The exact keywords that were used are listed in Supplement 2.
Selection of Studies
Three researchers separately reviewed the titles and abstracts of the retrieved articles to determine the presence of the abovementioned criteria. Full articles were reviewed for eligibility based on predetermined inclusion and exclusion criteria. Inclusion criteria were as follows: (1) patients with ischemic or hemorrhagic stroke; (2) age ≥ 18 years; (3) the use of NIBS (TMS, TBS, or tDCS); (4) objective, standardized tests or test batteries for assessment of cognitive function; and (5) baseline measurement and posttreatment measurement(s). Exclusion criteria were (1) nonhuman studies and (2) studies that only tested effects on motor, language functions and perception.
Qualitative Evaluation of Studies
For randomized controlled trials (RCTs), the PEDro scale (Physiotherapy Evidence Database) 21 was used. Points were only awarded if the article specifically mentioned the criterion of an item, with the highest possible score of 10. For studies without a control group, we composed a checklist containing relevant items of the following questionnaires: the PEDro scale, the Critical Appraisal of a Case Study questionnaire of the Center for Evidence-Based Management, 22 the Joanna Briggs Institute (JBI) Critical Appraisal-Checklist for Case Reports, 23 and finally, the JBI Critical Appraisal-Checklist for Case Series. 23 The specific items of the composed scale can be found in Supplement 3.
All studies were scored by 3 independent raters (RH, MG, and EL) and the interrater reliability was calculated (Cohen’s κ, ±SD). Studies with incompatible scores were discussed until consensus was reached. The final scores of each study are presented in Supplement 4.
Data Evaluation
Data regarding sample size, age, gender, time poststroke, stroke type, and the affected hemisphere were collected. Means and SDs were calculated if possible. For effect size of post hoc t-tests, Cohen’s d and r were extracted or calculated.
Detailed information was extracted regarding the NIBS methods, including stimulation frequency or intensity, active/resting motor threshold (for rTMS studies), target area and hemisphere, stroke location, number of sessions, session duration, testing period, and the type of control condition.
To evaluate cognitive function, the following variables were summarized per study: studied cognitive domain, outcome measures (levels of cognitive function, ADL, and/or participation), time points of testing (directly after treatment [T1], 1 to 2 weeks posttreatment [T2] and >4 weeks posttreatment [T3]), and the presence of a treatment effect. A treatment effect was defined as a significant difference between the experimental condition(s) and at least 1 control condition, for at least 1 outcome measure, at any time point posttreatment. The cognitive outcome measures were categorized under the following domains: neglect, memory, executive function, global cognitive function, and other cognitive domains (working memory and attention). Notwithstanding the framing of the go/no-go task as a test of attention by some authors, we preferred to categorize it as a test of executive functions—executive attention, to be more precise. 24 Semantic fluency tests were also categorized as tests of executive functions.
If there was ≥1 study for a NIBS technique (TMS/TBS/tDCS), separate headings are used in the Results section to distinguish between the different applied techniques for each cognitive domain. Furthermore, a brief summary statement is added for each cognitive domain for which multiple NIBS techniques have been applied.
Results
A total of 156 articles were assessed for eligibility. Authors were contacted if an article was not accessible. Of the 156 assessed articles, 40 were selected for review. There was a high consensus among the 2 raters, which resulted in an interrater reliability of κ =0.97 (Cohen’s κ). A flowchart of the selection process is depicted in Figure 1.
Flowchart of the selection process.
The total sample of 40 articles included RCTs (n = 21), studies with a crossover design (n = 9), case studies (n = 6), and studies with a mixed design (n = 4). Table 1 summarizes the study characteristics of the included studies.
Study Characteristics.
