
Abstract
Introduction. The effects of long-term stretching (>6 months) in hemiparesis are unknown. This prospective, randomized, single-blind controlled trial compared changes in architectural and clinical parameters in plantar flexors of individuals with chronic hemiparesis following a 1-year guided self-stretch program, compared with conventional rehabilitation alone. Methods. Adults with chronic stroke-induced hemiparesis (time since lesion >1 year) were randomized into 1 of 2, 1-year rehabilitation programs: conventional therapy (CONV) supplemented with the Guided Self-rehabilitation Contract (GSC) program, or CONV alone. In the GSC group, specific lower limb muscles, including plantar flexors, were identified for a diary-based treatment utilizing daily, high-load, home self-stretching. Blinded assessments included (1) ultrasonographic measurements of soleus and medial gastrocnemius (MG) fascicle length and thickness, with change in soleus fascicle length as primary outcome; (2) maximum passive muscle extensibility (XV1, Tardieu Scale); (3) 10-m maximal barefoot ambulation speed. Results. In all, 23 individuals (10 women; mean age [SD], 56 [±12] years; time since lesion, 9 [±8] years) were randomized into either the CONV (n = 11) or GSC (n = 12) group. After 1 year, all significant between-group differences favored the GSC group: soleus fascicle length, +18.1mm [9.3; 29.9]; MG fascicle length, +6.3mm [3.5; 9.1]; soleus thickness, +4.8mm [3.0; 7.7]; XV1 soleus, +4.1° [3.1; 7.2]; XV1 gastrocnemius, +7.0° [2.1; 11.9]; and ambulation speed, +0.07m/s [+0.02; +0.16]. Conclusions. In chronic hemiparesis, daily self-stretch of the soleus and gastrocnemius over 1 year using GSC combined with conventional rehabilitation increased muscle fascicle length, extensibility, and ambulation speed more than conventional rehabilitation alone.
Keywords
Introduction
In stroke-induced hemiparesis, muscles undergo alterations that involve both physical shortening and viscoelastic loss of extensibility.1,2 Plantar flexors are particularly affected by such changes.3-5 Ultrasonographic studies have demonstrated architectural modifications in the medial gastrocnemius (MG), including decreases in fascicle length and increases in tendon length.6-10 These changes progress with time if muscles are left in a shortened position and result in a muscle disorder termed spastic myopathy, which has specific genetic determinants.11,12
Muscle stretch techniques are commonly used to treat loss of muscle extensibility after a stroke. Their effectiveness, however, has been questioned.13-17 Yet in animals with muscles previously immobilized in a shortened position, it has been shown that full-time muscle remobilization could reverse the genetic changes involved in spastic myopathy. 18 In animals with muscles immobilized in the stretched position, morphometric changes occur that include an increase in serial and parallel sarcomere numbers and an increase in cross-sectional area.19-23 It has also been shown that the restoration of range of motion after contracture strongly depends on stretch duration and stretch load. 24 The question then arises as to whether a specific high-load, long-term stretching program produces similar changes in patients with a spastic myopathy as the result of spastic paresis and whether clinical improvements are associated with specific muscle adaptations, such as increasing muscle fascicle length and muscle extensibility.
To our knowledge, no randomized controlled study has used an experimental phase of muscle stretching for more than 6 months, despite the need to better define the long-term effects of stretching.16,17 One way to achieve sufficient doses of daily stretch is by teaching patients prolonged, high-load, daily self-stretch postures, which are to be performed at home. This technique has been described in a diary-based program called the Guided Self-rehabilitation Contract (GSC).25-30 In a recent retrospective study, we used this strategy for at least a year in patients with very chronic spastic paresis, with an average of 8 years following an acute central nervous system lesion, including stroke. 30 We observed marked improvements in passive range of motion for 6 lower limb muscles, including plantar flexors, where a long-term (>1 year) prescription of daily self-stretch was utilized, compared with muscles in the same patients where this strategy was not implemented. 30
The main objective of this prospective, randomized, parallel-group trial was to compare ultrasonographic structural changes and clinical assessments in the soleus and MG muscles in patients with chronic hemiparesis following 1 year of conventional therapy (CONV) versus those also performing daily self-stretching using the GSC. The main hypothesis for this present study was that 1 year of guided self-stretch would increase fascicle length and muscle thickness in the soleus and MG more than conventional rehabilitation alone. Secondary hypotheses included the following: (1) extensibility of the 4 muscles evaluated clinically in this study (soleus, gastrocnemius, gluteus maximus, and rectus femoris) and ambulation speed would increase with the addition of GSC more than with CONV; (2) clinically measured soleus and gastrocnemius extensibility would correlate with ultrasonographic measures of their fascicle length and thickness; (3) changes in extensibility of the 4 investigated muscles would correlate with the reported daily time of their self-stretch posture; and (4) a composite score of clinical extensibility for the 4 investigated muscles would correlate with ambulation speed at each visit of the study.
Methods
Study Design
This was an ancillary study to a multicenter randomized controlled trial, Neurorestore (ClinicalTrials.gov: NCT02202954). The aim of Neurorestore was to compare the effectiveness of 2 rehabilitation programs on upper and lower limb motor function in individuals with chronic hemiparesis: CONV alone versus the GSC performed in conjunction with CONV. The primary outcome measure of Neurorestore in the lower limb was the maximal ambulation speed over 10 m, performed barefoot. 31 Six national centers were involved. The participants in this ancillary study were all individuals from one of the trial centers (Henri Mondor University Hospital, Créteil, France), at which ultrasonographic measurements of plantar flexors and clinical measurements of extensibility in 4 lower limb key muscles were systematically, prospectively performed by a blinded investigator. The study was conducted in compliance with the Declaration of Helsinki and local regulatory requirements.
Participants
Criteria for inclusion in the Neurorestore trial were the following: (1) adults with hemiparesis caused by a stroke that occurred more than a year before enrolment; (2) baseline spasticity angle ≥5° on the Tardieu Scale in at least 2 of the following muscles–soleus, gastrocnemius, gluteus maximus, or rectus femoris– to ensure that the patients included indeed had spasticity (defined as an enhancement of velocity-dependent stretch reflexes) 1 versus only muscle-shortening or “fixed contractures”11,32; (3) the ability to ambulate over 10 m barefoot and without an assistive device while maintaining a comfortable ambulation speed between 0.1 and 1.3 m/s 31 ; and (4) written consent for the experimental protocol. Main exclusion criteria were recurrent strokes, a significant orthopedic disorder in the lower limb, or severe cognitive, aphasic, or behavioral dysfunction that precluded effective verbal communication or patient participation. Pharmacological antispasticity treatments, including botulinum toxin injections, were allowed during the study.
Study Interventions
At the first visit, participants were randomized into 2 groups: GSC in addition to CONV (GSC group) or a CONV only group (CONV group; Figure 1). In both the GSC and CONV groups, participants freely participated in CONV sessions per their physician’s prescription. Around the trial centers where this study was performed, community-based therapy is typically prescribed clinically 3 times per week. In the GSC group, participants were additionally instructed in the GSC stretching techniques.