Abbreviations: ADL, activities of daily living; BCT, Bird Cancellation Task; BIT, Behavioral Inattention Test; CBS, Catherine Bergego Scale; CNT, Computerized Neuropsychological Test; CoF, Copy of Figure; CPT, Continuous Performance Test; cTBS, continuous TBS; dlPFC, dorsolateral prefrontal cortex; F, female; H, hemorrhagic; I, ischemic; iTBS, intermittent TBS; LBT, Line Bisection Test; LCT, Letter Cancellation Test; LOTCA, Loewenstein Occupational Therapy Cognitive Assessment; M, male; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; MRT, Munich Reading Texts; MVPT, Motorfree Visual Perception Test; RBMT, Rivermead Behavioural Memory Test; RCT, randomized controlled trial; RSCT, Random Shape Cancellation Test; rTMS, repetitive transcranial magnetic stimulation; SCT, Star Cancellation Test; TAP, Test for Attention Performance; tDCS, transcranial direct current stimulation; TMT, Trail Making Task; TPPT, Two Part Picture Test. aCase study, only absolute improvement described; bexperimental group, control group not specified; cstudy with n=5 experimental group, n=5 control group, and n=3 that completed both conditions and were pooled for analysis (total n=13); dstandard error of measurement is used instead of SD.
Effect sizes and P values of the rTMS studies, separated for test, condition, and timepoint. The case study of Shindo et al 53 is not included.
Effect sizes and P values of the TBS studies, separated for test, condition, and timepoint. The case study of Vuksanović et al 53 is not included.
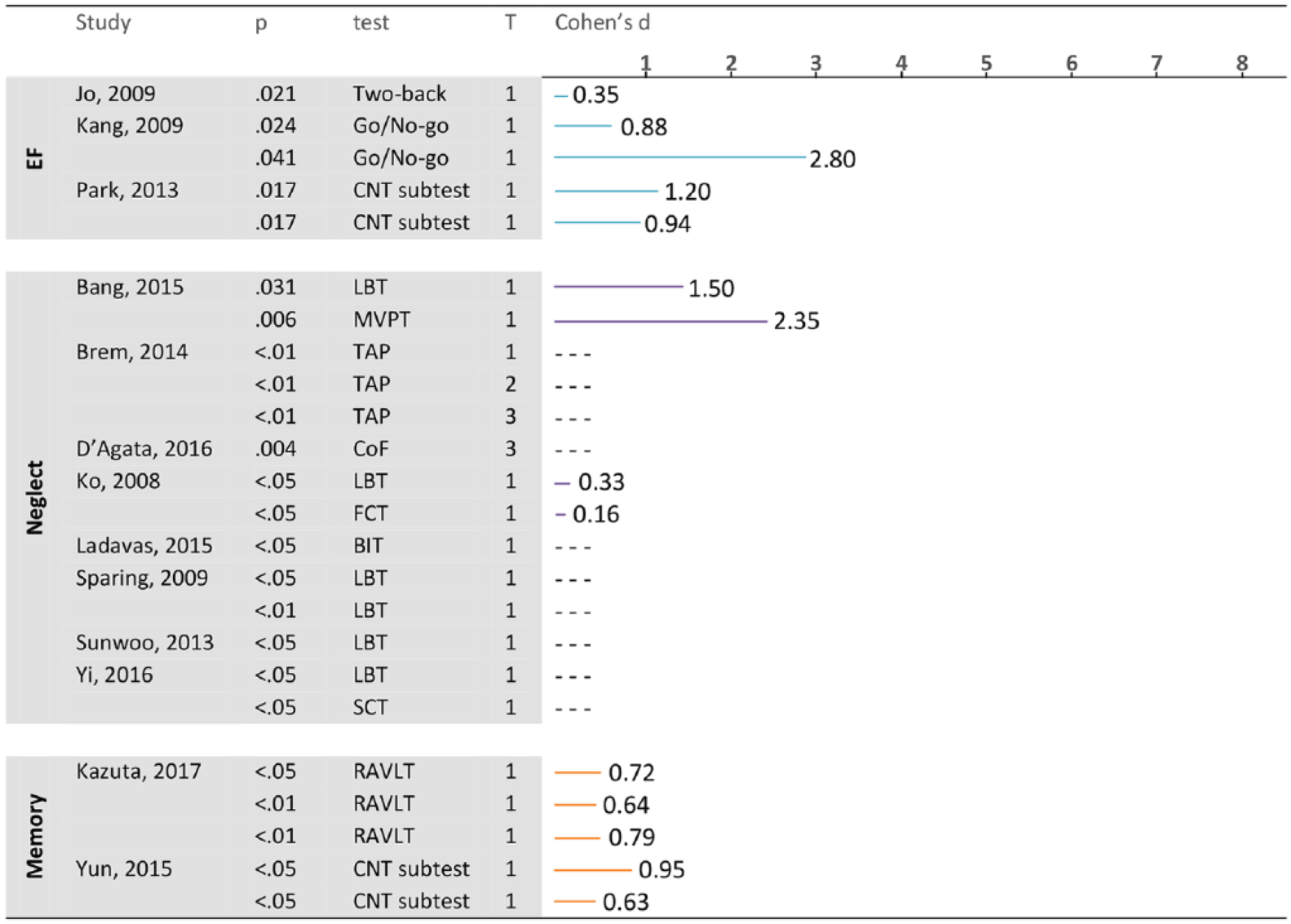
Effect sizes and P values of the tDCS studies, separated for test, condition, and timepoint. Results of subtests that are part of a global cognitive test battery are placed under the corresponding cognitive domain. The case study of Leo et al 55 is not included.
Study Characteristics
The included studies were published between 2001 and 2017, with 75% of the articles from the past 8 years. Among the studies, 92% were carried out in Asia and Europe and the remaining 8% in the United States and Africa (Egypt). The mean participant sample size for RCTs was 26.6 (SD = 12.7; range = 11-60), 10.1 (SD = 2.8; range = 5-20) for studies with a crossover design, and 13.3 (SD = 6.2; range = 34-38) for studies with a mixed design. The sample sizes for the case studies ranged from 1 to 8. The mean age of participants was 59.7 ± 8.3 years (n = 40; not specified in 2 studies25,26). The time post–stroke onset varied considerably between studies, and different time units were used (ie, days, weeks, months, years). The time poststroke ranged from 14 days (subacute) to 5 years (chronic) poststroke.
One or 2 relatively short neuropsychological tests were often used to assess a cognitive domain. Of the included studies, 7 used an outcome measure of ADL/participation in addition to the outcome measure(s) for the tested cognitive domain.
Treatment Characteristics
Inhibitory low-frequency rTMS of ≤1 Hz over the unaffected hemisphere was the most frequently used stimulation protocol (n = 13). Most studies applied rTMS at 80% to 100% resting motor threshold (n = 15). For studies that used multiple sessions (n = 13), the number of sessions varied between 5 and 28 (12.6 [SD = 6.7] sessions), the total testing period ranged from 5 to 28 days (mean 16.8 ± 6.9 days) posttreatment. The remaining 5 studies tested the effect of TMS in a single session only. Overall, the mean session duration was 15.4 ± 5.4 minutes (n = 15).
For studies that used TBS as a stimulation technique (n = 10), 7 studies used continuous TBS (cTBS) over the unaffected hemisphere, 2 studies used intermittent TBS (iTBS; one over the affected hemisphere and the other over the unaffected hemisphere), and 1 study applied dual TBS protocol with simultaneous cTBS over 1 hemisphere and iTBS over the unaffected and affected hemispheres, respectively. The TBS studies had a mean of 13.5 ± 10.3 stimulation sessions, within a total testing period of 7.4 ± 6.1 days. The mean session duration was 1.5 ± 1.3 minutes.
For studies that used tDCS as a stimulation technique (n = 16), tDCS was directed between an anode applied over the lesioned hemisphere and a cathode over the contralesional homologue area, in at least 1 condition in 8 studies. A total of 10 studies positioned an electrode in a neutral reference area in at least 1 condition (n = 10, see Table 1 for reference sites). In 3 studies, the reference location was not specified. For studies that tested the effect of multiple sessions over time (n = 9), the mean number of sessions was 14.2 ± 9.9, within a total testing period of 19.7 ± 14.0 days; 7 studies tested the effect of a single session only. The mean session duration was 22.4 ± 6.6 minutes.
Different additional therapies were given next to tDCS or rTMS—for example, conventional rehabilitation, physical therapy, (computer-assisted) cognitive rehabilitation, visual scanning therapy, smooth pursuit training, prism adaptation, speech and language therapy, cognitive neglect therapy, and mirror therapy.
Qualitative Evaluation of Studies
Cohen’s κ for interrater reliability was 0.624 (0.101) for PEDro ratings and 0.678 (0.144) for crossover/case study ratings, which is considered a substantial agreement. 33 Scores per study can be found in Supplement 4. As shown in Supplement 4, most studies were evaluated as high or very high quality (87.5% for RCTs, 88.2% for crossover/case studies).