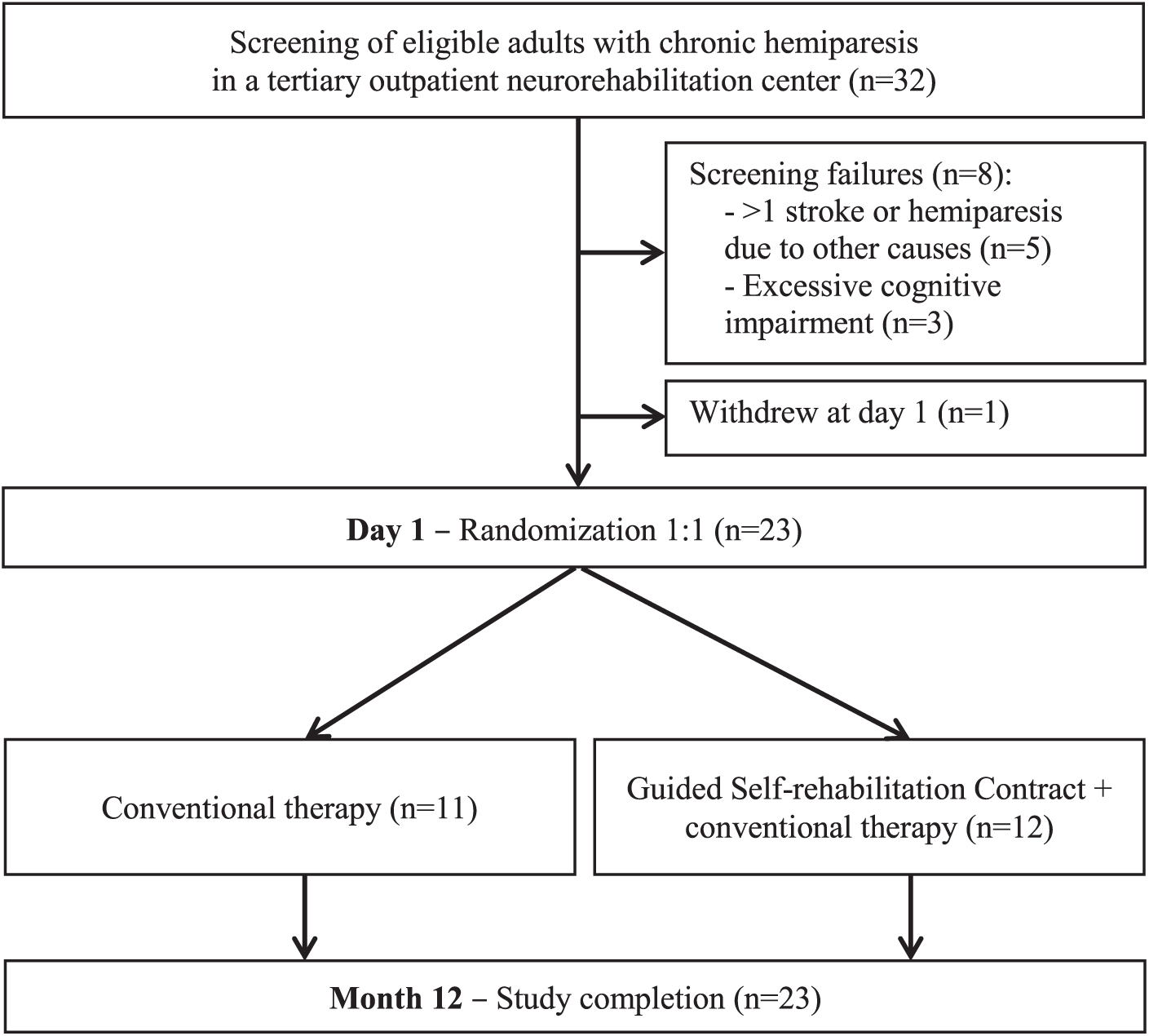
Flow diagram.
Principles of the GSC Method
The GSC methodology is a previously described and tested antagonist-targeting and diary-based strategy.25-30 In brief, the GSC is a reciprocal engagement between the patient and the therapist, which aims to increase the level of knowledge, responsibility, and motivation in order to ultimately increase the work intensity of the patient.
After randomization in the GSC group, the therapist explained the GSC methodology to the patient and specified the commitments for both patient and therapist. On one hand, the therapist was to identify relevant muscles to prescribe which muscles to stretch and to train against for each patient (see details below); educate through teaching and correcting the appropriate stretch and training techniques at each visit; and motivate by asking the patient to submit a self-monitoring diary to the clinician, containing the information on the practice accomplished according to the prescription since the last follow-up visit.33,34 On the other hand, the patient was to25,26 (1) perform daily the self-stretch and training program prescribed by the therapist and (2) record this activity on a diary and submit it to the therapist at each visit. Specifically, the therapist explained how to complete the diaries, which required the patient to record the daily stretching time and the number of active efforts accomplished in each training series every day, against each stretched antagonist.25,26 In addition, the therapist provided the patient with a manual that contained the prescribed stretching and exercise program and illustrations of each technique.25,26
The therapist then visited the patient at home every other week over the course of 1 year to retrieve and evaluate the diaries, with review and feedback on proper diary completion as a key strategy to maintaining motivation.33,34 The therapist also verified the self-stretch and training techniques being utilized, re-encouraged the patient, and modified the prescription depending on patient progress. Additionally, the therapist of the GSC group was free, at any point during the year, to initiate a self-stretching prescription for any new muscle, to temporarily halt the program if the interventions resulted in a symptom of concern (eg, if the patient felt any pain in the stretched muscle), or to decide, together with the patient, to change priorities in the treatment. For this study, all diaries of patients of the GSC group were collected by the therapist to later analyze the reported daily time of self-stretch posture as one of the outcome measures.
Specific Principles of the Self-stretching Techniques
Technically, the stretching program involved 2 stretching techniques for each targeted muscle: static self-stretching postures at high load and a series of rapid alternating efforts of maximal intensity against the muscle targeted for stretch. The first technique involved static postures of self-stretch at maximal load: participants were instructed to elicit and keep a strong and constant tension, but without pain, in the stretched muscle throughout the posture. The aim was to maintain this posture for a cumulative period of ≥10 minutes a day per stretched muscle. The second technique was an active training program that involved as many unassisted rapid alternating efforts or movements of maximum amplitude against the stretched antagonist muscle as possible over a short time (of 15 or 30 s).25,26 For example, the clinician would prescribe several daily 15-s series against the antagonist muscle being treated, depending on fatigability. Although the main objective of the training exercises was to gradually reduce antagonist co-contraction,35,36 such active exercises also provided phasic stretch to the co-contracting antagonist (through eccentric work) on each active movement. Practically, the patient was to alternate, for a given antagonist, between bouts of static self-stretch of the muscle and a series of active efforts against it. 25
Specific Description of the Stretching Technique for Each of the 4 Investigated Muscles
Self-stretch postures
For the soleus and the gastrocnemius muscles, the therapist asked the patient to use a scale and a wedge adapted to the degree of muscle shortening of these muscles (Figures 2A and 2C). The therapist also identified a secure and appropriate environment at home for the patient to implement these postures. Once the wedge was positioned on the scale, the patient placed the paretic foot on the wedge and then put as much weight as possible on the scale (with the knee flexed for soleus stretch and with the knee extended for gastrocnemius) to achieve sufficient load for the self-stretch posture. Self-stretched postures of gluteus maximus and rectus femoris have been previously described. 30 In brief, participants stretched the gluteus maximus while supine, bringing their knee as close as possible to their chest with the healthy hand (Figure 2G). For the rectus femoris, the patient wrapped an elastic strap around the ankle with the healthy hand while sitting, and then passed it over the opposite shoulder and pulled the strap with the good arm once supine. 30 Occasionally, other strategies were found by the therapist or patient depending on the environment at home (eg, Figure 2F).