The Effect of NIBS on Different Cognitive Domains
A total of 25 studies included patients with neglect or contralesional extinction. In 20 of these studies, patients with right-sided stroke were treated (3 studies did not report stroke side34-36), but the side of the neglect was not always reported. Two studies included patients with both right and left hemisphere damage and resulting contralateral neglect.37,38 Figures 2 to 4 shows an overview of the effect sizes of the various studies on the different cognitive domains.
TMS Studies
Of the 10 studies that tested the effect of TMS on neglect symptoms, 8 reported a significant treatment effect through inhibition of the contralesional parietal cortex. This protocol did not result in a treatment effect in the RCT of Lim et al. 39 In another RCT by D’Agata et al, 38 1Hz rTMS to the contralesional primary motor cortex (M1) did not alleviate neglect. The latter RCT included 34 patients and evaluated multiple cognitive domains. The studies indicating positive effects and with low risk of bias (n = 8) had different designs: RCTs, case studies, and 1 crossover study, with stroke populations ranging from 2 to 38 patients (effect sizes ranging from 0.74 to 5.27).
Kim et al 40 investigated in a RCT (low risk of bias) whether 10 sessions of rTMS would cause improved recovery from neglect compared with a single session in 34 patients with chronic right-sided stroke. Ten sessions of 1-Hz rTMS over the contralesional posterior parietal cortex (PPC) resulted in a greater improvement of performance on the line bisection and letter cancellation task, versus 1 session only. This is the only identified study that tested the effect of multiple stimulation sessions on cognitive functions, including neglect.
The inhibitory stimulation protocol can induce long-lasting effects; all studies that measured outcome at T2 or T3 (n = 5) reported a maintained treatment effect at these time points.
TBS Studies
Of the included 8 studies, 7 specifically tested the effect of cTBS over the contralesional left PPC, whereas in the study by Cao et al 41 (high risk of bias) the effect of iTBS over the contralesional dorsolateral prefrontal cortex (dlPFC) was tested (see Table 1). All studies, designed as RCTs or crossover, reported a significant treatment effect (effect sizes ranging from 1.48 to 6.57, or not reported). The evaluated study designs had a low risk of bias and had 11 to 38 patients included. Yang et al 35 compared cTBS, 1-Hz rTMS, and 10-Hz rTMS and found that cTBS caused the greatest improvements of neglect (line bisection task and star cancellation task), suggesting that TBS may be the superior method for alleviating neglect symptoms.
Koch et al 26 found that the effect of TBS had lasted until T2, whereas Cazzoli et al 42 reported that the effect had disappeared at T2. Similar to low-frequency rTMS, a cTBS protocol can carry effects for at least 4 weeks posttreatment (T3). 43
tDCS Studies
Of 8 studies, 7 found a significant treatment effect for at least 1 test (reported effect sizes 0.18-2.81). The studies formed a heterogeneous group of RCTs, crossover studies, and a single case study. Sample sizes differed from 10 to 30 patients, and the studies were rated as high-quality designs, except for 1 study of fair quality. Additionally, effects have been found with varying session numbers, observed in subacute and chronic patients. In all studies, the parietal cortex was the target location; that is, anodal stimulation of the lesioned area (unilateral montage 44 ) and cathodal stimulation of the contralesional homologue (bilateral montage36,45-47) or separate conditions with contralesional left parietal cathodal or lesioned right parietal anodal stimulation.48-50 Sunwoo et al 47 combined unilateral (lesional anodal stimulation) and bilateral montage (as described above). Smit et al, 46 who performed a high-quality crossover study with 5 patients, did not find any effect of tDCS on neglect severity. Brem et al 45 additionally evaluated the effect at T2 and T3 and found that the effect remained significant.
In summary, the majority of the studies reported significant treatment effects, including long-lasting effects. All studies targeted the contralesional PPC, except for 1 study that used an excitatory protocol in that region. 41 The studies had mixed designs and had a low risk of bias.
The Effect of NIBS on Memory Function
TMS Studies
Two studies reported a significant effect of inhibitory rTMS and tDCS on memory performance (effect sizes 1.03-1.57). Lu et al, 51 who conducted a RCT of high quality with 40 patients, tested a stimulation protocol of 1-Hz rTMS over the right dlPFC, irrespective of lesion location. The effects on everyday memory function (visual, verbal, recall, recognition, and immediate and delayed everyday memory) were significantly higher in the rTMS group compared with the sham group at 1 week and 2 months posttreatment. D’Agata et al 38 conducted a RCT of high quality with 34 patients, in which 1-Hz rTMS was applied over the contralesional M1 (after a wash-out period of 6 months tDCS, cathode onto the contralesional M1) in patients who underwent upper-limb rehabilitation after stroke. After the assessment of multiple neuropsychological tests, significant improvement was found for visuospatial recall memory (Copy of Figure test).
Another RCT of high quality (n = 18) tested the effect of rTMS (1 and 10 Hz) over the left dlPFC, compared with sham stimulation, on several neuropsychological tests, including a verbal learning test. 52 Patients with right-sided and left-sided strokes were included. After 10 daily sessions of rTMS, no significant treatment effect was found for any of the neuropsychological tests.
TBS Studies
The single case study by Vuksanović et al 53 (low risk of bias) investigated the potential of TBS to (primarily) improve language functions in a nonfluent aphasia patient. After bilateral TBS over Broca’s area and the contralesional homologue (cTBS contralesional, iTBS ipsilesional), apart from language improvements, short-term verbal memory and verbal learning improved, as reflected by scores on immediate and delayed recall conditions on the Rey Auditory Verbal Learning Test (improved by 100% compared to baseline). 53
tDCS Studies
A crossover study by Kazuta et al 54 with a low risk of bias included 12 patients with auditory verbal memory deficits (3-12 months poststroke). Irrespective of lesion location, the left temporoparietal area was stimulated with anodal tDCS and resulted in an increase in the number of correctly remembered words in the fifth and first to fifth trials (5 trials to recall a list of 15 heard words). Additionally, a primacy effect (first 5 words) was found for the tDCS condition but not the sham condition (effect sizes 0.64-0.79).
Leo et al 55 performed a single case study testing the effect of 40 sessions of cathodal stimulation over T8 (contralesional superior temporal gyrus) on several neuropsychological tests, including verbal learning and verbal memory, but did not find an effect on memory function. This study had a high risk of bias because several points were missing: for example, no clear inclusion criteria, no clearly described methods and results, and no take-away lessons for practice. D’Agata et al 38 tested several cognitive domains in patients who underwent upper-limb rehabilitation after stroke, yet reported no effects for memory.
Overall, various factors differed between the abovementioned studies: that is, stimulated region(s) (M1, right or left dlPFC, Broca’s area, temporoparietal area, superior temporal gyrus), stimulated hemisphere (contralesional hemisphere, ipsilesional hemisphere, both or irrespective of lesion location), and study designs (RCTs, crossover studies, and single case studies). Significant treatment effects were found in some studies (n = 4) and not in others (n = 3).
The Effect of NIBS on Executive Function
TBS Studies
Szaflarski et al 56 applied iTBS over the lesioned Broca’s area in 8 chronic patients (case reports). After 10 sessions, a treatment effect was found for iTBS on semantic fluency. 56 Vuksanović et al 53 reported on a single case of a chronic aphasia patient, in which iTBS stimulation was applied over the lesioned Broca’s area and cTBS stimulation over the contralateral homologue area, and found increased performance on the semantic verbal fluency task, especially at T2. 53 Both studies had a low risk of bias.
tDCS Studies
Leo et al 55 tested the effect of cathodal tDCS over contralesional T8 (superior temporal gyrus) and found no effects on verbal fluency after 40 sessions. 55 Kang et al 24 evaluated performance on sustained attention (go/no-go task) in a crossover study design (n = 20) after 1 session of anodal tDCS over the left dlPFC, irrespective of stroke location. Compared with healthy controls, significant improvements were found after tDCS at 1 hour (d = 0.88) and 3 hours posttreatment (d = 2.80).
In summary, we identified 2 studies that applied TBS over Broca’s area, reporting a significant treatment effect. A study in which tDCS was applied in 40 sessions found no treatment effect, whereas a single-session tDCS study reported positive treatment effects.