Self-stretching techniques at home for the 4 investigated muscles: A. Self-stretch posture for the soleus muscle. B. Alternating efforts of maximal amplitude against soleus. C. Self-stretch posture for gastrocnemius. D. Alternating efforts of maximal amplitude against gastrocnemius. E. Alternating efforts of maximal amplitude against rectus femoris. F. Self-stretch posture for rectus femoris. G. Alternating efforts of maximal amplitude against gluteus maximus. H. Self-stretch posture for gluteus maximus.
Alternating efforts
Short series of as many rapid alternating maximal amplitude movements (phasic stretch) or efforts as possible in 15 s were also used for stretching. Against the soleus, the patient was to attempt maximal active dorsiflexions in the seated position (knee flexed, Figure 2B). Against gastrocnemius muscles, the repeated effort was the same but in the standing position (knee extended, Figure 2D). Against rectus femoris, the patient was asked to perform–in a standing position–repeat maximal hip extension and knee flexion efforts by pulling the heel toward the buttocks (Figure 2E). Finally, against the gluteus maximus, the active movements were hip flexion and knee flexion movements of maximal amplitude (Figure 2H).
Study Assessments
Participants were evaluated biomechanically and clinically at the beginning and end of the 12-month rehabilitation program by an assessor blinded to the treatment group. The primary outcome measure was the fascicle length in the soleus muscle measured by ultrasound. Secondary outcome measures were (1) other ultrasonographic architectural parameters, including soleus thickness, MG fascicle length, and MG thickness; (2) clinical measurements, including maximal extensibility (XV1 of the Tardieu Scale) of the soleus, gastrocnemius, gluteus maximus, and rectus femoris muscles 32 ; (3) reported daily time of self-stretch posture for each of these muscles over 1 year; and (4) maximal ambulation speed.
Muscle Architectural Parameters
For each patient, ultrasound images of the soleus and MG muscles were recorded through a biomechanical assessment and later analyzed by a single investigator to collect the architectural parameters planned in this study.
Equipment
The biomechanical assessment was conducted using an ultrasound diagnostic scanner, EZU-MT24-S1, with a EUP-L53 probe (Hitachi Ltd, Tokyo, Japan), set at a 13-MHz frequency and 50-mm depth (Figure 3A). An ankle ergometer, Techno Concept (Mane, France), with 2 force platforms and 3 sensors (front, left, and right) measured ankle plantar flexor torques with the knee flexed. Surface electromyography of the soleus and MG was monitored using 2 pairs of electrodes (Blue Sensor NF-00-S/12, ARBO H135TSG, Cambridge, UK) and a g.USBamp amplifier (G.TEC Medical Engineering GmbH, Austria) to ensure that the muscle undergoing analysis had no significant activity (<1% of isometric maximal voluntary contraction [MVC], see below) during the measurements (ie, was at rest).
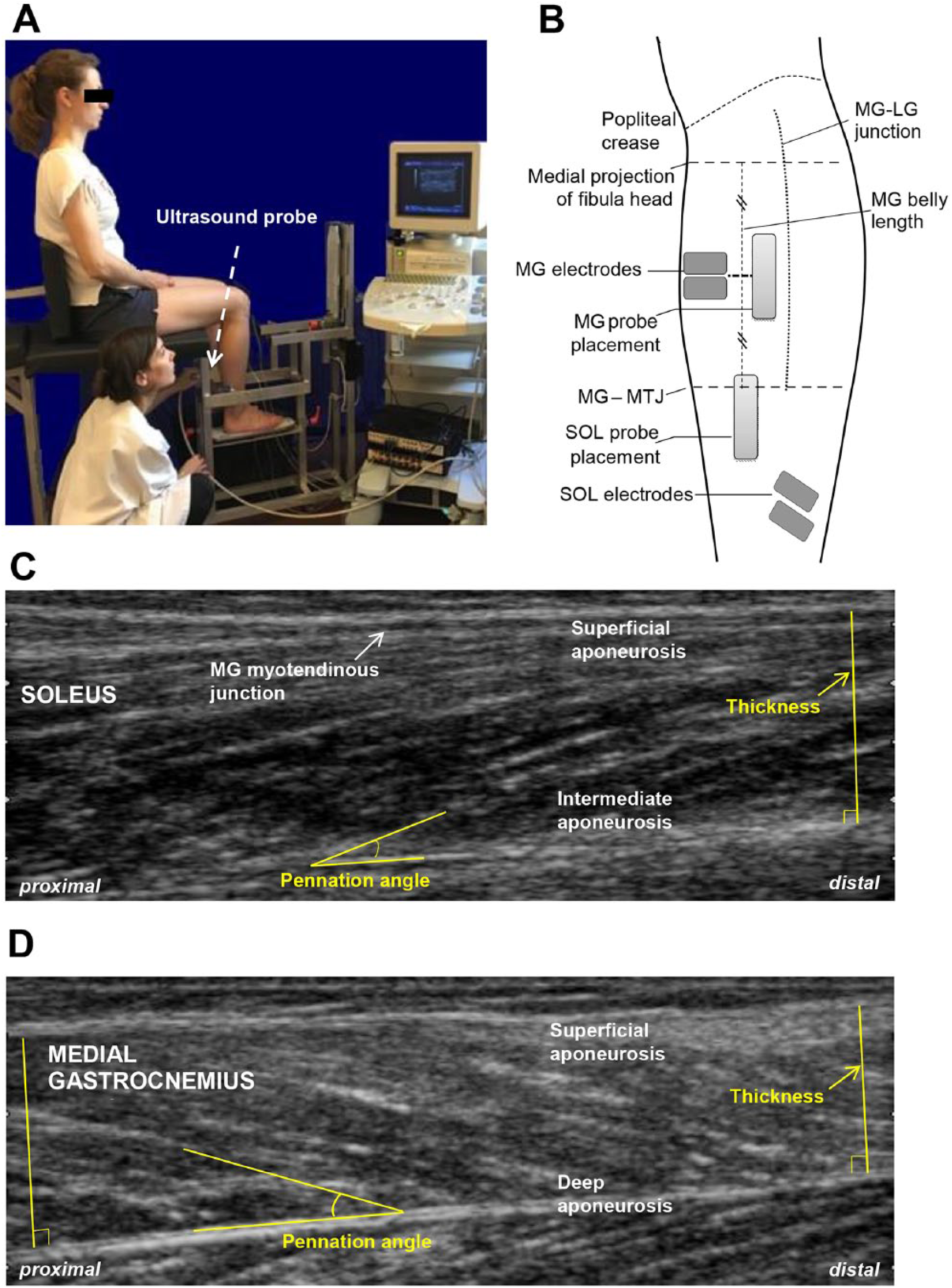
Methodology of ultrasound recordings: A. Position of patient in ankle ergometer with hip, knee, and ankle at 90°, maintained throughout the evaluation. B. Standardized positions of the probe during medial gastrocnemius (MG) and soleus (SOL) recordings and of the electrodes measuring simultaneously the electromyographic activity of these muscles. C. Measurements of pennation angle and muscle thickness of SOL using ImageJ software. D. Measurements of pennation angle and muscle thickness of MG using ImageJ software.
Experimental Procedure
Patient Position and Ultrasound Probe Placement
The patient was seated in the ankle ergometer in a reproducible position: hip, knee and ankle at 90° (Figure 3A). Ultrasound transmission gel was used for conduction between the probe and skin. The probe was always maintained perpendicular to the skin using lightweight pressure in order not to deform the skin.37,38 The investigator identified and marked the muscle-tendon junctions (MTJs) of the soleus (Soleus-MTJ) and the MG-MTJ. The MG belly length was estimated by taking the level of the proximal insertion from a horizontal projection of the fibular head to the medial side and measuring the distance between this line and the MG-MTJ (Figure 3B). These location specifications were not used as an outcome, but merely to standardize the MG ultrasonography probe location across assessments. Thus, for the soleus, the probe was placed immediately lower to the MG-MTJ, with this junction visible at the left of the ultrasound screen, and for MG, the probe was placed in the middle of the muscle belly, near the junction medial/lateral gastrocnemius (Figure 3B). A set of 3 images was recorded for each probe position.
Electromyograph (EMG) Electrode Placement
After the skin was abraded, 2 pairs of electrodes were positioned over the soleus and MG, adhering to Basmajian and Blumenstein 39 recommendations, while allowing for sufficient space for the ultrasound probe (Figure 3B). MVC was obtained during isometric contraction, as described by Baudry et al, 40 with the knee and foot strapped. Among 3 consecutive MVC tests, MVC was selected as the effort giving the highest level of EMG activity during the force plateau. Soleus and MG were then considered at rest if EMG activity was less than 1% of the activity obtained during isometric MVC. 41 Simultaneous monitoring of the force exerted on the ergometer and of EMG activity of the soleus and MG during ultrasound acquisitions was accomplished through a trigger signal.
EMG Data Analysis
EMG signals were amplified (gain 1000), bandpass filtered (30-3000 Hz), digitized (2500 Hz; Model 1401; Cambridge Electronic Design, Cambridge, UK), saved to hard drive, and processed using Spike2 software, version 7.02 (Cambridge Electronic Design), running on a personal computer. Signal processing involved DC removal, rectification, and smoothing using a 0.04-s time constant.
Analysis of Ultrasound Recordings
Muscle thickness and fascicle length were measured using ImageJ software. 42 All images were analyzed by the same investigator according to a previously described, standardized protocol. 43 For each muscle, only 1 of the 3 ultrasound images from the same reproducible location (defined above) was utilized for measurements. The choice was made based on image quality, including visible and parallel aponeuroses and visible fascicles.43,44
Muscle Thickness
Thickness was measured between the inner edges of the upper and lower aponeuroses, at the right of the MG-MTJ, and the right side of the image for soleus and at each lateral edge of the ultrasound image for MG (Figures 3C and 3D). Muscle thickness was defined as the average of these 2 measurements.
Fascicle Length
First, the pennation angle was measured as the angle between the muscle fascicle and the intermediate aponeurosis or the deep aponeurosis for the soleus or MG, respectively.38,44,45 Five angle measurements were performed. After eliminating the 2 extreme values, the pennation angle was defined as the mean of the 3 remaining angles. Fascicle length was then estimated according to previously described formulas, depending on the parallelism–or absence thereof–of the aponeuroses.43,44 The aponeuroses were considered parallel if muscle thicknesses measured at each edge of the ultrasound image differed by <2%. 44
Clinical Muscle Extensibility XV1 of the Tardieu Scale (PROM)
The passive extensibility (XV1) of each of 4 muscles of interest–soleus (XV1SOL), gastrocnemius muscles (XV1GAS), gluteus maximus (XV1GM), and rectus femoris (XV1RF)–was measured at each visit.11,32 XV1 of the Tardieu Scale is defined as the angle of arrest on the slow and strong stretch of the tested muscle (angle at which further slow-speed passive stretch would cause pain or jeopardize joint integrity) from zero as the theoretical angle of minimal stretch of the tested muscle group.11,30,32,46 XV1 provides insight on muscle tissue extensibility mostly.11,30,32,47 In this study, maximal passive extensibility of the 4 muscles of interest was measured as described previously (see e-Figure 1, available online, and legend). 30
During XV1 measurements, the patient was to stay supine and at rest as much as possible to minimize descending muscle activation. 1 XV1 was estimated with a goniometer at the knee and visually at the hip and ankle because reliability at these joints is similar whether using visual or goniometric evaluations of XV1. 48
Ambulation Speed
At each visit, ambulation speed over 10 m was measured barefoot at maximal speed, with the participant starting and ending the assessment seated. 31
Compliance With the GSC Program
Compliance in the GSC group was assessed based on the reported daily time for self-stretch, per muscle, as recorded in the subject diaries. In both groups, conventional rehabilitation time was also documented, without qualitative description of the treatment. Any antispasticity oral medications were also noted as well as the number, dates, doses, and locations of any botulinum toxin injections performed.
Statistical Analysis
Descriptive statistics were used for continuous quantitative variables, including fascicle length, muscle thickness, XV1, and ambulation speed. A Rank Analysis of Covariance test (Rank-ANCOVA) was used to compare the changes in fascicle length and thickness of soleus and MG (group and visit fixed factors; baseline value, covariate) as well as in XV1SOL, XV1GAS, XV1GM, and XV1RF from initial to final visits between the 2 groups. 49 Wilcoxon tests were used to compare the changes in ambulation speed in the 2 groups.
XV1Composite was computed as the mean of XV1 in the 4 muscles evaluated: XV1Composite = (XV1SOL + XV1GAS + XV1GM + XV1RF)/4. To reduce weighting discrepancies between the 4 evaluated muscles (normal values stated as: 120° for soleus, 115° for gastrocnemius, 150° for gluteus maximus and 240° for rectus femoris), XV1RF was reduced to two-thirds of its value. We compared the changes after 1 year in the 2 treatment groups using nonparametric testing.
We explored correlations between the architectural parameters (muscle fascicle length and thickness) of the soleus and gastrocnemius and their respective clinical measure of extensibility (XV1). We also explored correlations between the reported daily self-stretch time for each muscle and the mean ΔXV1 for that muscle between initial and final visits, and between XV1Composite and ambulation speed at each visit, using Pearson coefficients. All analyses were conducted with SPSS (18.0) software. Statistical significance was set at .05.
Results
Participant and Treatment Characteristics
Based on inclusion and exclusion criteria, 23 individuals were enrolled and randomized into the CONV (n = 11) and GSC (n = 12) groups (Figure 1). There were no significant differences in biomechanical or clinical participant characteristics between the groups at baseline, except for ambulation speed (Table 1). All participants had a spasticity angle >5° in soleus and gastrocnemius muscles (e-Table 1, available online).