The Effect of NIBS on Global Cognitive Function (Cognitive Screening)
TMS Studies
Five studies screened global cognitive function; 1 single case study found a significant treatment effect (effect sizes 1.03-1.57). 51 This study by Lu et al 51 tested the effect of 20 daily sessions of rTMS in combination with cognitive training on scores of short (Montreal Cognitive Assessment) and more elaborate (Loewenstein Occupational Therapy Cognitive Assessment) cognitive screening. 1-Hz rTMS was applied over the right dlPFC, irrespective of stroke location, and compared with sham sessions. Three RCTs with low risk of bias (sample sizes 15-60) without rTMS effects on cognitive screening scores, all targeted the unaffected (1 Hz) and affected (5 Hz) primary motor cortex.38,57,58 A case series (n = 2) by Shindo et al 59 tested global cognition (Mini-Mental State Examination [MMSE]) and did not find a treatment effect, probably because it lacked statistical power to draw any conclusions regarding this domain.
tDCS Studies
Two RCTs with a low risk of bias found no treatment effects on K-MMSE (Korean MMSE) scores.60,61 However, both studies also applied a larger, more elaborate test battery in which an effect of anodal tDCS of the bilateral prefrontal cortex was found (d = 1.20) on sustained attention in the study by Park et al, 61 whereas the study by Yun et al 60 reported auditory verbal memory improvements (d = 0.63/0.95) after left anterior temporal lobe stimulation with anodal tDCS, irrespective of lesion location. Taken together, a significant treatment effect was found in 1 of 7 studies. However, this result should be interpreted with caution because it involved a single case study.
The Effect of NIBS on Other Cognitive Domains
Working Memory
Jo et al 62 conducted a crossover study and tested the effect of anodal tDCS of the contralesional dlPFC on working memory (capacity) in 10 subacute stroke patients (2-back task). Task accuracy increased significantly after a single session of tDCS, reflecting a small to medium effect (d = 0.35). Kim et al 52 used HF rTMS to stimulate the lesioned M1 and LF rTMS to stimulate the contralesional M1 in 18 patients and found no effects on working memory (capacity). Two other RCTs with a low risk of bias tested working memory after stimulation of the primary motor cortex and did not find an effect.38,58 Both studies applied inhibitory contralesional TMS, and one of them also applied contralesional cathodal tDCS after a wash-out period of 6 months. 38
Attention
Leo et al 55 performed a single case study, with a high risk of bias, and tested the effect of 40 sessions of cathodal tDCS over contralesional T8 (superior temporal gyrus) on attention performance, measured with attentional matrices and the Trail Making Task, and found significant improvements on those tests.
Discussion
The aim of this review was 2-fold; first, to provide an overview of studies assessing the effects of NIBS on cognitive function in stroke patients and, second, to present results on (long-term) improvement after stroke with respect to cognitive function. The majority of NIBS studies (n = 37) showed treatment effects on at least 1 time point and in at least 1 cognitive domain. All 6 studies that included a long-term follow-up assessment (T3; >4 weeks after treatment) reported long-lasting results, up to 12 weeks after treatment. Notwithstanding these positive results, there is a significant lack of consensus on the effectiveness of intervention protocols for the different cognitive domains and timing of intervention after stroke.
Main Findings
Most NIBS treatment studies focused on improvement of neglect. Overall, different NIBS techniques alleviated neglect (see systematic reviews63-65). The PPC was often chosen as the target site because of its association with spatial perception and visuospatial neglect. 66 In direct comparison against 1-Hz and 10-Hz rTMS, cTBS resulted in the largest therapeutic effect. 35 Despite these overall encouraging findings, these effects have to be interpreted with caution because of the small sample size and short follow-up periods, which may be a potential for bias in the results.
The number of studies focusing on other cognitive domains was much smaller than in the neglect domain, and the results were mainly inconclusive because of heterogeneity in intervention characteristics (eg, stimulation protocols, number of treatment sessions), participant characteristics (eg, time poststroke), and/or study design (eg, RCT, crossover, type of outcome measures). This makes it difficult to identify methodological predictors of treatment effects per specific cognitive domain or across domains.
Long-Lasting Cognitive Improvement
Long-lasting cognitive improvements after NIBS treatment were found for the following cognitive domains: neglect, global cognition, working memory, attention, and memory.35,38,43,45,51,59 The long-term cognitive improvements are likely related to the number of stimulation sessions/days, where more stimulation sessions result in longer-lasting stimulation effects. 67 To develop a full picture of the duration of NIBS effects, further work is required to get an understanding of the responsible (neurophysiological) mechanisms behind the NIBS pattern (eg, repeated trains of rTMS, a cumulative effect after a long conditioning phase, and periodic sessions).68,69
Proper Assessment of Cognitive Impairment
One important observation was that the majority of studies only included 1 or 2 relatively short neuropsychological tests to evaluate a specific cognitive domain and the effect of NIBS. There is consensus that multiple tests that cover several modalities (eg, verbal/nonverbal, visual/auditory), time windows (eg, short-term, long-term memory), and frames of reference (eg, allocentric/egocentric) are essential for proper neuropsychological assessment and clinical evaluation of the presence and severity of cognitive disorders. 70 Lack of multiple outcome measures might have led to underdiagnoses of cognitive impairment, as a result of which NIBS treatment effects cannot be adequately demonstrated. Furthermore, it makes comparison between studies targeting the same cognitive function more difficult. In addition, almost all studies used only pen-and-paper neuropsychological tests, which are notoriously insensitive at picking up mild cognitive impairments and subtle treatment-induced changes in performance. Including not only more tests, but also tests with a larger variety in complexity will make the assessment of cognitive impairment as well as (subtle) changes after NIBS better. Consensus on which tests to use for each cognitive domain will be very helpful for future studies.
Clinical Relevance
The generalization of treatment effects to daily-life situations is one of the main goals of (cognitive) rehabilitation. 71 Outcome measures at the level of activity or participation, however, were not regularly included in test batteries.11,64 These outcome measures were only included in 7 studies, and significant treatment effects were reported in 3 of 7 studies. In neglect studies that also included the Catherine Bergego Scale (CBS), a scale to assess the presence of neglect in everyday life situations,50,72 a treatment effect was found for scores on tests that assess the core deficit (ie, impairment of lateralized attention, measured with a LBT) but not for neglect during basic ADLs (as assessed with the CBS). This means that there are improvements at the level of function, but not at the level of activities and/or participation. One possible explanation for this is that although both tests evaluate presence and severity of neglect, the underlying concept and complexity of the tests are fairly different.73,74 It is also possible that the neglect is not obvious during static pen-and-paper tests but can still be manifested under more demanding, dynamic, and/or complex conditions during daily life. 70 ADLs involve complex factors, such as movements, execution of multiple simultaneous operations, and situations beyond peripersonal space, which are not incorporated in static tests. 75 With respect to cognitive rehabilitation, the CBS is viewed as a more clinically relevant outcome measure because of its sensitivity to change and transfer of treatment effects in daily life. 70 For the other cognitive domains, such ecologically valid tests were not included in the studies.
Interhemispheric Inhibition
The responsible mechanisms for the physiological effects of NIBS and improvements on outcome measures remain unclear. It is most likely that cortical stimulation promotes adaptive (re)organization in the brain. 76 A common explanation for the beneficial effect of cortical stimulation is based on the interhemispheric imbalance model. 13 This model assumes that a stroke-induced imbalance in interhemispheric signaling leads to increased activity or excitability in contralesional regions and reduced activity or excitability in ipsilesional regions because the lesion relieves interhemispheric inhibition through transcallosal pathways. Inhibitory NIBS of the contralesional hemisphere and excitatory NIBS of the ipsilesional hemisphere could lead to restoration of interhemispheric communication. 13 The existence of interhemispheric imbalance after stroke has been shown in studies on motor function, neglect, and attention.77-79 However, the model may be oversimplified, and it remains unclear whether the interhemispheric imbalance model can be applied to other cognitive functions. 80
There are suggestions that neglect can be alleviated by stimulating the parietal cortex, regardless of the nature (inhibition or facilitation) of stimulation. 41 Interhemispheric imbalance would affect core attentional processes, such as endogenous and exogenous control, and the PPC is a core node in this network. 81 Duecker and Sack 81 proposed a hybrid model of attentional control, where interhemispheric competition can be detected within parietal regions of the dorsal attention network, but not within frontal regions of this network. These models may explain the results of improved neglect recovery after iTBS to the contralesional hemisphere, moving beyond the notion of inhibiting the hyperexcitable hemisphere and facilitating the hypoexcitable hemisphere. 41 The rationale behind stimulation site might also be different for the various cognitive deficits.