Participant Characteristics, and Ultrasonographic and Clinical Parameters at Baseline in the GSC Group Compared With the CONV Group.
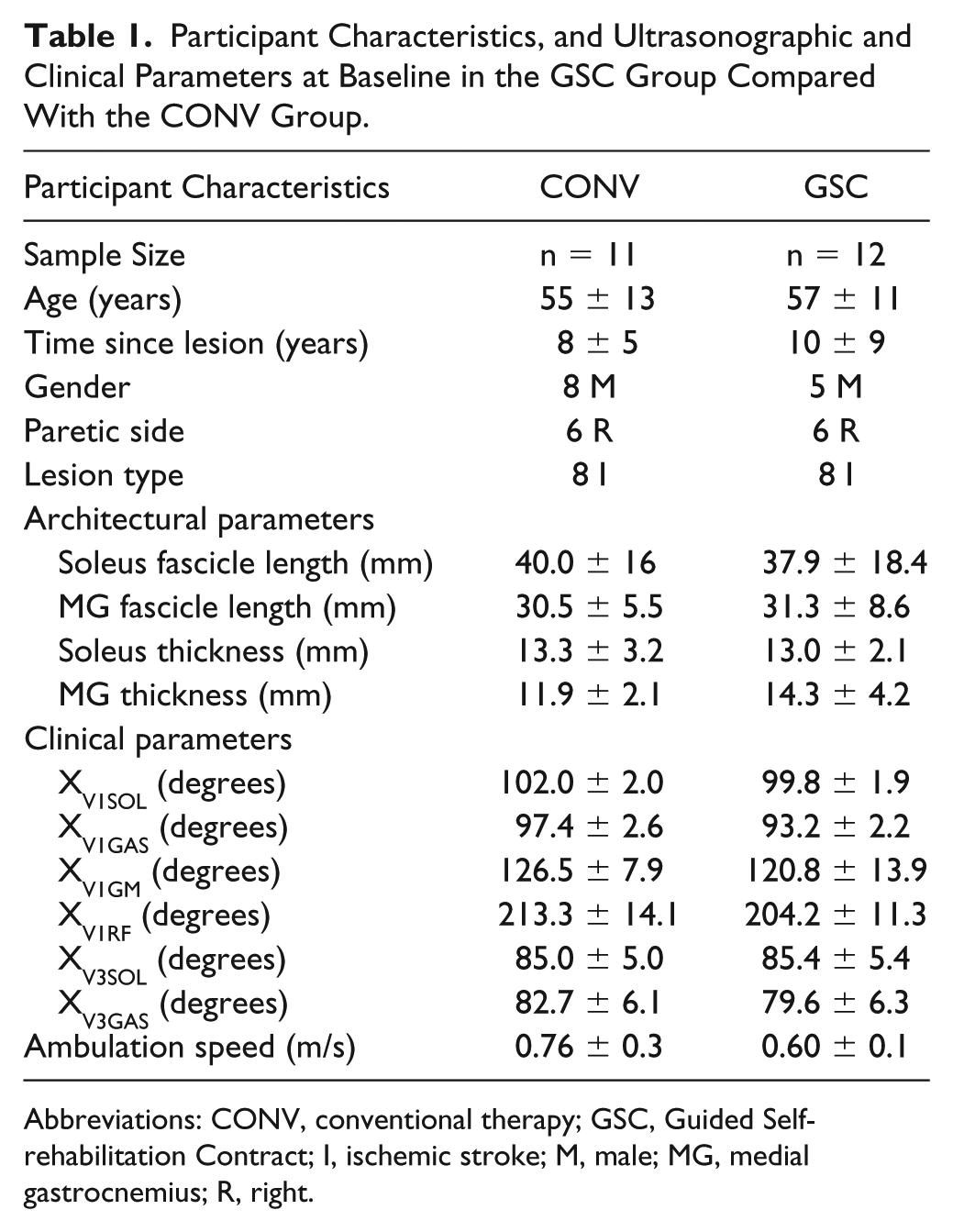
Abbreviations: CONV, conventional therapy; GSC, Guided Self-rehabilitation Contract; I, ischemic stroke; M, male; MG, medial gastrocnemius; R, right.
Amount of Conventional Therapy
In both groups, the frequency of the CONV sessions ranged from 0 to 3 sessions per week; the mean (±SD) time of conventional rehabilitation was 81.8 ± 55 min/wk (11.7 ± 7.8 min/d) for the CONV group and 57.8 ± 37.5 min/wk (8.2 ± 5.3 min/d) for the GSC group. Numbers of sessions per week varied by participant in both groups. In the CONV group, one individual did not undergo any conventional physiotherapy sessions during the study year, one participated in one 30-minute session per week, 4 in two 30-minute sessions/wk, and 3 in three 30-minute sessions/wk. Finally, 3 patients practiced three, 40-minute sessions/wk. Similarly, in the GSC group, 1 patient did not undergo any conventional physiotherapy sessions over the study year, 4 took part in one 30-minute session/wk, 3 in two 30-minute sessions/wk, 1 in three 30-minute sessions per week, and 1 in three 40-minute sessions/wk. No patient in either group took any systemic oral antispasticity agent throughout the 1-year follow-up.
Botulinum toxin was injected at some point during the 1-year follow-up in 3 patients of the CONV group and in 4 patients of the GSC group. Injection details, including timing, targeted muscles, and type and dose of the toxin injected, are reported in e-Table 2. Data from patients who underwent any botulinum toxin injection during the study period were excluded from the analyses of architectural and clinical changes in their injected muscles as well as from the ambulation speed analysis.
Self-stretching in the GSC Group
Of the 12 GSC patients, daily self-stretch postures were prescribed for at least a portion of the year for the soleus in 11 patients, for the gastrocnemius in 10, for the rectus femoris in 11, and for the gluteus maximus in 6. Data from patients who were not prescribed a daily self-stretch program for a specific muscle were excluded from analyses of all outcome measures for that muscle. Patients who were not prescribed a daily self-stretch program for the soleus and the gastrocnemius were also excluded from analysis of ambulation speed.
Compliance with respect to the prescribed program was 83% because 2 of the 12 patients (17%) did not perform the prescribed program for the entire year: 1 patient stopped the GSC after 8 months and another interrupted the program at month 6 for 6 weeks and then resumed until the end of the study year. The other 10 patients regularly practiced their same prescribed exercises and provided a completed diary throughout the year. The mean durations of daily self-stretch posture over the year, as recorded in the diaries, were as follows: 5.0 ± 3.3 minutes for soleus, 5.0 ± 2.1 minutes for gastrocnemius, 8.4 ± 3.9 minutes for rectus femoris, and 6.3 ± 3.2 minutes for gluteus maximus, for those patients in whom self-stretch was prescribed for the specific muscle evaluated. The mean cumulative daily duration of self-stretch postures was 24.7 ± 12.5 min/d for the 4 muscles combined.
Changes in Architectural Parameters
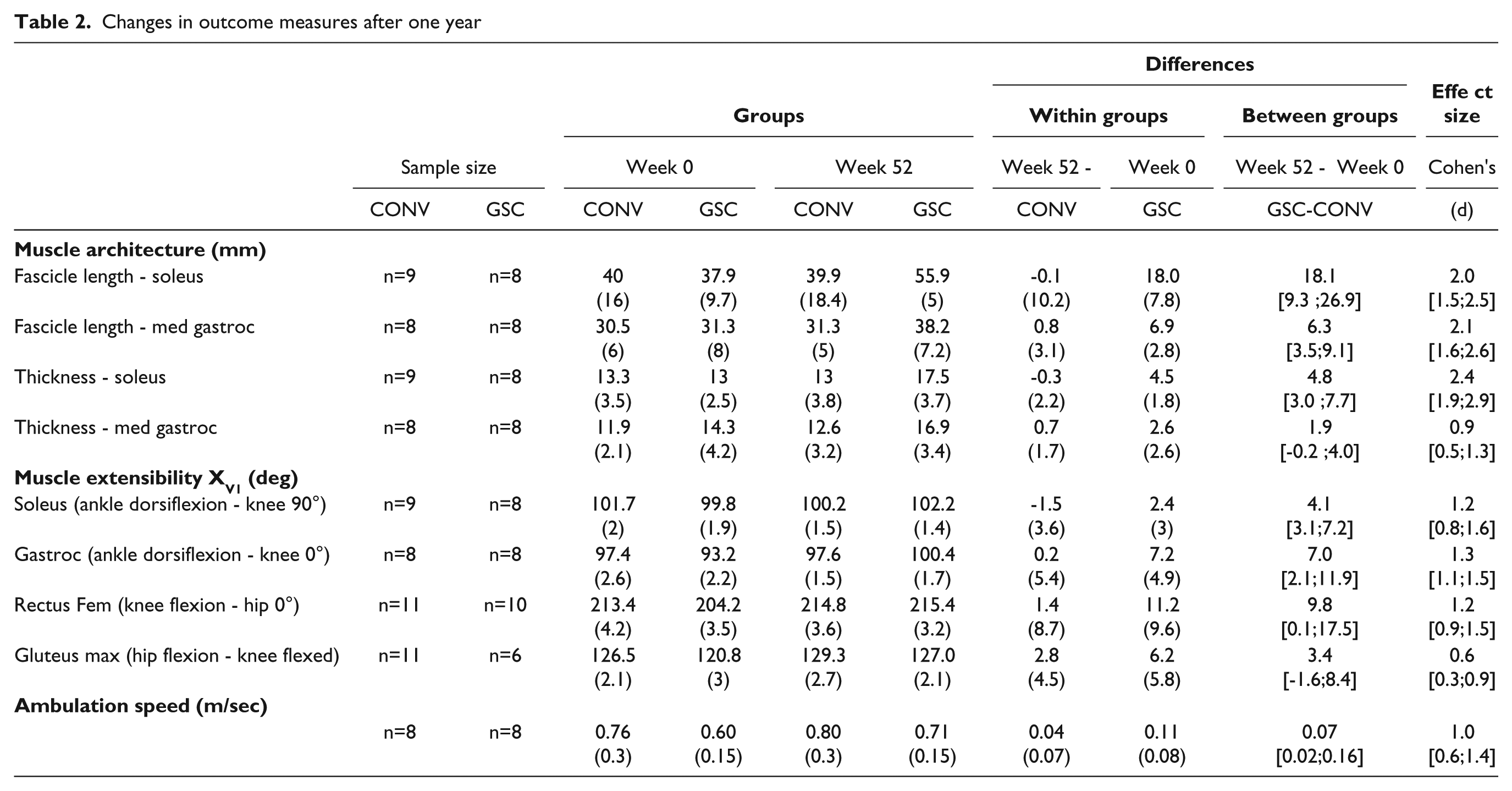
The between-group difference for the change in soleus fascicle length after 1 year was +18.1 mm (95% CI = [9.3; 26.9]), with greater length increase found in the GSC group (Table 2). Individual muscle changes for this parameter are displayed in Figures 4A and 4B. All other architectural changes after 1 year were also greater in the GSC group, except for MG thickness changes, which were similar in the 2 groups (Table 2).
Changes in outcome measures after one year
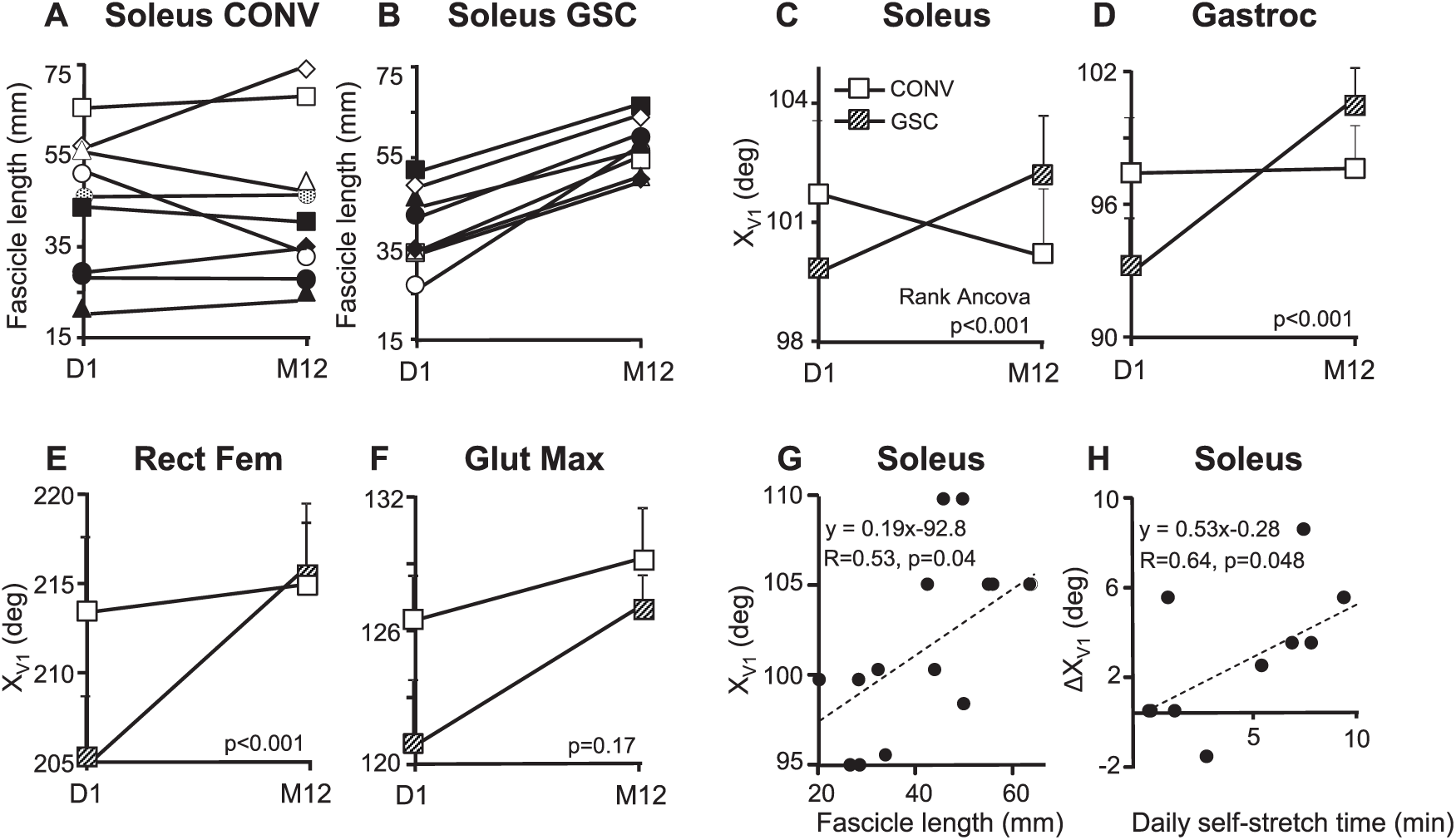
Changes in muscle architectural and clinical parameters after 1 year: A. Individual changes in soleus fascicle length in patients of the CONV group, from D1 to M12. B. Individual changes in soleus fascicle length in patients of the GSC group, from D1 to M12. C. XV1SOL in the GSC and CONV groups over 1 year. Data points, mean ± SEM. D. XV1GAS in the GSC and CONV groups over 1 year. Data points, mean ± SEM. E. XV1GM in the GSC and CONV groups over 1 year. Data points, mean ± SEM. F. XV1RF in the GSC and CONV groups over 1 year. Data points, mean ± SEM. G. Correlation between fascicle length and clinical measure of extensibility in soleus (XV1). H. Correlation between the reported daily time of soleus self-stretch posture and changes in clinical measure of soleus extensibility (XV1SOL).