Limitations
There are a few potential limitations to our review. First, we included some studies that were primarily aimed at upper-limb recovery, in which cognitive function was added as secondary outcome. Consequences of this primary focus may be that the NIBS target site was ideal for measuring effects on motor function, yet less ideal for improvement in cognitive domains. Second, we included studies with both ischemic and/or hemorrhagic strokes in our review. This may have caused outcome variation because it is not clear yet if the efficacy of NIBS is similar for both types of strokes or if cognition is similarly affected. Finally, lack of information on unpublished studies with nonsignificant results may have led to a biased interpretation of the results.
Conclusions and Suggestions for Future Research
This review shows that the use of NIBS may alleviate neglect after stroke. However, further research is needed to determine the most effective NIBS protocol(s) and to establish the (additional) effects of NIBS on other cognitive domains. A multicenter trial with multiple study arms for the different NIBS techniques and possibly additional therapies should be undertaken to explore similarities and differences. Precision medicine is another approach at the level of the individual. Genetics, algorithms, and computational models are used to make predictions about outcome and tailor treatment to the specific need of the individual. Our review pointed out that information on timing of intervention poststroke and severity of cognitive deficit was not always available or consistently reported. Similar terminology should be used and interventions in the different phases after stroke should be evaluated. Comparable protocols and parameters should be used (inhibitory vs excitatory, <5 versus ≥5 treatment sessions, patients from certain phases poststroke).
Ideally, future NIBS trials should include a standardized set of outcome measures to facilitate comparison between studies. Outcome measures assessing global cognitive function (cognitive screeners) seem less eligible because of the lack of specificity. 82 Several measures and approaches have been described to distinguish between statistically significant results and clinically relevant results, for example, minimal clinically important differences (cutoff values), Bayesian and graphical approaches, and the fragility index. 83 Outcome measures at the level of activities or participation or patient-reported outcome measures can also provide information on the patient’s perspective of recovery, outside the treatment setting. The Stroke Recovery and Rehabilitation Roundtable is working on consensus-based core recommendations for standardized measurement of sensorimotor recovery in stroke trials. 84 Such consensus-based recommendations should also be developed for the cognitive rehabilitation field. Quality of evidence should also be rated for the different outcome measures of interest according to the Grading of Recommendations, Assessment, Development, and Evaluation. 85
Supplemental Material
Supplement_2 – Supplemental material for The Effect of Noninvasive Brain Stimulation on Poststroke Cognitive Function: A Systematic Review
Supplemental material, Supplement_2 for The Effect of Noninvasive Brain Stimulation on Poststroke Cognitive Function: A Systematic Review by Eline C. C. van Lieshout, Roel F. van Hooijdonk, Rick M. Dijkhuizen, J. M. Anne Visser-Meily and Tanja C. W. Nijboer in Neurorehabilitation and Neural Repair
Supplemental Material
Supplement_3 – Supplemental material for The Effect of Noninvasive Brain Stimulation on Poststroke Cognitive Function: A Systematic Review
Supplemental material, Supplement_3 for The Effect of Noninvasive Brain Stimulation on Poststroke Cognitive Function: A Systematic Review by Eline C. C. van Lieshout, Roel F. van Hooijdonk, Rick M. Dijkhuizen, J. M. Anne Visser-Meily and Tanja C. W. Nijboer in Neurorehabilitation and Neural Repair
Supplemental Material
Supplement_4 – Supplemental material for The Effect of Noninvasive Brain Stimulation on Poststroke Cognitive Function: A Systematic Review
Supplemental material, Supplement_4 for The Effect of Noninvasive Brain Stimulation on Poststroke Cognitive Function: A Systematic Review by Eline C. C. van Lieshout, Roel F. van Hooijdonk, Rick M. Dijkhuizen, J. M. Anne Visser-Meily and Tanja C. W. Nijboer in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
The authors would like to express their gratitude to Ms Mariëlle Grosveld for her help in reviewing and rating of the articles.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Netherlands Organization for Scientific Research [VICI 016.130.662].
*
Please see Supplement 1 for a short explanation of the different techniques.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.