Changes in Clinical Muscle Extensibility XV1
After 1 year, XV1 change was greater in the GSC group than in the CONV group for the soleus (between-group difference = +4.1°; 95% CI = [3.1; 7.2]), gastrocnemius (between-group difference = +7.0°; 95% CI = [2.1; 11.9]), and rectus femoris (between-group difference = +9.8°, 95% CI = [0.1; 17.5]; Table 2). Between-group differences for the XV1 change were not significant for gluteus maximus (Table 2 and Figure 4).
Changes in Ambulation Speed
After 1 year, the between-group difference in maximal barefoot ambulation speed also favored the GSC group, with an improvement in speed of +0.07 m/s [0.02; 0.16] compared with the CONV group (Table 2). In both groups pooled, ambulation speed tended to correlate with XV1Composite, both at baseline and at 1 year (R = 0.41, P = .07, and R = 0.44, P = .051, respectively; Pearson).
Correlations Between Clinical Muscle Extensibility and Other Parameters
At baseline, XV1SOL correlated with soleus fascicle length (R = 0.53, P = .04, Pearson; Figure 4G) and tended to correlate with muscle thickness (R = 0.49, P = .06; Pearson), whereas XV1GAS did not correlate with muscle fascicle length or thickness (R = 0.06, P = .42, and R = 0.09, P = .37, respectively; Pearson). For the soleus, ΔXV1 correlated with the daily time of self-stretch posture (R = 0.64, P = .048, Pearson; Figure 4H), with a similar trend noted for the gastrocnemius (R = 0.61, P = .08; Pearson). No correlation was found for the gluteus maximus (R = 0.29; P = .58) or rectus femoris (R = −0.04; P = .51).
Discussion
This long-term prospective randomized controlled trial in chronic spastic paresis indicates that a daily plantar flexor self-stretch program within a GSC, performed along with CONV for 1 year, increased soleus and MG fascicle length and soleus thickness more than CONV alone. Measurements of passive muscle extensibility (XV1) in the soleus, gastrocnemius, and rectus femoris as well as ambulation speed also improved more than with CONV alone. Correlations were noted between ultrasonographic measurements of soleus fascicle length and clinical measurement of soleus extensibility (XV1SOL), and these soleus extensibility changes at 1 year also correlated with the diary-based reported daily time of soleus self-stretch posture. Thus, similar to what has been observed in short-term studies in animals with remobilized muscles, a long-term self-stretch program in our patients with chronic spastic paresis partially reversed architectural and clinical manifestations of spastic myopathy. 18
Effect Sizes and Potential Clinical Significance of Architectural Changes With GSC
The effect sizes for all between-group differences in architectural parameters were greater than 2.0 (except for MG thickness), which represents very large effects. 50 One of the architectural changes–namely, fascicle lengthening–may reflect the addition of serial sarcomeres.19-21 This may account for the observed increase in clinical muscle extensibility because these measurements for soleus (XV1SOL) correlated with the primary outcome measure of soleus fascicle length.
There was also a very large effect size for soleus thickness increase with GSC. In healthy patients, a 3-minute static gastrocnemius stretch, 5 days per week for 6 weeks, is sufficient to induce muscle thicknening. 51 The present results also corroborate classic animal data, which show that muscle thickness, cross-sectional area, and force production increase after prolonged stretch programs.22,23
The nonsignificant between-group difference in muscle thickness changes for MG could be explained by differences in fiber type composition and pennation angles, as previously shown in rabbit plantar flexors, 52 or more likely by the ultrasound assessment position used (knee flexed, ankle at 90°), which resulted in different tensions applied to each plantar flexor, and was more appropriate to evaluate soleus architectural parameters because of the higher level of tension in the soleus (see study limitations below). The correlation found between soleus fascicle length and XV1SOL as well as the trend between soleus thickness and XV1SOL, compared with the absence of these findings in the gastrocnemius, are consistent with this hypothesis.
The effect sizes for between-group differences in clinical extensibility of the soleus, gastrocnemius, and rectus femoris were smaller than those for architectural parameters, with wide CIs. 50 Finally, a small between-group difference was found for ambulation speed, also favoring the GSC group. 50
Reliability of Muscle Architectural Measurements
Muscle architectural parameters can be assessed with good to high reliability using ultrasonography, particularly for large limb muscles in a relaxed state, as in the present study.38,45,53,54 Among the strengths of this study are that a single, blinded assessor analyzed all ultrasound images, standardized probe locations were used for each muscle, and the probe was positioned perpendicular to the skin with a tilt range <5°; such factors have been shown to enhance ultrasound measurement reliability.45,54,55
Regarding fascicle lengths, the mean baseline fascicle length of each muscle was lower than normal values reported for healthy patients tested in the same position6-8: soleus mean fascicle length in healthy adults was 43 mm compared with 38 mm in this study, and MG fascicle length was 40 mm compared with 30 mm in this study. 6 As for muscle thickness, a previous study finding of 17 and 15.5 mm for the MG and soleus, respectively, in healthy patients, contrasts to the 13 mm in each muscle in this study. 53 Thus, our findings confirm and quantify a measure of calf muscle atrophy in chronic hemiparesis.51,53,55 Of note, only changes greater than 4 mm for fascicle length and 1 mm for muscle thickness may be considered beyond common standard errors for these measures and, thus, reflect significant changes in muscle architecture. 38 Changes of this magnitude were found in the GSC group only in the present study.
Stretch Techniques Involved in the GSC
In GSC, 2 different techniques were implemented for each muscle selected: a static self-stretch posture at high load and active series of efforts against the muscle targeted. Whether one or both of these techniques produced the changes seen in the various parameters is unknown. The correlation between daily self-stretching time and gains in extensibility for soleus (and trend in the MG) and the well-recognized importance of intensity and duration of stretch suggest that the increase in muscle fascicle length and extensibility was at least partly a result of the daily static self-stretch postures at high load.24,56-58 In addition, while performing a series of rapid alternating efforts of maximal intensity, some patients were unable to achieve movements of sufficient amplitude to generate any significant eccentric work on the stretched co-contracting antagonist (Figure 2D). However, this technique is also effective in reducing antagonist co-contractions and improving selectivity of the motor command 35 and, therefore, may have contributed to the increase in walking speed observed in the GSC group. A trial specifically comparing the effects of daily self-stretch postures versus rapid alternating efforts against the antagonist targeted for stretching is required to differentiate the impact of each technique.
Daily Time of Self-stretch Postures
A critical objective of the GSC strategy is to increase and sustain the amount of daily self-stretching postures. 25 This was achieved in this study, with a mean cumulative time devoted to the daily self-stretch postures for the 4 investigated muscles of about 25 min/d in the GSC group: that is, 175 min/wk compared with the 82 min/wk of CONV in the CONV group. As mentioned above, in the GSC group, changes in clinical soleus extensibility correlated with the daily time of soleus self-stretch posture (Figure 4H), which confirms data in animals and humans.24,56-58 Although these daily times of self-stretch for soleus and gastrocnemius muscles were less than recommended in the GSC strategies (≥10 minutes per stretched muscle), they may still have been sufficient to effect changes in theses muscles’ parameters, in view of the between-group differences found. For proximal muscles, however, we could not find correlations between time of self-stretch and extensibility changes. Of note, the gluteus maximus was rarely included in the self-stretch program, and in the rectus femoris, XV1 measurements have been found to be less reliable compared with other muscles. 59
Passive Muscle Extensibility (XV1) and Ambulation Speed
A modest but significant between-group difference of +0.07 m/s was found for ambulation speed, favoring the GSC group. There were trends for correlation between XV1Composite and ambulation speed at study onset and end, which corroborates trends previously published. 30 Accordingly, at baseline, the lower mean ambulation speed in the GSC group was associated with consistently lower XV1 for each muscle evaluated in this group (Table 1). Parallel observations have recently been reported in the upper limb of stroke patients, with ultrasound measured average fascicle length in elbow flexors significantly correlated with upper limb impairment level. 60
The specific gains in clinical plantar flexor extensibility reported here are likely to be functionally relevant because Schulz 61 demonstrated in healthy patients that an increase of 1.9° of additional active dorsiflexion in the swing phase was functionally meaningful in reducing trip risk. In this population with spastic paresis, it is possible to assume that changes in active dorsiflexion (not specifically measured in the present study) would parallel those observed in passive dorsiflexion because close correlations have been found between passive (XV1) and active (XA) measurements,62,63 and a recent work indicated an almost degree-for-degree improvement of passive and active ranges of dorsiflexion, together with strong correlations between active dorsiflexion and gait speed after a single intervention to reduce plantar flexor overactivity. 64 Of interest, the CONV-alone group was characterized by the same small change in ambulation speed (+0.04 m/s) as that previously found with long-term CONV. 65
Taken together, these observations suggest that overall lower limb muscle extensibility, among other parameters, affects ambulation speed, supporting the functional relevance of a program aiming to gain muscle extensibility, such as in GSC.
Limitations of the Study
The present study was only ancillary in a larger trial, and thus, muscles other than calf muscles were analyzed despite not being the primary target of this study. However, it is not believed that this invalidates the results. In terms of ultrasound measurements, limitations related to the techniques used might have affected some findings. Fascicles of the paretic plantar flexors were sometimes difficult to visualize using ultrasonography, which could have increased data variability. More important, patients were seated with the knee flexed for the assessments at 90° of dorsiflexion. Thus, lower tension in the gastrocnemius may have affected fascicle length or thickness measurements for this muscle compared with measures in the soleus, as has been discussed in the section “Effect Sizes and Potential Clinical Significance of Architectural Changes With GSC.” 9 Although ultrasound assessments were initially attempted in the knee extended position also, that position often caused discomfort and was not pursued. Further study quantifying the level of tension applied to each evaluated muscle in this study could help clarify to what extent the knee flexed positioning may have affected MG results.
From a statistical point of view, samples sizes were small. Botulinum toxin injections were allowed before and during the study period, and data were evaluated after excluding these patients, although combining toxin injection with therapy is current clinical practice in many centers. Additional issues affecting sample size related to differences in muscles to be stretched with GSC. Measurements were not included for evaluation if the patient did not perform the self-stretch program for the specific muscle being considered. For the gluteus maximus, as previously indicated, the small number of patients who were prescribed a self-stretch posture of this muscle might have contributed to the lack of significant results. In addition, this muscle is difficult to self-stretch efficiently by the patient, particularly when active function in the paretic arm is poor. 30 There was some variability in the self-stretching prescription for different muscles over different periods. Yet this variability is inherent to the GSC program, designed to allow the therapist to individualize the self-stretching prescription to the patient and the current situation. Despite these limitations affecting sample size, some of the changes in architectural parameters were highly significant, which suggests that tissue-modifying effects of submaximal self-stretch practiced for only about 5 minutes a day over 1 year might be powerful enough in plantar flexors of adult patients with chronic hemiparesis to result in the observed architectural differences.
The change in clinical extensibility of the plantar flexors (XV1) was also small. Among these differences, for gastrocnemius muscles, the between-group difference in extensibility changes (7°) was beyond the observed margin of errors of measurements but that in XV1SOL changes (4.1°) may have remained within the intrarater margin of error of measurements (5° for a single assessor). 59 However, as discussed above, these clinical changes are similar to those found in a previous long-term study in patients with hemiparesis, 30 and the correlations found suggest that overall lower limb muscle extensibility affects walking speed.
Finally, only quantitative data regarding the weekly time of CONV were retrieved for each patient; qualitative information on the variable techniques used by community-based therapists were not collected and could have differed between patients and groups.
Conclusion
In patients with chronic hemiparesis, a daily self-stretch program of soleus and gastrocnemius using GSC techniques combined with conventional rehabilitation over 1 year led to increased muscle fascicle length, extensibility, and maximal barefoot ambulation speed more than with conventional rehabilitation alone. Therapists might consider prescribing daily high load self-stretch postures within GSC when aiming to restore better architectural muscle parameters and extensibility in shortened plantar flexors.
Supplemental Material
Supplemental_Materials – Supplemental material for Ultrasound Structural Changes in Triceps Surae After a 1-Year Daily Self-stretch Program: A Prospective Randomized Controlled Trial in Chronic Hemiparesis
Supplemental material, Supplemental_Materials for Ultrasound Structural Changes in Triceps Surae After a 1-Year Daily Self-stretch Program: A Prospective Randomized Controlled Trial in Chronic Hemiparesis by Maud Pradines, Mouna Ghedira, Raphaël Portero, Ingrid Masson, Christina Marciniak, Dawn Hicklin, Emilie Hutin, Pierre Portero, Jean-Michel Gracies and Nicolas Bayle in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
The authors thank Caroline Giroux and Stevy Farcy for their technical assistance during the biomechanical assessments in this study, and Cheyenne Yammine for her thorough proofreading of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.